
Abstract
Diabetes distress has been shown to be highly prevalent in adults living with type 1 and type 2 diabetes with important implications for glycemic control, self-care, and self-management behaviors. Despite considerable focus on self-management and glycemic targets during pregnancy, current literature lacks information on diabetes distress in pregnancy, particularly in women with type 2 diabetes. This article outlines an explanatory sequential mixed methods research protocol to examine diabetes distress during pregnancy in women with pre-existing diabetes. The aims of the study were to: (1) establish the prevalence and correlates of diabetes distress in women attending a diabetes and pregnancy clinic; (2) use this quantitative data to inform development of an interview guide and plan for sampling for telephone interviews; and (3) explore and describe the experiences of diabetes distress during pregnancy. The quantitative strand was a cross-sectional survey of 76 women using self-reported questionnaires to collect demographic and clinical data, and validated tools to assess health variables, including the outcome of interest of diabetes distress using the Problem Area in Diabetes scale. The qualitative strand applied interpretive description methodology to explore the quantitative results using semi-structured qualitative interviews with 18 women to obtain patient perspectives of diabetes distress and experiences of managing diabetes in pregnancy. The explanatory sequential mixed methods research will provide an opportunity to add contextual qualitative experiences from women with pre-existing diabetes during pregnancy to provide a comprehensive picture of diabetes distress. The results will inform further research priorities that protect and promote mental health, psychosocial well-being, and self-management practices for this population.
Keywords
What Is Already Known About The Topic
- Diabetes distress is highly prevalent in the adult type 1 and type 2 diabetes populations. - There is limited evidence to inform the prevalence of diabetes distress and how women experience diabetes distress in pregnancy.
What This Paper Adds
- Identifies methods (with supporting rationale) that can be used to investigate diabetes distress in pre-existing diabetes in pregnancy. - Describes how an explanatory sequential mixed methods study design can be utilized to explore and explain complex clinical phenomena during pregnancy with pre-existing diabetes.
Introduction
The experience of pregnancy can be both a joy and stress for some women. For women with pre-existing diabetes, there are additional unique stressors during this time. While previous work examining the duality of managing the chronic health condition of diabetes during pregnancy has established important insights into the challenges women encounter, there is a need for research methods to comprehensively explore this issue in greater depth.
Pre-existing diabetes in pregnancy refers to type 1 diabetes (T1D) or type 2 diabetes (T2D) diagnosed before pregnancy (Feig et al., 2018). Rates of pre-existing diabetes have been increasing, largely driven by increases in obesity and T2D in women of reproductive age (Feig et al., 2018; Swinburn et al., 2011). In a large population study in Ontario, Canada, between 1996 and 2010, the number of women with pre-existing diabetes in pregnancy doubled from 0.7% to 1.5% (Feig et al., 2014). The rates of pre-existing diabetes among pregnant women in Canada from 2010 to 2011 was 2.7 per 1000 deliveries for women with T1D and 4.3 per 1000 deliveries for women with T2D (Public Health Agency of Canada, 2016).
Pre-existing diabetes in pregnancy is considered to be a high-risk condition due to the increased risks of adverse obstetrical outcomes including congenital malformations, spontaneous abortion, macrosomia, pre-term birth, preeclampsia, and stillbirth (Feig et al., 2006, 2018; Macintosh et al., 2006; Persson et al., 2009). Due to these risks, women with diabetes are tasked to adhere to strict blood glucose targets before and throughout pregnancy to lower their risks (Murphy, et al., 2010; The Diabetes Control and Complications Trial, 1996), which requires frequent self-monitoring of blood glucose and intensive insulin regimens (Feig et al., 2018; Wahabi et al., 2012).
Background
The challenges of coping with demanding diabetes self-management during pregnancy have been described in the qualitative literature (Berg, 2005; Berg & Honkasalo, 2000), however there is limited research that has specifically examined diabetes distress (DD) within the context of pre-existing diabetes and pregnancy.
Diabetes distress refers to the negative emotional state where individuals living with diabetes experiences feelings such as stress, anxiety, and guilt because of the burden of their diabetes self-management (Fisher, Skaff, & Mullan, 2008). Diabetes distress has been found to be significantly associated with poorer glycemic control, decreased self-care and self-management behaviours, and increased levels of depressive symptoms in adults with T1D and T2D (Fisher et al., 2010; Strandberg et al., 2014). Depression is another common challenge for individuals with diabetes, with estimates that 10–20% of individuals with T1D and T2D are affected by depression (Roy & Lloyd, 2012). While DD and depression are constructs that share features and frequently present as comorbid conditions, DD is defined by the specific context of living with the chronic disease of diabetes and the emotional response to diabetes stressors (Snoek et al., 2015).
Research conducted in women with GDM and T1D offers compelling signals that pregnancy is a time when women may be particularly vulnerable to DD. While women with GDM have diabetes temporarily for a short duration at the end of pregnancy, recent studies found elevated DD levels in 36% (Schmidt et al., 2019) and 40% (Lydon et al., 2012) of study participants. Another study of women with GDM found more frequent blood glucose monitoring, insulin use, dissatisfaction of clinical care, and lack of support from providers and partners were all significantly associated with higher distress scores (Kopec et al., 2015). Importantly, results from the study by Schmidt et al. (2019) indicate that DD may be a significant predictor of adverse pregnancy outcomes in women with GDM such as pre-eclampsia, macrosomia, jaundice, hypoglycemia, and caesarean section (aOR 4.70, p = 0.02).
Results from two small European studies of pregnant women with T1D showed nearly one-quarter (24.3%) were experiencing DD in early pregnancy (Linden et al., 2016) and at 28 weeks’ gestation, high mean DD scores indicated elevated levels of distress (Egan et al., 2017). A literature review by Rasmussen et al. (2013) of the transition to motherhood from pregnancy in women with T1D identified psychological well-being as a key theme throughout the 16 studies reviewed. Women reported increased stress during pregnancy, fears about losing the baby, and poor adjustment to pregnancy, indicating with these findings that psychological emotional distress was a common outcome (Rasmussen et al., 2013).
While this emerging evidence suggests that DD is a problem for women with GDM and T1D with clinically relevant levels of distress, there are important knowledge gaps. The qualitative literature has not specifically examined the experience and perceptions of DD during pregnancy. The population of women with T2D is particularly understudied and the current literature on women with T1D has methodological limitations, including small sample sizes, lack of confirmatory statistical results and not studying DD as the main outcome. Mixed methods studies have not yet been conducted that collect data on prevalence and correlates of distress and also explore distress qualitatively with patients to better understand its meaning and why some patients may become distressed and others do not in order to individualize management. Overall, there is a need for rigorous study of the prevalence and determinants of DD using a mixed methods approach to comprehensively address this multifaceted issue. Therefore, this study addressed those gaps of methodology and quality of available evidence by studying a local, Canadian population of pregnant women with T1D and pregnant women with T2D.
Objectives
The aim of this study was to examine DD in women with pre-existing diabetes in pregnancy from both quantitative and qualitative perspectives. This was accomplished by addressing the following objectives for women with pre-existing T1D and T2D in pregnancy: (a) determine the prevalence of DD and depressive symptoms; (b) determine the clinical and demographic correlates of DD; (c) explore the perceptions of DD in pregnancy; and (d) integrate the quantitative and qualitative findings to give a holistic picture of the prevalence and meaning of DD in order to gain insights on the scope of the problem and implications for diabetes care.
Methods
Explanatory Sequential Design
Mixed methods research uses both qualitative and quantitative methods in a single study for data collection and analysis and places emphasis on integrating the findings from both approaches (Tashakkori & Creswell, 2007). Mixed methods research enables the researcher to balance the strengths and weaknesses of both approaches (Morgan, 2014), which in combination with data integration leads to a deeper and richer understanding of the study phenomenon (i.e., DD) than if only quantitative or qualitative data were collected on its own. In this study, an explanatory sequential study design was used. This design consisted of an initial quantitative strand that was followed by a separate qualitative strand (Creswell & Plano Clark, 2018).
The purpose of an explanatory sequential design is to expand and elaborate on the study findings from the quantitative strand of the study through qualitative methods in the second strand (Creswell & Plano Clark, 2018). The depth and scope of DD understanding will be broadened through findings that come from both quantitative and qualitative methods. The other purpose of mixed methods is to achieve complementarity, which is the “explanation, elaboration, illustration, or clarification of results” from the quantitative strand with results from the qualitative strand (Greene et al., 1989). In this study, the qualitative results will provide insight into how to explain the statistical findings that come from the quantitative strand, potentially validating findings and assisting with answering the mixed methods question (Figure 1). Explanatory sequential mixed methods diagram.
As the function of this study is to explain and expand on the initial quantitative findings of DD with qualitative methods, a mixed methods approach was the most appropriate research methodology to achieve those aims. Lastly, a need existed to describe the quantitative results with detailed participant voices and perspectives.
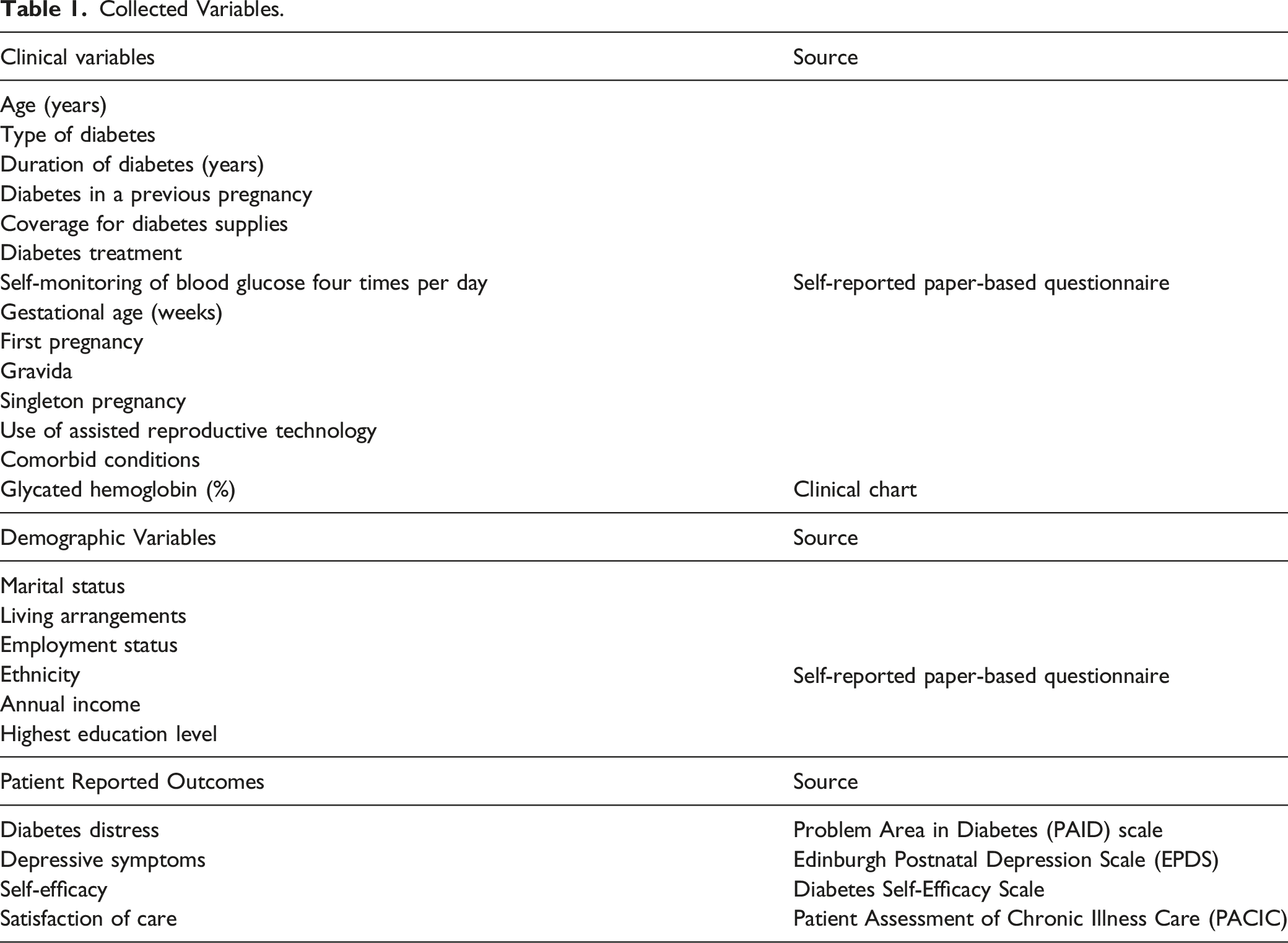
Quantitative Strand Design
Collected Variables.
Sample
The population was recruited from a diabetes and pregnancy clinic within a tertiary care hospital in Southern Ontario, which serves a large catchment area and is diverse in terms of ethnicity and socioeconomic status. Women who met the following inclusion criteria were eligible for the study: (1) 18 years of age or older; (2) followed at the tertiary care hospital diabetes and pregnancy clinic for obstetrical care; and (3) have a pre-existing clinical diagnosis of T1D or T2D. Individuals who were unable to read, write, or speak English were excluded from participation as there were no translation services available to complete the questionnaires or interviews.
Recruitment
Patients were recruited using a convenience sampling approach. Patients were approached during their pregnancy during a routine clinical visit by a member of their circle of care with information about the study. If the patient gave permission to discuss the study further, an overview of the study was provided by a member of the research team before informed consent was obtained in the privacy of a clinical room. The total sample of 76 women were recruited, which was sufficient to calculate the primary outcome of DD prevalence.
Data collection
Paper-based questionnaires were self-administered by the patient and checked by the research team for completeness and clarity at the end of the clinical visit. The most recent glycated hemoglobin value, the standard measure of glycemic control, was extracted from the patient chart. The questionnaires used in this study were the PAID scale to measure the primary outcome of DD, the EPDS to measure depressive symptoms, the Diabetes Self-efficacy Scale to measure self-efficacy, the Patient Assessment of Chronic Illness Care (PACIC) to measure patient satisfaction of care, and a demographic questionnaire to obtain demographic and clinical characteristics such as gestational age, living arrangements, education, ethnicity, income, employment, self-monitoring blood glucose frequency, and comorbid conditions.
Problem areas in diabetes scale
The PAID scale has 20 items rated on a five-point Likert scale of 0–4 and an overall score of ≥40 is considered to be positive for DD (Welch et al., 1997). The PAID scale has been found to contain four subscales: emotional problems, lack of social support, treatment-related problems, and food-related problems (Snoek, Welch, Pouwer, & Polonsky, 2000). The scale has been validated in diabetes populations and reliability for the scale was measured by internal consistency and it was found to have a high internal consistency score, with Cronbach’s alpha of 0.95 (Polonsky et al., 1995). Limitations of this tool include that it has not been validated for this study population or had reliability testing completed in women with pre-existing diabetes during pregnancy. Researchers demonstrated 2-month test-retest reliability of the tool (r = 0.83) and concurrent validity, showing significant associations between DD and theoretically-related constructs such as general emotional distress, disordered eating, depression, self-care behaviors, and diabetes coping (Polonsky et al., 1995).
Edinburgh postnatal depression scale
The EPDS is a 10-item scale that asks how the user has been feeling emotionally over the past 10 days. Questions are scored between 0–3 points per the scoring guide. Total score is calculated by adding the individual items for each question. A score above 13 indicates high risk for depression (Murray & Cox, 1990). This scale has been validated in both postpartum and pregnancy populations and has established reliability and construct and concurrent validity. The EPDS was found to have a low sensitivity of 77%, high specificity of 90%, and positive predictive value of 50% (Murray & Cox, 1990). High reliability of the EPDS was found with Cronbach’s alpha scores of 0.82, 0.83, and 0.84 for first, second, and third trimester, respectively (Rubertsson et al., 2011). Concurrent validity was established with Pearson’s correlations coefficient of >0.50 (p < .00) for all three trimesters.
Quantitative data analysis plan
Descriptive statistics was performed to calculate means, standard deviations, and frequencies of demographic and clinical variables collected. Inferential statistics for calculation of prevalence, independent t-tests, chi-square tests, linear and logistic regressions, and correlations was done using SPSS software. A p value <.05 was considered statistically significant. Prevalence for DD and depressive symptoms was calculated as the number of women who have a total PAID score ≥40 for DD and a total EPDS score ≥13, respectfully, divided by the total number of women in the study sample. To determine the associations between the continuous variables of DD scores, EPDS score, glycated hemoglobin, diabetes duration, age, gestational age, self-efficacy score, gravida, and PAID subscale scores, the Pearson R correlation coefficient was calculated. A chi-square test was conducted to examine differences between PAID DD and EPDS depressive symptom scores of women with T1D compared to T2D diabetes. To determine if there are differences in the sociodemographic and clinical characteristics in women with T1D compared to women with T2D, independent t-tests were conducted to compare means between the variables including age, gravida, gestational age, glycated hemoglobin, diabetes duration, PAID score, EPDS score, and self-efficacy score.
Qualitative Strand Design
Interpretive description was used to address the following qualitative research questions: (1) How do women with pre-existing diabetes receiving obstetrical care at a high-risk clinic in Ontario perceive DD during pregnancy? (2) How does the experience of varying levels of DD impact pre-existing diabetes management in pregnancy? Interpretive description is an approach to qualitative research that acknowledges “the constructed and contextual nature of human experience that at the same time allows for shared realities” (Thorne, Reimer Kirkham, & MacDonald-Emes, 1997). This method looks at a clinical issue or phenomenon that is relevant to one’s clinical discipline with the goal of developing themes and patterns that will help create an interpretive description that can be using to inform clinical understanding and practice (Thorne et al., 2004: 5). Because the aim of this methodology is to create knowledge that is relevant for the clinical context of applied health disciplines, this would make the findings relevant to clinical nursing practice (Thorne, 2016).
Sampling procedures
The qualitative strand used three types of purposeful sampling: nested, stratified, and theoretical. Nested sampling is a characteristic of explanatory sequential mixed methods designs in which the same individuals who took part in the quantitative stand are sampled again in the qualitative strand (Collins et al., 2007). Therefore, the same inclusion/exclusion criteria applied in the quantitative strand was also applied to the qualitative strand. The exception was that women could currently be pregnant and receiving obstetrical care at the tertiary care hospital or be in the postpartum period.
Qualitative research uses purposeful sampling, made possible through nested sampling in this study, in order to find and select information-rich cases (Palinkas et al., 2015). Purposeful sampling is a process of selecting certain units or cases based on a purpose rather than random selection (Collins et al., 2007) and can be used to achieve representativeness or comparability. This allowed the selection of a broader group of cases and set up comparisons between different types of cases. Results from the quantitative strand were reviewed to inform decision-making for qualitative sampling, with the potential to apply stratified and theoretical sampling. Stratified sampling showcased subgroups and allowed comparison across subgroups (Creswell, 2013) and was congruent with the qualitative study question because stratified purposeful sampling captured variations in the phenomenon of interest of DD (Palinkas et al., 2015). To facilitate this sampling, the cohort of participants from the quantitative strand were stratified by PAID DD scores and diabetes type. PAID scores were stratified into categories of high score/positive for DD (PAID ≥40) and low score/negative for DD (PAID <40). The initial interviews were then purposely initiated with women from both the categories of high score/positive for DD and low score/negative for DD and included both T1D and T2D. Following analysis of these initial interviews, theoretical sampling took place. Theoretical, or theory-based, sampling involves selecting participants based on emerging concepts or constructs (Palinkas et al., 2015). The objective of theoretical sampling is to elaborate on these concepts/constructs as they are uncovered by exploring their properties and variations (Palinkas et al., 2015). This form of sampling required the researcher to observe the direction the qualitative data was taking and let the data guide their subsequent sampling. It included examining the patterns, gaps, and outliers in the data and choosing subsequent participants to interview based on what constructs or variables, such as gravida, social support, and gestational age, needed further exploration and analysis.
Sampling in qualitative research typically occurs until data saturation is reached as there are no set guidelines or calculations for sample sizes to dictate when to stop data collection (Creswell, 2013; Patton, 2002; Thorne, 2016). Data saturation is when the researcher sees no new information being obtained and data is considered adequate (Morse, 1995). One justification for selecting a sample size range from Thorne (2016) is the assessment if background literature indicates that a phenomenon frequently occurs within the clinical population, and if so, whether selecting a small number of individuals to speak on their experience of that phenomenon will produce adequate data. Review of the literature suggests that DD is highly prevalent in the adult T1D and T2D population in Canada (Nicolucci et al., 2013) and has also been observed in women with pre-existing diabetes and gestational diabetes (Dalfra et al., 2009; Egan et al., 2017; Linden et al., 2016; Lydon et al., 2012; Kopec et al., 2015; Snoek et al., 2015). With this rationale, it was estimated that the number of women to be sampled in this strand would be approximately 18–20. In the proposed research, signals in the data that showed adequacy and comprehensiveness of the information indicated that no further samples were needed to answer the qualitative question (Morse, 1995; Patton, 2002) after interviews with 18 participants.
Data collection
Qualitative data was collected through semi-structured, one-to-one interviews, a common method for data collection in qualitative research to obtain rich information from participants (Creswell, 2013). Interviews were conducted over the telephone with a single interviewer (HT) to ensure consistency. Due to context of the COVID-19 pandemic, a shift from in-person interactions in clinical spaces had become a necessity. Fortunately, there are several established benefits to conducting interviews over the telephone including decreasing the burden and cost to the participants while avoiding extra travel (Musselwhite et al., 2007) and increasing flexibility to work around participant’s personal schedules while avoiding the constraints of finding time and space in a clinical setting. While telephone interviewing means that body language and other visual cues cannot be observed (Carr & Worth, 2001), there may be some welcomed anonymity in a telephone interview that allows participants to share their responses more openly and reduced response bias through increased comfort (Musselwhite et al., 2007).
The interviews were audio-recorded and took approximately 60 minutes per participant. Personal health information collected during the audio-recording was de-identified and kept confidential and secure on a password protected computer. The interviews were transcribed from the audiotapes verbatim.
A concurrent and iterative process of data collection and analysis was used. The first interview was led with a semi-structured interview guide and had optional probing questions. The interview guide was then shaped by the findings identified in the quantitative strand, the student thesis advisory committee, as well as stakeholder perspectives from a nurse practitioner and obstetrician gathered in a team meeting.
Qualitative data analysis plan
NVivo Version 11 computer software was used for organizing, coding, and analyzing study data. Two members from the research team reviewed all the transcripts. Analytical memos were kept throughout data analysis that capture themes, emerging patterns, questions, and any other pertinent elements about the data and phenomenon under study (Thorne, 2016). Interpretive description does not prescribe a single technique for data analysis (Thorne, 2016). Findings were built inductively by picking important elements in the data, grouping and sorting them into patterns, and the identifying the relationships that exists between the individual pieces of data and patterns. The initial analysis included reflection of the words and phrases that jumped out in an interview transcript. Early coding consisted of broad-based coding and after using a generic coding scheme and spending time on analysis, the collective whole of the data was reviewed and other codes assigned (Thorne, 2016). This was an active process to allow restructuring of the patterns within the data.
Constant comparative analysis is a type of inductive thematic analysis that was used to assign codes, group codes into categories, and compare themes/categories to each other (Thorne et al., 2004). This approach compares new data to emerging themes in order to determine if data supports and further develops the themes or provides contradictory results. In this method, data elements of interviews, statements, and themes were compared to all others that were the same or different (Thorne, 2016). Following coding, the analysis moved from data to patterns then relationships. Attention in analysis process was shifted between individual cases, the whole data set, similar cases, and contrasting cases so that associations and relationships in the data could be examined. The literature was consulted regularly to verify if the knowledge being developed from the data was truly novel and how others may view the data (Thorne, 2016).
The thoughtful clinician test was used to share the emerging themes and interpretations created by the research team with diabetes educators and physicians who work in diabetes and pregnancy clinic to obtain feedback if the findings were consistent with their experiences providing care for this population (Thorne et al., 2004).
Rigor
Strategies to promote rigor, or trustworthiness, were implemented during the qualitative strand of the study. Trustworthiness is made up of the elements of credibility, transferability, dependability, and confirmability (Lincoln & Guba, 1985). Credibility is validity, or believability, of the results (Lincoln & Guba, 1985). Prolonged time in the field completing 18 interviews of approximately 60-minute duration each was one action taken to ensure credibility. Triangulation is another method (Lincoln & Guba, 1985), which was done by verifying the data sources of interview notes against interview transcripts (Creswell, 2013) and triangulating researcher and stakeholder interpretations and experience against the data by using the thoughtful clinician test described above (Thorne et al., 2004). A credibility check was also used, which is when researchers using interpretive description review themes and interpretations with stakeholders (e.g., diabetes educators, physicians) so they may assess whether the initial findings are in alignment with their experiences (Thorne, 2016). The concurrent data collection and iterative analysis also served as a verification method for trustworthiness in this study.
Transferability is observed if the research conducted can be transferred to other contexts and was achieved through clear description of the study methods used to sample the participants and the study setting and context (Creswell, 2013; Lincoln & Guba, 1985). Description also included providing the demographic and clinical characteristics of the qualitative sample, which will assist readers to determine if the findings can be applicable to their local population. Dependability refers to findings that are consistent and repeatable and confirmability means that findings are neutral and supported by the data rather than biases (Lincoln & Guba, 1985). Rigor in these two areas were preserved by keeping an audit trail of the study processes and details so that other researchers could audit the research process, replicate the study, and attest to researcher objectivity (Creswell, 2013). All study processes were thoroughly documented, which included field notes, reflexive journals, interview guides and recorded interviews, and data analysis and interpretation notes.
The researcher who conducted the interviews (HT) kept a reflexive journal to document ideas, interpretations, and reflections of each interviews and to address personal assumptions of biases (Creswell, 2013). An initial reflection was documented by the researcher that declared her position, assumptions, biases, and expectations of the proposed research. Journal entries were created after every study interview to document feelings, opinions, challenges, and initial insights to create transparency.
Mixed Methods Integration
The first point of data integration was data connection (Creswell & Plano Clark, 2018) and occurred when the analyzed quantitative data was used to inform the subsequent qualitative data collection, specifically the sampling plan and interview guide development. Integration of qualitative and quantitative data occurred at a second point in this study during study interpretation (Creswell & Plano Clark, 2018). Following their separate analyses, the quantitative and qualitative data was integrated through data displays and development of meta-inferences (Creswell & Plano Clark, 2018).
Joint Mixed Methods Results Table.

One aim in the interpretation phase was to answer the overarching mixed methods question, which was done through the development of meta-inferences (Creswell & Plano Clark, 2018), the conclusions in a mixed methods study made by integrating the findings from the different qualitative and quantitative strands (Teddlie & Tashakkori, 2009). The following are example questions that were asked of the data to make meta-inferences: (1) Were there any different results learned in the Strand 2: Qualitative Study compared to the Strand 1: Quantitative study? (2) How do the interview responses about perceptions of DD during pregnancy build on the knowledge of prevalence and distress scores in this group? (3) What is the broader understanding of the phenomenon of DD in pregnancy?
Ethics
This study received approval by the Hamilton Integrated Research Ethics Board as an amendment of Assessing the Determinants of Pregestational Diabetes Control: A Prospective Cohort REB #14–222. All participants gave free and informed consent before taking part in any research activities. After a member of their circle of care introduced the study, a research team member obtained written consent in a private clinic room. Any women who participated in quantitative strand and who agreed to participate in the qualitative strand were asked to provide a separate verbal consent over the telephone to reflect additional participation in the interviews.
There was a risk that some women would meet the score threshold for high likelihood of depression. If that occurred, the process that was followed as outlined in the consent form was to inform their most responsible provider in the clinic for assessment. If a participant did not have a history of anxiety or depression, a referral to the women’s mental health clinic would be made by the most responsible provider. There were minimal risks associated with taking part in the qualitative phone interviews. Participants were informed that some questions they were asked could be interpreted as sensitive and they could choose not to respond if any question made them uncomfortable or upset. In the event that women experienced increased distress during the interview, there was the opportunity to debrief with the interviewer at the end of the interview in order to address any negative emotions or stress they were feeling. If the women found they were experiencing high levels or increased distress following the interviews, a referral to the women’s mental health clinic could be facilitated with the participant’s consent to allow them to meet with a mental health professional.
Significance and Implications
The holistic approach of nursing care includes addressing the psychosocial aspects of one’s health. In the context of diabetes, this is critically linked to one’s ability to self-manage their diabetes. As such, diabetes nurse educators and their interprofessional colleagues are well positioned to prevent, identify, and mitigate DD in individuals with diabetes.
The results from this study will add to what is known about DD in pre-existing diabetes and provide health care professionals working with this pregnant population understanding of: (1) the impact of this phenomenon on pregnancy and glycemic control; (2) who may be at risk of experiencing DD; (3) the patient experience of DD and their needs; (4) how health services can be improved to provide care to this population during pregnancy.
This study will provide research methodology that can be scaled up across the province, throughout Canada, or worldwide. Future work can include replicating cross-sectional surveys in other clinics to establish DD prevalence in larger cohorts in different settings across Ontario and Canada. This will allow regional, provincial, and national prevalence of DD in this population to be established. By ascertaining which correlates form a profile for risk, screening for DD could be targeted appropriately by those health care professionals with appropriate scope of practice.
Lastly, the study results may inform the development of new guidelines and interventions to prevent, support, and manage DD during pregnancy. Interventions such as peer support, health coaching, and tailored self-management education and support are all within the scope of health care professionals to deliver. By understanding the extent of DD and women’s experiences of DD, it can allow for the identification and adaptation of existing interventions or development of novel interventions that target DD during this time-sensitive period for women with pre-existing diabetes.
Conclusion
This explanatory sequential mixed methods study design will provide a comprehensive understanding of the scope, associated factors, perceptions, and experiences of DD in women who have T1D and T2D in pregnancy. The findings of this study will give insight into the need for further screening of DD in pregnancy and help create the foundations for tailored care of pregnant women who are experiencing DD.
Footnotes
Acknowledgments
We are grateful for the support from the clinical staff who contributed to study recruitment and triangulation of the qualitative findings. We would like to give our sincere thanks to all the women who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the researcher HT has received funding received by the researcher HT through awards granted by the Registered Nurses Foundation of Ontario (Diabetes Nursing Interest Group Research Scholarship), Canadian Nurses Foundation (AstraZeneca Award), and the Endocrine Awards (Diabetes Nurse Educator Gold Award).
Ethics
This study received approval by the Hamilton Research Ethics Board as an amendment of Assessing the Determinants of Pregestational Diabetes Control: A Prospective Cohort REB #14–222.