
Abstract
‘Dementia - Personalised Care Team’ (D-PACT) is a five-year NIHR funded programme, using realist methods to develop and evaluate a complex, person-centred intervention for people with dementia and their carers. During the early project stages, we engaged with multiple stakeholders, including people with dementia and their carers, to develop an initial programme theory (IPT) – into an elaborated programme theory (EPT), by helping to uncover intervention mechanisms leading to outcomes in specific contexts. Realist research methods for developing programme theories are under-reported. In addition, there is a paucity of practical guidance on how to engage underserved and vulnerable populations in complex interventions programme theory development. We attend to these gaps, providing a worked example of how we meaningfully engaged people living with dementia and carers, alongside field experts, as stakeholders in this process. Our IPT theory building included multi-stakeholder primary research exercises and meetings with PPI contributors and an Expert Reference Group. We adapted interview schedules, and used visual resources and scenario-based activities, to support stakeholders to think in a ‘realist’ way. Using realist and thematic analyses led to hypothesis-building of causal mechanisms. Sharing findings with stakeholders led to further refinement of the intervention design, ready for testing in a subsequent feasibility study. We found that, despite the cognitive challenges associated with dementia, innovative methods of engagement can enable this stakeholder group to understand the realist approach and provide a platform through which to share their experiences. Taking a highly flexible and unhurried approach, led to novel insights into the complexities of person-centred dementia support. We argue for more detailed methodological guidance, based on realist principles, on how to collaborate with underrepresented populations to rigorously gain insights as to what is likely to make a difference and refine initial programme theory.
Keywords
Background
Qualitative research methods can help researchers and practitioners understand key features of an intervention: how it works and how it should be delivered in order to activate mechanisms that will lead to the intended outcomes (Lewin et al., 2009). Stakeholder engagement in IPT development helps identify their priorities, and any tensions, ambiguities and varying pathways to outcome attainment, ensuring that the intervention is more likely to be feasible and effective for the context in which it is developed (O’Cathain et al., 2019). The realist approach to theory-building and evaluation (described below) advocates the collection and analysis of multiple data sources and perspectives to (a) understand how contextual factors influence health interventions and (b) uncover the underlying social and psychological factors identified as influencing programme outcomes (Gilmore et al., 2019).
The Realist Approach
Realist evaluation aims to understand complex social programmes, evaluating ‘what works, how, for whom, in what circumstances and to what extent?’ (Pawson et al., 2005; Pawson & Tilley, 1997). Realist review and realist evaluation are grounded in the realist paradigm (e.g. Wong et al., 2016; Pawson, 2006a), which situates between positivism (there is a real world can be apprehended directly through measurement) and constructivism (there is no singe reality; knowledge is constructed from human experience, e.g. Lincoln & Guba, 1986). Realism understands there is an objective reality which people interpret through cognitive and social processes. Realist research seeks to understand how and why interventions take effect by identifying, developing, testing and refining programme theory about how unobservable causal mechanisms interact to produce outcomes (Hawkins, 2014).
Developing and refining IPT is the first step in a theory-driven realist research cycle (Muckumbang et al., 2017). A fundamental tenet of realism is that every intervention implicitly applies, indeed requires, a programme theory: a set of ideas about what those who designed it want the intervention to achieve and how this will be achieved (Pawson & Tilley, 2001). Designing a practical intervention involves formulating prospectively and predictively a theory of what the key intervention components will be, how they will produce the outcomes that its designers want (Funnell & Rogers, 2011; Pawson & Tilley, 1997; Punton et al., 2020). There are various approaches to analysis in realist research, and the theory/building/refining process, but they all attempt to code and categorise data using the concepts of context, mechanism resources/reasoning and outcomes in some way (Power et al., 2019). The IPT formulates how the intervention, when introduced into pre-existing contexts, will activate mechanisms (and which mechanisms) to produce the intended outcomes (Kazi, 2003).
Mechanisms are understood as the ways in which a programme’s resources interact with the reasoning and unconscious reactions of the people using the intervention (Pawson & Tilley, 1997; The RAMESES II Project, 2017). The effect of such mechanisms is potentiated or constrained by personal, structural and organisational factors, known as ‘contexts’ (Pawson, 2006a; Pawson et al., 2005). IPTs represent ideas about how mechanism responses elicited through the intervention and introduced into pre-existing contexts may lead to outcomes (Kazi, 2003).
This involves articulating key intervention components and intended outcomes, as well as the possible underlying causal ‘mechanisms’, and, if possible, the required context(s) (Muckumbang et al., 2017; Pawson, 2002; Pawson et al., 2005). ‘Context, Mechanism (Resource and Response) and Outcome’ configurations (CMMOs) provide an analytical tool in realist evaluation (Dalkin, Forster, 2020). CMMOs convey that intervention resources/components (Mechanism resources) are brought to bear upon a person experiencing an intervention, in a way that influences a change in reasoning or reactions (‘Mechanism responses’), which in turn alters their behaviour leading to measurable or observable ‘Outcomes’ (Dalkin et al., 2015). Candidate IPTs about how an intervention works are gathered through various sources, consolidated, and refined iteratively, to explain how and why complex interventions work or don’t work. For example, Handley et al. (2017, p.8) developed realist statements capturing intervention theories on improving dementia-friendly hospital care, including:
‘Where behaviours that challenge are understood as communication of an unmet need
In realist theory building, statements may not cover all four elements, depending on the nature and stage of the research. The CMMO configuration is a heuristic designed to reflect the generic common structure of generative mechanisms, and so frame theory building. Other such heuristics exist (e.g. Mukumbang et al., 2018).
Realist methods involve theory-focused (as opposed to more open-ended) qualitative interview techniques (Manzano, 2016; Pawson, 1996). With candidate theories in mind, the interviewer might present aspects of IPT for interviewees to comment on (an explicit theory testing approach; likely to be more effective with policy makers and some practitioners) or test the IPT in other less direct ways (e.g. eliciting data about the effects of contextual factors from potential intervention recipients). Provided that realist interviewers adopt a theory-building mind-set, understand the IPT, and are alert to contexts, mechanisms and outcomes, they can plan their probe questions in the moment as an interview progresses. For example, a question about potential mechanisms might be = ‘What is it about that, that made or would make a difference to you?’ This ‘retroductive’ approach attempts ‘the identification of hidden causal forces that lie behind identified patterns or changes in those patterns’ (The RAMESES II Project, 2017, p.1). It can be used for IPT development, in addition to traditional inductive and deductive forms of reasoning, to build an understanding about how underlying mechanisms interact with different contexts to produce particular outcomes (Gilmore et al., 2019). However, this method is under-reported in realist evaluation (Manzano, 2016; Mukumbang et al., 2020).
Engaging Stakeholders in Realist Research
Calls for greater transparency in reporting how to develop programme theories using realist methods have been made previously (e.g. Welch & Tricco, 2016). Yet, there is still a lack of guidance, with clear practical examples, on the methods for doing so when formulating the IPT for a new intervention – including lack of advice on how to engage multiple stakeholders (particularly vulnerable, under-served populations) in this process. For interventions involving social generative structures, that is, social, organisation, policy and some psychological interventions (Dixon-Woods, 2014), potential enactors and beneficiaries are likely to know and understand something about the mechanisms, the contexts moderating mechanism activation, and what outcomes these stakeholders (as opposed to designers) would want from the intervention. Eliciting the knowledge, as part of developing the evidence base for new complex interventions, is likely to require the use of mixed research methods (Maciver et al., 2021). Extensive though it is, existing realist methodological literature says comparatively little about methods for producing an initial programme theory in these ways. It contains methodological studies and guidance for conducting realist reviews and evidence synthesis (Greenhalgh et al., 2011; R. Pawson et al., 2005; Pawson; Bellamy, 2006; Rycroft-Malone et al., 2012; Wong et al., 2013), but less about harnessing stakeholders’ perspectives in doing so. Those who have lived experience of issues under investigation can provide insights (e.g. Involve, 2012) unique to their personal knowledge of that experience. Research involving such individuals has been undertaken in various under-represented (in research) populations such as those with mental health difficulties (e.g. Pearson et al., 2015; Miller, Cook & Alexander, 2006; Shields et al., 2007), and older people (Clough et al., 2006; Littlechild, Tanner & Hall., 2015). UK health policy already regards public and service user involvement in healthcare research, including developing and evaluating complex healthcare interventions, as good practice (DfH, 2010; Mockford et al., 2012; MRC, 2019).
More specifically, publications on involving stakeholders with, or interested in, dementia to date, have mainly constituted evaluation protocols (e.g. Harding et al., 2018; van den Kieboom et al., 2019); reports on experiences of people with dementia involved in research (e.g. Waite et al., 2019), and the findings of such research (e.g. Handley, Bunn & Goodman, 2019; Ritchie et al., 2019). Few papers report on the process of involving people with dementia in developing theory-driven complex interventions. Handley et al. (2019) used realist interview techniques with people with dementia, but did not describe in detail how, given the cognitive challenges. Tolson and Schofield (2012) noted the lack of studies explaining in detail what methods are required, and that remains the case.
In the initial stage of the D-PACT project (see Box One for a summary of the project), we aimed to define and develop key components of a Dementia Support Worker (DSW) intervention for people with dementia and their carers based in primary care sites in two English regions (NW and SW). In this article, we contribute to filling gaps in literature, by describing, and critically appraising, the realist methods we used to engage stakeholders, including people with dementia, in contributing to the initial programme theory for D-PACT that we developed during our phase 1. We note the challenges associated with engaging in this way with this specific population group and the strengths and limitations of our approach. Finally, we conclude with lessons learnt from the approach we employed, offering recommendations to realist researchers planning and undertaking IPT development with vulnerable populations.
Box One: The D-PACT Project
The ‘Dementia - Person Aligned Care Team’ (DPACT) project is a five-year research programme funded by the National Institute for Health Research, seeking to develop and evaluate a complex dementia support worker intervention based in primary care, across two sites in the NW and SW of England. The five-year programme includes stages of theory-building (initial and refining), feasibility and a mixed-methods realist evaluation). This paper reports on the theory-building stage of the programme. Previous studies have demonstrated potential benefits of having a named trusted individual, based in primary care, providing continuity of proactive support (e.g. Iliffe et al., 2014; Greaves et al., 2015). This type of role exists in a variety of settings across the UK, but although highly valued, post-diagnostic support for families living with dementia at home is not available to everyone, and available support is often not well theorised or evaluated. Therefore, we took a multi-disciplinary realist informed approach to development and delivery of a Dementia Support Worker intervention, drawing on multiple sources of evidence, expertise and experience to understand what support is needed and when, how it should be delivered, and how this leads to more positive outcomes. The aim was to develop an individualised, person-centred support intervention, tackling a range of priorities for people with dementia and their carers to improve emotional and physical wellbeing. Phase 1 of D-PACT comprised:
Methods and Insights
Study Design: Programme Theory Development Overview
From the project start, there were tentative ideas about the intervention model and potential intervention components. Early on, our programme theory building was influenced by an existing person-centred complex intervention: the PARTNERS2 model of collaborative care based in GP surgeries for people with bipolar, schizophrenia or other psychoses (Gwernan-Jones et al., 2020). In turn, this model was informed by the Chronic Care Model (Wagner et al., 1996
Sources of data collection.

Following initial literature reviews, carried out by authors SG and LM, we developed a set of 21 tentative, mainly MM (Mechanism resource, Mechanism response) theory statements, using the structure ‘If x then y’ which described the causal processes we anticipated produced the intervention outcomes. Some short-term outcomes were built in, as a basis for further refinement. By the end of the prospective phase, we had further developed and refined our IPT into a set of 42 theory statements. These 42 constitute our Elaborated Programme Theory (EPT). Next, we report on the different sources we drew from, with examples of how we adapted our research processes to promote inclusion of people with dementia alongside other stakeholders, and contributions to our theory development this produced. Although we present these sources sequentially, in reality this process was not linear. Rather, it involved an iterative overlapping process of theory development, engagement with stakeholders, refinement of theory and developing new areas of theory concurrently (a process characteristic of realist evaluation). By these methods, we developed the IPT into an Elaborated Programme Theory (see Figure 1). D-PACT Timeline with corresponding Phase 1 IPT and EPT activities.
Ethics
The University of Plymouth ethics committee granted ethical approval for all non-NHS primary research activities described in this paper. South Central Berkshire Committee granted ethical approval for the overall D-PACT study (REC reference: 19/SC/0264).
Sample and Data Collection
Primary research activities are shown in Table 1: a, b and c. Manzano (2016) and R. Pawson (1996) recommend collecting data from the main actors in and observers of the intervention to inform development and refinement of CMOCs. We recruited existing dementia support workers/navigators and advisors through the Alzheimer’s Society UK; at the time the largest employer of such roles. People with dementia, carers and former carers were recruited through local non-NHS community memory cafes (see Supplementary material for details on capacity and consent procedures). Expert advisors were purposively sampled through literature searches and word of mouth. They included academics, policy makers, leaders of dementia organisations and high-profile people living with dementia identified through voluntary organisations and social media.
Given the early stage of the research, our initial interview questions were broad and exploratory, seeking to understand experiences of living with dementia and how the programme might work for different people in different circumstances. As we achieved greater depth and clarity of understanding, we were able to test out emerging theory with participants in later interviews. Audiotaped interviews and focus groups were conducted in a private space by researchers SG, LM, LW and AG, using semi-structured interview and topic guides. Researchers had extensive experience of interviewing, were trained in the fundamentals of realist methodology, and received additional training in effective communication with people with dementia.
Analysis of Primary Data
Analysis was carried out by authors SG, HW, AG and SMT. We used an analysis approach based on methodology described by Gilmore et al. (2019), coding evidence of causal associations deductively and inductively, to the initial 21 theory statements. The 21 statements were iteratively refined and expanded through analysis, researcher discussion and sense-checking (or ‘member-checking’: Lincoln & Guba, 1985) by our PPI/EFG stakeholder groups (see later in this article). Thematic analysis (Braun & Clarke, 2019) was carried out alongside the coding approach based on Gilmore et al. (2019), for its potential to develop themes on psychological and social phenomenon and help elucidate important contextual programme elements. We triangulated the two types of analysis, synthesising insights from the literature reviews and PPI/ERG engagement, to develop a more robust elaborated programme theory (EPT).
What follows is an account of methods used for engaging stakeholders in elaborating the IPT. Those with experience of living with dementia or caring for people with dementia contributed to theory development, as well as inspecting our emerging theoretical assumptions about our prospective intervention, in light of their own experiences (R. Pawson, 1996).
Approaches to Stakeholder Engagement in Realist Theory Development
a) Interviews with People with Dementia and Carers
We interviewed people with dementia individually or with carers, depending on practicalities and preferences (negotiated with participants). Involving people with dementia in the process of interviewing presented some early challenges. There are difficulties with processing and abstract thinking associated with dementia, so we had to take an unhurried approach and judge what was appropriate to ask in the moment based on our observations of people’s cognitive-communication abilities. Some questioning techniques were easier to use with field experts and practitioners, for instance, questions designed to uncover meaningful contexts, such as ‘We know that people with dementia and their circumstances vary greatly. What kinds of things do we need to take into account when developing this support role?’ usually led to responses from practitioners and field experts that could be followed up by the interviewer with further questions aiming to elicit a greater understanding of causality. People with dementia and carers were not always able to comprehend and respond directly to such explicit theory-based questions. With them, we did not focus quite so explicitly on trying to elicit new theory or gain feedback on our emerging theories. Instead, we maintained a relaxed conversational approach, asking open questions, allowing additional time, repetition and opportunities to talk ‘around’ an idea or topic area (which often elicited stories of experience). Whist attending to participants’ needs in this way, our approach was to try and uncover causal processes and meaningful contexts. Crucially, interviewers had an intimate understanding of the current developing programme theory, so could identify when ‘nuggets’ of information (Pawson 2006b) about, or gaps in, the theory came up naturally, and at those moments, ‘dig deeper’ to gain more understanding of possible causation. This was done by asking follow-up questions to elucidate causal mechanisms such ‘What was important about that?’ and ‘What was it that led to you feeling/thinking that?’, thereby gaining useful insights to inform intervention theory.
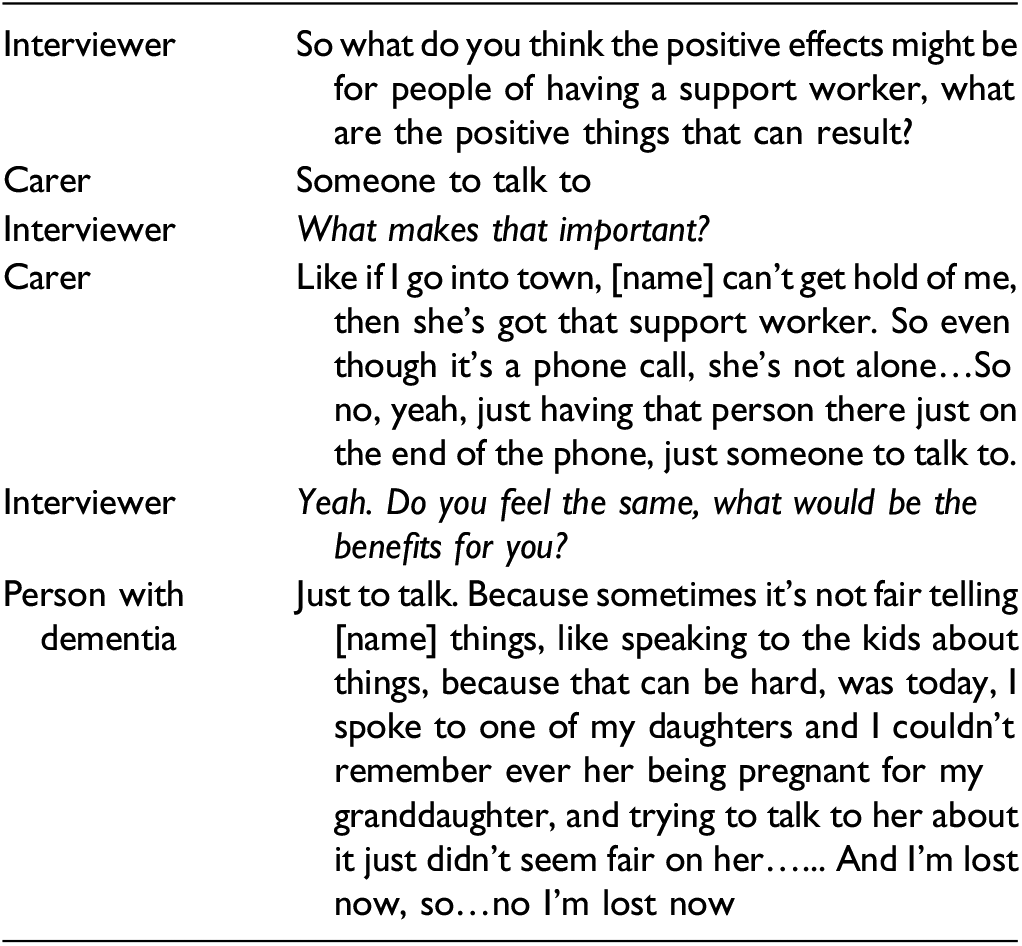
In Excerpt One, the researcher uses retroductive, probing questions, when interviewing a dyad, to uncover mechanisms from a person with dementia and their carer about why having a support worker would be valuable. Often, as communication becomes more difficult, carers become the spokesperson or representative for their relative/friend with dementia. In every-day life, this can be very helpful. However, in an interview setting, by directing a follow up question to the person with dementia, the interviewer ensures that both interviewees have an opportunity to share their perspectives. In this scenario, it was particularly valuable because the interaction revealed divergent ‘mechanism responses’.
Excerpt One
Although the person with dementia loses their thread, both interviewees are referring to an imagined resource of having someone with whom they can share concerns. However, whilst the resource is the same, the imagined responses are different. The carer talks about the reassurance they would gain from knowing the person with dementia had someone they could communicate with if they were ever away from the house; whereas the person with dementia talks about being able to discuss personal and sensitive topics without ‘unfairly’ putting this on the carer. So, whilst middle range theory (Merton, 1967) on carer burden might be used to explain one outcome of this proposed intervention, the more granular programme level theory we wished to capture, is informed by divergent, varying responses between individuals such as in this scenario.
Throughout the course of data collection and theory refinement, we noticed that, although interview questions were typically framed positively, for example, asking about the positive effects of having a DSW, responses were often not hypothetical positives. Instead, participants framed responses based on their (usually negative) experiences of how they were left feeling in the absence of the support in the past. This is illustrated in excerpt two, an interview with a person with dementia.
Excerpt Two

People with dementia may find it more difficult to think in abstract hypothetical terms. However, by giving them opportunity to describe their own real life past experiences we were still able to gather useful contextual insights about the relevance of and need for post-diagnostic support through developing an understanding around the impact of its absence. For instance, in the absence of formalised support, people living with dementia potentially have to try and find out for themselves how to cope and where to seek support, which can be difficult, and leave them feeling alone and exhausted. We used this ‘absence of’ narrative to consider how the ‘presence of’ could be hypothesised to lead to the opposite (positive) mechanisms and outcomes.
Box Two shows an example of one of the 21 initial programme theory statements before the methods of theory elaboration outlined above were applied. This relates to concepts elucidated in excerpt two regarding filling in the gaps in support. This incorporates the mechanism resource of identifying and filling the gaps in support and tailoring information to the person’s needs.
Box Two: Example from the 21 Initial Programme Theory Statements
IF the Dementia Support Worker, person with dementia and carer identify together things that are working well, information needs and opportunities that could be explored AND generate an action plan (Mechanism resource) THEN the person with dementia and carer will improve their understanding of dementia, their own situation and how support services can improve their wellbeing (Mechanism response) THEN they will engage more with services that can improve wellbeing, feel medication is less burdensome, increase self-care practices, have fewer behavioural symptoms (Short term outcome) Excerpt three (below) is from an interview with a dyad where peer support is discussed. Prior to this excerpt, the conversation was about arranging Power of Attorney. Here, the interviewer draws on experiences previously shared by the carer to try and elucidate what resources, hypothetically, might be offered to achieve a less negative response to feeling left in a void. Instead of responding entirely hypothetically, the carer then draws on the positive aspects of the limited peer support that was received, in order to respond. The interviewer then digs a little deeper using follow up questions, to further inform theories about the mechanisms underpinning peer support.
Excerpt Three
We continually reflected on transcripts of our own interviews, looking to see how we could refine our realist practice, for example, by spotting opportunities to dig deeper and expand on emerging theory.
b) Interviews with Field Experts
We conducted telephone interviews with a range of field experts. Although many of these participants had published research papers or reports on post-diagnostic support, in written work, hypotheses about causal mechanisms and how they interact with contexts to produce outcomes are not always obvious in these writings. Conversations that probe these issues are essential in realist enquiry. We found that for some field experts, we were able to be more explicit about theory in the interview. Excerpt four is from an interview with a dementia practitioner-researcher who is also a carer. The interviewer starts with a question that highlights the purpose of the interview as a quest to understand casual mechanisms.
Excerpt four

This elicits some contextual information regarding the complexity of and lack of clarity around dementia services. The interviewer digs deeper, asking a follow up question that hopes to unpick what resources might help to mitigate these challenges. The interviewee then theorises aloud about the potential for having a DSW who understands the network of services, knows what’s worth applying for and how long it will take, is honest about that, and essentially saves people a lot of disappointment and energy (that other interviewees have suggested might be best placed enjoying valuable quality time with the person they are caring for). Box Three shows an example of one of the eventual elaborated 42 programme theory statements that was influenced by these kinds of findings.
Box Three: Example from the 42 Programme Theory Statements
IF the DSW develops an understanding of the network of care and how systems work (what’s free, what costs, what’s worth applying for) (Mechanism resource) THEN they will feel that they are developing strengthening their skills knowledge and confidence in delivering the intervention and will be better able to recommend tailored support to people with dementia and carers
c) Focus Groups with Existing Support Workers/Advisors/Navigators
Manzano (2020) reports a limited use of focus groups in realist evaluations, and points to their potential in developing causal inferences. We employed a focus group methodology for support workers and advisors/navigators as it has benefits for theory-building. For instance, research participants can engage in group deliberation around their own perspectives and develop ideas/theories collectively ‘to create theory grounded in the actual experience and language of [the participants]’ (Du Bois, 1983). The methods section above explains the rationale for the focus group membership.
Excerpt Five follows on from a prior conversation about carers often feeling protective about the person they care for, and how they identify so strongly in their carer roles, they find it hard to break away and secure time for themselves. Consequently, they become close to burn out.
Excerpt Five

Participant one describes the issue as they see it: the carer might be inclined to resist opportunities for respite (context) and supporters might try to get round that by suggesting that they give it a go and see what happens (mechanism resource). The interviewer probes this further, trying to elucidate potential mechanism responses. Participant two jumps in to further expand on context, before Participant three contributes with an alternative suggestion for a resource (offering to go with the person with dementia to the new encounter) that can lead to a positive response (reassurance for the carer and agreement that this can happen).
Box Four shows another example of one of the 21 initial programme theory statements that was influenced in part by primary data collection insights, before formal analysis began. This incorporates the mechanism resource of supporting new encounters, illustrated in Excerpt five.
Box Four: Example from the 21 Initial Programme Theory Statements
IF the Dementia Support Worker sets up meetings with/makes referrals to/signposts to healthcare, social care and community resources AND offers support with new encounters (Mechanism resources) THEN the person with dementia and carer will feel more hopeful, more confident in their own abilities, allowed to do things for themselves (carers), and will start to try out new behaviours. (Mechanism responses).
Towards the end of one of our focus groups, we explained the realist approach and provided a simplified visual representation of the emerging IPT (Figure 2). Use of simplified visual representation of the emerging Intervention Programme Theory in focus groups.
We invited participants to write their thoughts and comments on this rudimentary visual representation, discussing key concepts at the same time. Their additions are shown in bold italics. We felt this was an appropriate point to introduce the theory of the intervention more explicitly as people felt comfortable expressing their views even if they were dissenting from the majority, and they could see clearly what we were trying to understand about how the intervention would take effect. Introducing the IPT later on in the focus group also avoided biasing their responses to earlier questions. Participants responded positively to this activity, adding their thoughts for instance on the scope of the role (e.g. working in partnership with other services, preventing crises throughout the dementia journey and raising awareness of dementia within the community) and the potential impact of the intervention (e.g. improving coping strategies).
d) Wider Stakeholder Involvement
Alongside early literature searches, we engaged with a Patient and Public Involvement (PPI) group and an Expert Reference Group (ERG) (see Table 1 for details). For instance, we asked these groups ‘What makes a good Dementia Support Worker?’ and combined their insights with evidence gathered from literature on DSW skills, background and attributes, to build implementation theory. The PPI and ERG contributors all felt that while some DSWs may come from a health/clinical background, a range of backgrounds should be considered for the D-PACT DSW role, including those with some social science or community working experience. In terms of attributes, they all felt DSWs should be non-judgemental, genuinely interested in people, friendly, caring, smiley, discrete, able to stay calm, not too official, and able to take a conversational and unhurried approach. The ERG group added that the DSW should have a kind of presence or ‘glow’ about them – a warmth that is evident as soon as you meet them, and also that they should be self-aware; able to reflect deeply on practice.
In terms of knowledge, both groups felt that prior knowledge of dementia, understanding of behaviour of individuals with dementia, skills in interacting with people with dementia and families, competence providing education/facilitation and giving information to people with dementia and families were all vital. However, they acknowledged all the knowledge necessary for the job will not be present from the start. These opinions coincided with recommendations from literature on the importance for DSWs engaging in educational programmes, reading, and attendance at network meetings with other people doing similar work (Iliffe et al., 2014) and influenced our theory building on how training should be implemented. For instance, mechanism resources of continuous learning opportunities and support with critical reflection were built into our analytic statements.
Concurrently with the literature review and interviews with people with dementia and carers, we discussed our developing IPT with a PPI group. We explored how these stakeholders felt the intervention programme should work, and contextual circumstances that may impact individuals' responses to the intervention and thus its effectiveness. Later discussions informed further theory refinement, thus leading to the more rounded, elaborated programme theory.
At the beginning of each PPI meeting, as part of a research ‘update’ we used visual reminders of the intervention-in-development to talk through and engage group members, re-orient them to the process and elicit new responses. This took the form of a photograph of a generic support worker, talking with a dyad, and clear written key word/phrase reminders of the main aims and strategies of the intervention, updated when new decisions had been made (with them) about what might work best. Taking this visual approach, reduced verbal and written language complexity, providing them with time and space to continue looking over the images for as long as they needed. Updating them on decisions clearly demonstrated to them that their contributions over time were meaningful, that is, they were feeding into the gradual development of the intervention.
PPI activity – Elucidating potential coaching approach mechanisms.

This exercise helped us gain additional perspectives, enriched by people with lived experience sharing their thoughts with each other to make collective sense of them (as opposed to individual interviews). Their insights added depth to our hypothesised mechanisms, adding detail to the range of potential resources and potential behavioural and psychological responses (See box Five, Statements One and Two).
Thematic analysis of the interviews and focus groups revealed important inter-related contextual factors regarding individuals’ characteristics and circumstances that we would need to consider in developing the intervention. The analysis highlighted how people with dementia and carers experience constant shifts in terms of their acceptance of their new life with dementia and adaptation over time. Feelings of control, social connectedness, hope and trust in others, wax and wane over time, influenced by the nature and progression of the dementia, their often disappointing experiences of support services, and
We took these findings to both the PPI and Expert Reference Groups, as a method of sense-checking whether our initial analysis resonated with lived/practice experience, thus avoiding potential burden of asking original participants to check our findings. We discussed with these groups how the floating contexts might map onto mechanisms. For example, we asked
PPI contributors also felt it would be important for the DSW to check whether agreed actions by health and social care services had been followed up, and take responsibility for chasing unactioned tasks, thus taking pressure off the carer to have to do so. Another way it was felt DSWs could combat cynicism (thereby mitigating the context of previous inadequate support) was to be mindful of any barriers to engagement in community assets relating to practical hurdles such as transport, finances and mobility and psychosocial issues, including embarrassment and anxiety. The resource offer should include active problem solving around these barriers as far as is realistic and practical. This goes beyond some existing models of dementia support, which focus mainly on signposting people to sources of information and help. This led to the importance of DSWs problem-solving and advocating around barriers to engagement becoming an integral part of the programme theory, as shown in Box Five, Statement Three.
Box Five: Examples from 42 programme Theory Statements, Informed by Wider Stakeholder Involvement
Statement One: IF the DSW adopts an unhurried and FLEXIBLE COACHING APPROACH (provides opportunities for the person with dementia and carer to take the lead in exploring what matters to them from their individual perspectives/is non-judgemental/resists providing all the answers/provides bits of simple practical advice where wanted) (Mechanism resources), THEN the person with dementia and carer will feel important/cared for/listened to/like they are part of an equal partnership with the DSW AND will be more likely to disclose what matters to them (Mechanism responses). Statement Two: IF the DSW supports conversations about forward planning (creating space to discuss the future, responding to readiness and revisiting as appropriate; planting the seed and building on each prior discussion) (Mechanism resources), THEN person with dementia and carer will start to open up/talk about what they want to happen in the future (Mechanism response). Statement Three: IF the DSW identifies and makes use of all resources to support achievement of actions (sets up meetings with/shares plan with/makes referrals to, signposts to healthcare, social care and community assets; supports person with new encounters; problem-solves barriers to engagement, e.g. transport) (Mechanism Resources) THEN, the person with dementia and carer – especially where they have been let down previously (Context)
We have shown the various ways we engaged with people living with dementia, carers and field experts, to inform iterative programme theory development. This involved combining primary research findings with evidence from literature and discussions with stakeholders, to develop a theory of how a Dementia Support Worker intervention might work/not work, for whom, how and in what circumstances. At the end of the prospective phase of the study, we had refined our initial programme theory, into an elaborated programme theory expressed in 42 CMMO style statements, as well as a practitioner manual and accompanying training. Engagement of stakeholders has enabled us to prepare for the feasibility phase, where our prototype intervention will be tested in practice. The theory will be further refined and consolidated through these next stages of the study.
Discussion
We have demonstrated how thoughtful engagement with stakeholders, including people with dementia, led to vital insights that informed the development of our programme theory in meaningful and significant ways. Together, the different groups provided multiple means to examine complex process and the mechanisms in operation, so refine and develop an initial programme theory into an elaborated programme theory. Encouraging stakeholders to engage in realist thinking required us to adapt our approach depending on the stakeholder group. As shown in Excerpt 4, we were able to use realist terminology such as ‘mechanisms’ with some field experts, as well as explicitly revealing to them parts of our IPT for inspection. With people with dementia and carers, we less explicitly elicited theory but were alert to opportunities, within an open and relaxed approach, to dig deeper and identify potential causal mechanisms. We also used visual methods, both pictorial and written, to support focus groups and PPI discussions. For people with dementia in particular, visual resources provided an aid to comprehension and recall. At any time in the conversations, there was a reminder of the topic and how the discussion was unfolding, allowing people to find their place in the discussion again if they became confused.
These adaptations enabled stakeholders to provide essential contributions to our elaborated programme theory for the intervention, providing a theoretical as well as ethical justification for involving the very groups of people intended to deliver and benefit from the intervention. Many of the stakeholders told us they had enjoyed taking part in the process and felt they were contributing to making a difference. This resonates with studies examining the empowering benefits for vulnerable groups of engaging in PPI (e.g. Bailey et al., 2015), which can lead to feelings of increased confidence and self-esteem; people often feel they have gained new skills and access to decision making.
We found focus group methodology could be used to good effect in realist enquiry. In our groups, Dementia Support Workers/Advisors/Navigators were articulate and interactive contributors, able to engage in free-flowing discussions, exploring divergence and commonality with only light touch researcher facilitation. Not all the members had met before, so the groups did not have preconceived views about the points being discussed. That can be an advantage because where there are no ‘taken for granted’ implicit shared meanings, participants are not able to reinforce these through the focus group discussions. Instead, they may be more open to exploring new ideas together (Flick, 2018). Being based in various settings, with differing policies and practice guidelines, their discussions led to deeper understandings of contextual influences.
However, the realist interviewer/facilitator role presents different challenges compared to individual interviews. In our case, the discussions were energetic, so facilitators needed to be agile in applying what they were hearing to the emerging programme theory, spotting moments where drilling deeper could lead to theory refinement and taking those opportunities before the conversation had moved on. There were moments where participants would do this work, questioning each other’s contributions and through debate, arriving at a more nuanced aspect of programme theory. Also, adept facilitators can track back to earlier moments and ask questions to encourage deeper thinking around causality, for example, ‘Earlier you mentioned x. I’m interested to hear more about why you think that is the case…what does x lead to?’.
Reflecting on our use of a tool to support realist thinking (see Figure 1), this worked well and may have introduced bias if we had presented it earlier in the focus group. However, we felt that we could have spent longer on this task given that participants engaged in this so enthusiastically. In future studies, we would allow more time for this activity to fully reap the benefits of a group that had established rapport and started to grasp the idea of realist enquiry. We would also consider explaining realist approaches in lay terms, as part of explaining the purpose of the particular method of data collection, depending on the particular participant group. Especially in a focus group, if participants have more of an idea of realist interviewing approaches, they may start to question each other in order to uncover casual links, thus revealing greater depth of understanding of contextually-contingent mechanism activation.
As we saw real potential for practitioners in this field to become effective realist thinkers, we explored this in our practitioner training. The application of realist evaluation does not have to rest purely with external evaluators. Practitioners can become realist evaluators, by reflecting on and learning to recognise mechanisms in action. This in turn enables them to adapt intervention components/mechanism resources in response to new emerging contexts; an idea proposed by Harris (2018).
It was necessary to interview most participants with dementia together with a participating carer, for practical and preference reasons. This could have been a limitation; in dyad interviews, participants may have been less able to speak openly about their experiences and thoughts. On the other hand, carers typically provided vital communication support for people with dementia, enabling involvement for those who might otherwise have not been able to participate. Interviewing dyads also allowed for discussion between the pair, through which they were able to hear and respond to each other’s perspectives, thereby stimulating new insights. This helps uncover more detail about mechanisms and how they may operate for each type of participant.
A more clear-cut limitation was the challenge of retaining a core group of people with dementia and carers as PPI contributors, due to the progressive nature of dementia and people finding it increasingly difficult to contribute, and people sadly passing away. This work has necessitated constant efforts from researchers to seek opportunities for group expansion and increased diversity within the group. This is a time-consuming endeavour and one which should be considered in research funding applications.
Overall, we have been flexible in our approach to involving stakeholders and are developing a fundamentally person-centred approach to dementia support built on this early work. In this article, we have provided practical examples that will be beneficial to other researchers developing realist programme theory, particularly for dementia interventions. Given the limited available guidance in this area, we highly recommend a greater sharing of such experiences, leading to the development of detailed methodological guidance. This will support researchers to rigorously develop and refine IPT, in collaboration with the underrepresented populations they seek to support, with clear application of realist principles.
Supplemental Material
sj-pdf-1-ijq-10.1177_16094069221077521 – Supplemental Material for Engaging Stakeholders in Realist Programme Theory Building: Insights from the Prospective Phase of a Primary Care Dementia Support Study
Supplemental Material, sj-pdf-1-ijq-10.1177_16094069221077521 for Engaging Stakeholders in Realist Programme Theory Building: Insights from the Prospective Phase of a Primary Care Dementia Support Study by S. Griffiths, L. Weston, S. Morgan-Trimmer, H. Wheat, A. Gude, L. Manger, T. M. Oh, P. Clarkson, C. Quinn, R. Sheaff, M. Clark, I. Sherriff, and R. Byng in International Journal of Qualitative Methods
Footnotes
Acknowledgments
We would like to thank Ms Caroline Sutcliffe and Dr. Karen Davies, University of Manchester, for their early involvement in data collection for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the National Institute for Health Research (NIHR) Programme Grants for Applied Research (RP-PG-0217–20004). This report is independent research supported by the National Institute for Health Research Applied Research Collaboration Southwest Peninsula. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.