
Abstract
Increasingly, social life—and accordingly, social research—is conducted in online environments. Asynchronous online focus groups (AOFGs) have emerged as an important tool to conduct remote research with geographically diverse populations. However, there remain few systematic accounts of AOFG methods to guide researchers’ decision-making in designing and implementing studies. This paper seeks to address this gap by describing a recent study on body image and health among transgender and gender diverse (TGD) young adults. In this study, eight AOFGs were conducted in August-October 2019 with 66 TGD young adults residing in 25 U.S. states. Each AOFG lasted four consecutive days with two prompts posted by moderators per day. Overall, participant satisfaction with AOFGs was high: 98% reported their experience was excellent, very good, or good and 95% would be somewhat or very likely to sign up for another AOFG. This example is used to illustrate key methodological decision-points, acceptability of the method to participants, and lessons learned. The goal of this paper is to encourage other researchers, particularly health researchers, to consider using AOFGs and to engage with the method’s strengths and limitations in order to develop new opportunities for online technologies to enrich the field of qualitative health research.
Keywords
Introduction
An increasing portion of social life is conducted in online environments and health research has followed suit, adapting online technologies for a range of research methodologies. This includes the adaptation of traditional in-person qualitative focus group methods to online environments (Rivaz et al., 2019). The direct technology-mediated analog of in-person focus groups is the synchronous online focus group (i.e., using phone, video conference, or group-chat technology to convene a group of participants and moderate a focused discussion in real-time) (Fox et al., 2007; Tuttas, 2015). However, a distinct technology-mediated focus group method has also emerged in recent years, one which confers a unique set of opportunities and challenges: the asynchronous online focus group (AOFG). An AOFG is a dynamic digital bulletin board method that takes place over a set number of consecutive days—typically 3 or 4, but in some cases for longer periods, such as 30 days (Zwaanswijk & van Dulmen, 2014). AOFGs can occur using a range of potential platforms, from paid subscription services (such as that described below) to freely available social media platforms such as Facebook groups (Biedermann, 2018). The study moderator(s) post discussion prompts one or more times per day, and participants can respond at their convenience—any time of the day or night—until the focus group closes.
While this method offered promise prior to the era of the novel coronavirus global pandemic (COVID-19), this global crisis has necessitated a paradigm shift in social and health research that has led to more widespread interest in “remote” and online research methods (Saberi, 2020). Yet even when pandemic-related physical distancing measures are no longer required, given the growing role of digital media, telehealth, and online communication in social life and healthcare, there will remain a need for online research tools like AOFGs that enhance researchers’ ability to conduct high-quality, remote social and health research.
In the early 2000s, a distinction was made between email-based and web-based AOFGs; at that time, web-based platforms were perceived as more confusing to participants (K. Stewart & Williams, 2005). However, web-based technologies have evolved dramatically since then and the ubiquity of social media in the current social landscape (as of 2019, 90% of young adults and 72% of all U.S. adults used social media) means that many users are now well-versed in the use of web-based discussion platforms (Pew Research Center, 2019). For some research projects, AOFGs may be an accessible, cost-effective, and powerful tool.
In order to determine whether an asynchronous or synchronous method is more suitable for a given research question, researchers must make a key decision about what Stewart and Williams refer to as “the temporal divide”: that is, they must decide whether it will be best for their research questions and goals to conduct discussions in real-time (synchronous) or not (asynchronous) (K. Stewart & Williams, 2005, p. 403). To make this decision, researchers need to consider the array of strengths and limitations of each approach. These strengths and limitations should be considered in the context of longstanding debates regarding traditional focus group methods, such as the goal of the method (i.e., a focus on researcher-participant interaction vs. between-participant interaction) and the unit of analysis (group vs. individual) (Kitzinger, 1995; Parker & Tritter, 2006; Smithson, 2000). A growing body of research documents the utility of synchronous online focus groups, including their ability to foster meaningful participant interaction and generate rich data on individual experiences and group processes, similar to traditional focus groups, while also conferring unique strengths such as convenience and geographic reach (Brüggen & Willems, 2009; Gratton & O’Donnell, 2011; Lally et al., 2018; Lobe, 2017; Tuttas, 2015; Wirtz et al., 2019). However, there remains scarce information to guide researchers interested in asynchronous methods.
That said, a growing number of studies using AOFGs highlight several strengths of the method (Williams et al., 2012). Chief among these strengths is the convenience of allowing participants to answer in their own time (Boateng et al., 2016; Zwaanswijk & van Dulmen, 2014). This enables participants with irregular work schedules or family responsibilities to participate in research that might otherwise not be feasible for them. Second, some recent studies have demonstrated the strength of AOFGs for addressing sensitive topics, especially those related to health, healthcare, or stigma, possibly due to the anonymous or identity-masked format, which can increase participant comfort with sharing sensitive information (Reisner et al., 2018; Ybarra et al., 2019). AOFGs have also been shown to enhance participants’ feelings of anonymity and safety, as well as sense of agency in participating (e.g., being able to choose their own name/online “handle” and thus how they are represented in research) (Wirtz et al., 2019). Third, the asynchronous online modality may be particularly suitable for some study populations, such as those in younger and middle age cohorts in Western contexts, who have been immersed in interactive media platforms (e.g., Facebook/Instagram, Twitter) for much of their lives. AOFG interfaces are typically akin to a social media platform’s asynchronous discussion tool (e.g., “feed”), increasing familiarity and usability for these populations (Boateng et al., 2016; Zwaanswijk & van Dulmen, 2014).
Fourth, there is some indication that AOFGs could alleviate some of the barriers that have been identified in synchronous online or in-person focus groups, such as overly-dominating group members (Smithson, 2000), by offering space for those who may require or wish for more time to come up with a response (Doull et al., 2018; Reisner et al., 2018; Ybarra et al., 2019) and allowing users to have a public “side conversation” that is not disruptive (Biedermann, 2018). However, there is a need for more research in this area. Finally, and related to the strengths noted above, AOFGs have been successful for connecting with geographically dispersed or otherwise “hard-to-reach” populations—including stigmatized populations, people with irregular schedules, those living in rural areas, caregivers of those who are ill who would require someone to arrange coverage for their duties, and people who have complex medical needs (Boateng et al., 2016; Cook et al., 2016; Doull et al., 2018; Earnshaw et al., 2020; Fisher et al., 2016; Fontenot et al., 2020; Huis In Het Veld et al., 2018; Reisner et al., 2018; Ybarra et al., 2019).
Although use of AOFGs is becoming more widespread in both market research and social sciences (D. W. Stewart & Shamdasani, 2017; Reisner et al., 2018; Woodyatt et al., 2016), there remain few systematic accounts of the method, its acceptability with participants, or key decision-points in determining whether and how to implement AOFGs, particularly for health research. This paper seeks to address this gap by using a case study to identify strengths and limitations of AOFGs in relation to longstanding dilemmas in the field of focus group research, such as managing participant engagement, the role of the moderator and between-participant interaction, and sampling and ethical challenges (Parker & Tritter, 2006; Williams et al., 2012).
Specifically, we present the AOFG method used for a recent study focused on body image and health among U.S. transgender and gender diverse (TGD) young adults. TGD people have a gender identity or expression that differs from their sex assigned at birth. This historically marginalized population faces severe health inequities in multiple domains, including two to four times greater risk of eating disorder symptoms as compared to their cisgender (i.e., non-transgender) peers (G. R. Brown & Jones, 2016; Diemer et al., 2015). We use this example to illustrate key methodological decision-points, feasibility, and acceptability of the method, as well as lessons learned about challenges and opportunities of AOFGs. Our goal is to encourage other researchers, particularly health researchers, to consider using AOFGs when relevant to their research question and a good fit for their study population. We also encourage researchers to engage with the strengths and limitations of AOFGs in order to improve the method and keep developing new opportunities for online technologies to enrich the field of qualitative health research.
AOFG Case Study: The BRIGHT Project
Study Background and Purpose
The Body Image and Resilience Study to Improve Gender Inclusive Health Interventions for Trans Communities (BRIGHT) was designed to inform the development of eating disorder preventive interventions for TGD young adults. Despite mounting evidence that TGD young people experience heightened risk of eating disorder symptoms and disordered eating behaviors (G. R. Brown & Jones, 2016; Diemer et al., 2015; Guss et al., 2017), and despite the existence of evidence-based interventions shown to reduce eating disorders risk factors in cisgender young women (Becker & Stice, 2017) and cisgender gay and bisexual young men (T. A. Brown & Keel, 2015), no evidence-based interventions have been adapted or tested to address the unique needs of TGD young people. Further, few studies have examined the role of intersecting social identities (e.g., gender identity, race/ethnicity) and social stressors (e.g., stigma, discrimination) in eating disorders risk factors among TGD young people. The BRIGHT Project sought to address these gaps with a goal of informing future intervention development to reduce health inequities in this marginalized population.
Rationale for Selecting AOFG Method
We utilized AOFGs to gather opinions, ideas, and experiences of diverse TGD young people. We elected to use a focus group methodology in general because “group processes [in focus groups] can help people explore and clarify their views in ways that would be less easily accessible in a one to one interview” (Kitzinger, 1995, p. 299). In particular, we sought to create a space for groups of TGD young people to individually and collectively explore and describe their shared and divergent experiences related to their social identities and eating disorder risk factors such as exposure to social stressors and body image-related pressures from peers and media.
We specifically chose to use focus groups that were asynchronous and online for three primary reasons, all related to our goal of increasing accessibility of the study to those often under-represented in TGD health research. First, we sought to maximize geographic diversity, given that much research on TGD populations has relied on samples drawn from major metropolitan areas and/or coastal regions. AOFGs allow participants to access the study from any time zone in any region. Second, we sought to maximize socioeconomic, racial/ethnic, and gender diversity and anticipated that the scheduling flexibility and convenience could enhance participation of young people who worked multiple jobs, balanced school and work, or had other nontraditional schedules. Third, AOFGs were selected for their potential to reach TGD young people who, due to stigmatization of TGD populations, might not be able to feel comfortable or safe talking out loud about their identities or other sensitive topics (as might be necessitated by a synchronous, video conference-based focus group) (Reisner et al., 2020). AOFGs can enhance feelings of safety and anonymity because participants do not have to speak aloud, and they can participate on their own timeline and when they are in a confidential environment.
Methods
Recruitment
Participants were eligible to participate if they were 18–30 years old, lived in the United States, were conversant in English, and identified as transgender, non-binary, or another gender different than their sex assigned at birth. Participants also needed to have access to a device that could connect to the internet. A multi-pronged purposive sampling strategy was used in collaboration with the community partner organization involved in this research (Trans Folx Fighting Eating Disorders [T-FFED]). This included social media posts, posting digital flyers to listservs and online forums, email outreach to community contacts, and chain-referral sampling.
Screening and Enrollment
Interested participants contacted the study team and completed a brief phone screening. Given the study’s particular interest in eating disorders risk factors and prevention strategies at the intersection of gender identity and race/ethnicity, participants were given the option to indicate their preference for group composition: a group with participants of their same gender identity, a group for people of color (POC), a non-identity-specific group, or no preference. Groups were then scheduled based on participants’ preferences and availability. Once a group was scheduled, participants were emailed an informed consent form followed by a brief (10-minute) pre-focus group online survey to collect standardized measures relevant to our research question (e.g., eating disorder symptoms, body image scales), and were provided with instructions to register for the AOFG platform. Overall, our team screened 108 potential enrollees, enrolled 71 in the study, and had 66 participants take part in an AOFG (Figure 1).

Asynchronous online focus group screening and enrollment of transgender and gender diverse young adults (August–October 2019). Note: All 68 participants who created a focus group platform log-in were invited to participate in a feedback survey following the final day of focus groups; 43 completed (63%).
Participant Characteristics
The multi-pronged recruitment strategy led to the successful enrollment of a demographically heterogeneous sample. By design, the sample was roughly one-third transgender women (29%), transgender men (29%), and non-binary people (39%); an additional 3% reported another gender identity (e.g., agender). Our goal was a sample that was at least 50% POC; though we approached this goal, we fell slightly short (44%). Over half the sample identified as White (56%), followed by Multiracial (18%), Latinx (12%), Asian (8%), Black (3%), and another race/ethnicity (3%). Participants lived in 25 U.S. states (Figure 2).

Distribution of asynchronous online focus group participants by U.S. state (n = 66 transgender and gender diverse young adult participants in 25 states).
AOFG Design and Procedures
We conducted eight AOFGs August–October 2019 (n = 66 participants). We used a subscription-based, secure online platform (http://Discourse.org) to conduct AOFGs. Group size ranged from five to 11 participants. Following procedures from previous studies (Reisner et al., 2018), each focus group took place over four consecutive days. Two sets of “prompts” (consisting of one to four questions) were posted per day, one in the morning, one in the afternoon/evening (recognizing differences by time zone). Participants could respond to the prompts or other participants’ posts at any time during the AOFG. Focus group participation was made anonymous through implementation of an anonymous username during registration to the platform. To give participants a feeling of control over their self-identification in the AOFG and set a welcoming tone, participants created their own anonymous usernames following specific study guidelines (username = participant-selected favorite color + favorite animal + study-generated unique ID number; e.g., BlueWombat000).
Two trained, Master’s degree-level moderators facilitated each focus group, which included: setting a welcoming tone for the group with brief introductions by moderators and participants, posting prompts, asking follow-up probes, and encouraging engagement. Participants were informed in advance that all posts would be reviewed before being posted to ensure safety and privacy (see Safety Plan, below). Moderators worked to approve each post in real-time by taking shifts throughout the day (8 am–8 pm U.S. Eastern Time). The study coordinator sent a reminder email to all participants each morning to alert them when the first prompt was posted. Throughout the AOFG period, participants could reach the study coordinator by phone, email, or text message with problems or questions.
Following the fourth (last) day of prompts, the moderators posted a final prompt asking participants to share any additional thoughts. The AOFG was then left “open” for 24 hours to allow participants to finish responding. Following this, the group was closed and participants’ accounts and access to the platform was terminated. The day after the focus group completed participants were sent a thank you email, resource list, information about how to receive their electronic gift card for participation, and a link to a brief participant feedback survey for process evaluation purposes. The feedback survey included closed-ended questions about study burden (amount of time spent), satisfaction, and digital platform used, as well as three open-ended questions about what worked well, areas to improve, and other feedback.
Participant Remuneration
All participants who completed the informed consent form and pre-focus group survey received a $25 e-gift card for their time, even if they did not end up posting on the AOFG message board. Following procedures used in previous AOFGs (Reisner et al., 2018), participants who posted at least once per day on 3 out of the 4 days of the focus group received an additional $25 (total remuneration: up to $50).
AOFG Guide
We developed a structured focus group guide (i.e., list of prompts) based on key research questions and review of the scientific literature, similar to traditional focus group guides but adapted to be administered over 4 days with limited opportunity for follow-up probing (see Table 1 for excerpt). The initial guide was developed by the core study team (PI and moderators) and then iteratively revised in collaboration with T-FFED and a clinical psychologist with expertise in adolescent/young adult populations. Topic areas included appearance pressures and sources from within and outside TGD communities, use of social media and dating apps and impact on body image concerns, social stressors, coping strategies, and recommendations for eating disorders prevention programs. In addition, for the POC groups, one section of the focus group guide was developed specifically to address research questions related to the intersection of appearance pressures within the context of racial/ethnic identity and racism.
Selection From Focus Group Guide for Asynchronous Online Focus Groups With Transgender and Gender Diverse Young Adults.

In addition to more traditional focus group questions, the online and asynchronous aspects of this method permitted new possibilities for focus group activities. Two different digital activities were implemented, described briefly below.
Social Identity Mapping Activity. As part of the Day 1 prompts, participants were provided with a blank “social identity wheel” adapted from an existing tool used in social justice trainings (University of Michigan, n.d.). Participants were asked to “fill in the wheel” with any identities that were significant to them using whatever technology they chose (including hard copy). Figure 3 provides an example. Participants were then asked to indicate (a) the identities with the greatest effect on how they feel about their appearance and/or body and (b) the identities with the greatest effect on how others perceive them. Participants were asked to post a picture of their wheel to the focus group platform (optional) and to elaborate on why they selected the identities they chose or why they did not select any. Most participants chose to post their map for the full group to see.
Digital Image Board Activity. On Day 2, participants were asked to use an interactive online “whiteboard” tool (www.webwhiteboard.com) to curate text, photographs, drawings or other images depicting and narrating some of the appearance-related messages they experience online or in other parts of life (Figure 4). Participants could choose to post their image onto the focus group platform, or to share privately with the moderators; most chose to post to the full group. Participants were asked to post in the AOFG discussion thread about the images/text they curated and their personal significance or meaning.

Example image from social identity mapping activity in asynchronous online focus groups with transgender and gender diverse young adults.

Example from digital image board activity in asynchronous online focus groups with transgender and gender diverse young adults.
Safety Planning
A safety plan was developed in consultation with a clinical psychologist and other researchers specializing in online methods with marginalized youth. Moderators reviewed each participant response before posting. If a participant expressed a safety concern (e.g., suicidality, self-harm) the assigned moderator consulted with the study team (PI, fellow moderators, and study psychologist, as needed) to provide the appropriate level of response to the safety issue and/or editing of the text if needed. Because participants were anonymous and remote, participants were informed during the consent process that the study steam would not be able to offer in-person or phone-based support. The safety plan included text templates that moderators would, when deemed appropriate by the study psychologist, use to reach out to participants via direct message within the AOFG platform; these messages conveyed the study team’s interest in the participant’s health and wellbeing and offered a list of relevant resources, including 24-hour crisis support lines. If a participant’s post included potentially identifiable information (e.g., a name), a moderator contacted the participant and requested they edit the post to remove the identifying information or requested permission to modify it on the participant’s behalf (to reduce participant burden). Safety concerns were minimal throughout all eight groups. The vast majority of posts were approved immediately.
Human Subjects Protections
Study procedures were approved by the Boston Children’s Hospital (BCH) Institutional Review Board and use of the online focus group platform was approved by the BCH Clinical Research Informatics Team.
Process Evaluation and Lessons Learned
We first present participants’ self-reported acceptability, overall satisfaction with the AOFG method, and digital platform preferences. We then reflect on four lessons learned through this pilot study, each touching on a core aspect of focus group design (participant engagement, between-participant interaction, sample considerations, and ethical considerations) and shedding light on challenges and opportunities afforded by this innovative qualitative method.
AOFG Acceptability and Participant Satisfaction
Following the conclusion of each focus group, the study team sent focus group participants a brief anonymous feedback survey (13 items). Overall, 42 participants (64% of all focus group participants) completed the survey. Because the surveys were anonymous we are unable to identify differences between participants who responded and those who did not. The AOFG method was generally acceptable to participants, with three-quarters (74%) of respondents reporting the AOFG digital platform was somewhat or very easy to use, and 98% reporting their experience in the group was good, very good, or excellent. In addition, 95% said they would be somewhat or very likely to participate in another such focus group and 98% said they would be somewhat or very likely to recommend the study to a friend. In regards to study design, 81% of participants felt the focus group length of 4 days was the right number of days, and 81% felt the group was the right size (group size in this study: five to 12 participants).
Participant-reported strengths
Participants provided qualitative feedback on their overall satisfaction with the study experience (see Table 2). For example, one participant reflected “It was a very good, reflective, and open research project…[the] format seemed to suit the study participants needs/comfort.” Other participants reported they enjoyed using the platform and noted strengths of the AOFG method (e.g., anonymity, convenience). Several participants described enjoying the way the interface allowed them to interact with other participants in the study (e.g., being able to read other people’s responses); some specifically appreciated talking with other participants with shared identities (e.g., “being in groups of similar people was great”). A few participants reflected on their positive experience within the AOFG during the course of the focus group itself, that is, by posting about the experience on the discussion board. For example, one participant posted to their group: “Sidenote: this group has been really awesome. And I am so thankful that I could read about everyone’s experiences <heart emoji>. Thanks for sharing.”
Participant-Reported Strengths of Asynchronous Online Focus Group (AOFG) Study of Eating Disorders Prevention Needs for Transgender and Gender Diverse Young Adults.

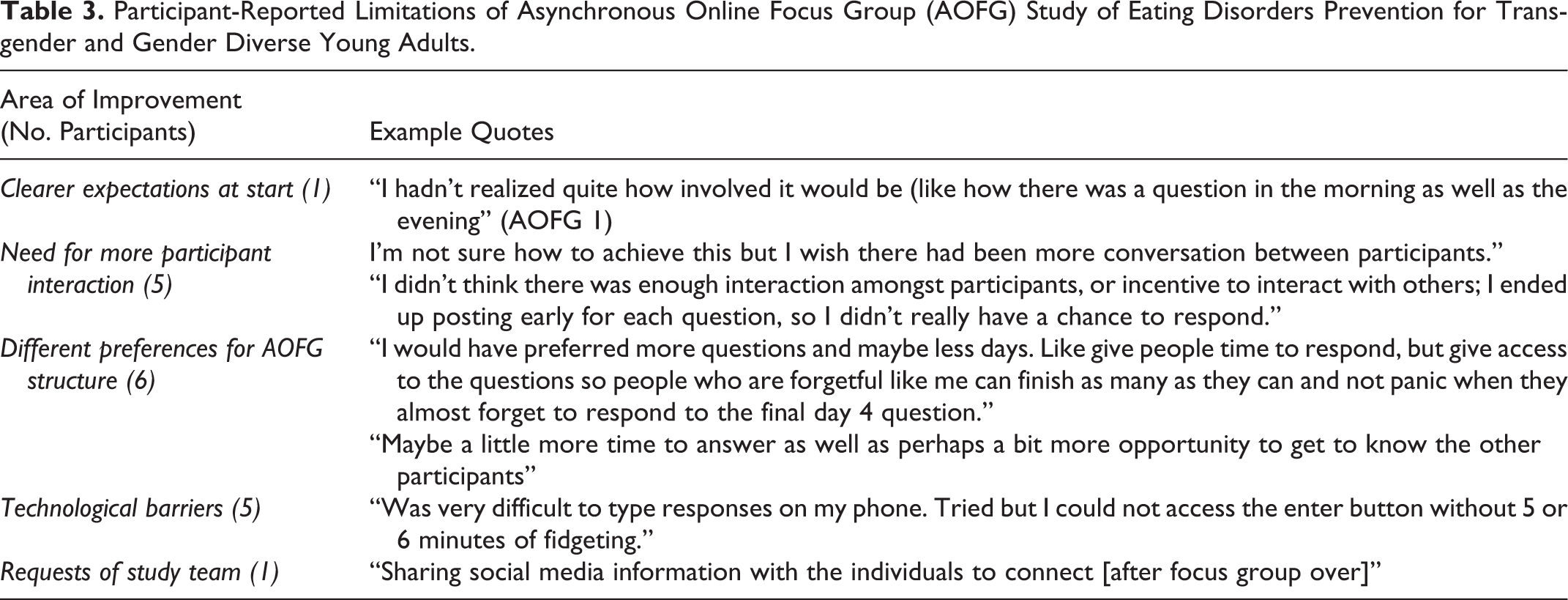
Participant-reported limitations
Participants also identified several areas for improvement (see Table 3), including technological barriers experienced by a minority of participants. Although only a few participants in this study noted technological barriers, this is a critical point as this remains a chief limitation of the AOFG method. Where possible, we adjusted study protocols to address challenges as they emerged, including improving phone screening procedures to clarify the study process and changing moderation techniques (see Lesson Learned #1). In addition, several participants desired more interaction among participants; this is discussed in more depth in Lesson Learned #2.
Participant-Reported Limitations of Asynchronous Online Focus Group (AOFG) Study of Eating Disorders Prevention for Transgender and Gender Diverse Young Adults.
Preferred Digital Platform Modality
Midway through fielding the focus groups, the team added an item to the feedback survey regarding participants’ choice of device for engaging with the AOFG. Approximately half of survey respondents received this question (n = 22). Of those, participants were split in how they engaged with the AOFG digital platform: 41% reported using only a computer/laptop, 41% reported using both a computer/laptop and mobile phone, and 18% reported using only a mobile phone to access the AOFG platform. No participants reported using a tablet.
Lesson Learned #1: Participant Engagement Strategies and Trade-Offs
Strengths
A key consideration for any focus group is the use of effective moderation techniques to engage all participants and ensure multiple perspectives are heard (Ruff et al., 2005). A concern with AOFGs is that participants may be less responsive or may drop out of the study prematurely due to lack of in-person connection. The participants in our study displayed high levels of engagement and responsiveness to the prompts over all 4 days of the AOFG. For the final prompt on the last day, 75% of the participants responded when we might have predicted an even more precipitous drop-off. Figure 5 shows the high proportion of participants responding across each day and each prompt. Further, out of eight prompts total to which participants could respond, 80% of focus group participants responded to six or more prompts, with 9% of the participants responding to three to five prompts, and 11% of participants responding to less than three prompts.
Techniques we implemented to achieve these relatively high levels of participation included: asking participants to post a brief introduction at the start of the AOFG period and modeling a welcoming tone with moderator self-introductions, a daily email, and having moderators respond to every single post with a brief affirming comment or follow-up probe, to demonstrate the study team’s appreciation and engagement. These techniques generally appeared to be well received (see Table 2).
Challenges
Although we were pleased with participant engagement, there are some drawbacks to using this method, including less opportunity for the study team to ask meaningful follow-up questions (probes) than one might have if moderating a synchronous focus group. While more in-depth probes are feasible (i.e., it is simple for moderators to post follow-up questions and create new sub-threads), our study team chose to minimize participant burden and reduce risk of overwhelming participants with multiple follow up probes, which a participant might only see when they log in to view the next core questions. Optimal balancing of participant burden with in-depth probing should be explored in future research.
Additional considerations
Prior research on optimal AOFG size for participant engagement is mixed, some suggesting that larger asynchronous groups will be more responsive over a longer period of time (K. Stewart & Williams, 2005), while other work suggests mid-sized groups (10–13 participants) may be optimal with regard to both feasibility and participant responsiveness (Hatten, 2014). In contrast, we observed that smaller groups seemed more engaged than larger groups. Overall participation levels in larger compared to smaller groups (Figure 5), while too small for statistical inference, suggest there may be benefits to smaller group sizes for participant engagement.

Asynchronous online focus group (AOFG) engagement: Percent of participants responding by prompt. Note: Smaller AOFGs (4) = 5–7 participants; larger AOFGs (4) = 8–11 participants. Two prompts were posted per day over 4 days, one in the morning (AM) and one in the afternoon/evening (PM). There was one introductory/welcome prompt (“Intros”).
Lesson Learned #2: Wide Variation in Between-Participant Interaction
Observing group dynamics and between-participant interaction is a central goal of many researchers who choose focus group methods (Kitzinger, 1995; Wilkinson, 1998), although this remains a contested area (Parker & Tritter, 2006). Our study team observed that levels of between-participant interaction varied widely by group.
Strengths
Some groups qualitatively appeared to connect or “click” with each other more than others, spontaneously offering each other support and affirmation on the discussion board. Similar to the patterns noted above with regard to group size, our team observed that some of the smaller AOFGs appeared to demonstrate a greater sense of cohesion and between-participant interaction. This included one case where a participant in a smaller group for transgender women (n = 5) noted in their feedback survey that they wished the study team could share “social media information with the individuals to connect” after the groups were over, reflecting the strength of the connections developed over the 4-day period.
Challenges
In contrast, some groups had minimal between-participant interaction. This pitfall was also identified by a few participants in the feedback survey (e.g., “It very much felt like we were just posting prompt responses and not talking to each other”; “I would introduce more interactive activities that allow participants to engage with one another if this is what is desired for the study. I kept seeing the same few people responding to each post every day.”). To address these concerns, midway through fielding the study, moderators began implementing a variety of techniques to engage participants with the prompts and each other. Successful techniques included tagging specific participants’ usernames in follow-up probes, “liking” posts, and responding to each post with supportive comments and/or follow-up questions for the group as applicable. Nevertheless, some groups remained less interactive, underscoring that the group interaction of synchronous focus groups may be harder to replicate in asynchronous environments (Zwaanswijk & van Dulmen, 2014). This is a critical consideration for researchers interested specifically in group processes. Future studies should investigate strategies to more reliably generate the sense of connectedness displayed in some of our AOFGs.
Lesson Learned #3: Considerations for Sampling, Collection of Rich Data, and “Fit” for the Study Population
Researchers who are contemplating AOFG study designs must consider their goals for sampling and the type of data they seek to collect. Inseparable from both of these considerations is the need to determine whether AOFGs, which rely on access to digital technology and asynchronicity, are a “good fit” for their target study population.
Strengths
As described previously, this AOFG study successfully recruited a geographically diverse, gender-diverse, and ethnically diverse young adult sample. The quality of the focus group data were rich, with participants providing lengthy and thoughtful responses to prompts and creative approaches to our interactive digital activities. A benefit of online focus groups is the opportunity to expand the kinds of data that can be collected; with this method, we also collected such forms of participant responses as emojis, “likes,” responses to each other’s posts, and additional links and images spontaneously shared by participants.
Challenges
The richness of the data collected may only be possible if the method is a good fit for the study population. Our study population—a young adult cohort that came of age in an era of nearly pervasive interactive online media use—appeared to be generally comfortable with the technology we provided. In addition, as this study was focused on an under-researched topic (eating disorders prevention) among a marginalized population (TGD young people), there was enthusiasm from many participants who reported being excited to participate in research that could benefit their community (e.g., from the feedback survey: “I’m glad to see that some folks are taking initiative to improve care for trans and non-binary people”). Before proceeding with an AOFG approach, researchers must evaluate the fit for their own study population. Some considerations for goodness-of-fit include the study population’s access to online technologies, comfort with digital communication platforms (e.g., social media), privacy concerns, and literacy-level.
Additional Considerations
Participants reported satisfaction with the flexibility and convenience of the AOFG structure as it allowed us to include those with non-traditional schedules (e.g., university students) and those without means to travel to an in-person focus group. AOFGs and other text-based data collection platforms may also have the benefit of being more accessible for some individuals with physical disabilities than traditional in-person research methods (Dahlstrom-Hakki et al., 2020). However, we were unable to make the study accessible to those without ready internet access and this remains a limitation of our own study. For studies with individuals who may experience even greater economic constraints or other barriers to internet access (e.g., unhoused populations), AOFGs may not be a viable method at this time.
Lesson Learned #4: Anonymity and Safety Planning
Online research methods have introduced a host of new challenges and opportunities related to protection of remote and/or anonymous research participants (Markham & Buchanan, 2017). Indeed, the anonymity of AOFG methods can be considered an opportunity to address a key ethical consideration with in-person focus groups (i.e., maintaining confidentiality of participants) (Ruff et al., 2005; Wilkinson, 1998). Researchers implementing an AOFG method, particularly one in which participants are anonymous or discussing sensitive topics, should consider development of a safety plan tailored to the unique AOFG environment.
Our top concerns in designing our study’s safety plan were: 1) ensuring our ability to preserve the anonymity of participants, and 2) ensuring participants who might disclose severe distress or acute crisis were provided with helpful and timely resources and responses from the study team. Additionally, while we wanted participants to feel comfortable sharing their experiences, we also wanted to ensure that the discussion space was emotionally safe for all participants, and therefore we prepared in the event that we would have to limit graphic or potentially harmful talk about mental health concerns (e.g., disordered eating behaviors, current suicidality).
Strengths
There were several advantages to using an anonymous platform for AOFG data collection, including reducing barriers to participation and collecting rich data. Several participants mentioned that they appreciated the anonymous, online format—both in the feedback survey and during the focus group discussions themselves (e.g., referencing their desire for similar spaces where they could connect with other TGD young people). Further, given the generously detailed and thoughtful responses participants provided we infer that many participants felt some degree of comfort sharing their personal stories in this environment.
Challenges
During the planning phase we realized that we would not be able to allow participant responses to be posted in real-time. Rather, screening and approval of submitted responses would be necessary to meet our safety plan goals. We opted for a rotating moderation team who traded off shifts over the course of 12 hours each day. Participants were informed in advance that the group would not be monitored at night. During the monitoring period, the moderator on duty reviewed and approved all posts within a few minutes of their submission; posts submitted overnight were reviewed and approved the following morning. This allowed the team to swiftly approve the majority of posts, and follow-up as directed by our safety plan in the minority of cases where there was a privacy or safety concern.
Additional considerations
In this study, safety concerns were minimal and the vast majority of all posts were approved immediately without modification or need for intervention. However, this may not be the case in all AOFG studies. Having a clinical psychologist on-call to review posts containing potential safety concerns was invaluable. Particularly when working with marginalized populations, we would emphasize the importance of being prepared to assist those who experience the burden of multiple forms of social and material stressors (e.g., stigma, racism, poverty, violence) and who may have limited access to mental health services or other support systems. Despite using our safety plan less than anticipated, our moderation team felt prepared to respond should a participant need support quickly.
Conclusion
AOFG methods constitute an innovative qualitative data collection method with growing utility and resonance in our increasingly digital social world. In the case study presented here we found AOFG methods yielded high levels of participant satisfaction and generated rich data on sensitive health topics among a marginalized population of young adults. As illustrated through our “Lessons Learned,” several limitations of the method must be considered, some of which speak to longstanding challenges and debates in the field of focus group research, and others of which are more recent issues related to use of emerging online technologies for social research. Limitations include barriers to accessing technology (i.e., AOFGs are sub-optimal for unhoused populations or those in regions without high-speed internet access), challenges in fostering a “group dynamic” or facilitating interaction between participants, the complexity of safety planning if participants are anonymous, and the importance of assessing a given study population’s comfort with an AOFG interface (i.e., those who are unfamiliar with social media or digital communication). Despite limitations, AOFGs are a valuable asset in a qualitative health researcher’s toolkit. Future research is needed to help identify strategies for promoting AOFG engagement and facilitating equitable access to AOFGs for those less familiar with or with less access to mobile technology.
Footnotes
Acknowledgments
The authors would like to thank the Harvard SOGIE Health Equity Research Collaborative, Trans Folx Fighting Eating Disorders, Lauren Sava at The Fenway Institute at Fenway Health, and all of the BRIGHT Project participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was conducted with support from Harvard Catalyst | The Harvard Clinical and Translational Science Center (National Center for Advancing Translational Sciences, National Institutes of Health Award UL 1TR002541) and financial contributions from Harvard University and its affiliated academic healthcare centers. Opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by Harvard Catalyst, Harvard University and its affiliated academic healthcare centers, or the National Institutes of Health.