
Abstract
The primary objective of this systematic review was to investigate how Western focus groups and Indigenous sharing circles have been blended for the study of Indigenous children’s health. The secondary objective of this study was to propose recommendations for adapting focus groups to include elements of sharing circles. This systematic review was conducted using a systematic search of original research articles published between 2009 and 2020 that (a) focused on North American Indigenous children’s health and (b) used group-based qualitative methods including focus groups and sharing circles. Each of the articles was screened for relevance and quality. The methods sections were reviewed, subjected to qualitative content analysis, and codes were analyzed to identify common themes and synthesize results. We identified 29 articles, most of which followed a community-based participatory research approach. In these publications, most included a community advisory board, ethics approval was obtained, and in some cases, community members were included as research assistants. There was evidence that sharing circles and focus group methods had been blended in the recent Indigenous children’s health literature. This was particularly apparent in the authors’ approaches to recruitment, location, facilitation techniques, question format and reimbursement. Several groups have published results that describe approaches that successfully incorporated aspects of Indigenous sharing circles into Western focus groups, thus establishing a research method that is culturally safe and appropriate for the study of Indigenous children’s health.
Keywords
Introduction
Western scientific research has been largely devoid of Indigenous ways of knowing (Martin, 2012; Peltier, 2018; Smith, 2013). For far too long, researchers have studied the health of Indigenous populations through a Western lens that fails to incorporate Indigenous culture and perspectives (Martin, 2012; Peltier, 2018; Smith, 2013). In recent years, there has been a call for researchers to participate in collaboration with Indigenous populations, ensuring that research projects are responsive to the needs of Indigenous peoples, and are conducted in culturally safe and appropriate manners (Martin, 2012; Peltier, 2018; Smith, 2013). With this call to action, researchers must be cognizant of the idea that there are alternative ways of knowing, and that both Western and Indigenous knowledge may work in compliment of each other to strengthen our collective understandings of health (Martin, 2012). Responding to this call to action requires Western researchers to include Indigenous methodologies and worldviews in their research; a notion referred to as “two-eyed seeing,” initially proposed by Mi’kmaw Elders Albert and Murdena Marshall (Bartlett et al., 2012; Martin, 2012; Peltier, 2018). The “two-eyed seeing” theoretical framework aims to improve collaborative research efforts in which both Western and Indigenous knowledge may be shared in a mutually respectful and beneficial manner (Bartlett et al., 2012; Peltier, 2018).
The Indigenous population is the most rapidly growing population in Canada (Statistics Canada, 2017). This population is also significantly younger than the non-Indigenous population in Canada, represented by a greater number of children and youth (Statistics Canada, 2017). Similar trends have also been observed in the United States (Executive Office of the President, 2014). These children and youth are particularly important to the future of their communities, as they are the generation of future leaders who will be responsible for the continuity of knowledge, culture, traditions and language (Greenwood & de Leeuw, 2012). In order to support these future leaders, we must protect and support their health so that they may live long, healthy lives that are free from the burden of disease. Currently, Indigenous youth in Canada and the United States face a number of health challenges and inequities that detract from this goal (Executive Office of the President, 2014; Greenwood & de Leeuw, 2012; Irvine et al., 2012). Overcoming these will require interventions aimed at improving the health of Indigenous children in a holistic and culturally-determined manner, while also promoting self-determination of Indigenous communities (Greenwood & de Leeuw, 2012; Irvine et al., 2012). In order to develop these interventions, there is a lot of research that needs to be completed in the area of Indigenous children’s health. Central to this research is the need to understand the perspectives of Indigenous children in regard to their own health. To facilitate these important conversations, researchers must develop methodologies that are culturally safe and appropriate, thereby satisfying the needs of Indigenous children and their communities, and the moral imperative of the researcher, who both aim to protect the health and well-being of the Indigenous children that they serve. One method in which this may be achieved is through the adaptation of Western focus groups to include elements of Indigenous sharing circles.
Focus groups are an example of an accepted Western qualitative research method that is commonly used to collect data from multiple participants at once, whereby all participants share their perspectives. In typical Western focus groups, participants are commonly recruited through advertising, using media such as flyers and posters (Rothe et al., 2009). Participants then gather at a central and convenient location where they participate in facilitated discussions for up to 2 hours (Côté-Arsenault & Morrison-Beedy, 1999; Rothe et al., 2009). Focus group discussions follow a semi-structured question format and are led by a trained facilitator, who is generally part of the research team (Rothe et al., 2009). Once the focus group is complete, participants may be reimbursed with monetary incentives (Rothe et al., 2009). Sometimes, focus groups will also have food and beverages available to participants (Côté-Arsenault & Morrison-Beedy, 1999; Rothe et al., 2009). Although focus groups are commonly used to study Indigenous health, this Western methodology lacks the inclusion of traditional methods of storytelling that are commonly used by Indigenous communities to gather and share information, thereby failing to honor Indigenous traditions and perspectives (Nabigon et al., 1999).
Indigenous populations have used sharing circles as a method of conveying stories and experiences for generations, with each community practicing a unique variation that is appropriate to their specific culture and traditions (Lavallée, 2009; Rothe et al., 2009). Due to the unique nature of sharing circles in each individual Indigenous community, it is important to adopt a protocol that honors the traditions and culture of the community by seeking advice from knowledge keepers. In general, the sharing circle approach provides a respectful and supportive environment whereby Indigenous peoples can autonomously express their perspectives and reflect on their experiences without interruption or questioning (Nabigon et al., 1999; Rothe et al., 2009). Through active listening to one perspective at a time, solutions to problems are identified, and the group achieves a shared understanding that aims to benefit the entire community (Nabigon et al., 1999; Rothe et al., 2009).
In addition to providing a safe environment for open discussion, sharing circles honor oral traditions and interaction styles that are specific to the culture within the community (Lavallée, 2009; Rothe et al., 2009). The experience of sharing circles may be deeply spiritual, intensifying connections among community members, the spiritual world and the earth, while also providing a mode of healing (Lavallée, 2009; Nabigon et al., 1999). Sharing circles may also be deeply emotional, allowing for both tears and laughter (Lavallée, 2009; Nabigon et al., 1999). Sharing circle participants are recruited through word of mouth, usually with the assistance of community members or local groups (Rothe et al., 2009). Participants gather at a location that is culturally relevant and where ceremony may be held (Rothe et al., 2009). Before the sharing circle takes place, the participants often engage in an opening prayer or ceremony, introducing a spiritual aspect to the session (Lavallée, 2009; Rothe et al., 2009). Sharing circles are facilitated by respected members of the community, such as Elders, who act humbly as equal participants, openly expressing their own perspectives, while also showing honor and respect to other sharing circle participants (Lavallée, 2009; Nabigon et al., 1999).
Discussion among sharing circle participants occurs in an open-ended format, sometimes using oral history and storytelling (Lavallée, 2009; Rothe et al., 2009). Participants have equal opportunities to speak throughout the sharing circle and may pass around an article (e.g., a talking stick or feather) from speaker to speaker, indicating who is able to speak openly without being interrupted (Rothe et al., 2009). Within the circle, speakers are afforded the opportunity to speak in a clockwise or counterclockwise manner, waiting for their turn while other participants complete their thoughts (Lavallée, 2009; Nabigon et al., 1999). Participants are able to share as much or as little as they wish, allowing for autonomy throughout the entirety of the process (Nabigon et al., 1999). When every member of the circle has spoken, participants are given another opportunity to speak and share any new thoughts or feelings that arise after listening to their peers, once again moving around the circle in a clockwise or counterclockwise direction and respecting each member's turn (Nabigon et al., 1999). Perspectives will be shared over a time period of approximately 3–8 hours, or however long it takes for community enlightenment to be achieved (Nabigon et al., 1999; Rothe et al., 2009). Once the sharing circle is complete, participants may be thanked for contributing to the sharing circle by receiving food and beverages, or a gift that is of cultural significance (Lavallée, 2009; Rothe et al., 2009).
It is recommended that researchers conduct their research in collaboration with Indigenous communities in a manner that is culturally safe and appropriate, as mainstream Western research methodologies may not satisfy the needs of the Indigenous populations being studied (Burnette et al., 2011; Flicker & Worthington, 2012; Priest et al., 2009; Ten Fingers, 2005). Integrated methodologies that combine Indigenous and Western paradigms may provide an avenue in which the goal of conducting culturally safe and appropriate research may be achieved. Combining elements of Indigenous sharing circles with elements of Western focus groups has been previously recommended for conducting qualitative research in Indigenous communities. This blending provides an opportunity to honor the culture and traditions of the Indigenous community in which the research takes place and satisfies the needs of Western academic peer-reviewed journals in which the researchers aim to publish their findings (Lavallée, 2009; Nabigon et al., 1999; Rothe et al., 2009).
Within the current literature, there are very few guidelines that assist researchers in developing integrated methodologies for health research involving Indigenous children. Children require different methodologic approaches due to their incomplete cognitive development and limited attention spans (Arbuckle & Abetz-Webb, 2013). Thus, we cannot generalize from adult literature. For Western researchers who wish to collaborate with Indigenous communities to examine the health and well-being of Indigenous children, this lack of guidance may pose as a barrier to culturally safe and appropriate research and may perpetuate a dangerous cycle of Western research methodologies being imposed on Indigenous children. In the increasing body of peer-reviewed literature focusing on Indigenous children’s health, there is a growing number of studies that utilize focus groups, sharing circles or a blend of both methods. However, without much guidance available for blending these methods, there is a high degree of variation in terms of how focus groups and sharing circles are being utilized in peer-reviewed studies involving Indigenous children’s health. Thus, the primary objective of this systematic review was to determine how focus groups and sharing circles have been implemented in published studies of Indigenous children’s health. We chose to narrow the focus of the review to focus on the peer-reviewed literature since this is a primary source of information used by academic researchers and because the peer-review process ensures a level of rigor within the documents. However, we acknowledge that there is a vast array of important information published in the gray literature and encourage scholars working in this field to read widely in their preparation. The secondary objective of this systematic review was to propose recommendations on how to adapt focus groups to include elements of sharing circles, creating a blended method that is culturally safe and appropriate when utilizing Indigenous children as research participants.
We chose to focus specifically on utilization of sharing circles in research related to children’s health and to focus on the North American Indigenous context. Although we recognize that other international Indigenous populations utilize sharing circles, there is a high degree of diversity in terms of how sharing circles are performed within these populations. As such, a focused review was chosen to limit the diversity of the findings and to avoid making too many generalizations.
Method
Literature Search
The first step in the process was a systematic search of the peer-reviewed literature to examine original peer-reviewed research articles that had applied focus groups, sharing circles, or a blend of both in a population of children. Search terms were established a priori that focused the search on group-based qualitative methodologies, the cohort of interest, and the setting of interest. In total, 19 search terms were identified. The timeline was originally set to include publications between 2009 and 2019 to reflect the most current research that had been published around a similar time as the Canadian Institutes of Health Research (CIHR) Guidelines for Health Research Involving Aboriginal People (2007–2010), and Chapter 9 of the Tri-Council Policy Statement outlining ethics of health research involving First Nations, Inuit and Metis people (2010).
A systematic literature search was performed in February 2019, and updated in June 2020, using PubMed and Bibliography of Native North Americans databases. A literature search of CINAHL was also performed using the search terms, but no new articles were identified. These databases were chosen so that both Western and Indigenous literature were equally represented in this literature review. Boolean search strategies, such as “AND” and “OR,” were employed in order to include as many key terms as possible in the literature search, which allowed for retrieval of the most relevant articles. Searches were also restricted to the English language, human studies, and a date range between 2009 and 2020. Literature search criteria are summarized in Table 1.
Literature Search Terms.

Relevance and Quality Assessment
Primary appraisal
As potentially relevant publications were identified through the literature search, each article underwent a primary appraisal of its relevance to ensure that the results were focused on the topic of interest. The content of titles and abstracts were examined for relevance using pre-determined eligibility criteria. The eligible criteria for research articles to be included were as follows: (a) an original research article (b) focused on North American Indian or Indigenous children between the ages of eight and 18, and (c) employed group-based qualitative methods such as a focus group, sharing circle, or equivalent method. One examiner independently performed the literature search and primary appraisal of all research articles. To assess examiner bias, a second examiner was given the eligibility criteria and asked to indicate whether they would include or exclude a subset of five articles based on the defined criteria.
Secondary appraisal
Full text articles that were deemed eligible for review based on the results of the primary appraisal were read in detail to confirm eligibility by assessing quality. The Critical Appraisal Skills Programme (CASP) Qualitative Checklist was chosen as an appraisal tool for assessing the quality of the eligible research articles (Critical Appraisal Skills Programme, 2018). A quantitative scoring system was applied using the CASP Qualitative Checklist to confirm if each article was of adequate quality to be included in the systematic review (Butler et al., 2016). Examiner bias was assessed by having a second reviewer independently appraise five articles that were chosen at random, using the CASP Qualitative Checklist as an appraisal tool. It is important to note that the review process was completed by both a Western researcher (primary reviewer) and an Indigenous researcher (secondary reviewer).
Data Extraction and Analysis
We applied a data extraction checklist that was developed by modifying the Cochrane Reviews Data Extraction Checklist (Higgins & Green, 2011). Our focus was primarily on methods and participants. This checklist was used to record relevant information from each article included in the systematic review. Grounded theory was utilized to guide inductive analysis of the methods sections of eligible papers (Charmaz, 2017). Open coding was used to formulate categories and subcategories from analyzed text. The categories allowed for the identification of important aspects of the methodology to be compared (e.g., community-based participatory research, recruitment, location, facilitation, duration, data ownership, etc.). The subcategories were then compared to identify the differences in methodology within each category, highlighting which articles utilized aspects of focus groups, sharing circles, or a blend of both. Microsoft Excel was used to record relevant phrases from each article and each of the assigned categories and subcategories. Filters were applied to the categories to group categories of similar meaning. This supported the identification of common themes and strategies used by researchers for studying Indigenous children’s health in group settings.
Results
In total, 148 articles underwent primary appraisal, and 41 articles were determined to be eligible for full-text review (Figure 1). Examiner bias during this stage of the appraisal process was determined to be limited as both examiners (one Western and one Indigenous) achieved identical appraisal results upon review of the same five articles. During the full-text review stage, 11 articles were excluded because they did not meet the study’s eligibility criteria. A common reason for exclusion was that studies focused on young adults above the age of 18 within their “youth” cohort. Using the CASP Qualitative Checklist during the secondary appraisal stage, one article was appraised as low-quality and was excluded from the systematic review (Figure 1). Thus, a total of 29 articles were included in the qualitative analysis.
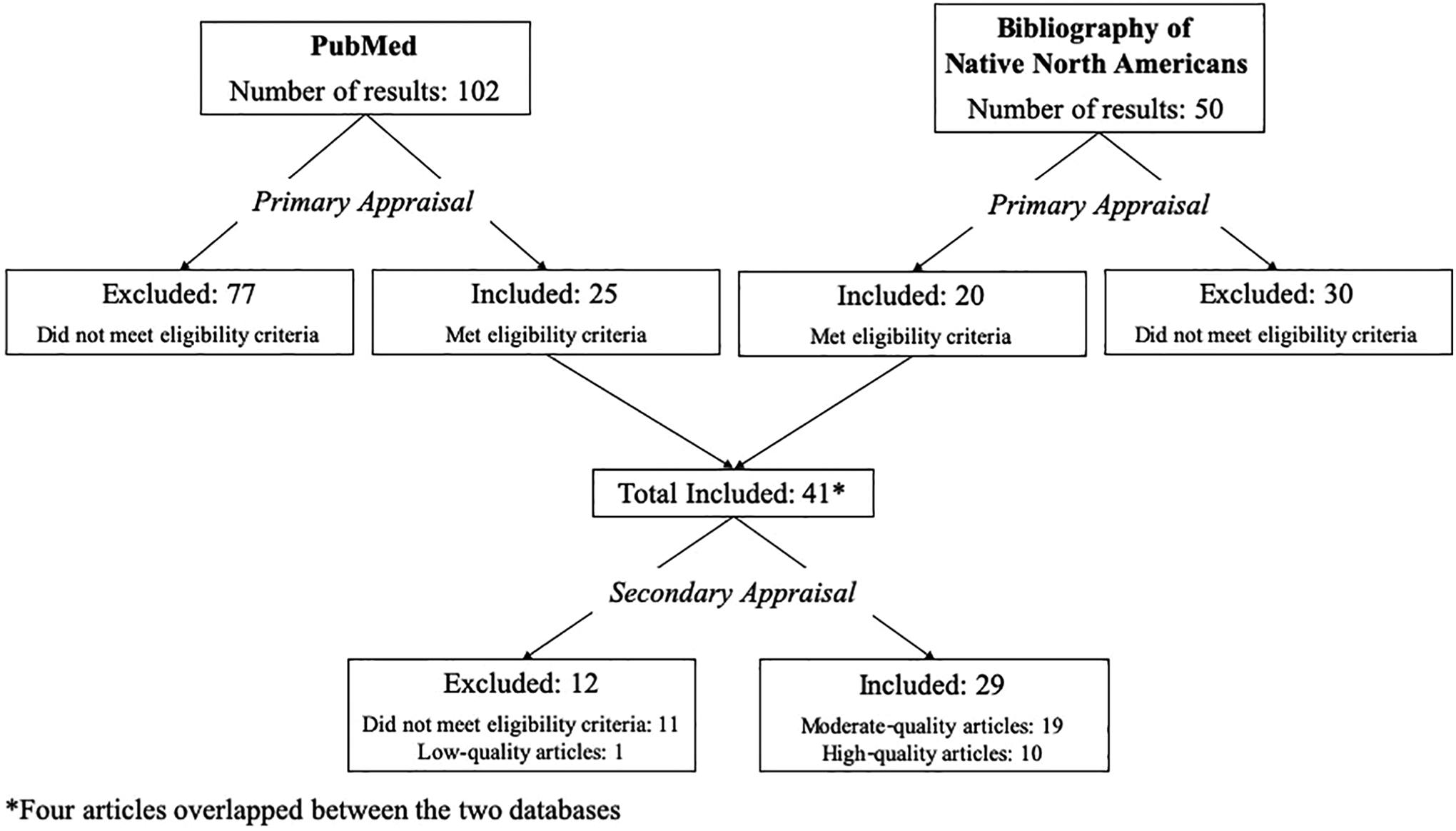
Summary of study selection and exclusion from electronic literature search.
Of the studies that were included in the systematic review, 19 articles were classified as being of moderate quality, and 10 articles were appraised as high quality. While assessing for examiner bias, both reviewers agreed that all five of the randomly selected articles should be included in the systematic review. However, there were some discrepancies between reviewers in terms of how the articles were rated (i.e., moderate-quality or high-quality). Upon discussion between reviewers, the first reviewer utilized the “hints” on the CASP Checklist, resulting in scoring three articles as moderate-quality and two articles as high-quality. The second reviewer chose not to use the hints on the CASP Checklist, resulting in high-quality rankings for all five papers. It should be noted that if the CASP Checklist is to be used as a quality appraisal tool for a systematic review, reviewers should have a mutual understanding regarding the use of the “hints” before independently reviewing articles to maximize consensus among reviewers. The final ratings were assigned based on the CASP Checklist with hints.
Study Initiation
The open coding of the reviewed articles identified several steps in study initiation as being important to the blending of sharing circles and focus groups, although these steps were not necessarily assigned to either a sharing circle or focus group methodology. These include important aspects of study initiation such as engaging in community-based participatory research (CBPR), establishing a community advisory board (CAB) or equivalent, obtaining ethics approval and seeking research assistance from the study community. These results aligned with our secondary objective to provide recommendations for designing blended methods that are culturally appropriate. Given the diversity of cultures and approaches to sharing circles in different North American Indigenous populations, engaging the communities are an important first step in achieving this goal.
Community-based participatory research
Researchers who wish to study Indigenous children’s health must have a firm understanding of CBPR before designing any research project involving sharing circle or focus group methodologies, to help guide their research. CBPR is a collaborative research initiative whereby communities are actively engaged in all aspects of the research process through equal partnerships with researchers (Israel et al., 2001). It is through these partnerships that communities have opportunities to define relevant research questions that aim to improve the communities’ health, devise research methods that are culturally appropriate, participate in data collection and analysis, and harness ownership of the data as well as control over the dissemination of results. It is also important to note that CBPR can be utilized in Indigenous children’s health research that takes place in Indigenous communities and in urban settings. CPBR also stresses the importance of relationships and reciprocity, which are fundamental to Indigenous cultures. Relationships are particularly important when engaging with Indigenous children, as they must trust that the researcher will nurture them and protect them from harms. This is exceptionally important given the history of traumas that have been inflicted on previous generations of their peoples.
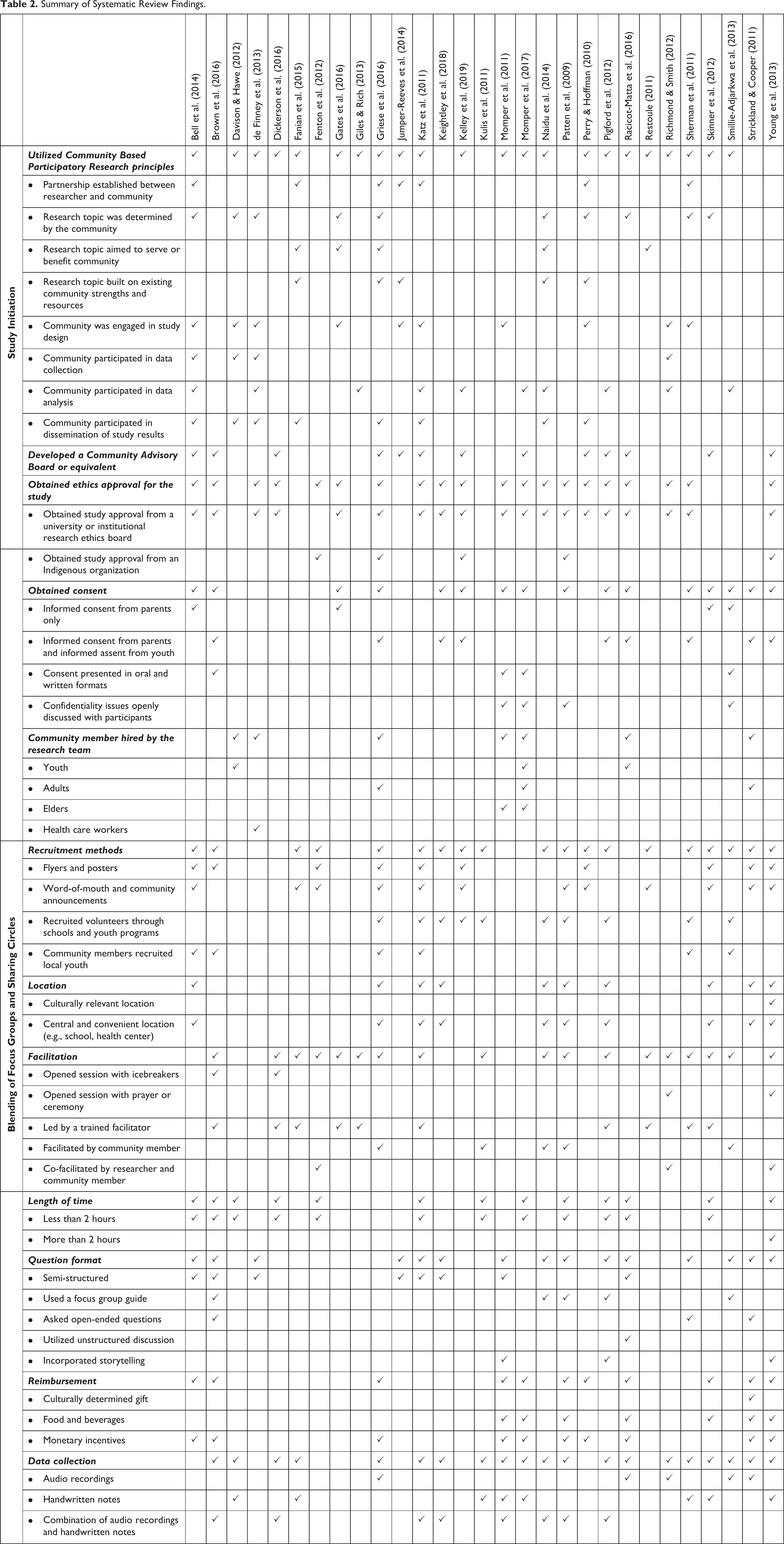
Of the 29 studies included in this literature review, 22 studies (76%) discussed using CBPR either explicitly or implicitly. These are listed in Table 2, under the sub-heading “Utilized Community Based Participatory Research principles.” Using CBPR, an equal partnership between the community and the researcher must be established, as was documented in seven of the 29 papers (24%) (see Table 2, subheading “Partnership established between researcher and community”). Thirteen studies (45%) explicitly reported the use of CBPR principles such as: the research topic was determined by the community, aimed to serve or benefit the community, or built on existing community strengths and resources (Table 2). The community was also engaged in the study design process and ensured cultural appropriateness of research methods in 10 (34%) of the studies reviewed (see Table 2, subheading “Community was engaged in study design”). Additionally, the community also contributed to data collection in four studies, analysis in 10 studies, and dissemination of study results in eight studies (Table 2).
Summary of Systematic Review Findings.
The article by Bell et al. (2014) was a particularly good example of a paper that expressed the use of CBPR principles throughout their study. Their methods section was explicit regarding the use of CBPR and supported this statement by including information on the formation of a partnership between the researchers and the community, and engaging the community in the research design, development, implementation, analysis and dissemination of results. In addition, the article by Perry and Hoffman (2010) provided a justification for the use of CBPR in research involving Indigenous communities, and documented the collaborative process in which the researchers involved community members in various steps of the study, thereby providing another good example of how CBPR may be utilized and reported.
Community advisory board
There were 13 studies (45%) that described using a CAB, which was also referred to as a steering group, steering committee, or planning committee (see Table 2, subheading “Developed a Community Advisory Board or equivalent”). When developing a research project that involves Indigenous children, the establishment of a CAB should be one of the first steps taken by the research team to ensure that the project aligns with CPBR standards and is culturally appropriate. Along with the primary investigators, the CABs were comprised of Elders, Tribal Council members, community health care workers, youth workers, educators, community youth, among other community members and stakeholders deemed appropriate by the community (Bell et al., 2014; Brown et al., 2016; Dickerson et al., 2016; Jumper-Reeves et al., 2014; Katz et al., 2011; Kelley et al., 2019; Momper et al., 2017; Perry & Hoffman, 2010; Pigford et al., 2012; Racicot-Matta et al., 2016; Skinner et al., 2012; Young et al., 2013). The CABs helped define the research question, participated in study design, assisted in data analysis by providing feedback and validation, and worked with the researcher to influence how the results are presented (Griese et al., 2016; Jumper-Reeves et al., 2014; Katz et al., 2011; Momper et al., 2017; Perry & Hoffman, 2010; Pigford et al., 2012; Racicot-Matta et al., 2016; Skinner et al., 2012; Young et al., 2013).
Study/ethics approval
Of the 29 studies that were included in this review, 19 studies (66%) indicated that they obtained study approval or ethics approval from a university or institutional review board (Table 2). It is important to note that in Canada, Chapter 9 of the Tri-Council Policy Statement requires that researchers engage with Indigenous communities prior to seeking institutional research ethics board approval (Government of Canada, 2019). Interestingly, five of the 29 studies (17%) described receiving study approval or ethics approval from Indigenous organizations (Table 2). These Indigenous organizations included the Assembly of First Nations (Fenton et al., 2012), Indian Health Service Institutional Review Board (Griese et al., 2016), Rocky Mountain Tribal Institutional Review Board (Kelley et al., 2019), Yukon-Kuskokwim Health Corporation Human Studies Committee (Patten et al., 2009), and the Manitoulin Anishinabek Research Review Committee (Young et al., 2013).
In addition to seeking study and ethics approval, there are additional ethical considerations when children and/or youth are included in a study. There were nine studies (31%) that described obtaining informed consent from parents as well as informed assent from youth, and four studies (14%) that described obtaining parental consent only (Table 2). To ensure that consent was understood by all participants, four studies (14%) presented consent information to participants in both oral and written formats (Table 2). Issues surrounding confidentiality were also openly discussed with study participants in four studies (14%) (Table 2).
Research assistance
To further promote community engagement, seven studies (24%) hired community members as research assistants for the duration of the study (Table 2). These community members included local youth (Davison & Hawe, 2012; Momper et al., 2017; Racicot-Matta et al., 2016), community members (Griese et al., 2016; Momper et al., 2017; Strickland & Cooper, 2011), Elders (Momper et al., 2011, 2017), and community health workers (de Finney et al., 2013). Including community members was important for enhancing trust and comfort between participants and researchers, and providing valuable insight into the study population and culture (Griese et al., 2016; Momper et al., 2017).
Blending of Sharing Circle and Focus Group Methods
The articles by Rothe et al. (2009), Lavallee (2009) and Nabigon et al. (1999) provided clear descriptions of the methods that typically belong to Indigenous sharing circles and those that more typically belong to Western focus groups. These descriptions were used to guide the analysis of the methodologies used by each of the reviewed articles. Specifically, recruitment of participants, location, facilitation and reimbursement were analyzed.
Sharing circles tend to recruit participants through word-of-mouth, usually through a community group, cultural center or local stakeholder (Rothe et al., 2009). The sharing circle itself is held in a culturally relevant location, whereby participants sit in a circle (Rothe et al., 2009). Before sharing occurs, a ceremony or prayer may be held (Lavallée, 2009; Rothe et al., 2009). A community member leads the sharing circle by using oral history and open-ended questions to guide discussion, while also acting as an equal participant (Lavallée, 2009; Nabigon et al., 1999; Rothe et al., 2009). An artifact, such as a feather or talking stick, may be passed around the circle in a clockwise or counterclockwise manner, indicating who is able to speak without interruption (Lavallée, 2009; Nabigon et al., 1999). Participants in possession of the artifact may talk as much or as little as they prefer and are respected and supported by their peers and the leader (Nabigon et al., 1999). The sharing circle may range from 3–8 hours, or however long it takes for community enlightenment to occur (Nabigon et al., 1999; Rothe et al., 2009). After the sharing circle commences, participants may be thanked with a culturally determined gift, food or beverages (Lavallée, 2009; Rothe et al., 2009).
In contrast, focus groups tend to recruit participants through advertising in media and posters (Rothe et al., 2009). The participants meet with the researchers at a central and convenient location, whereby participants are greeted and may engage in icebreakers prior to focus group discussions (Côté-Arsenault & Morrison-Beedy, 1999; Rothe et al., 2009). Focus groups are facilitated by a trained member of the research team who asks pre-determined questions in a semi-structured format (Rothe et al., 2009). The facilitator does not participate in the focus group beyond asking questions and collecting data. The length of the focus group is typically less than 2 hours (Rothe et al., 2009). Participants may be provided with food and beverages or reimbursed through monetary incentives (Côté-Arsenault & Morrison-Beedy, 1999; Rothe et al., 2009).
Of the 29 studies reviewed, 24 (83%) incorporated at least one aspect of sharing circles in their focus group methodologies, thereby demonstrating that the majority of group-based qualitative methods in peer-reviewed studies involving Indigenous children’s health in North America have some degree of blending. However, although each of these 24 studies utilized aspects of sharing circles and focus groups in their methods, there was a greater reliance on focus group methods, suggesting that the Western lens presented more strongly in the peer-reviewed literature. The aspects of the qualitative methods that were analyzed included recruitment methods, location of focus groups, identity of the facilitator, length of focus group session, question format and reimbursement. Of these methods, most of the blending occurred within recruitment methods, identity of the facilitator, question format and reimbursement.
Recruitment
Of the 29 articles included in this review, 19 (66%) described their recruitment methods (Table 2, “Recruitment methods”). Flyers and posters are recruitment methods that are typically associated with Western focus groups (Rothe et al., 2009). Ten studies (34%) described using these Western methods of recruitment (Table 2). In contrast, 12 studies (41%) recruited volunteers through word-of mouth or community announcements, 10 studies (34%) recruited volunteers at schools and youth programs, and six studies (21%) recruited volunteers utilizing local stakeholders and key tribal members (Table 2). All of these recruitment methods are associated with traditional sharing circles (Rothe et al., 2009). Interestingly, 10 of these 21 studies (48%) described their recruitment methods as a mixed-methods approach, whereby both Western focus group recruitment methods and traditional sharing circle recruitment methods were used to recruit youth volunteers (Table 2). Examples of mixed methods approaches included media advertising combined with community-based recruitment methods through word-of-mouth, community members, or local schools and youth programs. Recruitment of volunteers was, therefore, an example of one step in which focus groups and sharing circle approaches has been successfully blended.
Focus group location
Traditional sharing circles are held at places that are culturally relevant, in which ceremonies may be held (Rothe et al., 2009). One study described using a medicine lodge that was located on the reserve, allowing for prayer, a smudging ceremony led by an Elder, and dissemination of local teachings (Young et al., 2013). Focus groups, in contrast, generally take place in central and convenient locations (Rothe et al., 2009). There were 10 studies that described using convenient types of locations, such as schools or health centers (Table 2). However, it is important to note that many of these studies were held at convenient locations within Indigenous communities. From this information, it may be speculated that although focus group locations were often held in convenient locations (as per focus groups) instead of ceremonial locations (as per sharing circles), conducting interviews within the Indigenous communities provided a level of cultural relevance that aided the blending of these two methods. Interestingly, of the six studies that took place in urban settings (Brown et al., 2016; Kelley et al., 2019; Kulis et al., 2011; Restoule, 2011; Richmond & Smith, 2012; Smillie-Adjarkwa et al., 2013), one of these studies was conducted at a location that offered services and programming for Indigenous youth (Richmond & Smith, 2012), providing further cultural relevance.
Facilitation
Two studies described using icebreakers (Table 2), to allow the participants to feel more comfortable with each other and with the researchers, which aligns with typical Western focus groups. Conversely, there was one study that began each session with a prayer (Richmond & Smith, 2012), and another study that began their session with a prayer and smudging ceremony (Young et al., 2013). Both prayer and ceremonies are commonly completed before the initiation of a sharing circle (Rothe et al., 2009).
There were 20 studies that discussed the identity of their focus group leader. Ten studies (50%) indicated that their focus groups were led by a trained facilitator (Table 2), who was generally the researcher, as is common with Western focus groups. Interestingly, two of these studies included an Indigenous researcher (Katz et al., 2011; Restoule, 2011). In traditional sharing circles, the discussion is facilitated by a respected community member, such as an Elder or community health worker (Rothe et al., 2009). There were five studies (25%) in which the researchers trained community members (e.g., local youth, youth program facilitators, community health workers, community researchers) to be facilitators (Table 2), providing one example of how focus groups and sharing circles have been blended. There were also three studies (15%) in which a co-facilitation model was used, whereby the researcher was paired with a community member to lead discussion (Table 2). As an additional support, three studies actively engaged Elders during the focus group sessions as a guide and storyteller, and for post-interview debriefing with the youth (Momper et al., 2011, 2017; Richmond & Smith, 2012).
In terms of the interview length, most sessions resembled a focus group rather than a sharing circle, since 12 out of 13 studies (92%) that reported timing of focus group sessions were less than 2 hours (Table 2). In contrast, traditional sharing circles typically last from 3 hours to 8 hours (Rothe et al., 2009). Interestingly, one study conducted focus group activities over one day, aligning with the length of time of a sharing circle, but each activity lasted only 90 minutes, providing one example of how sharing circles and focus groups may be blended (Young et al., 2013).
Similar to interview length, question formatting was also more aligned with Western focus groups, rather than Indigenous sharing circles. Western focus groups are generally semi-structured and included a discussion guide or list of probing questions (Rothe et al., 2009). Eight studies (28%) specified using a semi-structured question format, and five studies (17%) used an interview guide (Table 2). Sharing circles, on the other hand, tend to utilize oral teachings and open-ended questions (Rothe et al., 2009). Some studies described using open-ended ended questions, unstructured discussion, or storytelling (Table 2). Sometimes these methods were used in combination with semi-structured questions or an interview guide, allowing for successful blending of focus groups and sharing circles.
Reimbursement
Monetary reimbursement, which is typical of focus groups, was observed in 10 studies (34%) (Table 2). Sharing circles, on the other hand, may include culturally determined gifts as a form of reimbursement (Rothe et al., 2009). This type of reimbursement was observed in one study (Strickland & Cooper, 2011). Both focus groups and sharing circles may also provide participants with food and beverages, providing one commonality between the two methods (Rothe et al., 2009). There were seven studies that distributed snacks, beverages, or a feast to participants (24%) (Table 2), sometimes in addition to monetary incentives. Since food and beverages are commonly provided by both focus group and sharing circle methods, this is one simple way in which these methods may be blended.
Data Collection and Analysis
The method of data collection is an important consideration for any study involving Indigenous youth and should be agreed upon by the CAB and the researchers. A combination of handwritten notes and audio recordings was a common method of collecting data from group discussions, as mixed methods were used in eight articles (28%) (Table 2). There were eight articles (28%) that described using handwritten notes as the sole data collection method (Table 2). One article indicated that audio recordings of participants were considered culturally inappropriate, or recording discussions would make the participants uncomfortable, and were, therefore, not permitted for data collection (Skinner et al., 2012). Only five articles described using audio recordings as the sole data collection method (Table 2).
In some instances, Indigenous community members aided the researchers in the data analysis process (Table 2). These community members included Indigenous researchers, members of the CAB, and focus group participants (Bell et al., 2014; de Finney et al., 2013; Giles & Rich, 2013; Katz et al., 2011; Kelley et al., 2019; Momper et al., 2017; Naidu et al., 2014; Pigford et al., 2012; Richmond & Smith, 2012; Smillie-Adjarkwa et al., 2013). Using the expertise of these community members, transcripts were verified for accuracy in both content and cultural context (Giles & Rich, 2013; Momper et al., 2017; Pigford et al., 2012). Furthermore, community members had the opportunity to identify information in the transcripts that should be kept confidential (Perry & Hoffman, 2010; Pigford et al., 2012). Engaging community members in the data analysis portion of research project is, therefore, recommended to ensure cultural appropriateness and to protect the privacy of the community.
Dissemination of Study Results
It is recommended that Indigenous peoples have equal ownership over data that was collected in their communities and have shared decision-making power over the dissemination of results from research studies that took place in their communities. One study described establishing a data sharing agreement that gave the CAB decision-making power concerning confidentiality, access to data, and dissemination of data (Perry & Hoffman, 2010). In two instances, the authors specified that members of the community participated in the authorship of research articles that resulted from the studies that occurred in their communities (Fanian et al., 2015; Naidu et al., 2014). This result is likely an underestimate, as authors may have included community members as authors without explicitly stating this in the text. There were some cases in which the communities preferred not to be named or preferred to have community identifiers removed from research articles or other forms of public dissemination of data (Giles & Rich, 2013). This provision allowed for communities to protect their identity, which was especially important when sensitive topics (e.g., alcohol and drug abuse among youth) were discussed.
Discussion
Blending of Sharing Circles and Focus Groups
Although most of the studies reviewed were able to adapt Western focus group methodologies to include at least one element of sharing circles, the focus group methodologies were much more prominent. This finding demonstrates that there is much work to be done to better incorporate Indigenous methodologies in group-based qualitative studies that focus on Indigenous children’s health. This work may be completed by encouraging Western researchers to become better versed in Indigenous methodologies, such as sharing circles, by paying more attention to balancing the two approaches, or by more actively engaging community members and traditional knowledge keepers in conversations surrounding study design.
Of the 29 studies reviewed, the article by Young et al. (2013) provided the best example of how to blend sharing circles with focus groups, as each aspect of their methods incorporated aspects of sharing circles. Before the initiation of their study, the researchers consulted a community advisory committee and hosted open community consultation sessions to discuss study design and results. Participants were recruited through community advertising. The focus groups were held within the community, at the health center’s medicine lodge. Each of the sessions began with a smudging ceremony and prayer led by a local Elder. Focus group sessions utilized a co-facilitation model whereby the researcher and a community member shared the responsibility of leading the discussion. Throughout the day, focus groups and other activities were held in 90-minute intervals, and participants were provided with food and beverages. Although this study provides a good example of how focus groups may be adapted to incorporate elements of sharing circles, a number of other studies reviewed provided other methods in which focus groups and sharing circles may be blended. Using the collective body of peer-reviewed literature reviewed in this study, we hope to provide recommendations for a general approach in which researchers can better incorporate aspects of sharing circles into their focus group methodologies.
Recommendations
Given the information provided in this review, a researcher who intends on studying Indigenous children’s health should be well-versed in the principles of CBPR. To initiate a research project of this kind, a CAB must be established. The researcher and the CAB should work in an equal partnership that (1) identifies a topic of study that is responsive to the needs of the community, (2) develops culturally appropriate research methods, (3) validates the accuracy of data, and (4) supports the dissemination of results. In addition to establishing a CAB, researchers should consider hiring a community member as a research assistant in order to facilitate trust and comfort between participants and researchers, and to gain a stronger sense of cultural context within their research. As per any studying involving humans, ethics approval from an institutional review board should be sought. If possible, researchers should also consult Indigenous research organizations for additional insights on ethical considerations for studies involving Indigenous children, as traditional Western institutional review boards may not be able to identify specific cultural needs.
In general, the articles included in this review tended to follow Western focus group methods to a greater degree than traditional Indigenous sharing circle methods. This finding may be influenced by systemic structures such as funding, ethics approval and peer-reviewed publications that may privilege the use of focus groups as an established Western group-based qualitative research method. There were, however, instances in which the focus groups were modified to include some elements of sharing circles, allowing for a blended method that achieved a greater degree of cultural appropriateness. Recruitment of research participants may include a mixed-methods approach which incorporates flyers and posters displayed within the community, as well as word-of-mouth recruitment disseminated though community announcements and key community members such as Elders, youth workers, or health care workers. The preferred location for these methods appeared to be a central and convenient location within the Indigenous community, or, in the case of urban studies, at a location where Indigenous youth services or programming were regularly held. If deemed appropriate by the community, a ceremony such as a prayer or smudging may be included at the beginning of the session, prior to initiating group discussion. Food and beverages may also be provided to participants as an incentive throughout the duration of the session. To lead group discussions, a co-facilitation model may be utilized, whereby a researcher is paired with a community member who is trained to facilitate group discussion. This model is important for establishing trust and comfort among researchers and participants, thereby increasing participation within group discussion. A multi-stage approach, in which participants return for multiple focus group sessions, may also help to improve trust and comfort over time. A semi-structured question format may be used; however, it is beneficial to include open-ended questions and to allow for unstructured discussion in which the topics may stray. The researchers should encourage responses from participants, but should not adamantly require responses, especially during discussions in which sensitive topics are discussed. Data from group discussions may be recorded using a method that is deemed culturally appropriate by the community. During instances when sensitive topics are discussed, it may be beneficial for the child participants to have access to a community member, such as an Elder, who is able to provide a debrief after the session is complete. Using these methods, a successful blending of focus groups and sharing circles may be achieved.
When analyzing the results of the study, several advantages became apparent when involving members of the community as Indigenous researchers, and actively engaging research participants (e.g., as part of member checking), community volunteers, and members of the CAB. Utilizing these resources in the data analysis process will aid the researchers in validating the content included in the resulting transcripts, understanding cultural content and correcting errors in cultural wording. These community members will also be able to identify information that must remain confidential, such as community identifiers or cultural practices that may only be discussed among members of the community.
The researchers and CAB should have an established data-sharing agreement that governs how study results are presented to the public. This agreement may have provisions that discuss ownership or authorship. In general, the researchers should be working in collaboration with the communities to determine if the research being presented is accurate and culturally appropriate.
Although these recommendations were derived from the collective body of literature reviewed in this study, it should be emphasized that these recommendations may not be appropriate for all populations being studied. As previously stated, there is a high degree of variability between various Indigenous cultures in North America, that translate into diversity in how sharing circles are conducted in individual communities. Therefore, it is always best practice to work with knowledge keepers in the community (ies) where a study will be conducted, as they will provide the most valuable information that will allow the researcher to follow local cultural protocols. In addition, this review focused specifically on North American Indigenous populations and may not be appropriate for use among Indigenous populations in other continents. We encourage researchers working in other regions of the world to build on the foundation provided by this review to analyze the use of sharing circles in other Indigenous populations, such as those in Australia.
Study Limitations
The majority of the information extracted from the research articles were taken from methods sections. In general, methods sections were the shortest section in research articles, forcing authors to be concise and to include only the most important details. Furthermore, we questioned whether publication bias may have led to the exclusion of cultural information from the methods sections (e.g., use of a talking stick), to provide more details on mainstream methodologies that are more widely understood and accepted by Western researchers and journals. Similar questions have been raised by other researchers within the literature (Adams & Faulkhead, 2012; Fitzpatrick et al., 2016; Priest et al., 2009; Smylie et al., 2014). In addition to journals requesting authors to exclude cultural information, the communities that participated in the research studies may have asked for cultural information to be excluded from the articles, in order to protect individual community’s cultural artifacts, rituals and traditions. While only one of the articles in this review explicitly stated that community identifiers had been removed to respect community preferences (Giles & Rich, 2013), it is possible that other articles removed community identifiers without explicitly stating that they had done so. Together, these factors may have contributed to this review’s finding that the majority of studies included in this review tended to resemble Western focus groups, rather than Indigenous sharing circles.
Conclusion
Indigenous children’s health researchers should strive to use methodologies that are both culturally safe and appropriate. One way in which this may be achieved is through the blending of Western and Indigenous research methods and ways of knowing. In this systematic review, there were many strong examples of how Western focus groups and Indigenous sharing circles have been successfully blended in the recent North American Indigenous children’s health literature, as most of the studies incorporated at least one aspect of sharing circles in their focus group methodologies. However, our results suggest that the balance is not equitable; the Western lens is stronger as the majority of studies more closely aligned with Western focus groups. Based on this evidence, recommendations have been proposed for future studies that aim to use group-based qualitative methodologies to gather information and perspectives on health from Indigenous youth in North America. These recommendations may be used to inform researchers of more culturally safe and appropriate ways of studying Indigenous children’s health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.