
Abstract
Vascular access is a potentially fatal vulnerability for hemodialysis patients, and a notable area for improvement for healthcare providers. Hemodialysis central venous catheters (HD-CVC) are associated with increased morbidity and mortality from infectious complications. Clinical practice guidelines on vascular access for hemodialysis and infection control do not provide a standard definition for infection of the HD-CVC exit site. The main aim of this protocol is to establish consensus on the signs and symptoms for preventing CVC exit site infection for patients receiving hemodialysis, based on the opinion of a panel of experts. The secondary study aim is to determine the optimum treatment approach according to the signs and symptoms of infection at the HD-CVC exit site, as prioritized by the panel of experts. For this purpose, a modified ranking-type Delphi technique will be used, with three rounds of evaluation conducted via an online questionnaire: the first two rounds will be used to prioritize, by consensus, the most relevant signs and/or symptoms of infection of the HD-CVC exit site or tunnel. Once this consensus has been achieved, a third round of evaluation will be conducted, asking the participants to ascertain the most appropriate treatment approach. The research team has drawn up a list of signs and symptoms related to infection of the HD-CVC exit site or tunnel, based on the definitions obtained from a previous systematic review. The results of the present study will enable us to design an assessment scale for HD-CVC exit sites, thus facilitating early identification and action if infection occurs. The availability of such an instrument will benefit not only clinical practice, but also research, healthcare education and training programs for professionals in this area.
Keywords
Background
Chronic kidney disease (CKD) is a major public health problem worldwide. Its prevalence ranges from 7%–12% (Romagnani et al., 2017) and nearly 700 million people around the world are affected (Bikbov et al., 2020). When the glomerular filtration rate is <15 ml/min/1.73 m2, renal replacement therapy must be initiated. Approximately 9.7 million people, globally, are currently receiving this type of treatment (Bikbov et al., 2020). Dialysis is the most widely used treatment for CKD, and 90% of these patients undergo hemodialysis (Himmelfarb et al., 2020). The cost of CKD care is high; in Canada, for example, the estimated annual cost is $32 billion (Manns et al., 2019). In the USA, CKD affects approximately 10% of Medicare beneficiaries but accounts for 20% of expenditure. Patients with end-stage renal disease are especially costly, representing only 1.6% of Medicare beneficiaries but responsible for 7.2% of healthcare spending (United States Renal Data System, 2019).
Vascular access is a potentially fatal vulnerability for hemodialysis patients, and a notable area for improvement for healthcare providers. Vascular access for hemodialysis must meet various requirements, such as providing adequate blood flow to achieve an optimal dialysis dose and offering safe access to the bloodstream (Ibeas et al., 2018). All clinical practice guidelines on hemodialysis recommend the internal arteriovenous fistula (autologous or prosthetic) as the ideal vascular access, due to its lower rate of complications compared to central venous catheters (CVC) (Canadian Society of Nephrology (CSN), 2012; Clinical Practice Guidelines for Vascular Access, 2006; Kumwenda et al., 2015; Polkinghorne et al., 2013; Vanholder et al., 2010).The use of CVC is associated with higher morbidity and mortality, related to infectious complications, and may contribute to poorer clinical outcomes and increased healthcare costs (Klevens et al., 2007; Stevenson et al., 2002; Taylor et al., 2004; Wang et al., 2015). It has been reported that the already high cost of haemodialysis (in Spain, it accounts for 1% of healthcare expenditure for 0.043% of the population, at an average cost of €40,136 per patient per year, and a range of €46,254 to €53,289 per patient per year) (Conde Olasagasti et al., 2017; Parra Moncasi et al., 2011) is substantially increased by the costs related to infectious complications from CVC. The total hospitalization cost of a CVC-related infection is estimated at $17,000 to $32,000 (Nissenson et al., 2005; Ramanathan et al., 2007; Reed et al., 2005), depending on the causative agent and the duration of treatment/hospitalization.
Nevertheless, CVC are commonly accepted as an alternative to arteriovenous fistulas, as they can be used immediately after implantation. The need to allow time for the maturation of arteriovenous fistulas, and the resulting uncertainty about when hemodialysis treatment can be started, contribute to the high frequency and prolonged duration of CVC use (Arhuidese et al., 2018). Some 70%–80% of incident hemodialysis patients initiate treatment via a CVC (Noordzij et al., 2014; United States Renal Data System, 2019). Among prevalent patients, however, the use of a CVC is 30%–40% less frequent (Noordzij et al., 2014; United States Renal Data System, 2019).
According to the literature, the incidence of bacteremia related to the hemodialysis catheter is highly variable (from 1.6 to 6.18/1,000 catheter-days for tunneled catheters and from 1.4 to 8.3/1000 catheter-days for non-tunneled catheters) (Develter et al., 2005; Weijmer et al., 2004). Similarly, the incidence of exit site infection ranges from 0.35 to 8.3/1000 catheter-days for tunneled catheters, and from 8.2 to 16.75/1,000 catheter-days for non-tunneled catheters (Betjes, 2011; Develter et al., 2005; Stevenson et al., 2000; Weijmer et al., 2004). This variability may be due to heterogeneity in the clinical management of patients and/or to varying degrees of adherence to clinical practice guidelines. It may also be due to differences in definitions of catheter-related infections.
Bacteremia originates from the adherence by microorganisms and their subsequent colonization of the catheter surface, creating a biofilm (communities of microorganisms growing within a matrix of exopolysaccharides, adhered to an inert surface or living tissue). Studies have shown that most (if not all) of the bacteria cultivated in the catheter lumen and in the blood of patients affected by bacteremia are similar to those detected on the catheter branches and around the exit site. This has important implications in daily clinical practice, since it lends experimental support to the idea that the control of biofilm formation, both in the catheter branches and at the exit site, is an important element in preventing catheter-related bacteremia (Abad & Safdar, 2011; Betjes, 2011; O’Grady et al., 2011; Pascual et al., 2011). Various definitions of exit site infection have been proposed in clinical practice (Ibeas et al., 2018; Lok et al., 2020; Mermel et al., 2009; O’Grady et al., 2002; Vascular Access 2006 Work Group, 2006), and consensus on this question has yet to be reached. Nevertheless, appropriate evaluation and management of the exit site is of fundamental importance, since it is a potential source of microbiological colonization, which if it gives rise to exit site infection can lead to bacteremia and sepsis (Harwood et al., 2008). The high degree of subjectivity and variability among current definitions of exit site infection, depending on the source, can result in inadequate management and the appearance of fatal complications. Therefore, it is necessary to seek consensus regarding the signs and symptoms that warn of the presence of exit site infection, and also on healthcare regarding the use of CVC, before the appearance of exit site infection, in order to prevent systemic infectious complications and even death.
Aims
The main aim of this protocol is to establish consensus on the signs and symptoms for preventing CVC exit site infection for patients receiving hemodialysis, based on the opinion of a panel of experts. As a secondary objective, we seek to determine the most appropriate treatment approach for such patients, according to the signs and symptoms of CVC exit site infection observed, according to the priorities established by the same panel of experts.
Explanation and Justification of Method
Current clinical practice guidelines on vascular access for hemodialysis and infection control do not provide a universal definition regarding exit site infection (Ibeas et al., 2018; Lok et al., 2020; Mermel et al., 2009; O’Grady et al., 2002; Vascular Access 2006 Work Group, 2006). In view of this heterogeneity, we believe it necessary to seek consensus on the unequivocal signs and symptoms of this infection. This consensus would then enable us to validate a scale facilitating the early identification of the presence of exit site infection, without the need for a microbiological culture. In addition, there should be agreement on the most appropriate treatment approach, according to the signs and symptoms observed. In this respect, the 2019 update of the KDOQI Clinical Practice Guideline (Lok et al., 2020) indicates as a recommended area for future research “further validation studies of diagnostic criteria for exit site and tunnel infections in hemodialysis patients.”
To reach the necessary consensus on these questions, using a systematic procedure, a very appropriate method is that of the Delphi technique, in which expert comments on a given area of study are compiled and analyzed estudiar (Hsu & Sandford, 2019).
The Delphi technique can be defined as an iterative multi-stage process designed to transform a set of different opinions into group consensus (Lynn et al., 1998; McKenna, 1994). It consists of a series of structured group processes, each termed a round, conducted in order to reach the greatest possible consensus among a geographically-dispersed group of experts (Burt et al., 2009).
The experts consulted via the Delphi method participate anonymously and on an equal footing, via their responses to a purpose-designed questionnaire (Fink et al., 1984). This methodology has been used in previous research in this field for the design of similar scales (Broadhurst et al., 2017; Ray-Barruel et al., 2014; Verberne et al., 2019).
Materials and Methods
Study Design
The present study uses a modified ranking-type Delphi technique (Thompson, 2009) to obtain evidence of content validity (Falzanaro & Pinto Zipp, 2013). We propose to conduct three rounds of evaluation, using an online questionnaire. The first two rounds will enable us to prioritize, by consensus, the most significant signs and/or symptoms of infection of the exit site and/or tunnel of the hemodialysis catheter. Once this consensus has been achieved, a third round will be conducted in which the participants will be asked to identify the most appropriate treatment approach.
Development of Questionnaire Items
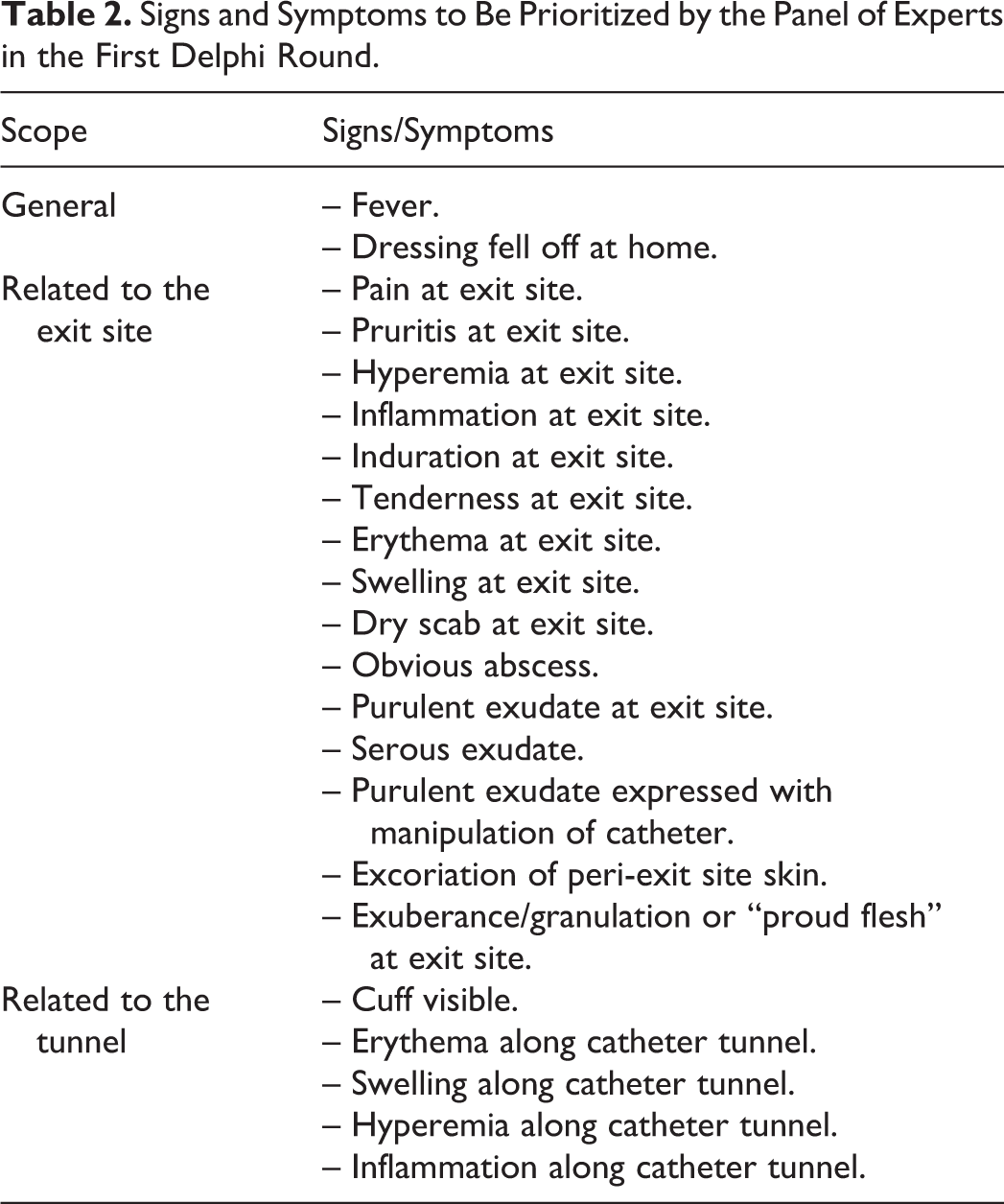
The research team has drawn up a list of signs and symptoms related to infection of the exit site or tunnel of the hemodialysis catheter, based on the corresponding definitions identified in a previous systematic review, which included a manual review of published clinical practice guidelines for renal care and infection control (Table 1). From this list of HD-CVC exit site infection predictors, the research team then conducted a critical analysis, resulting in a final list of 23 signs and symptoms, which constituted the items to be evaluated by the panel of experts (see Table 2).
Clinical Practice Guidelines and Definitions of Exit Site Infection for Hemodialysis Catheters.

Signs and Symptoms to Be Prioritized by the Panel of Experts in the First Delphi Round.
First round
The experts directly assess the items referring to the exit site or tunnel infection, after identifying clinical signs and symptoms derived from the systematic review, according to the relevance and identification value of the item (Steurer, 2011). This relevance, in the expert’s opinion, will be scored on a 4-point Likert scale, from 1 = Little relevance to 4 = Highly relevant. After the evaluation of each item, the expert will be invited to make additional suggestions or comments, as qualitative feedback, in open fields included for this purpose. After these first 23 items, the questionnaire will include an open question, inviting the expert to indicate any additional sign or symptom considered of interest.
Second round
The panel of experts will review the signs and symptoms suggested in the first round, together with the modifications and suggestions indicated. They will be asked to evaluate the degree of relevance of these items in relation to their usefulness for identifying HD-CVC exit site or tunnel infection. This evaluation will be scored using a 4-point Likert scale ranging from 1 = Little relevance to 4 = Highly relevant.
Third round
The first two rounds are expected to produce a list of essential signs and symptoms, prioritized to identify HD-CVC exit site or tunnel infection. In this third round, the panel of experts will be asked to indicate their recommended treatment approach in response to each sign/symptom, from a list of options, where more than one option can be selected. This list is based on the recommendations given in various clinical practice guidelines for the care of HD-CVC, including close surveillance of the exit site, local treatment of infection, systemic treatment of infection, and possible withdrawal of the catheter (Ibeas et al., 2018; Lok et al., 2020). An “Other options” section will also be included, in which the experts can indicate, if they wish, a treatment option not included in the initial list. If more than three additional treatment options are proposed, consideration will be given to conducting a fourth Delphi round in order to establish consensus.
Distribution and Completion of Questionnaires
The successive rounds of contact with the panel of experts (Holloway, 2012) and the subsequent collection of their evaluations, suggestions and comments will be conducted using an online tool designed for this purpose, such as “SurveyMonkey.”
Emails will be sent to internationally-renowned experts in the management and care of vascular access for hemodialysis, inviting them to take part in this survey. In addition, each prospective panelist will be sent information about the study and an informed consent form, which must be completed and signed before the end of the third round.
In each of the following rounds, further letters will be sent with information related to specific aspects of the process (Falzanaro & Pinto Zipp, 2013; Holloway, 2012).
In each successive round, the aggregated results from the previous one will be analyzed and summarized, and the suggested modifications incorporated, leading to the reformulation of the signs/symptoms considered (Keeney et al., 2006; Steurer, 2011). In every case, the participants’ responses will be processed anonymously.
The quality of the Delphi technique to be applied has been confirmed by reference to the checklist proposed by Hasson (Hasson et al., 2000), regarding methodological aspects such as preparation, steps to be followed, data collection and ethical considerations, to ensure that the data collection procedure is applied correctly and rigorously. This checklist is intended to overcome the variability traditionally associated with the use of the Delphi technique and to address the criticisms that have been made of the associated procedures, following the wide variety of methodological modifications that have been evidenced in prior research.
Sampling/Recruitment
Initially, the panel of experts will be obtained by intentional non-probabilistic sampling. In a second stage, a snowball sampling technique will be applied (Frewer et al., 2011; Goluchowicz & Blind, 2011; Holloway, 2012; Okoli & Pawlowski, 2004).
International experts in the management and care of vascular access for hemodialysis will be invited to take part. These experts will be identified from the contact details of the authors of the articles included in the systematic review, and from networks of practitioners and researchers, via scientific societies in the areas of renal care and vascular access. Those initially contacted will also be asked to suggest other potential participants, whether or not personally known to them, with appropriate profiles (McKenna, 1994; Steurer, 2011).
The following criteria for inclusion in the study will be applied: (a) active in at least one of the following professions: Medicine and Nursing; (b) meet the stipulated profile of internationally-recognized expert practice and geographic environment; and/or (c) have (co)authored at least one publication on the management of HD-CVC, indexed in Journal Citation Reports, or have participated in the development of research or protocols or clinical practice guidelines on vascular access for hemodialysis (Baker et al., 2006). Persons currently developing or working with similar instruments, and/or those who have published details of one in the last ten years, will be excluded from the sample.
Applying these inclusion and exclusion criteria, approximately 30 potential panelists will be invited to take part. These persons will be distributed proportionally among the professions, profiles and geographical environments considered. Allowing for non-responses and drop-outs, the final sample is expected to consist of at least 20 panelists, following the criteria defined by de Villiers et al. (de Villiers et al., 2005).
Data Handling/Analysis
Establishing an Initial Level of Consensus
A minimum level of consensus will be established for the relevance of the sign/symptom to be assessed, namely ≥75% agreement, determined by summing the response categories “Fairly relevant” (equal to 3 on the Likert scale) and “Highly relevant” (equal to 4 on the Likert scale) (Polit & Beck, 2006).
Items that do not reach 75% consensus in the first round will be eliminated, or modified according to the participants’ comments and suggestions, if any. Any such modifications will be made according to the panelists’ comments and respecting, as literally as possible, the proposals or reformulations suggested. Following this first round, the signs/symptoms (with the applicable modifications) agreed upon, together with the new ones proposed, will be evaluated in the same way in the second round (Steurer, 2011). The required level of consensus for the second round will be the same as for the first.
In the third round, consensus on the treatment approach recommended for each sign/symptom will be assumed when the frequency of agreement (determined as in rounds 1 and 2) is ≥75%.
Data Analysis
A descriptive analysis will be conducted of the scores given by the panel of experts, using the mean and the interquartile range regarding the degree of relevance of the signs and symptoms in the first two rounds of the Delphi process. The signs and symptoms producing mean scores less than 3 will be eliminated. The interquartile range will be used to represent the spread of the data and to evaluate the level of consensus for each sign/symptom. Those with a mean score of 4 (Highly relevant) and a small interquartile interval (equal to or less than 1) will be considered descriptors with a high degree of consensus.
The results obtained from the third round of the Delphi process will be used to calculate the percentages for each treatment option, for each sign/symptom.
The qualitative data from round 1 and round 3 will be collected and analyzed by content analysis techniques (Falzanaro & Pinto Zipp, 2013).
Ethics
This study has been approved by the Research Ethics Committee for Medical Products of Cantabria (CEIm of Cantabria, approval code 2019.146).
The email to be sent to potential members of the international panel of experts will be accompanied by information on the performance of the study with the Delphi method, the benefits of participating in the study, the guaranteed confidentiality of the data obtained and the voluntary nature of participation.
The personal data of all participants will be processed, communicated and transferred in full compliance with the provisions of the Spanish Organic Law 3/2018, of 5 December, on Personal Data Protection and the Guarantee of Digital Rights.
In addition, an informed consent form will be attached, which the participant will be asked to complete, sign and return to the principal investigator before the end of the third Delphi round.
Practical Implications/Discussion
The results of this study will enable us to design an exit site assessment scale for HD-CVC, facilitating early identification and action in response to infection.
According to previous research, the use of a validated exit site assessment scale can reduce the likelihood of local and systemic infectious complications by 10% (Goddard et al., 2006). For example, in the Hemodialysis Unit of the Valdecilla Hospital, approximately 20% of local infections and 8% of systemic ones are related to tunneled CVC (Cobo Sánchez et al., 2011, 2013; Martínez Alvarez et al., 2017). The financial savings from the use of a scale such as the one we propose would be €278,274 per year (€239,704 for systemic infections and €38,570 for local ones), calculated according to the current costs of the health services provided by the Cantabria Health Service (Consejeria de Sanidad del Gobierno de Cantabria, 2017).
At present, no validated scale exists for evaluating the risk of infection of CVC exit sites, tunneled or not. In view of the various clinical practice guidelines that have been issued on the need to objectively record the follow-up of infectious complications, together with the clinical and economic impact of this condition, undertaking the design and validation of a scale for evaluating the exit sites of HD-CVC, whether tunneled or not, appears fully justified.
The use of an exit site assessment scale based on signs of infection provides the following advantages: – It improves clinical safety of our patients and therefore healthcare results. – It provides greater objectivity in clinical observation, providing a uniform classification, thus facilitating the comparison of results. – It enables practitioners to measure the effects of interventions on the incidence of infectious complications at the exit site. – Patients can receive objective information about the status of the catheter exit site, encouraging greater involvement in self-care, especially when signs of infection are observed. – It improves the continuity of care and provides a documented, objective record of the evolution of the exit site.
The availability of an instrument such as the one we propose will benefit not only clinical practice, but also research, healthcare education and training programs for professionals in this area.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Marqués de Valdecilla Research Institute (IDIVAL), grant number NVAL18/05.