
Abstract
The rise of digital mobile communications has made possible novel research methods that can provide a better understanding of patients’ experience of non-communicable diseases. This study explores the opportunities and challenges in employing “digital diaries” via mobile phones to track the lived experiences of people with hypertension in the Philippines. Following in-depth interviews, 40 hypertensive adults were invited to submit digital diaries over 12 months. Mobile phones were found to be an efficient way of reaching participants, although it was difficult to collect in-depth narratives about their experiences using the medium beyond nominal responses about symptoms and treatment. Possible explanations include the asymptomatic nature of hypertension, which limited the participants’ experiences of the illness, as well as the platform itself, which our mostly-elderly, low-income participants may not be comfortable with. Despite these challenges, “digital diaries” hold potential for the study of other chronic conditions, provided that researchers engage in extensive co-production with participants to understand their preferences. Researchers also need more training in the use of these methods appropriately as part of a suite of methods for capturing the experience of people living with chronic illness.
Keywords
Introduction
Diaries are well suited in collecting longitudinal data, reducing the time between an experience and the account given of it, and thus reducing potential recall bias (Alaszewski, 2006; Bolger et al., 2003). Diary keeping has been used in health research since the 1930s (Keleher & Verrinder, 2003). In this respect, it offers advantages over more commonly used research methods, such as interviews (Reis, 1994). The use of a diary also eliminates the presence of the researcher, granting the patient autonomy in sharing their lived experiences as they unfold, free from some of the biases that can arise when being observed, while allowing silence from participants on topics they do not wish to share in an interview context (Alaszewski, 2006). The potential advantages offered by unsolicited diary entries, with spontaneously recorded accounts of everyday life, has been acknowledged in studying patients’ health and suffering (Jones, 2000). They have been used for chronic health conditions because of their ability to track patients’ lived experiences in detail (Alaszewski, 2006; Jacelon & Imperio, 2005). Diary methods can also capture environmental factors that can shape participants’ experiences (Bartlett, 2012). Thus, diary tools are seen as having the potential to capture authentic experiences that reflect individual priorities and values while promoting self-reflexivity (Alaszewski, 2006), helping participants to think through the problems they face that may be difficult to distill in the course of a single interview.
When used traditionally, however, as in writing notes in a journal collected later by researchers, diaries have certain disadvantages. These include the risk of loss or breaches of confidentiality, forgetting to keep diaries, or losing motivation to do so (Bernays et al., 2019; Bolger et al., 2003; Furness & Garrud, 2010; Herron et al., 2019; Jones & Woolley, 2014). Written diaries may not be appropriate for everyone and can exclude certain populations, including those with poor literacy and disabilities (Alaszewski, 2006; Griffiths & Jordan, 1998; Miller et al., 1999; Milligan et al., 2005; Stopka et al., 2004). Diaries using mobile technology are thus seen as a way to overcome these challenges (Bernays et al., 2019; Jacelon & Imperio, 2005; Stopka et al., 2004), especially with individuals who have long-term conditions in which interactions between a patient and a researcher are, of necessity, episodic (Alaszewski, 2006). They are also more flexible, interactive, and can better capture non-verbal facets of the everyday lives of participants, conveyed through videos, photographs, and audio recordings (Bernays et al., 2019; Buchwald et al., 2009; Thompson & Oelker, 2013).
Digital diaries, using mobile devices (e.g. mobile phones, tape recorders) do, however, share some of the disadvantages of the traditional diary approach, including privacy issues, where it may be difficult to make confidential entries, and devices being lost or damaged, risking the security of data (Bernays et al., 2019). They may also be problematic for those with auditory and communication difficulties, as well as those who are not technologically skilled (Furness & Garrud, 2010). Nonetheless, the rapid pace of technological advances increasingly provides means by which researchers and research participants can interact in a dynamic and collaborative process (Hyers, 2018).
There has been particular interest in the use of mobile phones in low-and middle-income countries (LMICs) (Bastawrous & Armstrong, 2013), where uptake of these devices has been rapid, in part representing a response to a lack of fixed infrastructure, such as telephone lines, but also a reduction in the price of devices and connection charges (World Bank, 2016). For health research, the revolution in mobile phone use worldwide would seem to offer many opportunities. However, as we have discovered, these opportunities are accompanied by important challenges. Mobile communication is also increasingly used in clinical research, with growing evidence suggesting that text messaging improves adherence to treatment and follow-up (de Jongh et al., 2012; Free et al., 2013; Gurol-Urganci et al., 2013; Horvath et al., 2012; Whittaker et al., 2019). Studies conducted in LMICs, including the Philippines, have identified similar effects (Albino et al., 2014; Crankshaw et al., 2010; Otieno et al., 2014; Palileo-Villanueva, 2017). However, the use of digital technologies to conduct qualitative health research, or indeed for qualitative research in general, has not been well documented (García et al., 2016).
Given the ubiquity of mobile phones in LMICs, we examine the potential of using a digital diary to collect patient narratives about hypertension management in the Philippines. The Responsive and Equitable Health Systems Partnership on Non-Communicable Diseases (RESPOND) is a longitudinal study employing mixed-methods to understand barriers to the effective management of hypertension at each stage of the journey (from pre-diagnosis to ultimate control) among low-income households in the Philippines and Malaysia (Palafox et al., 2018). We believed that digital diaries via mobile phones would be appropriate in the Philippines, which has been called the “texting capital of the world” based on its very high use of short message services (SMS)—a phenomenon that appears to transcend income group (Capistrano, 2013; Celdran, 2002; Lallana, 2004; Librero et al., 2007; Pertierra, 2005). The World Bank reported a more than doubling of the number of mobile subscriptions in just a decade, from 50 million users in 2007 to 115 million in 2017 (The World Bank, 2020). In 2019, it was reported that 89% of the adult population in the Philippines had access to some type of mobile phone and, despite very poor internet connectivity, Filipinos are among the most intensive users of the internet worldwide (We Are Social, 2020).
One element of the qualitative component applied in the Philippines is a digital diary recorded using mobile phones to capture the lived and evolving experiences of our hypertensive participants during the period between the two sets of in-depth interviews. The entries submitted by participants were stored on a secure online platform, with researchers accessing, managing and analyzing the data via a web-based interface. In this paper, we draw on our experiences to make recommendations on how to adopt this approach for qualitative health research.
Methodology
Study Setting and Participants
The rationale for choosing hypertension as the health condition of interest is that our previous research reported lower adherence to antihypertensive medication among the poor in Malaysia and the Philippines (Chow et al., 2013). Poor adherence partly reflects barriers associated with health systems and services common in LMICs (Khatib et al., 2014; Maimaris et al., 2013), but patients’ social realities may also affect their treatment choices, such as by precipitating “trade-offs” where, for instance, one must prioritize family and livelihood over hypertension care (Brathwaite et al., 2020). In this analysis, we focus our attention on the Philippines where the study was fully implemented and has now concluded.
In the Philippines, 600 adult participants were randomly selected from poor communities in an urban and a rural setting to participate in the quantitative survey. They were either previously diagnosed with hypertension (“aware”) or identified as having high blood pressure during the screening for RESPOND but not previously diagnosed with hypertension (“unaware”) (Palafox et al., 2018). From the quantitative database, 40 individuals were selected purposively for the qualitative component according to age, sex, urbanicity, and awareness. The selected individuals were contacted to confirm their participation and to arrange a visit. Written consent was secured from participants upon meeting. They underwent an initial interview, after which they were briefed about the use of digital diaries and were asked to participate for 12–18 months, to be followed by another interview. Table 1 provides the characteristics of our participants. All had access to a mobile phone, either personally owned or shared within their homes.
Sampling Characteristics of Qualitative Participants (Philippines).

Digital Diary Platform
We used a platform developed by On Our Radar (OOR), an innovative, secure, web-based application that collates participant-generated content in the form of video, photo, audio, and text captured and submitted using their own mobile phones (OnOurRadar, 2015). Previous incarnations of the platform have been used in a variety of settings (the United Kingdom, Sierra Leone, Kenya, Nigeria, and India) enabling participants, ranging from elderly individuals suffering from early-stage dementia in Britain to citizen reporters amid the Ebola outbreak in Sierra Leone, to share their daily experiences in both the health sector and beyond. Projects that employed the OOR platform have worked with isolated and vulnerable community members who were able to contribute entries using basic mobile phones, thus giving them a voice to shape policies and programs. The platform designed specifically for the RESPOND project was developed jointly with OOR team members, who have experience in adapting the application to diverse settings, and aimed to collect information that would allow a detailed mapping of the steps constituting the most common pathways followed by individuals to manage their hypertension. The on-screen layout is shown in Figures 1 and 2.

The on-screen layout of On Our Radar platform. Names of the researchers and participants were concealed.

The on-screen layout of On Our Radar platform. Names of the researchers and participants were concealed.
Researchers access the web-based platform via a two-step authentication process required to log-in. They may then create participant profiles and enroll them onto the platform. Each profile requires a designated mobile number, which is linked to the participant’s name, location, age, and email address (if applicable) in their profile. If a participant changes mobile number, a new profile must be created. Participants communicate with the platform by placing calls or sending messages to a designated locally-registered phone number.
The OOR platform also allows two-way interaction, whereby researchers may communicate with participants by replying via text message, for example to request participants to elaborate, to follow-up on issues and to encourage participation. The platform also incorporates a language translation function, which automatically converts participant entries from a local language to English. The platform was designed for this project in an open-source format, and was provided by the developers as a ready-to-use tool that will be retained by the partners and local stakeholders after completion of the project for use in other research projects.
Preparations for Participants and Researchers
To supplement their briefing on the digital diaries, participants were given an infographic (see Supplemental Appendix A) in the local language (Filipino), providing guidance on the type of information to submit; how to contact the research team should they have any questions or concerns about the diary or the platform; as well as information about the provision of mobile phone credit to remove direct financial barriers to study participation. The infographic was intended to serve as a reminder for the participants to share their everyday experiences of living with hypertension and sought to clarify what the researchers wanted to know, as there was a risk of “information overload” if this point was only communicated verbally. The guidance emphasized that all entries were confidential, and participants could provide as few or as many entries as they felt appropriate. The infographic also clarified that the platform was a data collection tool and not a means to discuss any legal or medical concerns.
Before using the platform, the researchers read a manual produced by the development team, with advice from the local advisory committee in the Philippines (see Supplemental Appendix B). The manual contained standard operating procedures, including guidance on modes of operation, strategies of participant engagement, research conduct, and expectations related to the digital diaries. It also included advice on how to manage submissions that fall beyond the study scope, for example, should participants seek medical, legal or financial advice. In such cases, the researchers were instructed to acknowledge the participants’ concerns and direct them to appropriate sources of advice within their community (e.g., local health centers and community halls, or municipal offices). It was made clear that the digital diaries would only serve as a means to capture the participant narratives related to their hypertension and not as a conduit for medical advice. The researchers involved in the operation of the platform received training, frequent support from the broader team, and advice on how to deal with unexpected behaviors or requests.
Analysis of Diary Entries
All diary submissions, primarily in SMS text format (total of 760 messages), were considered primary data and were analyzed predominantly using an inductive approach (Thomas, 2006) guided by grounded theory (Strauss & Corbin, 1994). The entries were exported from the platform to identify emerging themes about participants’ motivations and understanding on the use of the platform. Researchers ensured reflexivity in the collection and analysis of diary entries (Finlay, 2008). The first author, who is a local researcher, led the open coding of textual entries in their original format and language using NVivo. As most entries contained colloquial and abbreviated terms, looking at the data in their original form ensured that social and cultural contexts were maintained (Hymes, 1974). Emerging themes were discussed with the research team, composed of local and international researchers to identify their (often implicit) meaning.
Another type of diary entry, “call logs,” were collected by way of phone calls between researchers and participants. The summaries of calls were entered onto the platform by the researchers and translated into English. As such, call logs were considered as a secondary source of data in our analysis to acknowledge the re-construction of meaning and context that resulted from the translation process (Temple et al., 2006). Twenty-five call logs were carefully read and contrasted with the SMS text entries to show variation in the quality of data generated.
Results
Engaging Participants
The techniques used to engage participants in the digital diary process are summarized in Table 2. All participants were reminded weekly about the diary by sending a text message via the platform. Incentives, in the form of mobile credits intended to cover the direct costs of submitting diary entries in all forms, were provided weekly to the participants. Subsequent prompts and messages from the researchers concerned participants’ lived experiences with hypertension (e.g., asking how they address their condition if they reported they have high blood pressure, how they treat hypertension daily, why and how they monitor their blood pressure, what prompted them to take their blood pressure, and why they seek care). Success was defined as the effectiveness of these strategies in eliciting insightful or in-depth data from participants, while also sustaining their engagement over time, taking into account the frequency and the quality of received submissions.
Steps in Interacting via the Platform (See Supplemental Appendix B for More Detailed Information).

Initially, researchers planned to review collected diary submissions via the web-based platform interface two or three times a month; however, due to the limited engagement and depth of data provided by participants, weekly interaction became necessary to either remind them to submit diaries entries or respond to inquiries or prompts from researchers. These weekly messages were effective at increasing submission frequency but eliciting data with sufficient depth and to explore meaning required scheduled phone calls with participants. Because the platform did not integrate an outgoing call function, the research team set up a separate telephone phone number to conduct these calls, and “call logs” summarizing of these conversations were entered contemporaneously onto the platform by the researchers, as described above.
Levels of Engagement
While all participants initially engaged with the platform, by the end of the study only six could be considered to have actively engaged throughout, wherein they sent diary entries more than once a week, two of whom posted entries almost daily even without probing from the researchers (see Table 3). Eleven participants were semi-active, sending entries once a week or from time to time, especially when they had just received their weekly mobile credit. Twenty-three were infrequent users, who engaged with the platform irregularly. Four agreed initially to participate, but later reported that they did not like sending SMS. Seven participants also changed their mobile phone numbers during the study. Weekly messages and mobile credits were sent to all participants regardless of level of engagement.
Levels of Engagement Among Digital Diary Participants by Age and Sex.
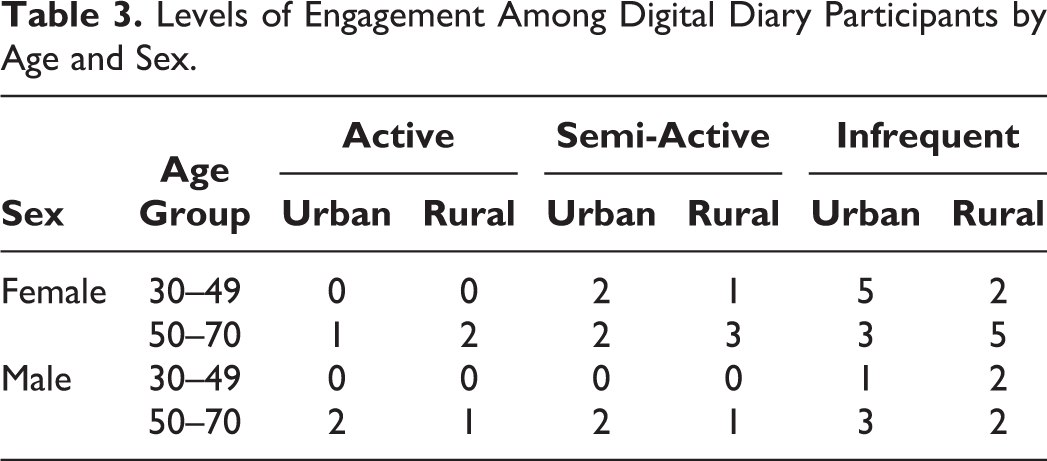
Our experience shows that digital diaries worked better for some types of participants than for others. For instance, active and semi-active participants tended to be in the older (50–70 years) age group; and more reported taking regular medication, having check-ups and frequent blood pressure monitoring (data not shown). Because the study was restricted only to participants aged 30 or above from low-income households, we were unable to assess whether those from richer households or younger participants would be more receptive. Also, we initially invited a balanced sample by age group and sex; however, women and older participants were more likely to agree as they were more likely to be at home. Men often work away from home for extended periods and were less likely to agree to participate.
Participants’ preferred mode of mobile communication (e.g., text message vs. phone call) also seemed to affect their engagement with the digital diaries. A final, important reason for a lower-than-expected level of sustained engagement, as revealed by the participants and despite the strategies enumerated in Table 2, relates to the asymptomatic nature of hypertension. As participants may feel well most of the time, they may not see the need to engage with the platform, and it is only when experiencing symptoms that they associate with hypertension (e.g., headache, nape pain, fatigue) that they submit diary entries.
Types of Data Collected
The textual information submitted fell into six broad typologies: (1) biomedical information about hypertension, (2) perceptions about hypertension, (3) health concerns other than hypertension, (4) key events related to their care pathway, (5) barriers to sending diary entries, and (6) requests for medical consultations. Table 4 provides illustrative quotes for each typology.
Types of Data Generated From the Digital Diaries.

Our objective was to collect in-depth patient narratives. However, most of the entries were limited to participants’ symptomatology, blood pressure readings, and laboratory test results, including cholesterol and blood sugar levels. We had asked them to share their experiences of managing their hypertension, while not imposing our views on what was important, but our open-ended manner seemed to have been interpreted by the participants as inviting them to tell us about their medical status rather than talking about how they felt about the management of their condition in the context of their daily life. The flexibility in our approach may also explain the entries about other health-related matters and why some participants asked for medical advice through the platform, despite being informed that researchers could not provide such advice.
Occasionally, the digital diary was able to capture key events in the pathway as they happened in near real-time, including the stopping of medication and seeking care. Eliciting more about the reasons and motivations for such decisions typically required calling the participants. As described above and in Table 2, this was an effective approach and necessary in cases where researchers had to ask many questions to generate detailed narratives that participants may otherwise find difficult to reflect on and covey via text messages. Some of these themes were followed up in greater depth during a second face-to-face interview. As illustrated in Table 4, Participant 36 decided to shift to an alternative treatment and stop taking medications. In her call log, she mentioned how “…taking medicine can also be costly sometimes since it’s not always free at the [health] center. Another reason is that herbal treatment is more convenient because of my work. I don’t get to visit the [health] center during its operating hours.”
Methodological Insights
Strengths and Weaknesses of Digital Diaries via Mobile Technology
A key strength of the digital diary method, also highlighted by other studies, is its ability to offer near real-time, two-way interaction with participants (Bolger et al., 2003; García et al., 2016). The instantaneous exchange offered by mobile devices allowed us to immediately monitor data quality, ask for elaborations and follow-up on developing issues. In other studies, assessing data quality, including learning about the concerns of the participants about using the platform, if any, happened after diary data collection was completed (Bernays et al., 2019; Jacelon & Imperio, 2005). Assessing the acceptability and appropriateness of maintaining digital diaries among the participants should also continue alongside assessments of data quality, given that participants’ enthusiasm might be tempered, and they might conceal their ambivalence in the research context (Bernays et al., 2019). The instant and two-way interaction with the digital diaries and phone calls also provided us the opportunity to check on participants, especially those who were infrequent or unresponsive users, to repeatedly confirm their interest.
Nonetheless, there are also clear challenges. The method required more time and engagement from both participants and researchers than traditional diary approaches. Initially, researchers were meant to check submissions to the platform once or twice a month, but the initial lack of in-depth submissions meant that weekly checks were necessary. As mentioned above, phone calls were also used to elicit more detailed narratives, but which required much proactive work from researchers. While the platform was designed with the ability to accept diary submissions in many forms, including SMS text, audio voicemail, photo and video message, and file audio messages, changes to the Philippine national telecommunication network after the project commenced meant that it was not possible to receive formats other than SMS text. This highlights one important limitation of the digital diary approach: its dependence on local infrastructure, even if designed to be compatible with basic mobile phones (i.e., not smart phones). There was also a disconnect between the study participants, Filipino researchers, and the UK-based application developers, who did not have the opportunity to test the software directly with the participants, and instead, did so by proxy via the research team.
Having a dedicated platform for digital diaries that uses mobile communications technology also reduces the risk of losing data from devices malfunctioning or being misplaced (Bolger et al., 2003); however, data continuity and confidentiality are key issues with mobile phones. Some participants needed the help of younger family members to submit entries. There were also instances when entries were submitted after changing their mobile phone number or using a borrowed phone from a relative or a neighbor. While the platform is able to receive submissions from unregistered numbers, it was unable to link such entries automatically to the participant’s profile, requiring additional work from researchers to rectify. Even when participants reported phone number changes to the research team, the process of re-registering led to some delays and breaks in the continuity of submissions. A study using mobile phones to promote adherence among tuberculosis patients in the Philippines found that their participants frequently changed their numbers as it is cheap and easy to do (Alejandria et al., 2009).
Shared ownership of mobile devices within households, a phenomenon already noted among the urban poor in the Philippines (Portus, 2008), was another factor that affected the frequency and continuity of diary submissions in cases where spouses working outside the home would take the phone from the participant during the day. A further unanticipated problem was the frequent use of abbreviations in the SMS text messages submitted, which the integrated automatic translation function was often unable to recognize. This added further work for researchers who manually translated these instances from Filipino to English.
While the platform increased the workload for the researchers in the short term, it did prove useful as an efficient means of storing, managing and analyzing participant data in multiple formats (i.e., text/audio entries, interview notes). Our experience was consistent with previous studies that found digital diaries to be a useful component of a suite of methods, rather than as self-standing (Bernays et al., 2019; Gibson et al., 2013; Herron et al., 2019). In our study, the digital diaries complemented the in-depth interviews well as we were able to follow up on themes that emerged from initial interviews and undertake highly personalized follow-up interviews informed by diary data. Data generated through digital diaries do, however, add to the complexity of analysis (Coxon, 1994). Each entry must be seen as a sequential element in an illness narrative, rather than a collection of distinct messages. Information on the illness pathway must also be juxtaposed against events in the participants’ life and changes in the local context. Using digital diaries via mobile phone was also an efficient way to maintain researcher links with participants and minimize attrition rates in longitudinal health research. After a year, we were able to reach 31 out of the 40 participants for a follow-up interview.
Lessons for Future Research
Our experience with digital diaries offers several lessons for those considering this approach. The first concerns the nature of the condition being studied. In our study, the fact that hypertension was not perceived to be a serious and/or chronic condition requiring constant attention, partly due to local conceptions of the illness (Lasco et al., 2020), may have resulted in low levels of engagement. Nonetheless, for situations or conditions that do have a major impact on the day-to-day experiences of participants, digital diaries may provide promising insights from individuals as they deal with symptomatic episodes, chronic pain, stress, or discrimination (Alaszewski, 2006; Bernays et al., 2014; Furness & Garrud, 2010; Hensel et al., 2012; Herron et al., 2019; Sargeant & Gross, 2011). The experiences of OOR using digital diaries in different settings are interesting, but insufficiently documented. For example, in the UK, digital diaries worked particularly well for people coping with the early stages of dementia and its associated stigma. These participants used the platform extensively and the frequent entries received provided rich data (Woodall et al., 2016). But in contrast, for our participants having hypertension did not profoundly interfere with their daily lives, thereby precipitating fewer opportunities for reflection and reducing the insights that might be communicated. The minimal attention that our participants dedicate to hypertension care because of its non-disruptive nature might be the major reason for the lower-than-expected levels of engagement, rather than any lack of interest, commitment or capability, which are usually considered barriers to using diaries for qualitative research (Bolger et al., 2003; Hyers, 2018). Thus, our experience suggests that digital diaries may not be suited to the study of all chronic health conditions.
A second lesson is that designing and using digital platforms for data collection requires an extensive process of co-production, involving software developers, researchers, study participants, and end users—which was particularly challenging given the international composition of our team. Although the research team had a deep understanding of the health systems in the study sites, a prior emic understanding of how participants engage with mobile technology and why would have helped to fine-tune the strategies used by researchers to engage, motivate and probe participants (Bolger et al., 2003; Hyers, 2018), as would have a better understanding of how people communicate about their disease, what they want to share, and when (García et al., 2016; Gibson, 2005). For example, co-production could have revealed important design considerations, such as the preference for different types of entries for different issues (e.g., SMS for factual information, and audio for evolving or emotive issues); and the strong preference some users had for using voice messages via Facebook messenger, despite the widespread use of text messaging. Notwithstanding, researchers in the Philippines expended considerable effort explaining the platform to participants, providing continuous support and adapting processes, which all proved essential to successful implementation.
Co-production is also critical for ensuring that digitally mediated diaries are culturally appropriate. Diaries were understood and expected to contain entries made by a single individual (Coxon, 1994), a view we held at the inception of our research. However, our early data collection experience revealed that mobile phones are often treated as a shared household resource in low-income households, and some participants also relied on family members to help use them. In some ways, this shared ownership facilitated participation, as in our study; but it also raises questions around privacy and confidentiality that must be appropriately considered in the study design. Also as described above, participants may unexpectedly change their mobile phone numbers during the year. Thus, protocols must be in place to address how such changes are handled to maintain contact, data continuity (i.e., with previous diary submission), and the quality of data, especially if digital diaries are to be implemented at a larger scale.
Finally, balancing the need to elicit quality data against the burdening of participants and researchers is an important ethical concern, which was also highlighted by earlier diary studies (Bolger et al., 2003; Ross et al., 1994; Stopka et al., 2004). Despite the added value of being able to conduct prompt quality checks through dialogue between researchers and participants using mobile phones, it is also important not to contact them too frequently and seek excessive clarification. The demands on participants’ time are much higher for digital diaries than when using other qualitative research methods, such as interviews and focused group discussions that last for a specified time. Importantly, diary methods seek to shift the focus to participants as data creators, giving them autonomy over they share and how often, and control over the flow of dialogue—including the decision not to respond at times (Corti, 1993). It is also crucial to determine which groups are best studied to use this method. The participants who engaged more actively were ones who tended to follow through with their treatment. Thus, digital diaries could potentially exclude those facing more challenging health and social situations (e.g., unemployment and lack of family support), or who intermittently access treatment or follow-up within the health system. Even some of the participants who were initially eager were less active later on as their life circumstances changed. In the future, more attention should be spent on recruitment, briefing and supporting all participants throughout the period of engagement.
Conclusion
Digital diaries via a mobile communication platform appear to be a promising means of collecting real-time information and following people with complex chronic conditions. In particular, the ability to maintain two-way interaction between participants and researchers offers the potential to enhance the quality of data obtained over more traditional diary methods, and can complement in-depth interviews to capture the dynamic experiences of patients with a chronic condition like hypertension. However, creating “digital solutions” for data collection is not enough, and such tools must be appropriate to the type of participant, their health condition, and the information sought. Motivating participants to engage with technology-based research methods is a key challenge, and preliminary work, including co-production to understand participants’ preferences, is critical. Researchers also must be given the requisite training and time to maximize the value of the method, using it as one part of an array of methods that elicit different dimensions of patient experiences and behavior in the context of their everyday lives.
Supplemental Material
Supplemental Material, sj-pdf-1-ijq-10.1177_16094069211002746 - Strengths and Weaknesses of Digital Diaries as a Means to Study Patient Pathways: Experiences With a Study of Hypertension in the Philippines
Supplemental Material, sj-pdf-1-ijq-10.1177_16094069211002746 for Strengths and Weaknesses of Digital Diaries as a Means to Study Patient Pathways: Experiences With a Study of Hypertension in the Philippines by Jhaki Mendoza, Maureen L. Seguin, Gideon Lasco, Lia M. Palileo-Villanueva, Arianna Amit, Alicia Renedo, Martin McKee, Benjamin Palafox and Dina Balabanova in International Journal of Qualitative Methods
Supplemental Material
Supplemental Material, sj-png-1-ijq-10.1177_16094069211002746 - Strengths and Weaknesses of Digital Diaries as a Means to Study Patient Pathways: Experiences With a Study of Hypertension in the Philippines
Supplemental Material, sj-png-1-ijq-10.1177_16094069211002746 for Strengths and Weaknesses of Digital Diaries as a Means to Study Patient Pathways: Experiences With a Study of Hypertension in the Philippines by Jhaki Mendoza, Maureen L. Seguin, Gideon Lasco, Lia M. Palileo-Villanueva, Arianna Amit, Alicia Renedo, Martin McKee, Benjamin Palafox and Dina Balabanova in International Journal of Qualitative Methods
Footnotes
Authors’ Note
Portion of this article was presented at the 7th International Jerusalem Conference on Health Policy on September 15, 2019 in Jerusalem, Israel on the topic, “New Challenges and Threats in the Age of Innovation.” The funder had no role in data collection, interpretation and reporting.
Acknowledgment
The authors would like to thank the research participants, as well as the Wellcome Trust/Newton Fund-MRC Humanities & Social Science Collaborative Award scheme for providing funding for this research.
Ethics Approval
The London School of Hygiene and Tropical Medicine Observational Research Ethics Committee and the University of the Philippines Manila Research Ethics Board Panel 1 (Ref: 2017-481-01).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lia M. Palileo-Villanueva has been and/or is currently involved in clinical trials of antihypertensive medications that receive some funding from the industry.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and publication of this article: This study was supported by a grant from the Wellcome Trust/Newton Fund-MRC Humanities & Social Science Collaborative Award scheme (200346/Z/15/Z).
Original Protocol for the Study
Palafox B, Seguin ML, McKee M, Dans AL, Yusoff K, Candari C, Idris, K, Ismail JR, Krauss SE, Lasco G, Majid FA, Palileo-Villanueva LM, Razak AA, Renedo A, Balabanova D. The Responsive and Equitable Health Systems—Partnership on Non-Communicable Diseases (RESPOND) study: A mixed-methods, longitudinal, observational study on treatment seeking for hypertension in Malaysia and the Philippines. BMJ Open 2018; 8: e024000.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.