
Abstract
As healthcare researchers conducting qualitative interviews, we might encounter participants who make remarks or display behaviors which go against principles of valuing diversity, equality and human rights; in other words, remarks and behaviors which could indicate racist, homophobic, xenophobic, islamophobic, sexist, misogynist, classist, etc. views and attitudes. In this article, we offer our reflections on how as researchers we might deal with such situations. We draw on methodological literature and on our own experiences as researchers, educators and practitioners in healthcare, to provide a critical discussion around researcher awareness and anticipation of emotional triggers, management and leadership of research, and understanding of ethics and legal frameworks of equality. We summarize and signpost toward methodological views under which such instances might be considered, including interpretivist and constructivist interpretations, and the concepts of positionality and adversarial discourse. Lastly, we offer practical suggestions for dealing with such occurrences in the context of qualitative research studies in healthcare, and for using researcher reflexivity as a strategy to surface and work through these situations. We hope that this article will provide accessible theoretical and practical guidance, for example to healthcare professionals who embark on their first qualitative interview study as part of a postgraduate course. Equally, we hope that this article will be of interest to more experienced researchers and invite further critical examination of the issues we highlight.
Introduction
I had to pause for a moment. The interview was delivering the type of data we were after: patient experience of being admitted on a hospital ward. The account was rich, in-depth, touching. Mary was a frail elderly grandmother who had suffered a stroke. Her story navigated the extremes of shock when she was told the diagnosis, and despair at the impact of stroke on her body and her prospects for the future. Juxtaposed were moments of hopefulness, when her recovery progressed and treatment was successful; and encounters of kindness from staff, other patients and visitors on the ward, which lifted Mary and made her feel a bit more like a whole person again. And then Mary talked about requesting help from nurses to use the toilet at night. She said that the night nurses were always quite rough with patients. “Most of them are black, you know.” I had to pause for a moment. How to interpret this comment, from one white person to another? After a brief silence, I said that I was sorry to hear about the negative experience and that it was important for us to find out where care could be improved. I delivered my response with an appropriate level of professional empathy and concern, focusing the conversation on the issue of poor nursing care, rather than on what might have been insinuated in stating that most of these nurses were black. I was able to maintain the flow of the interview. There were no further references to skin color. The interview concluded in a cordial manner, with mutual thanks, remarks about the importance of this research, and assurance that Mary would be informed about the outcome of the study. I left with a mental note: There was something there, about how a little remark could provide a peephole through which we might glimpse attitudes, views, opinions that—what would be the word—jar?—raise eyebrows?—make you do a (metaphorical) double-take?—set off alarm bells?—reflect stereotypical judgments, potential prejudice, disdain, or outright hatred? And then,—more importantly—how should I deal with that, as an interviewer doing healthcare research? (Experience recounted by STK; interviewee details have been anonymized.)
Many qualitative researchers will be familiar with what is described here and will have developed their own personal strategies, likely in the context of researcher reflexivity, for handling these types of situations during a qualitative interview. By “these types of situations” we mean moments in which an interviewee makes a remark or displays a behavior which goes against principles of valuing diversity, equality and human rights. For the purpose of this article we use the phrase “discriminatory remarks and behaviors,” which we mean to describe indicators of underlying views, opinions and ideologies such as racist, homophobic, xenophobic, islamophobic, sexist, misogynist, classist, etc. We write indicators because we wish to emphasize the need for nuanced and differentiated interpretation without passing premature judgment and also allowing for misunderstanding and misinterpretation, while at the same time remaining sensitive to these types of remarks and behaviors as signals of possible, probable, or likely underlying discriminatory attitudes.
Discriminatory attitudes are ever present in society and surface very much according to the social situation. A qualitative research interview constitutes such a social situation (Fontana & Frey, 2008, p. 121), and one that can develop a seductive atmosphere for interviewees, through immediate intimacy (Brinkman & Kvale, 2005, p. 162) and “fake friendship” (Duncombe & Jessop, 2012, p. 109) between interviewer and interviewee. An interviewee might therefore lower their usual social guard and voice views which would otherwise not be disclosed to a relative stranger. While there is much methodological literature on qualitative interviewing, little has been written specifically on how to (re)act in such situations as an interviewer. The purpose of this article is therefore to provide reflections and practical guidance, adding to the methodological literature in a way that we hope could be helpful to others.
In writing this article, we drew on our own experiences as researchers, educators, and practitioners in healthcare, as well as relevant literature, to provide a critical discussion and practical suggestions. We would like to preface this by making four points. First, we deliberately focus and reflect on these types of situations solely from the researcher’s perspective. It is probably equally likely that an interviewee might experience the same, i.e. the researcher might cause offense to the interviewee, and this viewpoint equally warrants explicit consideration. In this article, however, we address this issue specifically from the researcher’s perspective. Second, we have focused this article on the qualitative interview method, but the same also applies to other qualitative methods such as focus group discussion and ethnographic observation. We chose the interview, because in our experience this is a popular method for student researchers in healthcare, and we hope that this article will be directly relatable and practically useful to novice interviewers in healthcare.
Third, in this article we refer to research which is broadly situated within the topic area of healthcare, but which does not—on the face of it—explicitly address questions of discrimination, inequality, prejudice, unconscious bias, etc. in healthcare, for which the researcher would deliberately prepare, theoretically sensitize themselves to the issue, and carefully consider in advance their own persona and style of interviewing around the topic (Ford & Airhihenbuwa, 2010, p. S32; Guyan, 2017, p. 3). Rather, we are thinking of studies for which the researcher may enter the field on the (explicit or implicit) assumption that the topic under investigation is unrelated or neutral to issues of discrimination. Although there is a large body of evidence to demonstrate systematic and explicit racism and discrimination in healthcare practice and research (e.g. Ben et al., 2017), such an assumption could perhaps be grounded in healthcare professionals’ codes of conduct, which uphold an expectation of general ethical conduct, valuing diversity, and treating others with dignity and respect (e.g. Chartered Society of Physiotherapy, 2011, p. 11; Nursing & Midwifery Council, 2018, p. 6). When healthcare providers carry out research, their duty of care to their participants as patients often prevails (e.g. Health Research Authority, 2017, p. 14), leading to an overlap of the two roles and their respective responsibilities and loyalties. Moreover, healthcare research is generally conducted with the aim to benefit patients and the public, and there is often a lack of appropriate training for researchers, as research continues to fail to acknowledge the depth of the impacts associated with discrimination in healthcare. Interviewers might therefore view healthcare research as transcending people’s day-to-day differences and taking place in a “benign space” of good behavior and good intentions, removed from any unpleasantness that runs under the surface. This was the scenario we had in mind when writing this article, where, based on this assumption, an interviewer could unexpectedly be given a glimpse of an interviewee’s discriminatory attitude.
Fourth, while one could presume that most frequently encountered discriminatory attitudes concern racism, sexism, homophobia, and other such labeled attitudes, we prefer not to restrict our description to “-isms” and “-phobias.” Instead, we consider that discriminatory views and attitudes are held in multitudes of versions and facets around the world. The nature and relevance of these views will depend on the geographical, historical, cultural, and socio-political setting of the research, and some discriminatory attitudes will only come alive in a specific context. Additionally, these types of attitudes often arise from, or give rise to strong emotion. In this article, we therefore decided to refer to an emotional trigger to describe these unexpected moments, in which the interviewer could be put off balance, caught off guard, or taken aback when realizing the unpleasantness in an interviewee’s words, body language or facial expression.
We have structured this article in three sections: principal frames of reference on researcher emotion, management and leadership of research, and ethics and legal frameworks; how to deal with these types of discriminatory remarks and behaviors in the context of a research study in healthcare; and using researcher reflexivity for working through how we might (re)act in the moment when a research interviewee expresses such attitudes. While we address these aspects in the following sections in turn, there is some repetition of themes, and some threads circle back and forth. This is both deliberate and unavoidable because several facets of the topic link across. Overall, we hope that this article will be helpful to novice qualitative researchers in providing a starting point to considering these issues; and that this article may also be of interest to more experienced researchers, inviting further critical examination of these issues we highlight.
Principal Frames of Reference
In any piece of research, the careful consideration of topic, how the study is to be approached, and the selection of subjects and engagement thereafter is given much emphasis. It is a process that sits with the underlying premise of doing no harm. In some ways this scene is one contrived to create the uneasy balance of sufficient freedom and control to enable the richness of the material studied to be captured—a position whereby the researcher and the researched are to all intents and purposes at one in their focus. In reality there is always an inevitable slight shifting of the sands, which can see the balance of control move between participant and researcher. Yet, as researchers we principally strive to maintain an equilibrium.
But what happens when, despite the best laid plans, a situation arises when the scales become unbalanced and tip to such an extent that the researcher feels their values and ethics are compromised by something that has been voiced by the research participant (a trigger). These are not new challenges but those that play out in daily life; but the question of how to manage self and remain sufficiently neutral creates its own clash. Recognizing the potential for such a situation to arise and identifying the need for a strategy for managing such a situation is key. Although one could argue that there is an implicit understanding of the role of the researcher as a leader, and the explicit expectation that the researcher will strive to ensure integrity of their work, the management of unexpected vulnerability is often given insufficient space. In this section, we therefore outline principal frames of reference in relation to researcher emotion, leadership, research ethics and legal frameworks of equality.
Guyan reminds us that emotion has a place in research (2017, p. 9). We are emotional beings, and so however independent one would like to be in such situations, it is difficult to escape the premise that for every action there is a reaction. In fact, we know that this is not purely a reaction that affects our thinking, but it is also apparent in the body responses (Van der Kolk, 2015, p. 65). The self that is being projected may be that of an unconscious negative frame, a presentation which adds the potential for bias. Our emotional responses may be in some way tied in with our own emotional maturity. Goleman (1996), for example discusses emotional and social components in which our own personal awareness enables the appreciation of our own responses in different circumstances. These are described as self-awareness of one’s emotions, being able to manage such emotions, the ability to keep motivated on goals when managing emotions, and having sufficient empathy to appreciate the perspectives and emotions of others (Goleman, 1996, p. 43).
The inclusion of culture as part of emotional diversity is seen as crucial for developing emotional intelligence capabilities, especially in multicultural settings (Putranto et al., 2018, p. 19). Indeed, the role of culture and emotions within an emotional intelligence paradigm is seen as naturally aligned with the concept of emotional responses, i.e. being intrinsically understood and judged by the culture from which the response emulates (Pathak & Muralidharan, 2020, pp. 5–6). This can be appreciated under a framework of culture specific emotional intelligence. Earley and Ang (2003), for example, developed a construct based on the concept of cultural intelligence, a term seen as relating to the adaptability and response of individuals to new situations, where the interactions are culturally different to themselves. Like emotional intelligence, the model comprises four components of behavior and includes metacognitive and cognitive elements, concerned with being able to create understanding from the cultural signals in individual interactions and meetings, along with motivational and behavioral intelligence—the former relating to a continued drive for improvement, and the latter a behavior component concerned with how people are perceived to act (Ang et al., 2007, pp. 337–339). Perspectives from emotional and cultural intelligence are indicative of the complexities of the interactions of self with others and are an important feature of our daily communication, and therefore also relevant to qualitative interviewing. Earley (2002, pp. 277–279) asserts that individual motivation is central to the ability to be able to grasp an understanding of intercultural communication, and lack of individual impetus in this area results in a failure to achieve such learning. This position highlights the need for an awareness of our own responses.
It could be said that researchers in their preparation concentrate on the doing of the research (that is, its procedural processes) and show less focus on their own emotional responses during the research period or the interview itself. Besides, this also raises the question of who we are as we undertake the research—could it be that we stepped into a leadership position? If we consider leadership as directing a specific endeavor toward a common purpose (Northouse, 2010, p. 3), then are we not also a leader? For some this might feel uncomfortable as they associate the term leadership more with leaders of organizations. But here we pose the need to consider the notion of self-leadership, described as involving a level of autonomy with minimum need for additional instructions from others (Alvesson et al., 2016, p. 22). Whether intentional or not, there is a power dynamic in the interaction between interviewee and researcher that is more than likely to sit with the researcher—a position that is interconnected with notions of power located in structural norms, processes, and relationships, in which societal expectations of power also feature (Buchanan & Badham, 2008, pp. 46–53). Consequently, the researcher must hold responsibility for what happens when they are “in charge.” At the very least an exploration and examination of roles at some level is needed by the researcher, and most certainly a requirement to at least have spent time understanding how we feel ourselves, our own values and what this means for how we might approach and lead the work. In this manner, we also show an appreciation of our own impacts during the research, and consideration for our own ethical conduct.
The path to obtain a favorable ethical opinion might have been an onerous journey, sometimes with iterations of the project plan being submitted before final agreement. When final ethical approval is received, this knowledge that other eyes have had sight of the same offers reassurance that all has been covered. But in dealing with the unexpected triggers mentioned, it is often left to the researcher to consider what to do (Guillemin & Gillam, 2004, p. 269). Faced with dilemmas or difficult conversations that are outside of the scripted research path, there are often the two principal options: to act or not to act. Sometimes this decision is taken out of our hands, and the wider expectations of the organization or the law of the land require a response. Organizations will have their own cultures, norms and practices which dictate expected standards (Schein & Schein, 2017, pp. 10–13) and will instil a set of expected behaviors, which will almost certainly include the need for compliance with regulations and legislation. However, many researchers may be unaware of regulations and legislation, which would identify a gap in essential researcher training and potentially a lack of institutional oversight and accountability.
Let us take for example the protected characteristics of the Equality Act, 2010 in the United Kingdom (UK), which highlights the following areas of consideration (Section 4): age, disability, gender reassignment, marriage or civil partnership, pregnancy and maternity, race, religion or belief, sex, and sexual orientation. It would be the case that effort is made to ensure the researcher does not breach these expectations. Conversely, under this umbrella the researcher could at some level consider the experience of a trigger as being harassment and legally actionable. Harassment is unwelcome behavior that someone finds offensive and is linked to a person’s protected characteristic (Equality Act, 2010, Section 26). The Act identifies a number of behaviors including spoken abuse, physical gesticulations, facial expressions, or banter that is experienced as offensive, all of which could happen in the situation of a qualitative research interview.
In the definition of harassment, anything that is unwelcome is unwanted, and one does not need to have previously objected to it (Equality & Human Rights Commission, 2011, p. 93). This includes actions that cause humiliation, intimidation, or offensive atmospheres. To be unlawful, the treatment must have happened in one of the situations that are covered by the Equality Act, for example in the workplace or when the person is receiving goods or services. Moreover, the unwanted behavior need not have happened in the presence of a person with a protected characteristic. For example: “A manager racially abuses a black worker. As a result of the racial abuse, the black worker’s white colleague is offended and could bring a claim of racial harassment” (Equality & Human Rights Commission, 2011, p. 95).
Ethical and legal contexts provide frames of reference for researchers to consider their conduct in the field. Researchers are required to demonstrate their understanding of these. For example, in research protocols or in research ethics applications, qualitative healthcare researchers commonly elaborate on strategies for dealing with potential safeguarding concerns (i.e. neglect or abuse of a vulnerable person) which might be uncovered during the research (Cronin et al., 2014, pp. 99–115). But it is perhaps fair to say that strategies for dealing with the discovery of potential discriminatory practices are less routinely thought through in this way.
How to Address the Issue in the Context of a Research Study in Healthcare
Following on from these principal frames of reference, we now turn to the question of how the triggers we describe, and the underlying discriminatory views and attitudes they potentially indicate, might be dealt with in the context of a research study in healthcare. In this section we continue the threads of emotion, management, leadership, ethics, and legal frameworks in a non-linear manner and in relation to research governance, methodology and study design.
Researcher’s emotional and mental wellbeing
Perhaps the most straightforward consideration is to offer adequate protection to the researcher. The issue of personal safety is obvious, especially when interviews are conducted by a lone researcher outside the workplace, e.g. at the interviewee’s home. But there is also the risk of more subtle emotional and psychological harm to the researcher, particularly if the trigger connects on an emotional level, for example because of personal experience or a personal characteristic. We consider a situation in which an obvious commonality between interviewee and interviewer (e.g. both are white) might lower the interviewee’s threshold for expressing a certain discriminatory view (e.g. racist toward people from a non-white ethnicity). The interviewee might make a “tester” remark to gauge how their attitude will be received, and from the interviewer’s reaction decide whether to continue or retreat. Or the interviewee might be forthcoming in their views, in a way enveloping and appropriating the interviewer to a discriminatory worldview, based on their obvious commonality. For a researcher with no personal connection to the issue, this might create a moment of social awkwardness or discomfort due to the content of what is being conveyed; but to an interviewer with a personal connection (which might not be obvious, e.g. a white interviewer in a romantic relationship with a non-white partner), this can be detrimental. A study by Dickson-Swift and colleagues (2008) explored emotional and psychological harm to qualitative researchers and provided this testimony from a qualitative interviewer: I think you never really know how it’s going to go, you never really know what the people are going to be like or where it’s going to head. It’s qualitative and sometimes it can go to places where you didn’t think you would go and they can sometimes be very intimate and dangerous, both for you the researcher and for the participants, you can’t really think through all the possibilities. You can never really know exactly the types of things that you as a researcher will be faced with in this type of research…things that really make you think, make you worry, make you sad…you can’t prepare for all those. (Dickson-Swift et al., 2008, pp. 136–137)
Micro- and macro-ethics
Researcher safety and wellbeing are essentially ethical considerations, and ones that are usually addressed without difficulty because they are generally supported by labor and employment legislation. In contrast, the following considerations cross the boundary between scientific rigor, scientific merit and research ethics in dealing with discriminatory views of research participants: The question arises whether these triggers and resulting exchanges during an interview should be picked up upon by the researcher in the analysis; and whether—or in how far—these should be incorporated in the analysis and presentation of findings. Discriminatory comments in interview transcripts constitute research data, and it is the researcher’s decision to either pay attention to these passages of text, or ignore them; to either surface these data by assigning them a code, or not; to either take these data forward through qualitative analysis, or not; to either include these data in the presentation of findings—thereby placing accounts from private life in the public arena (Birch et al., 2002, p. 1)—or not.
These decision-points make apparent the type of leadership enacted by the researcher—in which direction does the researcher choose to take the research. These choices might already constitute uncomfortable lines to cross; but more complexity is added if we consider that qualitative research is often conducted in an iterative manner, letting one interview inform the questioning and probing in the next interview; and conducting interim analyses of earlier interviews to inform the direction of later interviews. Bearing in mind that we are thinking of studies in healthcare which, at face value, are unrelated to any discriminatory “-isms” or “-phobias”: at what point does the researcher decide to not only pay attention to, but to actively inquire into these types of triggers in subsequent interviews? And what are the ethical implications of turning from investigating a benign, uncontroversial healthcare topic to potentially laying bare interviewees’ discriminatory attitudes?
There is an ethical conflict here, between displaying the necessary empathy to establish rapport with the participant, and maintaining a professional distance, as Rubin and Rubin describe: The goal is to achieve some empathy, but not so much involvement that you cannot see the negative things, or if you see them, feel that you cannot report them. A second goal is to learn to go for balance rather than neutrality, that is, you should ask about multiple sides of a story, questioning each interviewee with intensity and empathy. That means that you may have to learn to empathize with different and conflicting points of view, a task that is not always easy. If you find yourself sympathizing with interviewees who are killers, racists, or religiously intolerant, or who are abusing public trust, you might begin to have questions about yourself. The interviewer might wonder, who am I really? Is there a “me” apart from the research roles I assume? Another problem occurs if researchers feel that they have abused a friendship by getting information to use in research and writing. (Rubin & Rubin, 1995, p. 13)
In this context, a helpful ethical framework described by Brinkmann and Kvale (2018, pp. 29–37) makes a distinction between micro-ethics versus macro-ethics. Micro-ethics concerns the relationship within the interview situation, i.e. obtaining the interviewee’s informed consent to participate, ensuring their confidentiality, informing them about the character of the research and their right to withdraw at any time, avoiding harmful consequences to participants, and considering the researcher’s role in the process (Cronin et al., 2014, pp. 99–115). In contrast, macro-ethics concerns the research in relation to society and culture at large, i.e. considering how the knowledge produced will circulate in the wider culture and affect humans and society (Kvale & Brinkmann, 2009, pp. 312–315). A piece of research may present ethical problems or dilemmas on either level. Brinkmann and Kvale (2018, p. 36) relate the example of a study by Adorno and colleagues who used therapeutic interview techniques to circumvent participants’ defenses and identify prejudices and personality traits. Conducted in the wake of the Second World War, the study aimed to give insight into the roots of anti-Semitism. On a micro-ethical level this may be questionable, but on a macro-ethical level it was intended to bring beneficial political and social consequences. Similarly, we might ask ourselves whether it is ethically justifiable to gloss over triggers for the purpose of maintaining a harmonious and uncontroversial relationship within the interview situation, when this means that opportunities to deepen and widen our knowledge about issues of discrimination, prejudice, etc. are lost. Moreover, we might consider research a contributory mechanism for entrenching or silencing issues of discrimination in healthcare, unless researchers decide to surface these data. Topical examples of how research has succeeded in raising awareness of discriminatory practices in healthcare are the mounting evidence of persistent discrimination against black and minority ethnic staff at senior managerial and executive level in the National Health Service (NHS) in the UK (Priest et al., 2015), described in a metaphor of “snowy white peaks of the NHS” (Kline, 2014, pp. 64–65); and concerns about the disproportionally high covid-19 mortality rate among people from black and minority ethnic backgrounds—both in healthcare workers and in the general population in the UK—during the coronavirus pandemic in 2020 (Kar, 2020; Public Health England, 2020, p. 13).
These ethical considerations are not straightforward, and most authors will agree that ethical frameworks, rules, algorithms, or roadmaps provide some guidance but rarely resolve all concerns. There therefore remains the researcher’s responsibility to continuously demonstrate ethical awareness and thinking, and defendable ethical conduct (Birch et al., 2012, pp. 4–6). At a minimum, it would seem to us that data providing insight into participants’ discriminatory views and attitudes should be recognized and coded as an “atypical” category that gives impetus for a further study or publication beyond the original intention of the research (Cook, 2012, p. 337).
Research paradigm and epistemology
Further to the above, we now turn to considering how research paradigm and epistemological assumptions might relate to dealing with these types of discriminatory views in the context of a research study. It is probably fair to suggest that the thinking of qualified healthcare professionals in general aligns more with the quantitative, or positivist research paradigm, because much of medical, nursing, and allied health professionals’ training is grounded in the biomedical sciences. A healthcare professional turned novice interviewer might therefore realize that their initial understanding of the interviewer role is that of an objective and neutral researcher who un- or discovers “the one reality.” However, considerations more in line with interpretivist and constructivist thinking (Fontana & Frey, 2008, pp. 116–118) could be helpful in informing our interpretation of triggers and participants’ discriminatory views in the research data, and we hope to provide some accessible examples to illustrate this. Linking with our thoughts around the researcher as a leader, this will perhaps further highlight that the qualitative interviewer is not an external observer, but that they hold leadership through close involvement and agency in the research.
In an interpretivist approach to the research interview, we are paying attention to how the interviewer might influence the generation of data and the subsequent meaning-making during the interpretation of the data. Briefly, interpretive research seeks to understand social reality and behavior through insights into peoples’ own meaning-making (Given, 2008, p. 464). In this context, we consider how the interviewee’s words and non-verbal communication (i.e. the research data and the understanding and knowledge drawn from it) might be shaped by the interviewer’s characteristics, personality, demeanor, etc. and the values and attitudes which the interviewer projects (Fujii, 2018, pp. 82–89). Portelli (1991) provides an example of this in his account of interviewing the folk poet Trento in the 1970s. Portelli asks Trento to sing examples of local folk songs, and two of the songs are “unmistakably Fascist.” Sometime later, Portelli is surprised to learn that Trento is not a fascist but a communist, and Portelli reflects on how he himself might have contributed to the type of data generated in this interview: Trento didn’t know me, when I first recorded him. His life experience had taught him that he would be safer singing religious, ritual, sentimental, humorous, or conservative songs to an outsider who didn’t look or talk like working-class and who had said nothing about himself. I had thought I was not supposed to “intrude” my own beliefs and identity into the interview, and Trento had responded not to me as a person, but to a stereotype of my class, manner, and speech. I had been playing the “objective” researcher, and was rewarded with biased data. (Portelli, 1991, pp. 30–31)
If we acknowledge that the way the interview situation is being constructed will impact on how it will play out (Mao et al., 2016, pp. 6–7), we can be aware of strategies to minimize any triggers. These strategies could include the conscientious use of non-prejudicial language by the researcher (Arksey and Knight, p. 94), during the interview but also in the lead-up to the interview, for example in information materials about the study, in communication with participants when making arrangements for the interview, etc. In a subtle way, the deliberate use of language sets the tone for the interview. Participants who are sensitive to this will often pick up on these cues and adjust their own language accordingly. Because the meaning of words changes over time and may differ according to the geographical context, it is advisable to consult relevant guidance such as the British Sociological Association’s notes on non-racist, non-sexist and non-disablist language (British Sociological Association, 2004, n.d.). Similar to the conscientious use of language, Arksey and Knight suggest that projecting a “professional” image (e.g. outward appearances) and manner (e.g. authoritative in research skills and subject matter) as a researcher can help to avert potential discriminatory comments, for example sexist treatment of women interviewers in male dominated environments (1999, pp. 137–138).
Further to these embedded strategies, the researcher may also construct the interview situation through a deliberate declaration of what is acceptable, for example through a disclaimer in participant information materials, similar to posters one might see displayed in hospitals which remind that staff will treat all patients equally with dignity and respect, and that staff deserve the same from patients. This approach is perhaps most starkly represented in paid research, which creates an almost contractual situation and power dynamic in which social boundaries and ground rules may not only be announced, but also reinforced by withdrawal of payment from the participant should they overstep. This leads on to the issue of tactics of control and resistance in the power dynamic between interviewer and interviewee which has been discussed in more detail, for example by Cook (2012, pp. 334–336) in the context of research with marginalized groups; and by Kvale (2006, pp. 483–486) who offers a discussion of asymmetrical power relations in contrast to a prevailing view of the “warm, caring and empowering” nature of interview research.
While many authors will emphasize the importance of establishing and maintaining a “rapport” or “good relationship” between interviewer and interviewee (e.g. Keats, 2000, pp. 23–27), there are perhaps other more helpful approaches when the subject matter turns to something discordant, raw, or unpleasant. One example of such a departure from the idealized good relationship is the concept of positionality described by Fujii (2018, pp. 12–34). Here, researchers apply reflexivity to become aware of how interviewer and interviewee see one another. This inter-personal focus involves considering what assumptions they are making about who the other person is, what they are after, or what they might know; and becoming aware of differences in power, social status and privilege between the researcher and interviewee. Rather than seeking to create rapport in the sense of closeness or harmony, the aim is to build a working relationship in which interviewer and interviewee arrive at mutually agreeable terms for interacting and conversing with one another. This can allow them to work together, even if—for example—the interviewee dislikes or disrespects the researcher (Fujii, 2018, p. 15). Further to this inter-personal focus on positionality, the concept is also prominent in critical qualitative methodologies which explore the role of power and social position in the interpretation of experience and the creation of knowledge (Jacobson & Mustafa, 2019, pp. 1–2; Mao et al., 2016, pp. 1–2). Explicit awareness of the researcher’s own social identity(ies) and positionality(ies), and an acknowledgment that the “I” or the “self” of the researcher is situated at the core of the research process, enable the researcher to probe beyond prevailing assumptions and understandings and engage in self-critical reflection on dynamics of power and privilege in the research (Jacobson & Mustafa, 2019, pp. 2–3; Mao et al., 2016, pp. 3–5).
Lastly, departing even further from the idea of the harmonious research interview, Kvale (2006, pp. 486–489) considers agonistic or confrontational interviewing, in which the interviewer deliberately acknowledges and seeks out conflicts in the interview. In the context of discriminatory attitudes, an agonistic interviewer would engage with the trigger, dig deeper, and even challenge the speaker. The understanding is that this interview style will construct a different type of knowledge to an empathetic approach, i.e. it will lay bare conflict and dissensus (as opposed to consensus), mark dividing lines between majority and minority opinions, and potentially advance the formulation of ideas about the topic through adversarial discourse (Kvale, 2006, p. 489). While this agonistic approach—the extreme opposite to empathic interviewing—is a less commonly encountered method and might be more suited to experienced and assured researchers, it is a useful illustration of how agency and leadership of the researcher influence the dynamic and knowledge construction that is taking place during an interview.
Researcher Reflexivity and How to (Re)Act in the Moment
When it comes to (re)acting in the moment when an interviewee expresses a discriminatory attitude, it is helpful to, first, be aware of the possibility of experiencing triggers; and second, to have reflected on possible scenarios and to have prepared some type of action plan. In Figure 1 we have provided questions which can be used by a researcher to increase awareness of their own typical emotions and response patterns to triggers; to increase awareness of ethical and legal frameworks; and to consider their own position with respect to insider/outsider status. The latter refers to a sense of membership or belonging to a group, based on a characteristic such as ethnicity, sexual orientation, etc. (Guyan, 2017, p. 4). It is most helpful to view in/outsider status on a continuum, rather than a dichotomous state; and it is also possible within the same group to be an insider with respect to one characteristic, e.g. ethnicity, but an outsider with respect to another, e.g. socio-economic status (Corbin Dwyer & Buckle, 2018, p. 1). Importantly, there is no principal advantage or disadvantage to being an in- or outsider researcher; rather, it is useful to be aware of and to reflect on the potential benefits and pitfalls of either. An insider researcher for example may garner trust and buy-in from research participants more easily, but they might fail to apply critical depth in their questioning due to assumed shared understandings (Corbin Dwyer & Buckle, 2009, pp. 57–59; Guyan, 2017, pp. 5–11).

Questions to support self-reflection and positionality before conducting qualitative research interviews.
The questions in Figure 1 are developed from our own experience and from literature (e.g. Ang et al., 2007; Guyan, 2017) to draw together aspects of emotional intelligence, positionality, research leadership, and legal and ethical contexts. They are intended to provide a concise starting point for researcher reflexivity with a specific focus on equality and diversity. For further methodological depth and practical guidance, we refer the reader to the wider literature on researcher reflexivity (e.g. Finlay, 2012; Finlay & Gough, 2003), reflective practice models in healthcare (e.g. Fragkos, 2016) and approaches for introducing a critical focus on equality to healthcare and research (e.g. Dunbar et al., 2002; Ford & Airhihenbuwa, 2010; Guyan, 2017). More specifically in the context of critical researcher reflexivity and positionality, Mao et al. (2016) have described the spiral critical reflexivity model, Jacobson and Mustafa (2019) have developed the social identity map tool, and many authors have published illustrative accounts of their own reflective practice (e.g. Berkovic et al., 2020; Carter et al., 2014; Mwambari, 2019; Paragg, 2014) which provide helpful examples to researchers who are relatively new to “doing reflexivity.”
Having completed an initial reflective activity, the researcher may then play through scenarios of how to react to a trigger. In Figure 2 we have compiled a collection of practical strategies which we have used or considered in the past, to keep the interview going or to extricate ourselves if things get too uncomfortable. This list should not be understood as a menu of stock responses; but it is meant to assist readers in observing and comparing their own response patterns and identifying other strategies from their own experience. These strategies represent different degrees of (dis)engagement with a trigger. We take the view that it is not helpful to make judgments on preferred response strategies, or to offer formulaic or algorithmic pathways to (re)acting in the moment. But we suggest that at the beginning of an interview study, researchers should take the time to reflect on these possible responses against the frames of reference we have outlined (researcher emotion, management and leadership of the research, research ethics, and legal frameworks in equality). Whether this is conducted as self-directed activity, as group exercise with peers and supervisors, or as formal researcher training session, we hope that this will support colleagues’ reflective practice and ideally provide greater preparedness for handling triggers in the field.
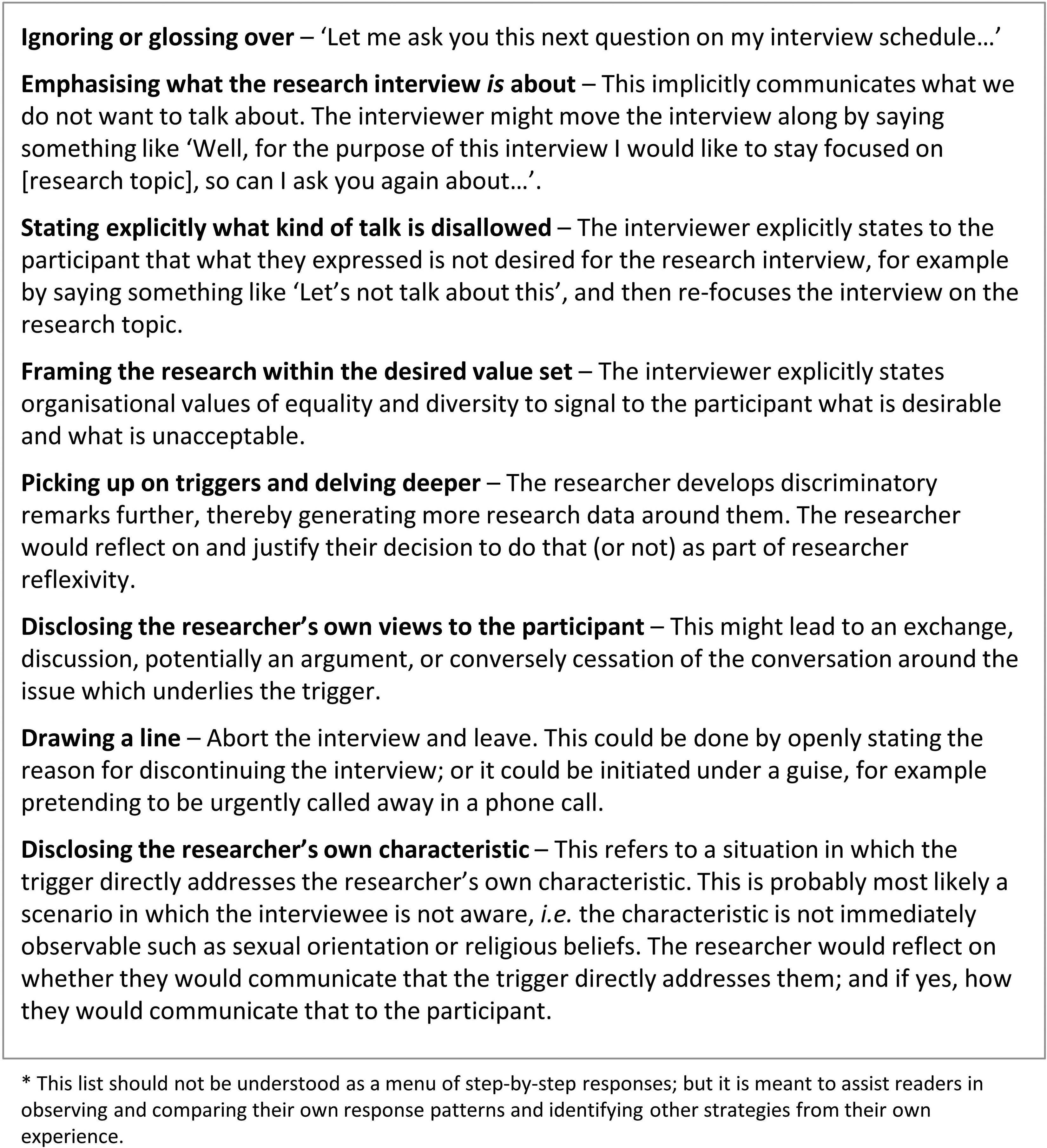
Possible ways to (re)act in response to a trigger*.
Navigating reflexivity in the field
We now turn to an example of how one of the authors (JE) experienced a trigger, leading to reflections on how a researcher should perceive and deal with discrimination in their work setting. This example stems from a research project about knowledge mobilization in healthcare, for which JE conducted key informant interviews with staff (including senior managers and leaders) in selected NHS organizations across the four regions of the UK. JE had been introduced to these interviewees during online meetings and face-to-face at project events and had felt accepted and welcomed to some extent by most. However, during subsequent site visits for one-to-one interviews, it became apparent that there were misconceptions held by some interviewees about her identity and role. She recounts her experience as follows: On every visit, I would be allocated an unoccupied room or office in a convenient section of the hospital for the interviewees to find me. Most of the time, the door would be closed, but there was usually a glass pane—an aperture through which one could peer through. I would be seated with my notes and audio recorder ready on the table and mentally prepare myself to meet the interviewee. The corridor was usually quiet, as a conducive location for good conversation was allocated. I would hear steps approaching, I would look up and often times offer a smile of acknowledgment and expectation. I would often notice individuals glance at me through the glass in the door, but they would often walk past. The steps would continue down the corridor and then return, as I was often the only one about. They would look through the opening again, this time long enough for me to beckon, then open the door and ask: “Are you…………?” or say something along the lines of “Is this where we come for the…………. interview?” The respondents had always been given prior information about the location for the interview. I was more often than not the only person around, but it seemed like I could only be “the one” for a proposed meeting after all offices along the corridor had been explored—perhaps for a more suitable candidate (???) (Experience recounted by JE; details have been anonymized.) Most of the respondents appeared rather curious and inquisitive about my professional background and qualifications for the role I played as an evaluator. Some would further inquire how I came to be in the role, or “how I came to do what I do.” At first, I was very happy to explain and did not give much thought to interviewees’ inquisitive nature and manner. But I soon sensed an undertone that the legitimacy of me in my role as a researcher was being questioned. I began to closely observe the pattern and reflect on it, as it continued to happen in subsequent interviews and organizations. Being of African heritage and dark skinned, I was mildly aware of representing minority ethnicities or being a token of diversity at project events, where almost all attendees were usually white. This was not new to me in the years I have spent working in academia and health research. But now I was beginning to wonder whether my natural appearance had an effect in such a manner that interviewees doubted my competency for the role in the project, or—more fundamentally—questioned my right to conduct interviews with this elite group of senior healthcare managers. I began to consider whether these occurrences indicated unconscious bias and subtle discrimination meted on me as a researcher. (Experience recounted by JE; details have been anonymized.)
Reflecting on her experiences, JE considered the concept of in/outsider status. This appeared suitable, because her view had changed from assuming acceptance into the group (based on initial “official” introductions and friendly incidental conversations with gatekeepers and participants) to experiencing unexpected outsider status. JE reflected that it was unlikely one could exist as a complete insider or outsider throughout the tenure of a research project. In her opinion, a researcher would most likely straddle both at various points of the research, moving from one to the other, but often in a rather fluid manner (Corbin Dwyer & Buckle, 2009, pp. 60–62; Guyan, 2017, pp. 5–11). This reminds us of the concept of identity politics and its subjectivity, in that everyone juggles different identities in order to enjoy the advantage of “belonging.” Also, that an individual’s identity is derived from their experience as well as interpretation of knowledge through the various discourses which they would have been exposed to (Healicon & Sapin, 2006, p. 7).
Research participants tend to develop and hold different views about the researcher’s role and identity, which may surface covert discriminatory attitudes and practices. Being aware and able to understand and recognize issues where they occur, enables the researcher to respond in a calm and measured way. For the purpose of the project in question, JE surfaced her experience of covert discrimination by enacting researcher reflexivity but decided to compartmentalize and set the issue aside during the conduct of the research. Nevertheless, these reflections left a distinct impression and led to further considerations which have influenced the writing of this article.
Conclusion
In summary, we have provided a collection of considerations and practical suggestions on how to deal with discriminatory remarks and behaviors in the context of qualitative interview research. Our article brings together aspects relating to researchers’ awareness of emotion, management and leadership of research, and ethical and legal frameworks. Drawing on our own personal experiences as researchers, educators, and practitioners in healthcare, we hope that this article will serve as a helpful resource. Specifically, novice researchers may draw on the concrete strategies we describe to support their own study or use this article as first literature from which to read further.
Our starting point in developing this article has been a specific situation—the moment when a qualitative interviewer gains unexpected insight into a research participant’s potentially discriminatory attitude or point of view. In addressing this particular experience, we hope that this article will contribute to filling a gap in the literature between methodological texts that are aimed at healthcare researchers but do not explicitly address issues of discrimination; and those texts that originate from and specifically concern the field of equality research.
We would like to conclude our article by encouraging colleagues—students, researchers, academics, educators, and healthcare professionals—to consider how to deal with these types of emotional triggers and discriminatory views, and to do this early in the research process through conversations, exercises and training with supervisors and/or peers. We would like to encourage colleagues to raise awareness and support reflexivity around emotional triggers and discriminatory views, by incorporating these issues into education and training (e.g. in the teaching of qualitative research methods) and into the usual research processes (e.g. making it an explicit point of attention for reviewers of research proposals and ethics applications). Lastly, we encourage colleagues to emphasize that interview content around emotional triggers and discriminatory views constitutes important research data. It is up to our research management and leadership to unpack and develop these data and in this way further these aspects of our knowledge.
Footnotes
Authors’ Note
Kulnik, Egbunike, and Francois contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.