
Abstract
Research networks have significant value and are essential for conducting high-quality applied health research. In this article, we describe the establishment, content, and contribution of a Danish national qualitative interpretive description (ID) network. There are only a few examples of clinical research networks and in most qualitative research methodology is not highly prioritized. Still, a number of nurses and allied health professionals work with qualitative methods and applied health research. This may call for different kinds of networks depending on the geographical context, management support, background, and goal of the network. In this article, we share our knowledge of different kinds of networks and in particular our experiences with an ID knowledge-creating network. The network has provided us with results in the form of stimulating professional conversations and discussions. It has also strengthened the methodological depth of our research and the epistemological standpoints.
What Is Already Known?
Participating in research networks is meaningful and necessary in order to strengthen collaboration. Transferring knowledge from research to practice is one of the most difficult and important issues. Clinical research networks on qualitative research are rare. Research networks are essential for conducting high-quality applied heath research
What This Paper Adds?
Researchers with the ambition to provide applied clinical research are challenged. A knowledge-creating network inspired by action learning can create collective learning among researchers Practical considerations are important in establishing a network and ensuring a trusting relationship. Stimulating professional conversations and discussions on how to provide meaningful clinical practice research is useful in knowledge sharing and helps researchers to achieve methodological depth.
Introduction
Application of research and employment of health researchers with an allied health professional in clinical practice is new in many countries, including Denmark. The general picture is that those working in clinical practice settings are often the sole (nurse) researchers in their departments (Banner, Janke, & King-Shier, 2016; Berthelsen & Hølge-Hazelton, 2017; McGill Qualitative Health Research Group [MQHRG], 2018). To our knowledge, only a few examples of interdisciplinary clinical research groups exist where qualitative research methodology is prioritized (Banner et al., 2016; MQHRG, 2018. However, a number of nurses and allied health professionals work with qualitative methods and applied health research.
In 2015, we established a knowledge-creating network, “the interpretive description (ID) network.” The ID network has a common interest in strengthening applied health research in nursing supported by the research methodology ID (Thorne, 2016). This article describes the establishment, content, and contribution of this Danish national research network, focusing on the ID knowledge-creating network and applied research.
The inspiration to write this article came from our presentation of the network at the “15th Qualitative Methods Conference in May 2016.” The topic of the conference was collaborative approaches to research including diverse experiences, issues, and success stories. The take-home message from our presentation was that our experiences with establishing the research network were worth sharing with an international audience and that research networks are essential for conducting high-quality applied health research.
Research Networks and Knowledge Creation
Being part of a research network is meaningful and necessary in order for a researcher to gain new insight, establish new relations, increase competencies, and strengthen collaboration between otherwise-divided actors (Thomas, Griffiths, Kai, & O’Dwyer, 2001).
Researchers engage in different kinds of networks. Some are well established and formal; others are informal and ad hoc. According to Katz, Lazer, Arrow, and Contractor (2004), there are common features for all kinds of research networks, even though they may have different aims. First, a research network is a set of actors and their relations. Secondly, the members of the research network share common interests. Thirdly, together with a specific aim, the overall aim of a research network is to create synergy between the competencies and members’ resources in the network process (Katz, Lazer, Arrow, & Contractor, 2004).
Different research networks have different aims. One aim could be to increase the network members’ competencies in a specific area, for example, by engaging and training network members in research (Thomas et al., 2001). Another aim might be to enhance collaboration between different actors, such as a “collaborative practitioner research network” (Lunt, Ramian, Shaw, Fouché, & Mitchell, 2012). Another type of network is the knowledge-creating network where the aim is to create knowledge within a particular practice area and to share that knowledge with others (Büchel & Raub, 2002). Studies show that knowledge-creating networks give rise to positive knowledge-sharing that goes beyond the common interest of the networks (Ramian, 2016).
Büchel and Raub (2002) describe four different kinds of knowledge-creating networks: (1) professional learning networks, (2) hobby networks, (3) best practice networks, and (4) business opportunity networks (Büchel & Raub, 2002). Table 1 describes the aim and characteristics of the different knowledge-creating networks. The ID network is a professional learning network, and the choice of ID as the focal point in our network was not coincidental. We were interested in discussing the potential and usefulness of ID. This was not only for the sake of our own interests as qualitative health researchers engaged in applied research. It was also because we felt that ID was particularly good at facilitating conditions that can support engagement and linkage between knowledge producers and knowledge users in clinical practice; a role sometimes described as “knowledge brokers” or “knowledge mediators” (Dagenais, Laurendeau, & Briand-Lamarche, 2015).
Knowledge-Creating Networks: Aims and Characteristics.a

ID and Applied Research
The research methodology ID (Thorne, 2016) takes its starting point in clinical practice. ID is a qualitative inductive research methodology developed by Dr. Sally Thorne (Thorne, Kirkham, & MacDonald-Emes, 1997). ID is described as a generic qualitative approach (Kahlke, 2014), as it challenges the necessity of following the rules and structure of specific qualitative methodological traditions and instead strives to generate “usable” knowledge (Thorne, 2016). The emphasis on generating knowledge that will be meaningful and relevant to the context of applied practice is essential. This means that qualitative health research must answer questions that arise from practice and that research must be helpful for nurses and nursing clients. Hence, ID seeks to reach out and describe the complexity of clinical practice to develop meaningful and essentially useful new insights (Thorne, 2016).
ID in particular aims to answer questions that have a direct relevance to everyday life in the clinic, thereby providing evidence-based answers applicable to clinical practice (Thorne, 2016). Still, the clinical application of research in practice is a difficult task (Pentland et al., 2011) though important for the legitimization and acceptance of the practice of applied health researchers such as both clinical nurse researchers and other staff and leaders. Therefore, it was highly relevant for researcher and knowledge users to investigate ID’s distinctive capacity in relation to the above as well as the advantages and disadvantages of using ID.
Now, we have positioned professional learning networks within the larger context of how networks operate and explained why ID constitutes a particularly relevant methodological focus for network development. In the following, we describe how we developed and structured our ID network. Moreover, we will present some critical reflections on how the network has contributed to our professional work as qualitative researchers.
The Heartbeat of the ID Network—Establishment and Content
How the Network Began
The network was established when some of the later members realized that a number of studies from the applied research field in Denmark used ID as a methodology and source of inspiration (Bregnballe, Schiotz, & Lomborg, 2011; Handberg, Lomborg, Nielsen, Oliffe, & Midtgaard, 2015; Handberg, Nielsen, & Lomborg, 2014; Jensen, Lomborg, Langdahl, & Wind, 2016, 2014; A. N. Olsen, Bradley, Lomborg, & Nortvedt, 2013). We had a mutual or collective interest in applied health research and the ID research methodology, which is often a reason to create a network (Katz et al., 2004). We invited other researchers to the first network meeting. Besides being a researcher, the only condition for participating in the network was a serious interest in ID and applied research. At this point, the primary aim of the network was to discuss ID, but it appeared that the meetings generated space for much more than methodological issues related to ID.
Seven persons constituted the ID network, and the first network meeting was held in August 2015. The participants were junior and senior researchers with different kinds of employment positions at hospitals and universities. We came from all over Denmark and had both formal, affective and proximity ties to each other (Katz et al., 2004), which could be strong (such as long-term friendships) or weak ties (such as acquaintances). All members had at least one strong tie to another member in the network. Even though other professionals were welcome, we started out as a nurse-only network. In relation to ID, two of the members had performed ID studies (Handberg et al., 2015; Jensen, 2014), one had just started an ID study, and the rest of the members had performed other kinds of applied qualitative research projects (Kjerholt, Wagner, Delmar, Clemensen, & Lindhardt, 2014; Soelver & Krogsgaard, 2016; Thomsen & Holge-Hazelton, 2016).
The Meetings
The network meets once every 4 months and spends the day together. Prior to the meetings, two or three of the network members draft an agenda. Each meeting, except from the first, generates the overall agenda for the next meeting. We always end up with unsolved topics with need for room for further debate. The agenda outlines different topics to be analyzed and discussed, as well as expectations to the specific preparations required of the network members for the next meeting. Preparation for the first network meeting was to read five articles describing Danish studies including ID as a part of their methodology. One member prepared a presentation concerning challenges in applied research from an ID perspective. Box 1 is a glance at how discussions can take place during a network meeting.
Action and Outcome: A Short Glance at a Discussion of Applied Research Based on ID Studies and Danish ID Studies—Meeting, August 2015
The meeting started with a presentation by one of the members, who kick-started a debate concerning the particular aspects of applied research based on interpretive description (ID) strategy, as this is outlined as one of the core element of ID. Thorne (2016) states that an ID study must provide knowledge that is helpful for nurses and nursing. How is this different? Examples and experiences with other kinds of qualitative research strategies and traditions were discussed, for instance, Hammersley and Atkinson (2007), who describe that “the immediate goal of ethnography should be the production of knowledge—rather than for example, the improvement of professional practice” (pp. 368-376). The debate concluded that the consequence of this means that results created in an ID study can never be value-free. A member of the network drew the other members’ attention to the work of Risjord (2010), who claims that professional disciplines have a value orientation that academic disciplines lack. Subsequently, we uploaded the chapter from Risjord’s book in the common Dropbox ID folder and returned to it on several of the subsequent meetings.
Following lunch, another theme which one of the members had struggled with was brought up for discussion: “Can you call it an ID study if the study does not lead to ‘meaning’ or specific purpose in clinical practice?” and Does this define a limit for ID studies? The Danish ID studies we had read and looked into all emphasized that an ID study aims to produce knowledge applicable to clinical practice. In line with this, the research questions, for example, to describe male cancer survivors’ barriers toward participation in cancer rehabilitation as a means to guiding future targeted men’s cancer rehabilitation (Handberg, Lomborg, Nielsen, Oliffe, & Midtgaard, 2015), all highlighted the importance of having implications for clinical practice. Was this an argument against the use of ID design in a theoretical or philosophical nursing study? Furthermore, if providing clinically relevant knowledge is an essential element of the ID design, does this lead to an adverse effect on the result because one has to end up with clinically relevant knowledge? One of the group members described how, during an ID study, she constantly reminded herself that the result should be helpful for nurses and nursing clients. This led her to deselect interesting findings which meant less application to the clinical context. Therefore, we debated if this is a condition for conducting an ID study then it places a limitation on ID studies, which must be accounted for in the description of study limitations. Some of the members of the network pointed out papers that were critical of ID, for instance, the paper by Hunt (2009), which debates strengths and challenges in the use of ID. This and another critical article were then uploaded in the common Dropbox folder after the meeting (Berterö, 2015; Hunt, 2009).
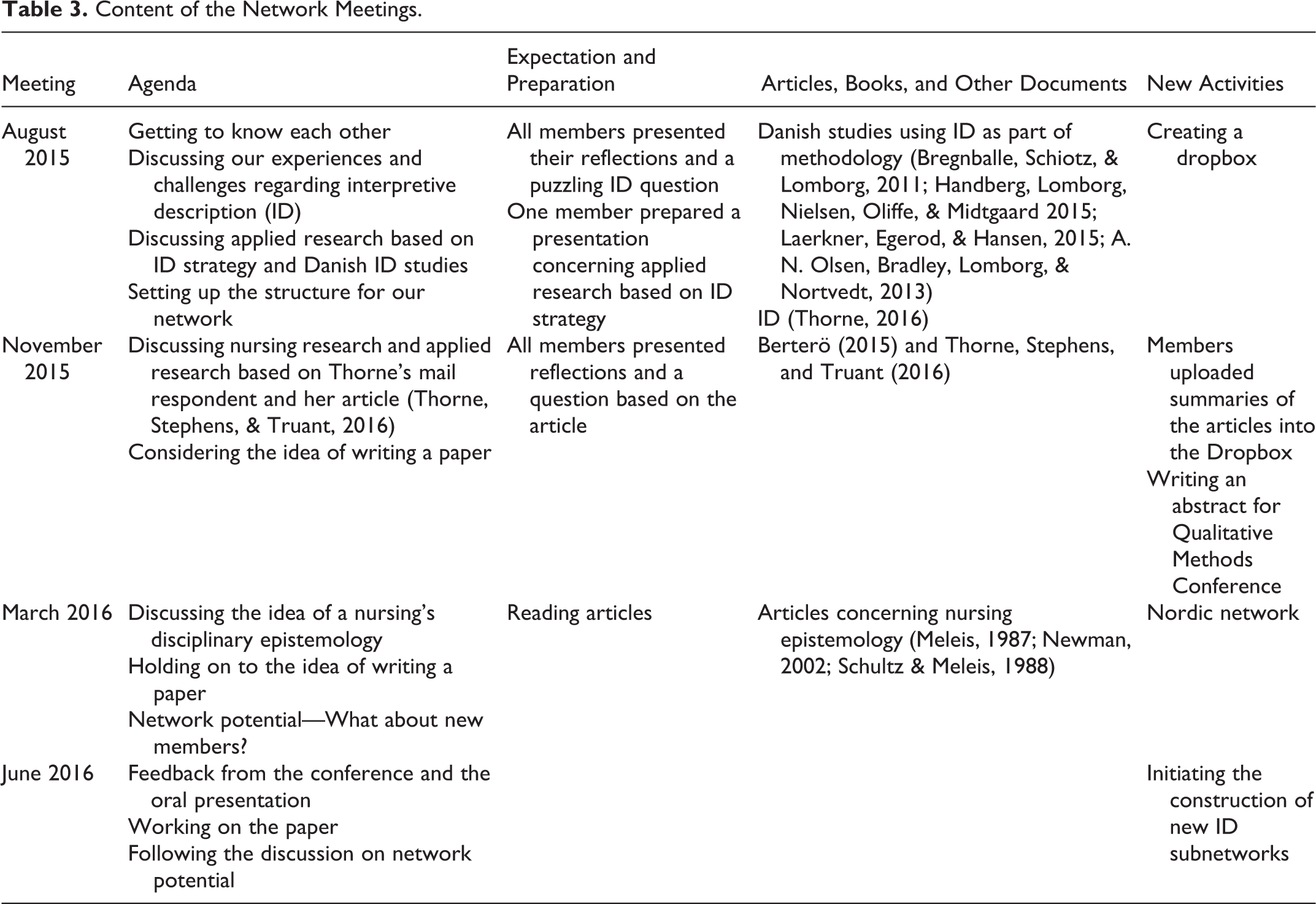
Overall, our meetings and discussions are explorative and stimulating and inspired by experiences from action learning and action research (Kjerholt, Wagner, Lindhardt, Delmar, & Clemensen, 2016; P. R. Olsen & Hølge-Hazelton, 2016; Thomsen & Holge-Hazelton, 2014). Action learning was well-known in health-care practice as an approach to the development of, for instance, clinical nursing practice (Wilson, Mccormack, & Ives, 2008). Action learning is a collective term for practical approaches and methods to create learning in and about clinical practice. It is characterized by studies in inquiry-based learning and reflections in relation to, for example, the participants’ actions and practices and by learning groups with specific parameters and voluntary participation (Wilson et al., 2008). Further descriptions of our network activities and the content of the network meetings from August 2015 to June 2016 are outlined in Tables 2 and 3.
Meetings and Conference Activities in the Danish Interpretive Description Network.

Content of the Network Meetings.
Between Meetings
At the end of a meeting, we always have questions or dilemmas that need further discussion. In the group, we have different experiences and methodological approaches to qualitative research and thus different interpretations of ID. One of the group members had a formal relation to Dr. Sally Thorne. We therefore wrote and posed some of the questions to her. For instance, during a meeting, we debated the term “noncategorical theory” and how ID’s goal was not theory development. Another example of questions is from our November 2015 meeting where we discussed the paper: “Building Qualitative Study Design Using Nursing’s Disciplinary Epistemology,” written by Dr. Sally Thorne, Stephens, and Truant (2016), published in the Journal of Advanced Nursing. The discussion on the paper took us further into the perspectives of the epistemology and ontology of nursing. We found some answers in the article (Thorne, Stephens, & Truant, 2016). Again, after some long and intriguing discussions, we e-mailed a number of unanswered questions regarding these issues to Dr. Thorne. We wondered if a specific definition was available or possible. Therefore, we asked “Is there (or do you use) a specific definition of nursing epistemology?” In her reply, Dr. Thorne (2015) informally described some of her ideas regarding an epistemology of nursing and she referred to the editorial published in nursing inquiry. Furthermore, she encouraged our network to take on the challenge of trying to write something about “what that core disciplinary epistemology of nursing would be in scaffolding good qualitative studies.”
Thus, on several occasions, our informal communication with Dr. Sally Thorne contributed with some fascinating answers or new perspectives on our questions and puzzles, which we used for fruitful discussions at our next meeting. This highlights the idea that networks can communicate with other researchers or networks by asking questions or inviting them to debate ideas and perspectives.
Contribution of an ID Network
Our network across the country has resulted in this inspiring collaboration giving us the opportunity to share, discuss, and develop knowledge. A consequence of seeking challenges and developing clinical practice through research may expose you as a researcher. Therefore, it is essential to build trust in a network (Büchel & Raub, 2002). In our network, we believe we have a space to share these experiences, and we agreed on confidentiality in the group. We all have a professional background in nursing, and we all conduct qualitative research and consequently a kind of shared understanding. Therefore, despite different positions and institutional affiliations, the network has established a forum where ID has been a theme throughout our discussions of theory as well as pragmatic approaches to research and developing clinical practice. By doing so, we have established a forum allowing us to share and debate issues of power in a context free from competition. In other words, our network was founded in a noncompetitive environment, with the aim of sharing perspectives and creating knowledge on ID and developing clinical practice. Furthermore, equality was also strengthened because our meetings have been organized by rotation to take place in different parts of the country, providing equal opportunities (in terms of time and transport expenses) for members to attend the meetings. We have learned that practical considerations are important in establishing a network. It is an ongoing process, and the practical considerations include how to ensure a trusting relationship, how to decide on which kind of leadership is needed, and when and how to include new members in the network. In our network, we did not elect a formal leader or a network coordinator. Instead, we all contributed to leading the development of the network and coordinating meetings. We have still been able to establish a well-functioning professional learning platform, but larger networks and other kinds of network often require clear leadership and a network coordinator (Banner et al., 2016; Büchel & Raub, 2002).
Our meetings and discussions were inspired by action learning and characterized by learning together by collective discussions and reflections in relation to our practical work and studies (Wilson et al., 2008). In the light of this, the aim of our network has evolved during the first year. The aim is no longer “only” to discuss ID and methodological issues. Our meetings created space for much more, for example, a discussion on “the idea of a nursing epistemology” (Table 3). Furthermore, the meetings gave rise to reflections individually in-between meetings, and we shared our reflections with each other by e-mail, which again gave rise to collective discussions. In this way, the action learning approach initiated a continuous reflection and discussion circle and thus developed our knowledge about ID and other issues in relation to our work.
In our work, we are challenged researchers, whose ambition is to provide meaningful clinical research. By establishing this network and from the discussions at the meetings, we found that we share several challenges: (1) We meet methodological challenges when we focus on research occupied with changes in practice and implementation of changes. Box 1 provides an insight into this challenge. (2) We depend on collaboration with practitioners, and at the same time, our research can be challenging to existing practice. Hence, nursing researchers who are conducting qualitative applied research in clinical practice can experience considerable pressure. This resonates well with a case study of nurse researchers’ experiences of working with research and development culture in clinical practice: “Caught between a rock and a hard place” (Berthelsen & Hølge-Hazelton, 2017). (3) We use other methods and analysis strategies than most of our researcher colleagues. (4) We are occupied with applying research in clinical practice, which is not common for traditional biomedical researchers but is a core element in ID research methodology to “serve the knowledge need of the discipline.” Being part of the ID network has provided us with energy to meet this challenge, but also with arguments for doing ID studies, which shapes the sensibility of practice context and thereby becomes clinically relevant (Thorne, 2016).
Overall, the content of our meetings and discussions founded in ID has taken us far in literature evolving around ID and nursing epistemology in general. This includes reflections regarding the interconnection between research, development, and implementation, including our roles as knowledge brokers. Furthermore, presenting and discussing our experiences regarding the network at the Qualitative Methods Conference in Glasgow 2016 and the drafting of this article are additional products of our network. Another outcome is the initiation of a Nordic ID network meeting, which has resulted in the establishment of a Nordic ID network group. Individually, a larger part of the group members is now conducting ID studies and they are head supervisors for ID studies (e.g., PhD studies and other kinds of qualitative research studies) or teaching in the ID methodology at the university. Therefore, we are also hosting a meeting with focus on the new ID studies, where PhD students and other researchers are invited to participate. Furthermore, we are hosting a 1-day conference on applied health research and ID methodology in the near future. In order to strengthen the Nordic ID network group, our plan is to host a Nordic network meeting within 2 years.
Conclusion
We have shown that our collaboration is fruitful in many ways every time we engage in stimulating professional conversations. Professional learning networks like ours provide a platform for facing the challenges of and developing the competencies required by clinical researchers. One goal is to gain knowledge to develop the methodological depth in our research, to strengthen the epistemological standpoints, and to understand the underlying layers of our research.
Still, as one of the members of the network described the collaborative spirit of our network: “The ID network is like a little sprouting seed, we need to nourish and maintain it.” This means the shaping of our network is never-ending, since networks by nature are highly dynamic and change over time.
Footnotes
Acknowledgment
We would like to thank Dr. Sally Thorne for taken the time to go into dialogue on our questions and to elaborate her fascinating perspectives on interpretive description. It has resulted in the possibility to take our discussions a step further.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.