
Abstract
Focus groups are a useful data-generation strategy in qualitative health research when it is important to understand how social contexts shape participants’ health. However, when cross-lingual focus groups are conducted across cultural groups, and in languages in which the researcher is not fluent, questions regarding the usefulness and rigor of the findings can be raised. In this article, we will discuss three different approaches to cross-lingual focus groups used in a community-based participatory research project with pregnant and postpartum, African immigrant women in Alberta, Canada. In two approaches, we moderated focus groups in women’s mother tongue with the support of real-time interpreters, but in the first approach, audio recording was used and in the second approach, audio recording was not used. In the third approach, a bilingual moderator facilitated focus groups in women’s mother tongue, with transcription and translation of audio-recorded data upon completion of data generation. We will describe each approach in detail, including their advantages and challenges, and recontextualize what we have learned within the known literature. We expect the lessons learned in this project may assist others in planning and implementing cross-lingual focus groups, especially in the context of community-based participatory research.
Keywords
Introduction to Cross-Lingual Focus Groups
Focus groups are a data generation strategy in qualitative research in which researchers foster discussion among participants while paying close attention to the group interaction (Barbour, 2013; Mayan, 2009). Hennink (2007, p. 4) describes that the essential purpose of focus groups is “to identify a range of different views around the research topic, and to gain an understanding of the issues from the perspective of the participants themselves,” allowing researchers to capitalize on the richness and complexity of group dynamics (Kamberelis & Dimitriadis, 2011).
This strategy of data generation has been increasingly used in public health research and practice as a way to develop knowledge, attitude, and practice surveys; assess community health; enhance health promotion and education strategies; and investigate the social context of various health behaviors (Yelland & Gifford, 1995). In particular, focus groups are useful in health services research with minority groups, such as immigrants, “whose voices have been otherwise muted” (Barbour, 2013). When discussions occur in a nonthreatening, nonjudgmental setting, participants who historically have had limited power may feel more comfortable, and assured, about sharing their social constructions of health with peers and researchers (Barbour, 2013; Hennink, 2007; D. L. Morgan & Krueger, 1993; Umana-Taylor & Bamaca, 2004).
Using focus groups to explore how social context shapes immigrants’ health experiences is of particular relevance in Canada—the industrialized country with the highest immigrant population among the former Group of Eight (G8) nations (Newbold, 2005; Statistics Canada, 2013). In 2011, 20.6% of Canadians reported a mother tongue—defined by Statistics Canada (2015) as the first language learned by a person at home in childhood—other than English or French, and 80% of the population who preferred speaking an immigrant language at home lived in one of Canada’s six largest censuses metropolitan areas (Statistics Canada, 2012, 2013). This linguistic diversity poses challenges to health researchers that go beyond effective communication, as they also need to understand how different cultures use language to express their perceptions and experiences of health and disease (Wallin & Ahlstrom, 2006). Therefore, understanding how cross-lingual and cross-cultural communication influence interpersonal exchange, and participation, in focus groups is crucial to the usefulness and rigor of qualitative findings (Esposito, 2001; Graffigna, Bosio, & Olson, 2008).
When cross-lingual focus groups are conducted in languages in which the researcher is not fluent, two main approaches are commonly used for data generation (Barbour, 2013). Before outlining these approaches, it is important to define some of the words that are frequently used in this subject area. An interpreter translates back and forth between one or more individuals, whereas a translator works with recorded material, translating from one language to another (Wallin & Ahlstrom, 2006). For research purposes, translation is described as the transfer of meaning from participants’ mother tongue language to the study language, frequently English (Choi, Kushner, Mill, & Lai, 2012; Esposito, 2001). As such, translating from one language to another is a complex process as words carry sociocultural and political values that may not be captured through literal meaning (Hsin-Chun Tsai et al., 2004; Kapborga & Bertero, 2002). Consequently, both interpreters and translators not only enable cross-lingual research but also facilitate researchers in understanding the nuances of participants’ cultural beliefs and practices.
One technique for conducting cross-lingual focus groups involves a real-time interpreter who translates participants’ responses to the moderator (i.e., researcher) as the discussion occurs (Barbour, 2013), as shown in Figure 1. This allows the researcher to take an active role in data generation and in influencing the direction of focus group questions. Yet, the researcher relies on the real-time interpreter’s understanding of focus group questions and their ability to translate the meaning of participants’ answers and comments as discussion happens.
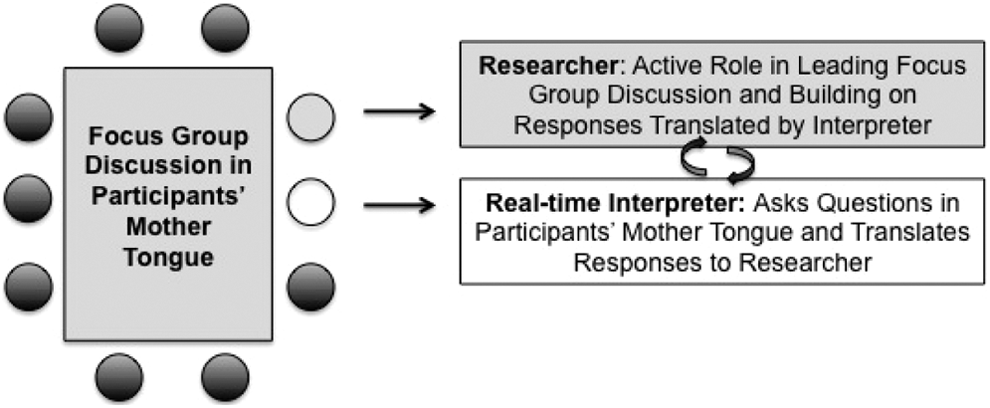
Interpreter-assisted focus group moderated by the researcher.
Another technique involves employing a bilingual moderator who conducts the focus group discussion in participants’ mother tongue (Barbour, 2013). Following the discussion, the bilingual moderator uses the audio recording to translate conversations into the research language (Choi et al., 2012), as illustrated in Figure 2. In this case, researchers rely solely on a bilingual moderator to generate meaningful data (Umana-Taylor & Bamaca, 2004).

Focus group moderated by bilingual moderator followed by translation.
Regardless of how cross-lingual focus groups are conducted in participants’ mother tongue (i.e. bilingual moderator or real-time interpreter/moderator), researchers need to take into account, and address, any communication issues that may affect data quality, including (1) translation across languages and (2) the importance of working with a real-time interpreter or bilingual moderator who understands participants’ social context, cultural background, and language. If not properly addressed, these issues may threaten the validity of focus groups’ data and, consequently, overall rigor of the qualitative research project (Choi et al., 2012; Esposito, 2001; Yelland & Gifford, 1995).
This article outlines our experience conducting cross-lingual focus groups with immigrant women in Alberta, Canada, using three different approaches: (1) a real-time interpreter with audio recording, (2) a real-time interpreter without audio recording, and (3) a bilingual moderator followed by translation. Focus groups were the data generation strategy that worked best with our participating communities. However, we expect that the information presented here will assist researchers engaged in cross-lingual, cross-cultural research in not only selecting the most suitable approach to focus groups but also planning for other methods of data generation, such as interviews and group interviews.
Current Study: Investigating New African Immigrant Women’s Experiences During Pregnancy and Postpartum in Alberta, Canada
Low socioeconomic status, language difficulties, and sociocultural barriers can negatively affect many aspects of a healthy pregnancy, including dietary practices, physical activity, and women’s receptivity to prenatal and postpartum care (Berggren, Bergstrom, & Edberg, 2006; Gagnon et al., 2009; Paul, Graham, & Olson, 2013; Small et al., 2008; Urquia et al., 2010). In a recent qualitative investigation of low-income, pregnant women living in Rochester (NY), multiple socioecological factors (e.g., stress, poor access to healthy foods, low social support, etc.) were found to put them at increased risk of excessive gestational weight gain and poorer pregnancy outcomes (Paul et al., 2013).
In Canada, refugee and nonrefugee women (hereinafter called immigrant women) often have unmet social, economic, and health needs during pregnancy and postpartum and poorer birth outcomes (Gagnon et al., 2009). Given all the adaptation that migration requires, and the importance of pregnancy for women and infant’s health, we sought to understand immigrant women’s perceptions of a healthy pregnancy and their experiences during pregnancy and postpartum while receiving support from a community-based organization, the Multicultural Health Brokers (MCHB) Co-operative, in Edmonton, Alberta.
The MCHB is an independently run health worker (i.e., health broker) cooperative that provides perinatal services and supports to at-risk immigrant women. The MCHB offers women holistic, strategic services that expand beyond a single health concern, (e.g., low birth weight or premature birth) and include actions related to housing, income, food security, and women’s education, in other words, overarching social determinants of health (Torres, Spitzer, Labonte, Amaratunga, & Andrew, 2013). The overall goal of health brokers is to contribute to immigrant women’s successful settlement, adaptation, and integration into Canadian society, and, as a result, improve their pregnancy and birth outcomes.
A Community-Based Participatory Research (CBPR) approach was used to engage African immigrant women who participated in a perinatal group offered through the MCHB. CBPR represents a viable approach for working with minority groups and addressing health disparities that affect people living in marginalized communities (Israel et al., 2010; Minkler & Wallerstein, 2008). Focused ethnography was the qualitative research method used in this study. This method is sensitive to how culture shapes, and possibly explains, women’s everyday lives and health behaviors in the perinatal period (Graham et al., 2013; Higginbottom, Pillay, & Boadu, 2013; Knoblauch, 2005). Parallel to traditional ethnographic research, in focused ethnography, the attention to culture remains; however, it is more contained to a particular setting or focused on certain issues and within a shorter time frame (Graham et al., 2013; Knoblauch, 2005).
We introduced the project to the group of health brokers connected to immigrant communities through MCHB, and those who were interested in better understanding the sociocultural context where their clients experience pregnancy and postpartum agreed to participate, and engage their communities in the research. Thus, over an 8-month period, we established a meaningful partnership with health brokers from four African communities in Edmonton (Eritrean, Ethiopian, Oromo, and Somali) and their clients, that is, African immigrant women (Minkler & Wallerstein, 2008). The health brokers from these four communities became partners in this study (Minkler & Wallerstein, 2008). They determined, alongside the researchers, focus groups as the preferred data generation strategy and advised on which questions to pose (Israel, Schulz, Parker, & Becker, 1998; Minkler & Wallerstein, 2008).
We opened the first focus group with women with a general question of what it meant for them to be healthy during pregnancy and postpartum. Women then began to express their perceptions and experiences of health during pregnancy and postpartum by contrasting their countries of origin and Canada, which were, respectively, described as “back home” and “here.” After each focus group, researchers and health brokers discussed what questions had been explored with women and what questions or topic areas had yet to be examined in following focus groups with each participating community. We engaged health brokers’ in these discussions as a key principle of CBPR and in an effort to better understand women’s cultural backgrounds, social contexts, and preferred ways of sharing their stories.
Ten focus groups (n = ∼8 women per group) were conducted with women from the above-mentioned African communities who had been living in Canada between 1 and 36 months. Women and health brokers from these communities spoke diverse languages and dialects. Therefore, the composition of focus groups, and approach to each cross-lingual focus group varied, with health brokers actively participating either as real-time interpreters (Eritrean, Ethiopian, and Oromo) or as a bilingual moderator (Somali). Although real-time interpreters facilitated focus groups with Ethiopian, Eritrean, and Oromo women, the approach to focus groups among these communities differed in relation to data recording. Focus groups with Ethiopian and Eritrean women were audio recorded, whereas those with Oromo women were not audio recorded. Overall, focus groups were conducted in women’s mother tongue in the MCHB’s office or in another community setting. Focus group data were supplemented with audio-recorded debriefings (between the two researchers who were consistently present during data generation) and direct observations. These gave researchers a crucial opportunity to reflect on their experiences as focus groups moderators or observers; record their key observations about research settings and participants; discuss data generated through focus groups and observations; and prioritize questions or topic areas for future focus groups. We analyzed all data through qualitative content analysis while being sensitive to interactions among participants, between participants/health brokers and participants/researchers, and recognizing how different approaches influenced different interactions.
Ethics: Approval and Considerations
We aimed at investigating African immigrant women’s perceptions and experiences during pregnancy and postpartum, was approved by the Research Ethics Board at the University of Alberta. Due to language barriers, we anticipated that obtaining participants’ consent in cross-lingual research might be challenging. Therefore, we asked interpreters to explain the purpose of the research at the beginning of each focus group and reiterate that participation was voluntary. Data generation started upon women’s verbal consent, and audio recording only occurred if participants also consented to being recorded. We paid close attention to women’s nonverbal cues, such as facial expressions and nodding, and addressed any noted discomforts or possible concerns women had by explaining the purpose of focus groups and audio recording and by reiterating that both participation and recording were optional.
Women in this study received a 25-dollar gift card to a local grocery store as an honorarium for focus group participation. Over the course of the study, however, the number of participants consistently increased, and the amount provided had to be decreased to 10 dollars per participant per focus group due to budgetary restrictions. This unanticipated change was likely related to the fact that we were working with immigrant women living with poverty, who not only valued the monetary honorarium but also the opportunity to socialize with other members of their communities.
The next sections of this article will provide insights into the process of conducting cross-lingual focus groups within a cross-cultural CBPR study. We will describe in detail three different approaches to cross-lingual focus groups used in this CBPR study, along with corresponding advantages and challenges. We will also comment on general aspects of the data collected.
Interpreted-Assisted Focus Group Moderated by Researcher With Audio Recording
We conducted three focus groups with Eritrean and Ethiopian women (average of 10 participants per group) in their mother tongue. Focus groups were audio recorded and moderated by an English-speaking researcher with Eritrean and Ethiopian health brokers acting as real-time interpreters. Following the focus groups, the audio recordings were transcribed verbatim and analyzed. Health brokers took turns in the role of real-time interpreters, translating the researcher’s questions to participants and translating participants’ answers to the researchers. The health brokers matched participants’ ethnicity and sex (female) and were similar in age. This was highly desired as other studies have also described how matching interpreters and participants can help to build meaningful research relationships with participants (Kapborga & Bertero, 2002; Wallin & Ahlstrom, 2006; Yelland & Gifford, 1995). In addition to knowing women’s language through grammar and vocabulary, health brokers had background knowledge of their clients’ cultures and social contexts, which better enabled us to explore perceptions and experiences of health during pregnancy and postpartum using focused ethnography (Agar, 2006).
Interpreter-assisted, cross-lingual focus groups allow the researcher to take an active role in moderating the discussion and in influencing the direction of probing questions (Barbour, 2013). The interpreters/health brokers acted as a active “conduits” between the moderator (i.e., researchers) and the participants (Kapborga & Bertero, 2002) as shown in the transcript excerpt below:
Moderator: You know how last time you mentioned that back home you are treated like a queen [during pregnancy], you get all the attention and if you’re craving anything you always have someone to fill these cravings. We were wondering how the lack of rest here affects their pregnancy or how that affects their health?
Interpreter: Okay, I remember we touched upon this and so that is part of what they were saying last time, the stress is because of that, they intend to grab anything and everything which is why then we are in the problem we are in. I’ll translate that. [Conversation in women’s mother tongue]
Interpreter: ‘We get stressed and we can’t sleep. If you don’t sleep well and if you don’t get enough rest, you get frustrated and you get very tired. So that’s one of the results.’
Moderator: When you said that you get frustrated, who can help you, what type of supports would you need when you feel like that? [Conversation in women’s mother tongue]
Interpreter: So what she’s saying is there is nothing to compare, really. She said, ‘in fact I’ve had three of my children back in Africa and so the treatment there and here, there’s nothing to compare. ( … )
In our study, interpreter-assisted, cross-lingual focus group generated rich data and allowed us to investigate Eritrean and Ethiopian women’s perceptions of a healthy pregnancy and their experiences in a new country. However, because during focus groups interpreters provided constructions of women’s comments and responses, rather than word for word translation, we had to trust we were given the “right”—or accurate—construction of women’s perceptions and experiences. Overcoming this issue can be difficult when conducting focus groups in any language other than the one(s) the researcher has fluency as interpreters may inevitably add their own views to answers or respond to questions themselves (Kapborga & Bertero, 2002; Wallin & Ahlstrom, 2006). In the context of our focused ethnography with women from diverse cultural backgrounds using a CBPR approach, by including their own experiences of pregnancy and postpartum in Canada, health brokers were going beyond the translation of women’s words as they actively tried to make cultural practices and beliefs more comprehensible to researchers. Nevertheless, we note here the importance of emphasizing with interpreters the fact that reaching consensus among participants, as a strategy to facilitate English-speaking moderator’s understanding, is not necessary or desirable. We tried to do this by promptly responding to women’s facial expressions and group reactions, for example, “what did she say that made everyone laugh?” or “she seemed confused when you [health broker] were speaking.”
Having transcribed focus groups data was valuable for validity. Nevertheless, in our experience with this study, it is important to consider the higher costs of transcription of cross-lingual focus groups, and the time it may take to clean the transcripts, especially if participants have strong accents. The number of participants in each focus group varied greatly due to the CBPR approach taken in this study. Still, when possible we would recommend limiting the number of participants in cross-lingual focus groups with an interpreter to a maximum of six as an effort to facilitate group interactions, manage time, and improve quality of verbal data for transcription. In groups with more than six participants, women who had more fluency in English often started answering questions directly to the moderator, while the interpreter translated questions to the group as a whole. In these occasions, our attention was divided between participants answering questions with and without the aid of the translator, and as a result, transcribed data had gaps with inaudible parallel conversations that later on had to be filled by the researcher during verification of transcripts.
In addition to focus groups and time spent with interpreters, as previously described, we also engaged with the participating women outside the formal focus groups by attending weekly perinatal classes that addressed a variety of topics (e.g., brain and fetal development, healthy eating). These opportunities to engage with the focus group participants allowed us to better understand women’s cultural background and social context, preferred ways of learning, and to observe their interactions with health brokers. In various occasions, we were able to sit beside women who were learning or knew some English and were eager to tell us more about their home countries, families, and pregnancy experiences in Canada. Despite language barriers, in one-on-one informal conversations with participants, we were able to verify the most relevant findings from focus groups, and add more details to our findings through observations.
Interpreted-Assisted Focus Group Moderated by Researcher Without Audio Recording
We also conducted three focus groups with Oromo women (average of six participants per group) in their native language. The process for these focus groups was very similar to that mentioned earlier; an English-speaker researcher moderated the focus groups, and the health broker carried out real-time interpretation.
However, Oromo women did not consent to having their discussions audio recorded. Oromo people represent a large ethnic group in Ethiopia with different religious practices and long-standing history of political conflicts in the area. Graffigna, Bosio, and Olson (2008) suggest that communities in developing countries, with low incomes and levels of education, and ruled by nondemocratic governments, are usually more concerned with privacy of collected data. It is likely many of our Oromo participants have experienced political persecution and were uncomfortable being audio recorded for this study. Additionally, their religious practices did not allow for any form of image recording, such as videos and pictures, and this also seemed to influence their preference for no audio recording. As a result, the researcher had to take notes as the health broker interpreted participants’ answers.
Like the process outlined earlier, the researcher conducting the interpreter-assisted focus groups without audio recording spent time with the health broker before focus groups in order to prioritize questions and gain an initial understanding of women’s cultural beliefs and norms in relation to focus groups’ topics. Also, after concurrently moderating focus groups with Ethiopian/Eritrean and Oromo communities, researchers debriefed for approximately 30 min after each focus group. This proved critical for the one researcher who could not rely on an audio recording, as she had the opportunity to go through her notes and recount participant’s comments or answers to questions as interpreted by health broker. Debriefings after all focus groups and observation activities were audio recorded, transcribed verbatim, and analyzed using qualitative content analysis. The passage given subsequently was extracted from a transcript of the researchers’ debriefing:
Researcher: So, the first question was, what are your every day foods? So, I asked her if she could ask them to kind of compare what they used to eat back home and then what they eat here? And then how anything has changed. It’s funny cause one lady she started laughing as soon as she heard the question and she was like, well I eat everything the same that I eat back home. Well what is it that you eat back home, tell me specifics; and she said she eats rice, pasta, macaroni, injera, corn, lentils, beans, sweet potatoes, and potatoes. They eat fruit every single day. And she said they have a garden in their backyard. And I said so what does that mean though? You garden? And she said, well it’s not like just in our backyard; we have fields and fields, like we are farmers. We are all farmers back home. So, it is just that our backyard is all of this farmland. So we will go back to our yard quote/unquote and we will pick like—what did she say, bananas and oranges and avocados, mangos, sugar cane. They’ll get seeds to harvest fruits and vegetables and things like that. And she said it is really easy to get.
Similar to the interpreter-assisted, audio-recorded focus groups, the health broker involved in the nonrecorded focus groups had very close ties to the women in her community; thus, it is possible she might have added her own views to participants’ answers or responded to questions herself (Kapborga & Bertero, 2002; Wallin & Ahlstrom, 2006). Nonetheless, because the Oromo health broker as a mother and immigrant who had experienced pregnancy and postpartum in Canada fit participant’s inclusion criteria, we considered her own accounts as additional information about African immigrant women’s experiences during pregnancy and postpartum in Canada.
The nonrecorded, interpreted-assisted focus groups pressed us to learn about other intricacies of this data generation method in cross-cultural research. For instance, we learned that sitting beside the Oromo health broker, and maintaining eye contact with participants, helped to build rapport between researcher and women, and maintain engagement. Wallin and Ahlstrom (2006) in their review of interpreter’s role in cross-cultural research did not find any reports on most appropriate seating arrangements during cross-lingual data collection; thus, it is challenging to discuss this, especially since what is most appropriate is likely dependent on the cultural backgrounds of participants.
Furthermore, many times during focus groups, Oromo women posed questions to the English-speaker researcher about delivery and nutrition postpartum and expressed frustration when she told them she was not the most appropriate person to answer their questions. In focus groups exploring Cambodian and Vietnamese mothers’ beliefs about sudden infant death syndrome, Yelland and Gifford (1995) encountered a similar issue as participants expected moderators (i.e., midwives) to assume the role of experts and information providers during focus groups. Although situations like this might cause discomfort to researchers, it could represent a positive sign that women began to perceive researchers as members of their social networks with whom they could build or improve knowledge about pregnancy and postpartum in Canada (Moll, Amanti, Neff, & Gonzalez, 1992). Moll, Amanti, Neff, and Gonzalez (1992) in their ethnographic work with Latino families in the United States described that culturally and historically constructed “funds of knowledge” developed through interactions with social networks helped working-class households to increase their ability to survive and thrive in the midst of economic and social difficulties (Moll et al., 1992).
Overall, despite the challenges in data generation with Oromo focus groups, the interpreter and participating women provided us with valuable insights into how their culture shapes women’s pregnancy and postpartum experiences in Canada. This, in addition to observation of perinatal classes, enabled gathering rich data that increased our understanding or African immigrant women’s perceptions and experiences during pregnancy and postpartum “back home” and “here” (i.e., Canada).
Focus Group With Bilingual Moderator Followed by Translation
The Somali health broker advised that the best way to foster participation from women in her community would be to conduct focus groups in participants’ mother tongue, in a community setting prior to their monthly group cooking program. In addition, focus groups were to be moderated by the health broker herself and audio recorded. As illustrated in Figure 2, the bilingual moderator (i.e., Somali health broker) would listen to the audio recording and then translate and transcribe into English.
Four focus groups with Somali women (average of seven participants per group) were conducted. English-speaking researchers attended all focus groups to observe interactions among participating women and answer any questions about discussion topics or overall research process. Focus group questions were provided to the bilingual moderator ahead of time and briefly discussed with the researchers before the beginning of each focus group. As previously noted, this is an important strategy to increase data validity. It is worth highlighting that the Somali moderator had previous research experience and demonstrated great ability in fostering discussion and eliciting women’s opinions. However, as discussed by Esposito (2001), in this approach to cross-lingual focus groups, researchers do not have the opportunity to guide or redirect focus group questions, and we were completely reliant on the health broker’s skills as a bilingual moderator to generate relevant data (Kapborga & Bertero, 2002; Umana-Taylor & Bamaca, 2004). In addition, similar to interpreter-assisted focus groups, it was difficult to say whether or not the moderator provided women with her own perspectives while explaining the meaning of translated questions.
Focus group discussions were audio recorded, and following completion, the bilingual moderator completed translation and transcription into English. Translating focus group data requires more than fluency in another language, as various contextual and social factors influence this highly complex interpretive process (Baker, 2006; Esposito, 2001). For instance, there may not exist words in the participants’ mother tongue that are equivalent to English; therefore, meaning-based rather than word-for-word translation is warranted (Esposito, 2001). The Somali health broker was responsible for translating and simultaneously transcribing this meaning-based data. Due to the health broker’s competing priorities, and the amount of time required for meaning-based translation, there was a significant delay in completing the translation and transcription of recordings. The transcript was not verbatim, but a summary of the conversation, as shown in the following excerpt:
Somali Health Broker: What a healthy eating mean to you during pregnancy and after pregnancy here in Canada and in Somalia? What do you think are the main differences?
Somali Health Broker’s translated summary of women’s answers: In Somalia—we do not control what we eat. Everything we eat is organic. Most of the people have no options to choose what they eat. Food variety is limited. There is no culture or dialogue of discussing healthy food. Women eat whatever is available to them. For most of the people fridge or food storage is not available. We buy the food we eat on daily basis and you can get fresh food from the market. [ … ]
Somali Health Broker: How about in Canada?
Somali Health Broker’s translated summary of women’s answers: In Canada—we go to the food market once a week and usually we take bus or drive. Most of the food is frozen, except fruits and few other items. We store food in the fridge. Sometimes we cook two meals together. It’s easy to manage cooking here in Canada. We are aware about the healthy eating, but they are expensive. We try to balance the food we eat and avoid as much as possible fat or high carbohydrate food. Healthy food is expensive. The majority of our community is low income and cannot afford to buy.”
Furthermore, because focus groups were conducted with a bilingual moderator followed by translation and transcription, data analysis could only begin once researchers received the transcript. Not being able to analyze data as generation occurred could have represented a serious threat to study rigor had we not been able to analyze the data from the other three African communities and researchers’ debriefings and use this to inform and adapt interview questions and the research process with the Somali women.
Cross-Lingual Focus Groups in Cross-Cultural CBPR: Is There a Best Approach?
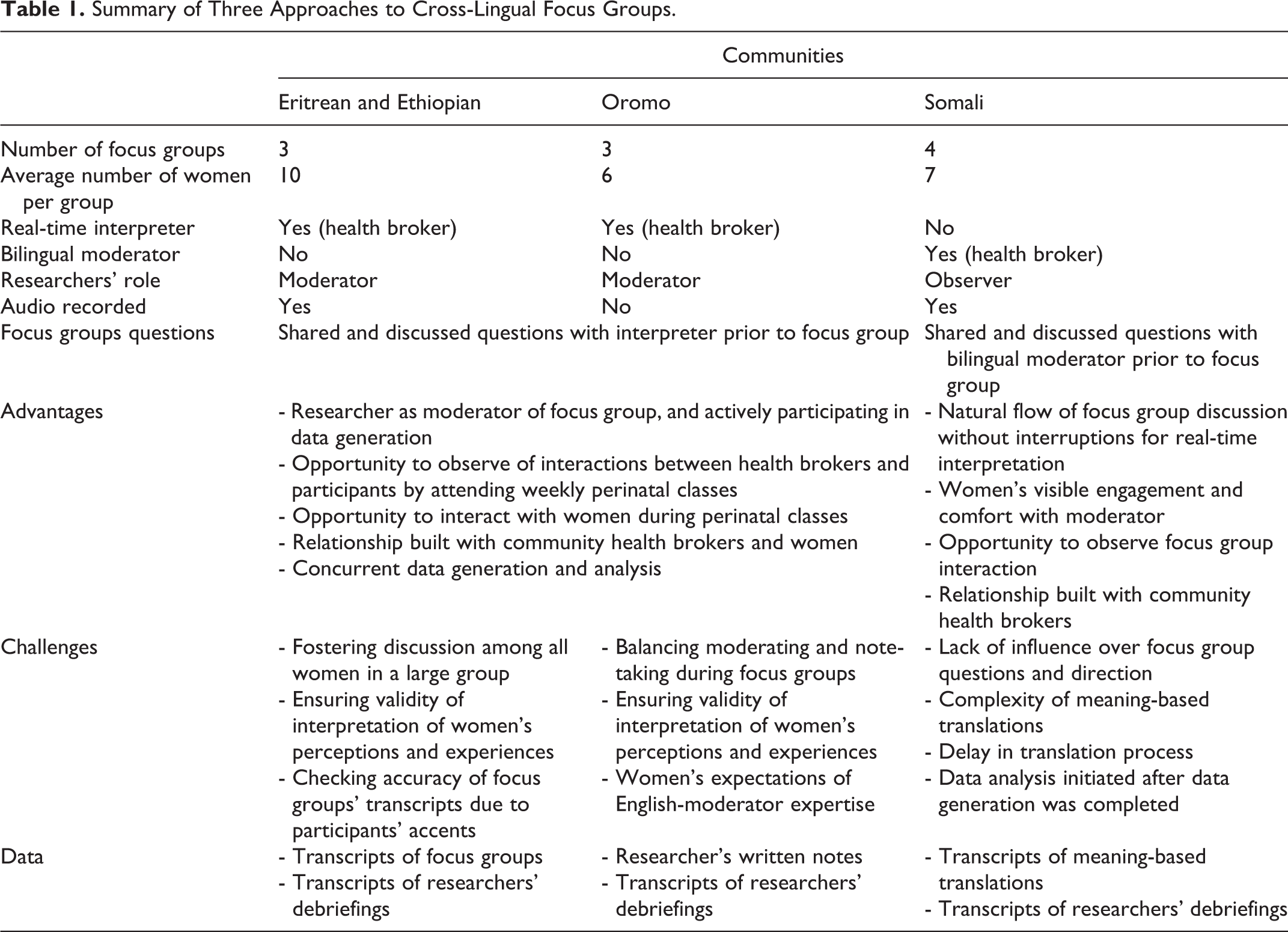
In this CBPR study with African immigrant women, three community-driven approaches to cross-lingual focus groups were taken, summarized in Table 1. Cross-lingual focus groups embrace participants’ multiple realities and socially constructed knowledge. However, conducting both interpreter- and translator-mediated cross-lingual focus groups require adequate planning, implementation, and culturally sensitive analysis and interpretation of data (Esposito, 2001).
Summary of Three Approaches to Cross-Lingual Focus Groups.
The principles of CBPR guided this study, including the planning and implementation of focus groups. As such, health brokers who were real-time interpreters and translators decided on the most appropriate ways to create an exchange among themselves, the researchers, and participants. Not only did this contribute to the quality of ethnographic data generated throughout all focus groups but also allowed researchers to better adhere to ethical principles of CBPR. Consistency with ethical principles of all partners around the table throughout the research process is what ensures respectful generation of data that matches communities’ realities—also described as “ethical validity” (Edwards, Lund, & Gibson, 2008). Furthermore, health brokers assisted researchers in understanding the extent to which African immigrant women’s sociocultural contexts define their pregnancy and postpartum experiences in Canada, especially in contrast to their home countries. Acknowledging that women may have hybrid experiences from “back home” and “here,” and our limitations in understating their multifaceted realities, makes the role of health brokers even more relevant. They were not simple interpreters and translators of language but of women’s experiences, which were embedded in cultures health brokers could easily grasp and make comprehensible to researchers (Agar, 2006).
Graffigna et al. (2008) have demonstrated the importance of the research setting and “medium” (e.g., face-to-face and online) in focus group data collection. In any project using a CBPR approach, researchers should have the opportunity to correctly select the appropriate setting and medium, given that the participating community is part of both designing and conducting the research. As such, different approaches to focus groups across cultures are likely to result in different format, content, and depth of data. Our research shows that in CBPR one size does not fit all, even if working with communities from similar cultural backgrounds. These differences are indeed what garner excellent focus group data.
We argue that what is equally important for good quality data is that researchers are present in the setting over a period of time for participation in and observation of community activities whenever possible and that community participation in the research process is continuously fostered. Agar (1996) describes that “devotion to the initial learning role is one of the major ingredients that makes ethnography the unique concoction it is” (p. 120), and this “devotion” was very pertinent to our focused ethnography, especially through health brokers. They allowed us access to background knowledge about participating African communities and guided how research activities were to be performed throughout the study (Agar, 1996). Engaging with communities requires time and researchers’ commitment to mutual trust, respect, and colearning (Cargo & Mercer, 2008; Castleden, Sloan Morgan, & Lamb, 2012). In addition, engagement in cross-cultural CBPR is critical to understanding participants’ sociocultural and political contexts (Wallerstein & Duran, 2006) and properly seeking their input during data generation, analysis, and presentation of findings. As such, participation is not only a means to an end but also a strategy to ensure validity of qualitative data, and, most importantly, to empower communities (L. M. Morgan, 2001; Wallerstein & Duran, 2006).
Hsin-Chun Tsai et al. (2004, p. 24) emphasize that “threats to the accuracy, trustworthiness, and/or validity of cross-cultural, cross-language qualitative research continue to exist if the data analysis process does not include those who understand the culture and the language of the participants.” In this CBPR study, community stakeholders (i.e., health brokers) not only contributed to researchers’ understanding of focus group data but also added details to women’s comments and responses that greatly enriched overall findings. Health brokers’ participation was crucial and enabled researchers’ to gather qualitative data that truly honored African immigrant women’s health perceptions and experiences during pregnancy and postpartum. Most importantly, we recognized their ethnic and linguistic pluralism. We hope this will help to build evidence on the extent to which African immigrant women’s cultures and realities shape their perinatal experiences in Canada and inform what Hornberger (2002) calls nation-building policies—policies that open possibilities for immigrants who have not assimilated the Canadian official languages and sociocultural contexts (Hornberger, 2002).
To conclude, we answer the question, is there a best approach? In this study, there was not a best approach to cross-lingual focus groups. Engagement with health brokers and communities during and beyond focus groups allowed us to mitigate challenges with each approach and gather meaningful, rich, and valid data. In cross-cultural CBPR, the best approach to cross-lingual focus groups is the one identified by the community, the one that respects their prefered ways of sharing knowledge, and allows researchers to colearn with participants. For those using cross-lingual focus groups, we stress the importance of following the principles of CBPR, especially community engagement, and of considering the advantages and challenges of each approach presented here. What might be feasible yet rigourous will vary in given settings and cultures.
Footnotes
Acknowledgments
We sincerely thank all the women and health brokers who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project is funded by Alberta Innovates Health Solutions. Maira Quintanilha received additional support from the Women & Children’s Health Research Institute, Community University Partnership, Queen Elizabeth II Graduate Scholarship, Elizabeth Russell MacEachran Scholarship and President’s Doctoral Prize of Distinction at the University of Alberta, and is currently supported by the Vanier Canada Graduate Scholarship.