
Abstract
A study on how Zambian migrants living in Cape Town perceive and experience the implications of labial elongation on women’s health was conducted. Labia minora elongation (LME) is a genital modification that some women in east and southern Africa practice. This tradition is not common in Western Cape province (southwestern part of South Africa). The aim of this article is to discuss the methodological choices made in the design and conduct of this study, in which a White European male interviewed the female study participants on the health implications of a practice that is considered a woman’s private issue. Constructivist grounded theory informed by a feminist perspective was chosen as the most suitable methodological approach to enable cogeneration of knowledge with the female participants. The methods and tools used by the lead investigator facilitated access to the participants’ emic views. Grounded theory methodology holds the potential to be an appropriate methodological approach for researchers who seek to erode the power imbalances influencing research processes that aim to explore the associated meanings and health implications of female genital modifications, such as LME, as narrated by the women who practice them.
In some cultures, women engage in various female genital modifications (FGMo) in preparation for womanhood, marriage, and sex; for hygiene and grooming; and for other health-related purposes (Bagnol & Mariano, 2012; Martin Hilber et al., 2012). In sub-Saharan Africa, these practices are sometimes an expression of women’s strategies to control their partners, and to ensure commitment in their marriages (Bagnol & Mariano, 2012; Pétursdóttir, 2010). Commonly, knowledge of the motivators, procedures, and substances employed is transmitted to young girls around the onset of menstruation, when they are considered ready to be guided into womanhood (Bagnol, 2013; Bagnol & Mariano, 2012; Martin Hilber et al., 2012).
One such FGMo is labia minora elongation (LME), which consists of the manual stretching of the inner folds of the external female genitalia. This is carried out with the aid of herbs and creams, until the desired length is achieved, which can range from 2–8 cm (Martínez Pérez, Tomás Aznar, & Bagnol, 2013). Women who practice LME have reported that one of the main motivators is to enhance both partners’ sexual pleasure (Martínez Pérez, Bagnol, & Tomás Aznar, 2014).
In recent qualitative and anthropologic research, it is possible to find the perspectives on LME of some women insiders of this FGMo from eastern Democratic Republic of Congo (Grassivaro Gallo, Mbuyi, & Bertoletti, 2010), Lesotho (Khau, 2012), Malawi (Pétursdóttir, 2010), Mozambique (Bagnol & Mariano, 2012), Rwanda (Fusaschi, 2012), and Uganda (Parikh, 2005). The only recent example of mixed-methods research that is framed in a public health approach is the gender, sexuality, and vaginal practices study in Mozambique (Hull et al., 2011; Martínez Pérez, Bagnol, & Mariano, 2014). Additionally, in northern Italy, the Padova Working Group (PWG) on female genital mutilation studied the experiences of migrant African women with LME. The PWG reported that some migrant women might feel inadequate and different, and some had undergone labiaplasty (Grassivaro Gallo et al., 2010).
Aim
This study is the core component of a doctoral dissertation in health sciences. The PhD candidate (GMP) aimed to follow the PWG recommendation to investigate the psychosocial and sexual well-being of migrant women in countries, where LME is not normative. A qualitative study was conducted in Cape Town (Western Cape province, in the southwestern part of South Africa) to explore the values, meanings, and experiences that the Zambian migrants associate with LME as well as to document its health risks and benefits. LME is practiced among Zambian women (Mwenda, 2006; Rasing, 2001) but is not practiced among women born in Cape Town (Martínez Pérez et al., 2015). To the best of our knowledge, there is no qualitative research in the literature reporting on the perceptions of Zambian women who have practiced LME and who have migrated to other African countries, where LME is not customary.
The primary aim of this article is to discuss how the constraints identified during the proposal development stage guided our methodological choices. A subsidiary aim is to expose how different elements from feminist and constructivist grounded theory helped the researcher to overcome some of the anticipated constraints and cogenerate knowledge with the women.
It is not the aim of this article to report on the findings that relate to the health implications of LME, which are reported elsewhere (Martínez Pérez et al., 2015). This article is cowritten by the doctoral candidate, his supervisor (CTA), and his coinvestigators (MM and BB). In this article, the candidate is referred to as the researcher to isolate his identity as lead interviewer and principal investigator. The female study participants are referred to as the women as—based on our methodological approach—they were considered not only participants but also anonymous cogenerators and coconstructors of data and knowledge.
Method and Material
This study was qualitative in design. A constructivist grounded theory methodology (Charmaz, 2008, 2012), informed by a feminist perspective (Plummer & Young, 2010; Wuest, 1995, 2011), guided study design, conduct, and reporting. The Human Sciences Research Council (Pretoria, South Africa) and the Comité Ético de Investigación Clínica de Aragón (Zaragoza, Spain) granted ethics approval.
The study took place in the city of Cape Town between December 2013 and May 2014. The inclusion criteria for this study were Zambian women and men aged above 18 years old, with knowledge of LME, and who had been living in South Africa for at least 1 year. The women must have had experience of LME. Men were invited as participants as their sexual preferences play a role in women’s motivations to practice LME (Martínez Pérez, Bagnol, & Mariano, 2014; Martínez Pérez, Bagnol, & Tomás Aznar, 2014).
Snowball sampling was used to identify all women and men participants. The first two “seeds” who provided an introduction to other participants were identified among the social acquaintances of our coinvestigator, who is a Black Zambian woman (MM). The researcher continued sampling from these two first seeds. No woman approached declined to participate. Nineteen men were approached, and 2 refused to participate.
In total, 20 women and 17 men were enrolled in the study (Table 1). The mean age was 32 years for both women and men. The women had lived in South Africa for 6.6 years on average and the men 4.9 years. There was balanced representation of married and single participants among women and men. Three women were divorced. With regard to their education, one woman had a primary school education, and eight women and three men had completed secondary school. Half of the participants held college and university degrees. Eleven tribes were represented; however, Bemba was the ethnolinguistic affiliation that most participants belonged to (11 women and 6 men, respectively).
Sociodemographic Characteristics of Study Participants.

In-depth interviews (IDI) were conducted with all 37 participants. Three natural group discussions (NGD) with women only and two NGD with men only were conducted. A Black Ghanaian woman with experience in health and social research who was raised in the Western Cape was enlisted as cointerviewer to accompany the researcher during the interviews with the female participants only.
Data collection took place in a location chosen by the participants. Prior to data collection, the purpose of the research was explained, and written informed consent was obtained. Contact details for the researcher were specified on the consent form in case of any participants were interested in requesting the study publications. Each participant received ZAR 100,00 (approximately USD 9,00) to cover their transport expenses.
A semistructured interview guide for the IDIs and NGDs was informed by two reviews on LME (Martínez Pérez, Tomás Aznar & Bagnol, 2013; Martínez Pérez, Bagnol, & Tomás Aznar, 2014). All data collection took place in English. All IDIs and NGDs were tape recorded, and the researcher personally transcribed all recordings verbatim. Personal identifiers were not transcribed; the recordings were classified with an alphanumeric code to ensure anonymity.
Transcriptions were line by line coded by means of gerunds (Charmaz, 2012; Plummer & Young, 2010). Data collection and analysis took place concurrently until saturation of the properties of the categories that emerged from the data were achieved (Charmaz, 2012). At this point, sampling was discontinued.
Trustworthiness was ensured through a variety of measures (Elo et al., 2014; Sikolia, Biros, Mason, & Weiser, 2013), namely, triangulation of findings from the IDIs and NGDs against the literature on LME, examination and reporting of deviant cases, use of representative excerpts to reflect the emic views of the participants, and sharing of the main preliminary findings with the participants in the NGDs. Additionally, during the analysis process, the researcher had the emerging concepts and core categories peer reviewed by our Zambian coinvestigator.
Results
In this section, we first describe the constraints that we identified at our study proposal stage. We then explain how a feminist and constructivist grounded theory was identified as the most suitable methodological choice to help the researcher overcome the preidentified constraints. Finally, we use excerpts from the women to illustrate how some of the methods and tools were useful for exploring their insider views into the phenomena in question and also into the appropriateness of our research approach.
Preidentified Constraints
The question of the importance of the investigator characteristics arose when the researcher proposed the study of the health implications of LME as experienced by Zambian migrants as the core component of his doctoral dissertation. The researcher is a White European gay middle-class man with a hybrid background in health and social sciences. Gender, class, and race differences might impede rapport in qualitative research (C. L. Williams & Heikes, 1993). Thus, all these elements of dissimilarity held the potential to influence the research process.
During the preparation of the study proposal, guidance was sought from the literature as to how a man could position himself to collect data on LME, but no relevant material was found. There is a paucity of qualitative research authored by men with a specific focus on LME.
John Williams measured the length of the labia minora of 124 women attending antenatal care in Zimbabwe (Williams, 1969). Kenneth Kaoma Mwenda described the motivators and the procedure of LME in Zambia and analyzed how LME, under African customary law, violates the rights of girls and women (Mwenda, 2006). Likewise, Michael Gelfand (1979) and Herbert Aschwanden (1982) described LME among the Shona and the Karanga in Zimbabwe. Neither Mwenda nor Gelfand or Aschwenden stated whether they obtained their data directly from methodologically interviewing women who had practiced LME.
The colonial anthropological literature contains other scattered references to LME based on the observations of men writers who had visited east and southern Africa (Fusaschi, 2012; Ploss & Bartel, 1935). The tendency among these writers was to reflect on LME from a religious and ethnocentric perspective. The researcher studied writers such as, for example, Bishop Bigirumwami who described LME in Rwanda as “inspired by the same devil” (Fusaschi, 2012) but was unable to find definitive guidance on how to collect and analyze data in collaboration with women as study participants.
LME is a practice that is taught as part of initiation rites of adolescent girls into womanhood and is described in recent qualitative literature as women’s “secret” (Bagnol & Mariano, 2012; Fusaschi, 2012; Tamale, 2006). In east and southern Africa, women’s secrets also include guidance on FGMo other than LME, such as intravaginal insertion of substances or intravaginal cleansing and instruction on sexuality, hygiene, and marriage that girls receive during their initiation rites (Bagnol, 2013; Bagnol & Mariano, 2012). In reporting their experiences interviewing women in Tete, central Mozambique, Brigitte Bagnol and Esmeralda Mariano, French and Mozambican women anthropologists, respectively, wrote that there was an “unexceptionally open and intimate atmosphere at the interviews” which helped them to go in-depth into some of the themes discussed, including LME (Bagnol & Mariano, 2008, p. 44). Notwithstanding their experience in Tete, on her recent research on initiation rites in northern Mozambique, Bagnol (2013) explains that achieving a deep insight into the core of women’s secrets was difficult because of the “distortion, concealment, lies and misinformation” that emerged as major methodological fieldwork dilemmas (Bagnol, 2013, p. 150). Thus, another important concern identified at the outset of our study was the acknowledgment that exploring LME involves exploring a gendered practice which is culturally sensitive, closely interwoven with FGMo and other sexuality matters, only discussed in private and in many cases only among women who have attended initiation rites.
A Grounded Theory Research on LME
All the a priori-identified constraints led us to use grounded theory methodology. Some scholars advocate the use of a single grounded theory interpretation—be it feminist, constructivist, classic Glaserian, or Straussian—as a full-package methodology (Breckenridge & Elliot, 2012). The researcher considered different interpretations of grounded theory and accepted Charmaz’s advice to use “the strategies that work for you and your study but be aware of what you do and what you claim” (Charmaz, 2012, p. 3).
This study was mainly informed by constructivist grounded theory. Epistemologically, constructivist grounded theory infers that there exist multiple realities that are constructed by people based on the meanings that they assign to the world around them during their interaction with the objects (Charmaz, 2008). Constructivist grounded theory involves people as active agents in the research process, and data and theory are created through an interactive, inductive, and contemporaneous process by both researcher and participants. Data and theory are, thus, coconstructed (Charmaz, 2008). Considering all the constraints described above, this approach seemed the most suitable to jointly explore the women’s views on LME.
Additionally, the researcher adopted a recommendation to reconcile a feminist perspective with constructivist grounded theory when conducting research on women’s health (Plummer & Young, 2010; Wuest, 1995, 2011). A feminist perspective was helpful in framing how the researcher could be perceived as a stranger scrutinizing a sensitive topic from a position of power. It was expected that an approach in which the participants are invited to be anonymous coauthors and cogenerators of knowledge in the research process could palliate the effect of this power-gendered relationship. Furthermore, a feminist perspective was helpful for the researcher to allow reflexivity—a reflection on his impact and reciprocal influence in the research process.
A feminist perspective was necessary for the researcher’s accountability to develop nonexploitative relationships with the women, to listen to their voices while coding and analyzing the data, and to conduct a study that would generate knowledge that should be useful to women. Charmaz (2012) advocates for research findings to be used for social justice. Wuest (2011) advocates for the findings to be useful for the women, and to be used for social change. This aspect was expected of our study from the proposal development stage; the findings had to provide insightful information on the health risks and benefits of LME. It was expected that this new knowledge could help to inform culturally appropriate and women-driven public health interventions to promote and improve the sexual health of women who practice LME.
Having chosen our methodological approach, it was necessary to operationalize it in order to establish an effective researcher–participants interrelation. In Table 2, we offer an overview of the measures and tools used during the conduct of this study.
Some Measures to Ensure Trustworthiness Used in This Study.

A literature review was requested as part of the researcher’s doctoral dissertation. The literature was examined for guidance on how a man could interview women about their experiences with LME. The search was also helpful in justifying the relevance of this study as the Zambian migrants’ experiences with LME were unreported in the literature. Dunne (2011) and Charmaz (2008) recommend mapping the investigator’s actual knowledge onto the study topic, reflecting on how this knowledge determines preconceived ideas, and delaying further review of the literature. In this study, although a review was conducted at the study proposal stage, the researcher waited for the core categories to emerge before seeking additional references on issues around womanhood and masculinities in Zambian culture.
Having only a partial awareness of the literature facilitated the use of theoretical sensitivity (Wuest, 2011). Theoretical sensitivity allows placing preconceived ideas aside and immersing oneself in the data to discern what the participants perceive as meaningful. Theoretical sensitivity enables investigator and participants to establish a close bond in which they coconstruct the theory together as data are collected and analyzed contemporaneously (Charmaz, 2012).
The transcriptions were coded line by line at first (Charmaz, 2012). Coding was done using gerunds to better depict actions and processes (Charmaz, 2012). At the same time, memo writing was conducted to assist in the definition of concepts and categories. Memoing also served as a “reflexive journal” (Giesler, 2013) to reflect on how the researcher characteristics could impact the research process.
In any study of the implications of LME for the health of women, both men and women should initially be probed for its associated health risks, its motivators, its role in enhancing sexual pleasure, and its importance for marriage. Thus, the researcher began the first IDIs and NGDs with a broad set of questions that were similar for both sexes (Table 3). As concepts and categories started to emerge from the data, the interview guide developed and incorporated different gendered areas. Exploration of all categories continued until their properties were considered saturated, which is a grounded theory approach known as theoretical sampling (Charmaz, 2012).
Interview Guide: Initial Set of Topics Explored With Study Participants.
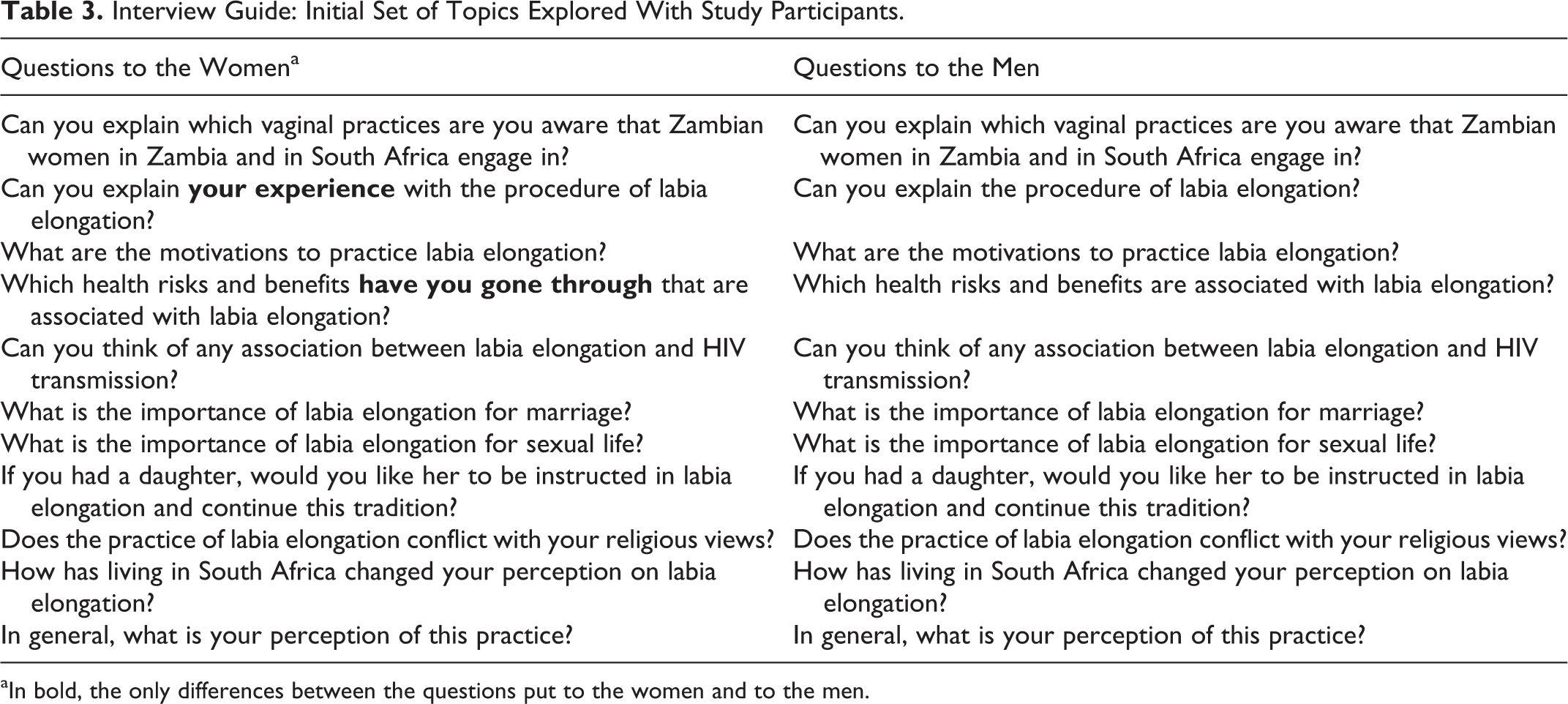
aIn bold, the only differences between the questions put to the women and to the men.
Cogenerating Data and Knowledge on LME With the Women
During the data collection stage, the researcher used some methods to build rapport, practice reflexivity, minimize the impact of gendered power imbalance in the research process, and, overall, ensure the trustworthiness of the study and the usefulness of its findings for women’s health. We conclude this Results section by explaining some of the methods used by the researcher.
With the cooperation of the women, the core category in this study was defined as “becoming a Zambian complete woman.” The notion is that compliance with LME benefits the psychosocial health of some Zambian women, because the practice ensures that they will be perceived as “complete” women whose upbringing complies with tradition (Martínez Pérez et al., 2015). This notion is exemplified by the following excerpt: When you meet your husband, they make sure the man is gonna marry you [sees that] you are complete. How wonderful woman you are! Because when you are married you cannot act as someone who is not married. For us, they see that you have pulled the stuff, those that we call “malepe” [elongated labia]. It means; “now you are a woman, you do not look like a child anymore!” (Nsenga woman, 34 years, married, cook)
To gain access to the women’s emic in central Mozambique, Bagnol and Mariano (2009) used the same metaphors, symbolic language, terminology, and silences that the women use. The researcher used the same measure and he used only terms that, to the women, were acceptable to be heard from a man. As a result, the women showed themselves comfortable during the IDIs and NGDs. Most women used traditional terms that the researcher avoided, such as genitalia parts and the word “malepe” (elongated labia). According to the women, they would not use such private terms in discussions with men in Zambia: “Malepe” is actually very sensitive. It is not an easy topic to discuss. And as we are talking right now here you are undressing us. That is how we feel. So normally we do not talk about these issues. We would never use “malepe” in front of a man in Zambia. (Bemba woman, 34 years, married, social worker)
The women’s interaction with the researcher helped him in the process of memoing and reflexivity. During the interviews, many women addressed the researcher as “you, Westerner,” or “you, researcher,” or “you, White.” The women had identified some elements of dissimilarity and had positioned the researcher as foreign from their culture, a native from a country (Name of researcher’s country) they knew little about. At the same time, the women acknowledged that the researcher shared with them some characteristics. Both the researcher and all the women were labor migrants in Cape Town. And the researcher was a doctoral student, a health worker and middle class, characteristics he had in common with many participants.
Contrary to what the researcher had anticipated, the similarities and dissimilarities the participants identified did not impede the joint exploration of the health implications of LME. On the contrary, had the researcher shared ethnolinguistic affinities with the women, rapport could have not been built in the same way. As one 34-year-old Bemba female participant explained in an NGD, if the researcher had been a Black Zambian man instead, they would not have been discussing LME so openly because “it is our private parts that we are talking about” and, in public, “Zambian women, we even don’t talk about it.”
Being a man was the researcher’s characteristic that held more potential to prevent the women from cogenerating data. Reflexivity helped the researcher to understand that to overcome the gendered power imbalance, he had to be honest with the women not only on the study purpose but also on any other personal data they might request from him. Being transparent throughout the data collection helped to build rapport. Commonly, some women were interested to know his own opinion on LME and whether LME was practiced by women in his home country. The researcher replied that he was in the process of learning about LME with the participants and had not yet gained enough insights to form an opinion on the harmfulness or innocuousness of LME. He noted that women in Spain do not practice LME but that some undergo labiaplasty and other various cosmetic genital surgeries.
At the point in the NGDs where the importance of LME for Zambian men was discussed, some other women wanted to know whether the researcher had ever had sex with a woman with elongated labia. He responded that he had never had sex with any woman with elongated labia. In response to this last query, the women, invariably, relaxed, smiled, and even joked: Have you ever gone with a woman with that? No! You go practice! [All women laughed] I don’t know how ethical in research that is [laughs]. I can’t answer that. But I had been around in this world, I had been with a number of men in my life and they always have the same experience, they tell me certain things … And I would feel very womanish. (Bemba woman, 34 years, married, social worker)
The women appreciated that they were confronted with findings from studies on the health implications of LME conducted in countries others than Zambia. In this way, the women became, once more, anonymous coconstructors of data and theory. For instance, the women were asked their opinion on research that suggests that the instructions young women receive from their elders on LME might encourage them to seek early initiation into sex and thus risk HIV transmission (Etyang & Natukunda, 2005; Grassivaro Gallo & Endrighi, & Viviani, 2008). All women disagreed:
If you want to have sex is not because I have elongated certain thing in my body. It is about the mindset, how I feel … And actually that statement is very forced … I don’t think I would wake up in the morning and say; “oh, because I had pulled my stuff, then I have to go and have sexual whatever.”
That is why you research this, to find out if that statement is true or not. Actually it is very false. They have got that information from their own corners. They haven’t gone around asking people “why?” … We have our own solid reasons, which is very traditional and very respectful. Actually, it is something we really don’t even need to talk about. But because it is affecting people worldwide, that is why we have come here: to put out our views. (Excerpt from NGD with Women #3)
During the joint exploration of the literature on LME, the women were also asked for their views on the World Health Organization’s tagging of LME as female genital mutilation (FGM) (OHCHR et al., 2008):
I don’t think there is anything to do with harmfulness. Because when you are pulling, there is not any blood, pain, anything … It is just skin that you pull and it elongates on its own, just growing as your ears keep growing. It is just something that grows; nothing to do with harmfulness.
So for you it is not comparable at all to FGM? What do you think about people coming from Europe, looking at your traditions, and getting to these conclusions and statements?
I think it is lack of knowledge about our traditions. That is why they give negative answers. In that aspect, I would understand them, because they don’t understand why we do that. But I think that what I would definitely do is talk to them, and make them understand if they are interested.
Like what you are doing right now.
We don’t hide. If you really want to know more about it, come and I will tell you. We are comfortable! (Excerpt from NGD with Women #3)
The NGDs turned out to be a good opportunity for the researcher to encourage discussion among the women on some of our methodological choices. The women were concerned that many scientists do not return to the African women as primary sources to verify the credibility of scientific interpretations of data collected in Africa:
When people come from Europe to do studies here in Africa, it should be encouraged that they do not do studies on their own, but with the people that are from the particular region where the study is taking place. Because the way you will understand what it is going on will be different from the way the person who is part of the tradition will understand the whole thing …
My coresearcher is a Zambian.
It is a good approach, excellent. That person would be able to look at things from a different angle than you. (Excerpt from NGD with Women #2)
Rapport was built with the women who put aside the social conventions that impel them to defend the rationale behind LME. Many dared to be opinionated on the social significance of the motivations behind LME because it was clearly explained to them that our study purpose was to generate knowledge that could be used for interventions to improve women’s health: I would want to know the outcome of your research. It is something that I never thought of; somebody carrying out a research [on LME]. Culturally, us Africans, we are so strong and so stiff about our cultural aspects, and women are just told: “Oh, you have this kind of practice, we have been doing this and that, but it is up to you.” That is why I say I am interested to know the outcome of your research. (Rita, Bemba woman, 34 years, married, social worker)
To generate study findings that are used for social change, the researcher also asked the women to express their opinion on the risk reduction strategies that have been proposed out of research on LME in Uganda (Martínez Pérez & Namulondo, 2011) and in Mozambique (Martínez Pérez et al., 2014). The women, the majority of whom perceived LME as a beneficial practice, gave some advice on which hygienic measures the girls could follow to prevent the short-term physical harm associated with LME. However, most disagreed that education on LME should be given by health-care workers or at public health facilities. The following excerpt exemplifies a deviant case—that of two women who, when discussing strategies to prevent the potential harm associated with LME, claimed that LME needs to be discontinued:
No, no, no … When it comes to this issue [risk reduction on LME], I don’t think we should carry on with it. The only thing is to encourage them [the girls] to stop …
… the labia pulling starts when you are young. So the first teachers would be the parents … so it starts in the house and then it spreads out in schools, in churches, in hospitals. So in short, it takes the entire community to sensitize about the whole topic. Of course highlighting the dangers of it and the advantages of it. (Excerpt from NGD with Women #1)
Discussion
This article describes the methodological choices made in order to conduct a study of the health experiences of LME as experienced and perceived by Zambian migrants living in Cape Town. At the study design stage, constraints identified were the characteristics of the principal investigator, paucity in the literature of experiences of men investigating LME, and the status of LME as a private women’s issue. Constructivist grounded theory (Charmaz, 2012), informed by a feminist perspective (Plummer & Young, 2010; Wuest, 2011), was chosen as the most suitable methodological approach to overcome these constraints during the study fieldwork stage and to cogenerate data and theory with the participants.
In agreement with a feminist perspective, this study had to be useful for the women’s health (Plummer & Young, 2010; Wuest, 2011). LME is valued by some Zambians in South Africa because it is perceived as a beneficial practice for the women’s social and sexual well-being. The women expressed concern that some preventable and minor adverse effects, such as pain or swelling, might derive from the procedure of LME (see Martínez Pérez et al., 2015). Nevertheless, the majority disagreed with the World Health Organization’s tagging of LME as female genital mutilation. They also disagreed with previous research asserting that the instruction that the youth receive from their elders on LME might encourage them to seek out sex and thus risk HIV transmission (Etyang & Natukunda, 2005; Grassivaro Gallo & Endrighi, 2008). The women’s emic perspectives can be helpful to inform public health interventions to improve the sexual health of women who practice LME. One of these potential interventions could be risk reduction strategies to help the young girls practice LME in the safest and most hygienic way (Martínez Pérez & Namulondo, 2011). To the women, as LME is a sensitive practice that women do not discuss in public, any instruction on how to prevent potential harm must be given by the young girls’ female relatives.
One of the strengths of this study is the methodological approach used to cogenerate the knowledge needed to achieve the study purpose. Constructivist grounded theory informed by a feminist perspective provided tools and methods for the researcher to build rapport with the participants. In agreement with the participants’ perspectives on our methodological approach to researching traditional FGMo in southern Africa, it is recommended that any future research on LME involves both women and men as participants, shares and explores preliminary study findings with the participants, and counts on the collaboration of an African coresearcher who is knowledgeable or a member of the participants’ culture. To minimize the impact of investigator’s personal characteristics in the research process, it is recommended to practice reflexivity assisted by memoing and theoretical sensitivity, to share previous research findings in the frame of natural group discussion, to discuss the appropriateness of the methodological approach, and to explore with the participants the capitalization of study findings for women’s health.
We should not overemphasize the adequacy of our methodological choices. A limitation is transferability, or the extent to which our approach can be transferred to other African settings (Elo et al., 2014). We should be circumspect in reproducing this attempt to have women interviewed in a more traditional African environment. As our research was carried out with women migrants and in an environment in which the FGMo under study is not customary, it needs to be further examined how the methodological approach that we propose may be operationalized in contexts other than South Africa. Another factor contributing to this limitation of transferability is that we did not succeed in enrolling sufficient participants with only a primary education, which might have influenced the type of discourses on LME that emerged during the interviews. Additionally, social desirability might have influenced the narratives of the participants. A specific limitation of this article is that we focused on the interaction between the researcher and the women because this was a major concern that arose at the study design stage. Findings on men’s perspectives and experiences with LME are reported in another article (Martínez Pérez et al., 2015).
Men Researching Women’s Private Issues
The appropriateness of men researchers interviewing women and reporting on women’s private issues in the frame of academic research deserves separate discussion. In 2013, the PhD candidate (GMP) attempted to conduct this very same study in Malawi. In spite of having been granted approval from the district health authorities, the local ethics research board blocked his initiative. The response was clear: a man should not directly probe women as study participants for women’s issues that are culturally sensitive in Malawi. Indeed, at the study design stage for this study in Cape Town, the previous rejection in Malawi influenced the relevance that the researcher placed on choosing the most suitable methodological approach to research such a private tradition in the most ethical and culturally appropriate manner.
The emphasis on protecting African women’s practices from academic scrutiny might not be associated with the biological sex of the interviewer but with the historical damage that Western researchers have done to the image of African women. Undeniably, it is legitimate that local ethics review boards, scholars and women themselves want to protect their image, values, and identity from further harm. As Nawal El Saadawi puts it: Imperialist scholars could write about us African as barbaric, uncivilized, morally, mentally, and sexually debased people while ignoring their barbaric, uncivilized aggression against our men and women. They could use old patriarchal habits, such as female circumcision, to label us and justify their colonization as an emancipatory effort. (El Saadawi, 2005, p. 24)
Ethnographers such as Bishop Bigirumwami have contributed to the image of the African woman as “barbaric.” The construction of that image by different Westerners can be traced back to the late 19th century, when Ploss wrote on the elongated inner labia of the “Bushfolk” and the “Hottentots” (Ploss & Bartel, 1935). His chapter on the “Hottentot apron,” as he termed the elongated labia, is a good account of the material that discussed whether the “apron” was congenital or a consequence of “masturbation.” Ploss pondered “the significance or purpose of the elongation in the terms of comparative anatomy? Is it an atavism, a symptom of primitive development?” (Ploss & Bartel, 1935, p. 335). Blanchard, one of the writers that Ploss quoted, thought that there was a “remarkable resemblance between the vulva of the female chimpanzee and the local structure of the Bush woman” (Ploss & Bartel, 1935, p. 335).
The World Health Organization might have contributed to the historical damage. In 2008, in a multiagency statement, LME is described as “a form of female genital mutilation because it is a social convention, and hence there is social pressure on young girls to modify their genitalia” (OHCHR et al., 2008, p. 27). At the same time, the World Health Organization “ignores” the fact that European and American women are engaging in labiaplasty, replenishing of the labia majora, vulvar lipoplasty, clitoral hoodectomy, and other procedures, as performed by genital surgery specialists in the private sector (Braun, 2009). “What I would definitely do is talk to them, and make them understand if they are interested” stated one woman when the classification of LME as mutilation was discussed. Unfortunately, we cannot explain to the women why those who determined what is classed as female genital mutilation did not “talk to” the women in Zambia to “understand” LME.
It may take years before more culturally sensitive studies can help restore the image of the African woman as barbaric. What we aimed for is precisely what the women considered appropriate: request collaboration from African women as the primary sources of knowledge, explore the values and implications for health of LME with them, report on their experiences as they perceive and narrate them, and let their recommendations guide any proposal of public health interventions to improve women’s sexual health. Our approach agrees with efforts to deconstruct the Western image of Africans led by the feminists Sylvia Tamale and Signe Arnfred in their invitations to the scholarly community to “rethink” African sexualities (Arnfred, 2004; Tamale, 2011). Our approach also agrees with Benson Mulemi’s proposal to employ Afrocentric approaches to “ameliorate” the representation of African women by means of assuming our responsibility, as researchers, to coproduce knowledge and to explain participants’ reality from their emic perspectives (Mulemi, 2012).
The majority of studies on sex and gender matters that have a component of IDI count on researchers and respondents being of the same sex (C. L. Williams & Heikes, 1993). Nevertheless, there are exceptions. In high-income countries such as the United States, men researchers have interviewed women on issues as private as, for instance, recovery of their sexual function after an acute myocardial infarction (Abramsohn et al., 2013). Female researchers have interviewed men in Switzerland on very sensitive issues such as sexual dysfunctions in adolescence (Akre, Michaud, & Suris, 2010). Looking at the pace at which African societies are entering the global village, is it realistic to assume that African women live in such a stagnant environment that they cannot be interviewed by men? Are we, as researchers from Western countries, contributing to maintaining the patriarchal status quo whereby some east and southern African women inhabit, interact, and move in different gendered spaces than men? Globalization, the impact of the mass media, improved access to education and health services, and recent public exposure of private matters led by the need to hinder traditions that place women in a more vulnerable position than men to HIV transmission, and so on, are blurring the frontier between what men and women can discuss between them, in public forums, with health practitioners, and with researchers of either sex.
Future Prospects
The biological sex of the researcher might not have as strong an influence on the research process and the research outputs as the choice of methodology used to conduct research on women’s matters. Both female and male researchers could contribute to Tamale’s, Arnfred’s, and Mulemi’s endeavors to ameliorate the representation the West has created of African women’s sexualities from the etic perspectives of the anthropologists of the colonial era. Whatever methodological choices researchers of either biological sex make, they should always count on women’s perspectives to generate knowledge. The literature could benefit from researchers reporting on how they engaged themselves in exploring women’s sexual matters. Experiences such as the one reported in this article could help researchers make informed methodological choices in future research on LME and other FGMo.
African women must be involved in a discussion on the circumstances in which men researchers should be allowed to investigate women’s issues. There needs to be a debate about the taboos surrounding certain FGMo for the population under study, for the academic community, ethics review boards, and for the researchers themselves. Furthermore, Giesler’s study on the experiences of men social work students in a university in United States may provide a useful framework for future research (Giesler, 2013). Researching women’s private issues as a man is a nonnormative profession, so it would be instructive to adopt Giesler’s multiple masculinities approach to analyzing how men researchers “do” gender when researching women’s issues in a sub-Saharan African setting.
Further research should also be carried out on which grounded theory approaches can help to erode the power dynamics than could place a researcher—woman or man—in a hierarchical position of superiority when interviewing women. A systematic review of experiences with grounded theory in research on traditional practices in sub-Saharan Africa might foster better understanding of the role different interpretations of grounded theory and grounded theory-derived methods and tools can play in the cogeneration of data. It may also assist theory coconstruction in collaboration with participants who are expected to step forward and disclose their most sensitive issues in order to promote social change and improve the health and well-being of the women in the region.
Conclusion
Constructivist grounded theory, enriched by a feminist perspective, might be a suitable methodological approach for the examination of traditional FGMo. In our study, this approach enabled a man researcher to cogenerate knowledge on the implications for health of LME as perceived and experienced by Zambian women in Cape Town. In future research on women’s private issues, researchers must practice reflexivity to address their impact in the research process. Sharing previous research findings, being open to disclosing personal data at the participants’ request, and discussing the implications for practice of the study findings might assist in building rapport and in palliating the effect of a power imbalance in the researcher/participant relationship. A thoughtful consideration of all possible methodological options at the outset of any study with African women on traditional practices that might impact their health must be done in order to ensure that the study findings are useful for women’s health and for social justice.
Footnotes
Acknowledgment of the Importance of Reflexivity
Theoretical sensitivity (enhanced by a feminist perspective).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.