
Abstract
Nurse anthropologist, Madeleine Leininger, developed the culture care theory and ethnonursing research method to help researchers study transcultural human care phenomena and discover the knowledge nurses need to provide care in an increasingly multicultural world. The authors propose that the ethnonursing method can be useful for research that addresses providing care in other disciplines, including education, administration, physical, occupational, and speech therapy, social work, pharmacy, medicine, and other disciplines in which research findings have implications for human care and health. The authors discuss the culture care theory and describe the ethnonursing research method's enablers, data analysis phases, and qualitative evaluation criteria. The theory is presented as a guide for using research findings to design culturally competent and congruent care to promote well-being among diverse people, groups, communities, and institutions. Resources include a reference list of key source publications, a discussion of exemplar studies, and samples of a theory-based, open-ended interview guide and data coding system.
Keywords
Introduction
The idea for this article occurred after the authors presented a poster titled, “The Use of the Ethnonursing Qualitative Research Method to Study Culture Care, Cultural Competence, and Culturally Congruent Care,” during the 2009 Thinking Qualitatively conference at the University of Alberta's International Institute for Qualitative Methodology (IIQM) (see Appendix A). Conference participants proposed that the ethnonursing research method had potential for use in other disciplines.
M. M. Leininger—a nurse anthropologist world-renowned as an educator, researcher, theorist, and the founder of transcultural nursing—developed the culture care theory (CCT) and ethnonursing research method to study transcultural human care phenomena (Leininger, 2006a). The method uses an open, largely inductive process to document, describe, understand, and interpret peoples' care meanings (how they experience and value care) and daily lifeways (cultural practices). The CCT and ethnonursing research method generate knowledge to help nurses and other professionals care for people from similar and diverse cultures in an increasingly multicultural world (Leininger, 2006b). The ethnonursing researcher acts as a co-participant to discover how people know, experience, and practice care in their daily lives. Observation of and participation and reflection with participants throughout the research process allow discovery of emic (people's) and etic (professional's) values, beliefs, care practices, and health practices.
The purpose of this article is to raise awareness of this method for researchers outside of nursing. The CCT and ethnonursing research method are useful for research that addresses providing culturally competent care or related concepts in education, administration, and health care disciplines such as physical, occupational, and speech therapy, social work, pharmacy, medicine, as well as any discipline in which research findings have implications for human care and health.
Birth of the Theory and Method
The ethnonursing research method—one of two research methods developed within the discipline of nursing—was designed at a time when nurses needed to shift from largely ethnocentric views to multicultural views in order to effectively serve people worldwide (Leininger, 1997; Ray, 1981). While studying the Gadsup Akuna people of New Guinea in the 1960s, Leininger (2006c) wanted to learn about their ways of caring from their emic (local or insider) view and how this contrasted with American and other Western lifeways. This project has served as the exemplar for subsequent ethnonursing research studies and contributed to the conceptualization of the culture care theory.
Evolution of the theory and method is documented in Leininger's major published works, which begin with her work in nursing and anthropology (1970) and culminate in the second edition of her culture care theory book (2006a; 2006b; 2006c), with subsequent journal articles published through 2012 (1978; 1985; 1990; 1995; 1997; 2002; 2011; in press).
Foundations of Culture Care and Ethnonursing
The culture care theory asserts that care is the essence of nursing and the dominant, unifying focus of the discipline, and care influences the health and well-being of people in profound ways within their environmental contexts. From an anthropologic perspective, Leininger (2006a) found that care is deeply embedded in peoples' worldviews, social structures, and values, thus, making it an elusive phenomenon that is challenging to study. Healthcare providers and other professionals need substantive knowledge in their disciplines to guide their care decisions and actions as they move beyond local and national perspectives to a global worldview. Professionals also need access to the care knowledge of diverse cultures to guide their clinical practices, teaching, curricular work, consultation, research, and administration.
Discovering embedded care phenomena requires an inductive, open-inquiry method that can explicate complex, covert, and largely unknown local people's views about care, health, and well-being. Using the construct of culture from anthropology and care from nursing, Leininger (2006a; 2006b) created the culture care theory and ethnonursing research method to advance a global perspective in nursing science and to establish the field of transcultural nursing.
The purpose of the CCT and ethnonursing research method is to discover, describe, and systematically analyze the care expressions, patterns, and practices of people in their naturalistic environmental contexts. The goal of the theory and method is to discover generic (folk) and professional care practices that promote health and well-being and to explore ways to use both types of care to plan and implement culturally congruent care that is satisfying, meaningful, and beneficial for people to achieve optimal health and to face disabilities or death (Leininger, 1997; 2006a).
Culture care theory has four major tenets:
culture care expressions, meanings, patterns, and practices are diverse and similar
worldview, multiple social structure factors, ethnohistory, environmental context, generic care, and professional care are critical influencers on culture care and predict health and well-being
generic/folk and professional care are essential for health and wellbeing
three action and decision modes guide the provision of culturally congruent care:
culture care preservation and/or maintenance
culture care accommodation and/or negotiation
culture care repatterning and/or restructuring. (Leininger, 2006a)
These theoretical tenets led to the formation of eleven related theoretical assumptions that researchers can use in Western and non-Western cultures in different geographical locations. These assumptions include the ideas that care is the dominant, central focus of nursing; care is essential for human health and well-being and survival; and culture care includes commonalities and differences (Leininger, 2006a, p. 18–19).
Orientational Definitions
The study of culture care involves complex phenomena, including what informants (participants) know and experience. To help the researcher discover this new, qualitative knowledge—and avoid focusing solely on a priori definitions— orientational (not operational) definitions are used in the ethnonursing research method. Cultures usually have their own care definitions, which need to be teased out during the research process. Orientational definitions are explicated inductively from the informants (research participants) and their situations based on what they know and experience. This process allows the researcher to access and define culture-specific knowledge. Essential terms of the theory and method explicated in previous work are listed in Table 1. These definitions are intentionally broad to allow the researcher to discover peoples' specific views about these terms. Hence, new dimensions of the definitions emerge as the research process unfolds (Leininger, 2006a).
Orientational Definitions
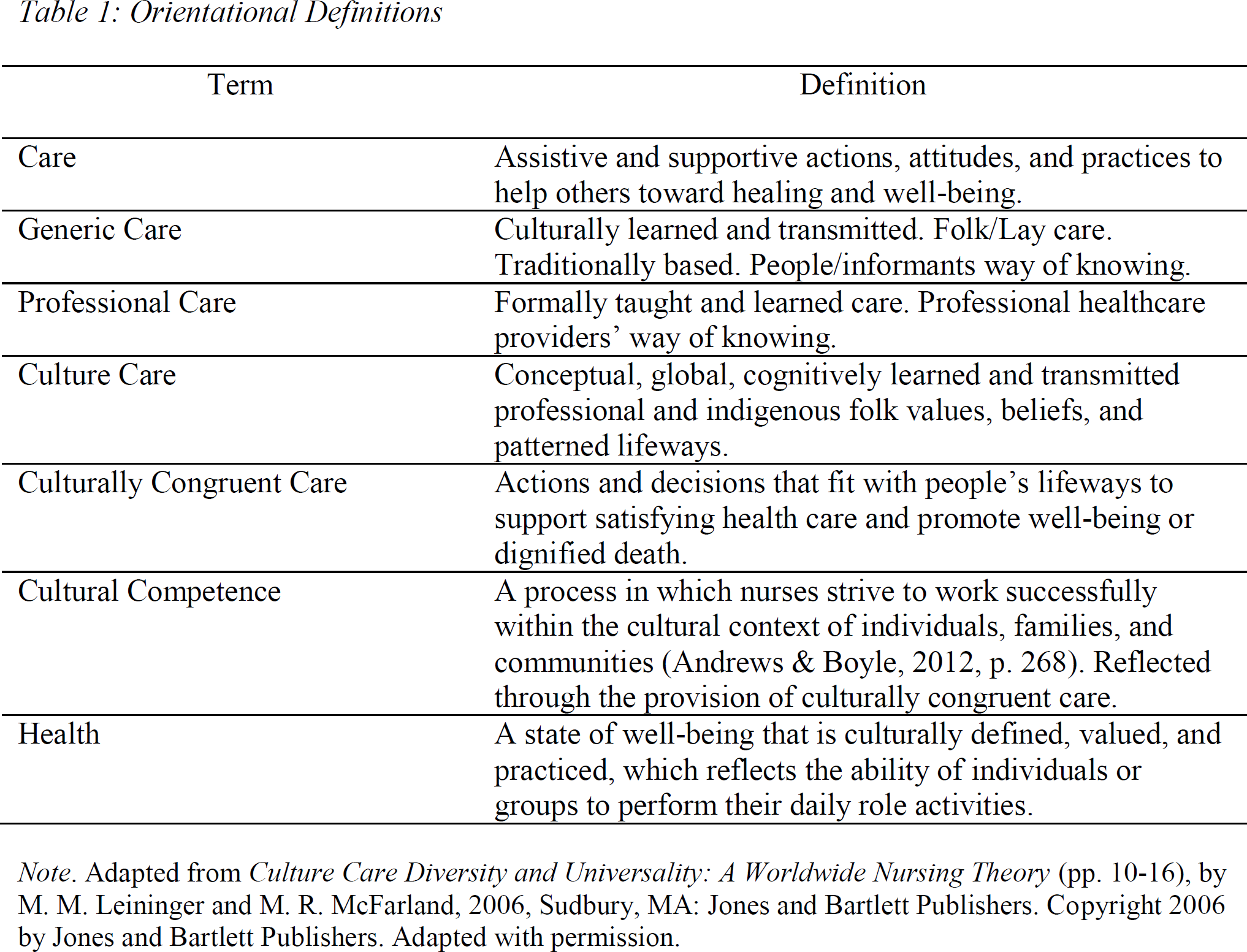
Note. Adapted from Culture Care Diversity and Universality: A Worldwide Nursing Theory (pp. 10–16), by M. M. Leininger and M. R. McFarland, 2006, Sudbury, MA: Jones and Bartlett Publishers. Copyright 2006 by Jones and Bartlett Publishers. Adapted with permission.
For example, in an ethnonursing study (guided by the CCT) with German-American elders living in a nursing home, generic care was orientationally defined by researchers at the beginning of the study as culturally learned and transmitted traditional folk/lay care. The orientational definition of generic care evolved throughout the study into care as doing for others through individual and collective care, care as families helping elderly family members, care as spiritual/religious helping, care as having the nursing home clean and orderly, and care as living the German-American lifeways and traditions (McFarland & Zehnder, 2006).
Ethnonursing Research Process
The ethnonursing research method includes five general principles to guide the researcher. The first principle advises maintaining an open discovery, active listening, and genuine learning attitude in working with informants in the total context in which the study is conducted. The researcher remains an active learner by showing a willingness to learn from the people, demonstrating respect, and avoiding ethnocentric bias. The second principle stresses actively participating with the informants in reflection about the meaning of what is seen, heard, or experienced. The researcher develops sensitivity to the emic (local) view and considers how this affects the etic (professional) perspective. The third principle encourages recording whatever is shared by informants to preserve their ideas and meanings. The fourth principle emphasizes using an experienced ethnonursing research mentor to guide the research. The fifth principle clarifies the purpose of using ethnonursing in combination with another research method (Leininger, 2006b). Primary and definitive sources about the ethnonursing research method, such as classic articles and book chapters, are included in the reference list. These in-depth resources provide detailed descriptions and examples of the major phases of the ethnonursing research method.
Researchers should develop their domain of inquiry (DOI) or study focus based on their general interest in and major hunches about care and culture. Broad research questions without preconceived responses can guide the researcher's thinking and allow new discoveries to be made. Study participants in the ethnonursing method are called informants. Key informants are those people holding the most knowledge about the DOI or major focus of the study. General informants may not be as knowledgeable about the DOI, but their general ideas can stimulate the researcher to reflect on similarities and differences in the research data among informants (Leininger, 2006b).
Research Enablers
Research enablers are important guides that help the researcher tease out in-depth culture care and general cultural knowledge from informants living in diverse cultural contexts. The Sunrise Enabler (Figure 1) serves as a cognitive map of the culture care theory (Leininger, 2006b).

Leininger's Sunrise Enabler to Discover Culture
The Sunrise Enabler provides a guide for the researcher to explore multiple influences on care and culture. The Observation, Participation, Reflection Enabler helps the researcher to enter the informants' world and remain with them throughout the study. With this enabler, the researcher gradually moves from being an observer and listener to an active participant. During the reflection phase, which occurs throughout the study, informants provide essential confirmatory data about the research phenomena. The Stranger to Trusted Friend Enabler helps the researcher befriend the informant to obtain authentic, credible, and dependable data. When the researcher becomes a trusted friend, informants generally will be more open about sharing their insights (Leininger, 2002; 2006b).
In the ethnonursing research process, an Open-Inquiry Guide Enabler is developed to encourage in-depth, open-ended interviews with informants. The guide is based on the components of the culture care theory and Sunrise Enabler and is customized for each study based on the domain of inquiry and the research questions. The use of this enabler encourages informants to share their ideas about care and other phenomena of interest. McFarland (1995) customized an inquiry guide to study Anglo- and African American elders living in a long-term care institution (see Appendix B). A description of the Phases of Ethnonursing Data Analysis Enabler guides the researcher through four sequenced phases of analysis as follows (Leininger, 2006b).
Four Phases of Data Analysis
The researcher begins data analysis on the first day of the research study and continues with regular coding and analysis of all data until the end of the study. In phase one, the researcher analyzes detailed raw data, including recorded and transcribed interviews, observations, participatory experiences, and field notes.
During the second phase, data are coded and classified as they relate to the domain of inquiry and research questions. Researchers may find qualitative software such as NVivo useful for organizing data. The data coding system has categories and domains labeled from constructs in the culture care theory (see Appendix C; McFarland, 1995). Additional unique codes specific to a study or discipline may be added or codes not applicable to a study may be deleted.
In phase three, data are scrutinized to discover saturation of ideas and recurrent patterns of similar and different meanings. Here, the use of the CCT enhances the ethnonursing research method as the researcher examines both the universal and diverse meanings of care. Discovering the commonalities people share as well as their differences is essential for knowing peoples' values, beliefs, and practices within their environmental context. Often comparing and contrasting cultural similarities and differences leads to findings that would not have been discovered if only diversities had been considered. In working with the theory and method over many years, the authors have found that cultural similarities often provide the glue that binds people together within the human family. Many people value the same cultural and social structure dimensions, such as family and religion; however, the related care patterns are similar and diverse within and among cultures.
For example, German-American Lutherans (McFarland & Zehnder, 2006), African-American Baptists, Anglo-American Methodists (McFarland, 1997), and Lebanese- and Syrian American Muslims (Wehbe-Alamah, 2006; 2011) universally valued care provided by their families. However, diversity was reflected in the care patterns specific to each cultural group. German- and Anglo Americans valued care provided by their spouses and adult children while African Americans valued care from their extended families, including “brothers and sisters” who were members of their churches (McFarland, 1997; McFarland & Zehnder, 2006). Lebanese- and Syrian American Muslims valued care from their extended family members; however, because they had immigrated to the United States and were without family nearby, they traveled yearly to Lebanon and Syria during the summer to experience care while visiting with family and friends (Wehbe-Alamah, 2011).
Spiritual or religious care was found to be universally essential to enhance health and well being and maintain satisfying lifeways for elders from diverse cultures. However, diversities were reflected in the care patterns of different groups. For example, in an ethnonursing study of Anglo-and African American elders in a long-term care setting, it was discovered that both groups valued and received religious and spiritual care from their respective churches (McFarland, 1997). The presence of a Methodist chaplain and the support given by several Methodist churches in the community where the retirement home was located helped Anglo elders face living out their lives in an institutional setting with increasing disabilities and the inevitability of death. Community church choir members frequently sang at the church services conducted in the retirement home and women's groups helped with craft activities. African Americans living in the same retirement home received a more personal form of care from church members who were considered family. They did banking and laundry for elders and often transported them to medical and dental appointments. German Americans valued living in a Lutheran home that was owned and operated by the church. Since German was the first language of most residents, church services in German were held weekly in the nursing home chapel. Elders related that the spiritual care offered by the Lutheran chaplain at the nursing home helped them get through each day (McFarland and Zehnder, 2006). Elderly Polish Americans valued living in their own homes in their Polish-American neighborhood close to the local Polish-American Catholic church. Spiritual care was viewed as having opportunities for attending services, visiting, and eating daily lunches with their neighbors in the church basement, which served as a senior meal site (McFarland, 2002).
The fourth, and last, phase of data analysis includes interpretation and synthesis of findings. The researcher explicates and confirms major themes, care actions and decisions, and new theoretical formulations with the informants (Leininger, 2006b). Follow-up interviews—via face-to-face meetings, phone calls, or emails—help clarify interpretations, meanings, and findings. It is important to note that these data analysis phases are not linear; rather, the researcher is involved in all four phases at various points in the study. For instance, data is confirmed with informants at every phase of the study. Mixer (2011) conducted an ethnonursing research study to discover how nursing faculty in the South Eastern United States teach culturally competent care. The researcher followed up lengthy face-to-face interviews with faculty informants via email and telephone conference calls to confirm research findings. Findings revealed students were taught to provide culturally congruent and competent care through role-modeling in clinical settings but without an organizing theoretical framework. The researcher recommended the use of a framework, such as the culture care theory, to promote student learning based on evidence from transcultural nursing research and to help them understand culture within the context of a broadened worldview.
Qualitative Criteria for Evaluating Ethnonursing Research
Qualitative research has its own unique purposes, history, philosophical foundations, and methodologies. Lincoln and Guba (1985) and other methodologists have developed qualitative evaluation criteria. Leininger (1991a; 1991b) acknowledged their work and further developed six qualitative criteria to evaluate ethnonursing research: credibility, confirmability, meaning-in-context, recurrent patterning, saturation, and transferability. Credibility refers to the truth, accuracy, and believability of findings established mutually by the researcher and informants over time. Confirmability refers to establishing verifiable and direct evidence with participants. The researcher confirms with informants the accuracy of patterns and themes formulated based on data collected. Data are maintained and systematically documented to ensure findings can be traced to actual data collected, which provides an audit trail. Meaning-in-context focuses on the significance of interpretation and understanding of the actions, events, communications, and other activities of informants within their environmental context. Recurrent patterning refers to experiences, human events, and lifeways that reflect the tendency to occur in patterned ways over time. Saturation refers to the notion that data is collected until redundancy occurs; informants share similar content and the researcher notes recurrence of the same information. Transferability refers to whether the findings of a particular ethnonursing research study would have similar meanings in another context with a similar cultural group (Leininger, 1991b; 2006b).
Using a research mentor is recommended when conducting an ethnonursing research study, and mentorship has been found to be useful for researchers to reduce biases; to reflect on the data and ensure findings are well grounded; and to facilitate meaningful linkages with similar and diverse data and discoveries from other ethnonursing research studies (Leininger, 2006b). Ethnonursing research method mentoring has occurred in both face-to-face and electronic formats. However, if a mentor is not readily available, many published ethnonursing research studies and other resources provide detailed descriptions of the research process. The reference list provides citations for selected culture-specific studies and examples from these studies have been incorporated throughout this article.
Action and Decision Modes for Practice Disciplines
Researchers in a practice discipline generate findings to contribute to general knowledge, but they are also obligated to provide recommendations for applying that knowledge in practice. The culture care theory offers three action and decision modes for providing culturally congruent and competent care: preservation and/or maintenance; accommodation and/or negotiation; and repatterning and/or restructuring (Table 2).
Culture Care Theory Action and Decision Modes

Note. Adapted from Culture Care Diversity and Universality: A Worldwide Nursing Theory (p. 8), by M. M. Leininger and M. R. McFarland, 2006, Sudbury, MA: Jones and Bartlett Publishers. Copyright 2006 by Jones and Bartlett Publishers. Adapted with permission.
These three modes give the researcher a framework for using data discovered in ethnonursing research studies to design creative and practical approaches for providing culture-specific and holistic health care for diverse people, groups, communities, and institutions. For example, in an ethnonursing research study of rural Dominican Republic adults, informants expected their folk and spiritual care be combined with professional care. Using the modes of culture care preservation and culture care restructuring, the researcher recommended that healthcare providers should actively learn about these Dominican values and expectations and then create an environment that welcomes local folk caregivers and spiritual health practices (Schumacher, 2010). In another ethnonursing research study of botanical healing practices of elder African American women in the Mississippi Delta, culture care accommodation/negotiation was recommended to encourage elders with knowledge of botanicals with medicinal or therapeutic qualities to be members of the health care team (Gunn & Davis, 2011). These examples illustrate how the ethnonursing research method generates knowledge that assists healthcare professionals in the provision of care that is meaningful and culturally congruent for people.
Using the Culture Care Theory with Other Research Methods
The ethnonursing research method and culture care theory were developed to be used together. However, the theory can be used with other qualitative methods. Leininger (1997) contends that qualitative and quantitative paradigms have different philosophies, purposes, goals, methods, and desired outcomes; therefore, these paradigms should not be mixed within one study because this would violate the integrity of each paradigm. However, it is acceptable to mix research methods within a given paradigm as long as the philosophical premises and purposes are congruent. A researcher should have an explicit purpose to add or mix methods within a paradigm and the researcher needs to be fully knowledgeable about each method. While there are a number of qualitative research methods that can be used with the culture care theory, the choice of methods should fit the research interest, domains of inquiry, or phenomena under study. Ethnography, phenomenology, life histories, and focus groups have been used with the culture care theory and, sometimes, in combination with the ethnonursing research method (Leininger, 1990; 2006b).
Another option is to conduct parallel studies in each paradigm—one in qualitative and one in quantitative, either in sequence or at the same time with different participants—to compare findings in relation to the purposes of each paradigm (Leininger, 1997). For example, the authors of this article are conducting a series of sequential studies to discover the culture care competencies of nursing students and graduates from two universities at different points in their program progression —at graduation and later in their nursing practice. A quantitative tool is used to measure cultural competence while qualitative enablers with ethnonursing research and phenomenological methods will be used to discover the culture care values, beliefs, and practices of nursing students and graduates who strive to provide culturally congruent care.
Multidisciplinary Use of Ethnonursing Research Methodology
The ethnonursing research method has a long history of success in nursing. Researchers have produced substantive findings with diverse cultural groups, including gender-specific groups; institutional cultures and subcultures, e.g., deaf culture (McCreary & Coeling, 1999); homeless persons (Hubbert, 2005); elders (McFarland, 1997); children; teenage gang members (Morris, in press); adults; students and faculty (Mixer, 2011); diverse cultures in the workforce (McFarland, 1997); and in program evaluation (McFarland, Mixer, Lewis, & Easley, 2006). These studies document valuable, evidence-based knowledge and culturally congruent care practices that are potentially transferable for use by health care providers in other disciplines. All health care disciplines strive to provide culturally competent and congruent health care and educational services, conduct culturally competent research, and administer culturally competent organizations. Professionals from these disciplines seek to discover knowledge about care and health from the peoples' points of view to ensure that their care is acceptable and satisfying. Use of the culture care theory and ethnonursing research method has multidisciplinary relevance because all these professionals—whether they practice in homes, clinics, hospitals, schools, or communities—seek to provide satisfying and culturally competent care for their clients.
The universal discovery among ethnonursing research studies has been the need and desire to combine generic and professional care to provide culturally congruent care for patients, families, community members, students, faculty, or administrators. The authors propose it is essential for other disciplines to discover care constructs and unique ways to combine generic and professional care for their own clients. Culture care research—using the ethnonursing research method guided by the culture care theory—within and across health care disciplines has the potential to promote multidisciplinary, coordinated, and integrated culturally congruent plans of care for optimal health outcomes and increased client satisfaction.
Conclusion
This article has offered a research method and a theory to health care professionals and others that could facilitate discovery of evidence-based and culturally competent care specific to their discipline. The ethnonursing research method and the culture care theory assist in discovering, honoring, and enhancing people's ways of knowing and give credence to the way people want to be cared for. Researchers from health care disciplines who are interested in discovering care phenomena with cultural implications from the people's point of view are invited to consider using the ethnonursing research method and the culture care theory as a method and framework for conducting relevant studies. The authors welcome comments and feedback.
Footnotes
Acknowledgements:
The authors wish to gratefully acknowledge Dr. Madeleine Leininger's development of the culture care theory and the ethnonursing method and to express appreciation for her ongoing support.
Appendix A
From “The Use of the Ethnonursing Qualitative Research Method to Study Culture Care, Cultural Competence, and Culturally Congruent Care,” by Mixer, S. J., Wehbe-Alamah, H., McFarland, M. R., & Burk, R., 2009, Poster session presented at the Thinking Qualitatively Conference, International Institute for Qualitative Methodology (IIQM), University of Alberta.
Appendix B: Culture Care of Anglo-American and African American Elders: Resident Open Inquiry Guide
This is an actual interview guide used in a research study. In this research, the investigator was studying nursing care provided to elderly residents. A researcher from another discipline would adapt the guide to reflect the healthcare provider and/or recipient of care being studied. For instance, a physical therapist would ask, “I am interested in learning from you about the physical therapy care/services you have received here” (I. Care –1.). This interview guide is presented as a template for a researcher from another discipline to adapt for his/her study.
Is there anything else you want to tell me about your life here?
Or about the care you receive here?
About your health since you have been here?
From Culture Care of Anglo- and African American Elderly Residents within the Environmental Context of a Long-term Care Institution, by M. R. McFarland, 1995, Doctoral dissertation, pp. 269–273. Copyright 1995 by M. R. McFarland and adapted from Culturalogical Care Assessment Guide. In M. M. Leininger (Ed.), Culture care diversity and universality: A theory of nursing (pp. 73–117), by M. M. Leininger, 1991, New York, NY: National League for Nursing Press. Adapted with permission.
Appendix C: Coding Data System for the Leininger,Templin,and Thompson Field Research Ethnoscript
This is an actual coding guide from a research study conducted by a nurse with residents in a long term care setting. A researcher from another discipline would adapt this template to reflect the healthcare provider, the recipients of care, and the context of the study. For instance, a physical therapist might want to change the code “professional nursing care” to “professional physical therapy care/services” (Category III, Code 25).
CATEGORIES AND DOMAINS OF INFORMATION
(Includes observations, interviews, interpretive material, and non-material data)
CATEGORY I: GENERAL CULTURAL DOMAINS OF INQUIRY
CATEGORY II: DOMAIN OF CULTURAL AND SOCIAL STRUCTURAL DATA
(Includes normative values, patterns, functions, and conflicts)
CATEGORY III: CARE, CURE, HEALTH (WELL-BEING) AND ILLNESS OF FOLK AND PROFESSIONAL LIFEWAYS
CATEGORY IV: HEALTH AND SOCIAL SERVICE INSTITUTIONS
(Administrative norms, beliefs, and practices with meanings-in-contexts)
CATEGORY V: LIFE CYCLE and INTERGENERATIONAL PATTERNS
(Includes ceremonies and rituals)
CATEGORY VI: METHODOLOGICAL AND OTHER RESEARCH FEATURES OF THE STUDY
From Culture Care of Anglo- and African American Elderly Residents within the Environmental Context of a Long-term Care Institution, by M. R. McFarland, 1995, Doctoral dissertation, pp. 285–288. Copyright 1995 by M. R. McFarland and adapted from personal communication, M. M. Leininger, (Fall, 1992). Adapted with permission.