
Abstract
Translation issues emerged from a qualitative study, conducted in French and English, that gathered patient perspectives on a newly implemented undergraduate medical curriculum entitled Physicianship: The Physician as Professional and Healer. French-speaking participants were interviewed using a translated interview guide, originally developed in English. A major finding that francophone participants contested the idea of the physician-healer in a manner not witnessed among the anglophone participants. Consultation with multilingual health professionals was undertaken to explore whether the contestation was the result of poor translation of the word healer. This process confirmed that no appropriate French equivalent could be found. With hindsight, the authors emphasize the importance of pretesting translated research instrumentation. An ecological perspective on language equivalency is also emphasized, in which emergent linguistic discrepancies are viewed as opportunities for learning about the culture-language relationship.
Introduction
In 2005 the McGill University Faculty of Medicine implemented a new undergraduate curriculum entitled Physicianship: The Physician as Professional and Healer. The impetus for the new curriculum was to develop medical student comprehension of what it means to have a mindset of a physician, above and beyond the scientific and technical aspects of clinical proficiency. The curriculum underscores the idea that healing is the primary mandate of medicine and that professionalism is the way in which the physician delivers that mandate. The program offers courses on healing and professionalism and emphasizes a revised clinical methodology grounded in observation skills and narrative competence. Other elements include training in attentive listening, communication skills, physical examination, clinical thinking and reasoning, and self-reflection. Further detail of the curriculum's theoretical framework is provided elsewhere (Boudreau, Cassell, & Fuks, 2007).
As an adjunct to implementation, curriculum planners established a research agenda aimed at elucidating the perspectives of the main stakeholder groups in medical education: patients, students, and teachers. In this article we discuss the methodological issues that arose from an exploratory study conducted with patients. The study, entitled Patients' Perspectives on Physicianship: Implications for Curricular Reform (Boudreau, Jagosh, Slee, Macdonald, & Steinert, 2008), was conducted with adult patients (N = 58) from the main teaching hospitals of the McGill University Health Centre (MUHC). The project gained approval from the institutional review board of McGill University and the MUHC prior to the start of data collection. Patients were asked to share their understandings and experiences of being ill and to provide personal examples of positive and negative experiences with medical care. They were asked to share their thoughts on educating medical students under the banner of physicianship, define the concepts professional and healer, distinguish between healing and curing, offer their advice to physicians-in-training, and give recommendations to curriculum planners.
The MUHC is required by law to offer services in both French and English. Because of the bilingual and multicultural context of the clinical setting, the research was conducted in both languages, giving French- and English-speaking patients an opportunity to provide input on curriculum reform. All five members of the research team were English speakers. One member was unilingual; the other four were partially bilingual in that they could read and speak but not write in French. Two (the two authors of this paper) of the five members were responsible for conducting all of the interviews. Out of 58 interviews, 10 were conducted exclusively in French, 3 involved a mixture of French and English (with French predominating), and the remaining 45 were conducted in English. The interviews were tape recorded and transcribed; however, no transcriptions were transcribed from one language to another, meaning that a dual-language interview set was used for coding and analysis.
The research was not designed to compare perspectives between the French and English data. However, the difference of perspective concerning the physician-as-healer concept between French- and English-speaking participants was a predominant finding and needed to be addressed early on in the study. In this paper we describe our experience in the search for language equivalency and report on the theoretical and practical insights gained concerning translation and the piloting of translated research instruments.
Approaching translation
Numerous authors have cited the importance of incorporating translation theories and methodologies into the design and implementation of cross-cultural research (Brislin, Lonner, & Thorndyke, 1973; Lonner & Berry, 1986; Overing, 1987). The literature on translation theory originates in quantitative research fields for the application of survey, questionnaire, and psychological test instrumentation across multilingual settings. In that context, the standard approach to translation has been the technique of back-translation, in which the research instrument is written in the source language, translated into the target language, and then retranslated into the source language (Brislin et al., 1976; Werner & Campbell, 1970). The three documents are then analyzed and piloted with a sample participant population to test for consistency.
Critics of the back-translation approach point to its basis in positivism, arguing that the technique “makes global assumptions that research is language free and that the same meaning in the source language can be found in the target languages” (Larkin & Dierckx de Casterlé, 2007, p. 469). The critique is that back-translation focuses on linguistic equivalency while glossing over key relevancies of cultural context. Shenkar and Von Glinow (1994, cited in Usunier 19991), have exemplified the problem by pointing out that the word autonomy cannot be adequately translated into a Chinese language. Back-translated results such as “right of self-determination” convey a significantly different meaning. Sechrest, Todd, and Zaidi (1972), similarly, have suggested that words such as responsible, suggestible, aloof, and tough have nuances within the English medium that creates difficulties in finding just the right equivalents in other languages. Interviewing, a qualitative method, provides the interviewer with the opportunity to explore language equivalency issues with participants during data collection. However, those designing multilingual qualitative research are still confronted with the task of adequately translating predesigned interview scripts (Larkin & Dierckx de Casterlé, 2007) as well as coding and analyzing multilingual interview data (Twinn, 1997). A common result of applying back-translation to qualitative research instruments such as interview scripts has been confusion over whether a particular finding should be attributed to lack of cultural equivalency or to substandard translation (Irvine et. al, 2007; Mullen, 1995; Schmieding & Kokuyama, 1995).
More recently, postpositivist perspectives concerning the practical and theoretical challenges of translation research have described translation as an act of cultural mediation or intercultural communication (Koskinen, 2004). Here, translation garners increased potential by expanding the scope of inquiry beyond linguistic equivalencies into the field of the language-culture relationship. Usunier (1998) noted that “comparing across cultures without awareness of language always results in biased and impoverished findings” (p. 49). Awareness of language means to understand how a given language is related to a given culture. “When one is dealing with ethnographic translations that seek to explicate the culture-language context from one culture into another, the concern should be with use of language in the social and cultural context' (Gales, 2003, p. 133).
To exemplify the meaning behind positioning language in its culture, linguistic scholars have suggested that English-speaking North America has a low-context culture. This means that linguistic meaning is not as deeply embedded in the culture as it is in other cultures (Boyaciggiller & Adler 1991; Hall, 1978; Yamazaki, 2005). Thus, a tendency exists among English-speaking North American researchers to underestimate the significance of language specificity in cross-cultural research in which English is the originator language (Gales, 2003). Boothman (2002), similarly, noted that although it might be possible to find an analogous concept from one paradigm (or language) to another, the significance of the particular concept might vary for each language. This idea is also similar to Mullen's (1995) perspective that cross-cultural research involves both translation and calibration. Whereas translation involves finding equivalency between source and target languages, calibration explores whether a word has the same placement or weight in the linguistic field of the target language as the source language.
These insights pertaining to translation research exemplify the radical shift in perspective that mark the field's transition from positivism to postpositivism. Wilss (2004) wrote,
Formerly the role of the translation scholar was characterized … by shaping and reshaping - sometimes approaching the limits of triviality—theoretical models of the translation process … There is now … a shift in the mode of scientific thinking in which results are no longer pre-fixed (prescribed), and predictable. (p. 780)
The ecological model of translation (Vinokurov, Geller, & Martin, 2007) captures the essence of this shift in thinking. An ecological view of a translation process is one that accounts for the unpredictability and uncertainly involved when working with the dynamics of the language-culture relationship. Ecology emphasizes the importance of the language context and the interplay of elements within the linguistic system. This framework treats source language and translated texts as equally legitimate cultural artifacts (Temple, 1997). Vinokurov and colleagues developed a step-by-step approach to pretesting for equivalency across languages while simultaneously working under the premise that “all hypotheses are true, even contradictory ones” (p. 2) and that “there are no right or wrong translations, just different versions that fit particular contexts” (p. 3). Using what they call a modified decentering technique, they consider the original language and the translated versions to have equal validity, thus treating translation discrepancies as reliable points of reference so as to uncover otherwise hidden meaning discrepancies between cultures or languages. This approach is rooted in the viewpoint that meaning is constructed as well as expressed by language (Barrett, 1992) and that expecting to always find universal conceptual equivalences across languages and cultures is a theoretically flawed principle. The ecological perspective does not suggest abandoning the search for linguistic equivalencies across languages. It simply contextualizes the search in the broader field of language, culture, and meaning. As Temple and Young (2004) stated, “the lack of one-to-one relationship between language and meaning does not absolve the researcher from investigating the role of language in cross-cultural research. Instead, it indicates that the boundaries of language are permeable” (p. 174).
Our translation experience
The original interview script was developed in English from a series of pilot interviews with English-speaking teachers, learners, and patients. Our methodological process in pretesting the research instrumentation is congruous with the general literature highlighting the importance of pretesting (Lindquist, 1991; Peat, Mellis, Williams, & Xuan, 2002; Prescott & Soeken, 1989). Pretesting was conducted to ask participants for feedback to identify ambiguities and difficult questions (Teijlingen, Hundley, & Graham, 2001); clarify and define the parameters of the study (Frankland & Bloor, 1999); and develop familiarity, confidence, and ease using the interview script (Holloway, 1997). The script was semistructured to encourage the exploration of uncharted but potentially relevant ideas for curriculum reform.
To prepare for the French interviews, an independent translation service translated the interview script and the consent form into French prior to the start of data collection. Although steps were taken to pilot the project to strengthen the validity of the questionnaire in English before translation of the script occurred, it was an oversight on our part to not pilot the translated French script with French-speaking patients. Pretesting translated research instrumentation is well documented, particularly in the literature on back-translation methodology (Brislin et al., 1973; Jones, 1987; McDermott & Palchanes, 1992) and less so for qualitative research involving translation (Larkin & Dierckx de Casterlé, 2007; Vinokurov et al., 2007). By not pretesting our translated instrumentation, we missed the opportunity prior to commencement of the study to investigate discrepancies in translation and arrive at potential solutions for the linguistic difficulties that were subsequently encountered once the French-language data collection began.
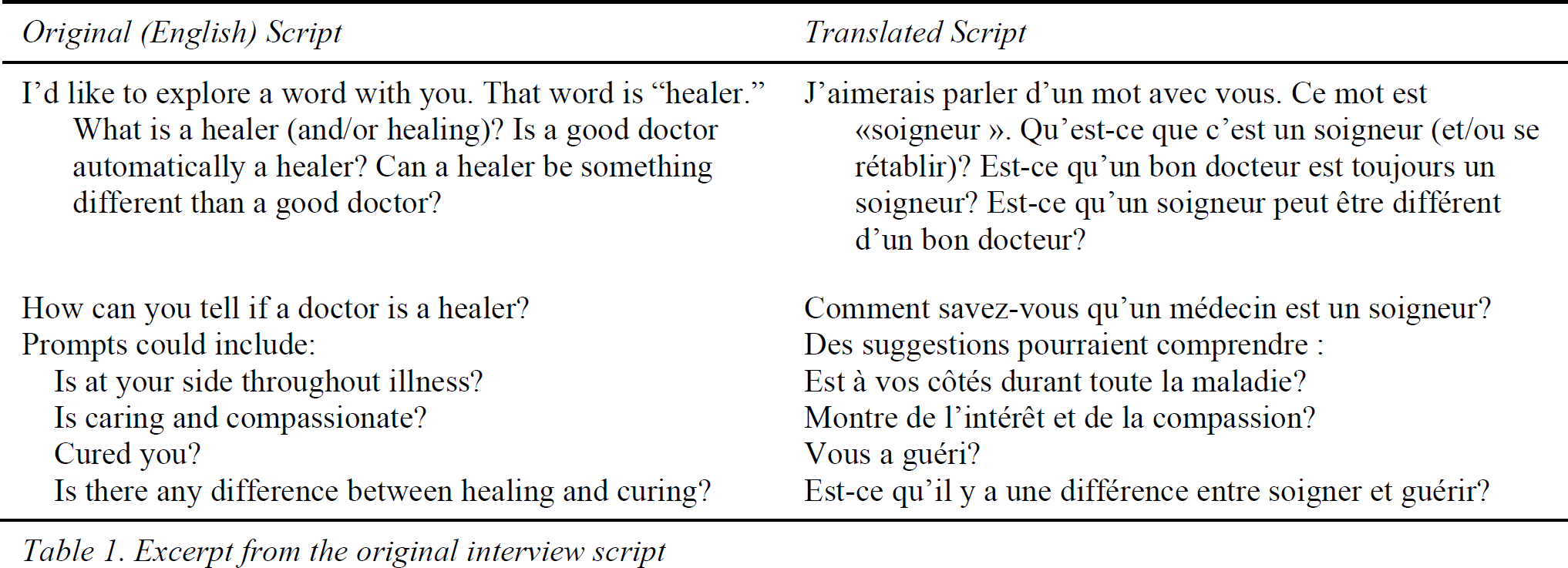
An issue that arose related to contestation of the term healer. The English title of the research project, as represented on various documents, including the consent form, was: Investigating the Patient's Perspective on the Physician as Healer and Professional. The title translated into French became Investigation de la Vision du Patient: le Médecin en tant que Soigneur et Professionnel. The noun healer was translated into French as soigneur, and the noun and/or adjective professional was translated as professionnel. The section of the interview script that dealt with the concept of healing included several prompts based on related and/or contrasting words. The French version of these prompts translated the noun healer as soigneur and the verbs healing as se rétablir and curing as guérir (Table 1). We used additional words and phrases during French interviews, including the noun guérisseur, which is usually translated as “healer” and/or “curer,” and the verb heal, used in both its transitive form (e.g., “The doctor heals [the patient]”) and intransitive form (e.g., “The patient heals [herself]”).
Excerpt from the original interview script
In this section we discuss some of our findings related to the issue of translation. Our exemplar French quotations and approximate English translations are provided in Tables 2 and 3. The masculine form of French nouns is used in this manuscript; in the actual interviews, both masculine and feminine forms were used. Specific words for which there appeared to be multiple meanings or for which the translation is not immediately obvious are highlighted and placed in parentheses: { }.


We discovered that the concept of professional was similarly conceived both English- and French-speaking participants. The words professional and professionnel were generally linked to interpersonal skills that could be captured with the phrase “good bedside manner.” The concept was described as behaviors and approaches such as “be encouraging, respectful, honest, compassionate, punctual, properly attired and a good communicator.” Professional was occasionally associated with a negative connotation, as in “maintaining a professional distance.” The extent to which comments about professionalism carried a negative connotation appeared to be similar whether the interviews were conducted in French or English.
For the terms healer and healing in relation to the role of the physician, only a few anglophone patients felt that the term was not suitable for teaching medical students to become doctors. Examples of negative descriptions included “gobbledygook,” “folklore,” and “smoke and mirror.” The majority had neutral or positive associations toward the term. Among English-speaking patients, the phrases associated with the word healing were often positive (e.g., “soothing,” “peaceful,” “warmth,” and “comforting”). Healing was generally described as a process whereby the focus is on emotional and spiritual dimensions of illness. It was seen as a desirable quality of doctoring.
In French, the concept of healer was problematic. Several participants vigorously resisted linking the word soigneur (our a priori linguistic equivalent for healer) with physicians. This tendency, to conceive of the function of healing as being preferentially attached to allied health personnel (e.g., a midwife) did not emerge as a salient feature of interviews conducted in English.
The significance of this finding was accentuated by the fact that the healer concept in question was one of the central aspects of the new curriculum. We were attempting to understand the perspectives of French-speaking patients of the healer role of the physician, yet study participants were hesitant to consider healer, translated using the term soigneur, as a characteristic of physicians. As our data collection progressed, we began to change our approach in the French interviews by telling our participants we were having difficulty translating the healer concepts into a suitable French form. This opened up a new dialogue in subsequent interviews about linguistic equivalency. When we encountered interviewees who were fluently bilingual, we explored the concepts using different words. Tables 4 and 5 contain quotations from bilingual interviews.

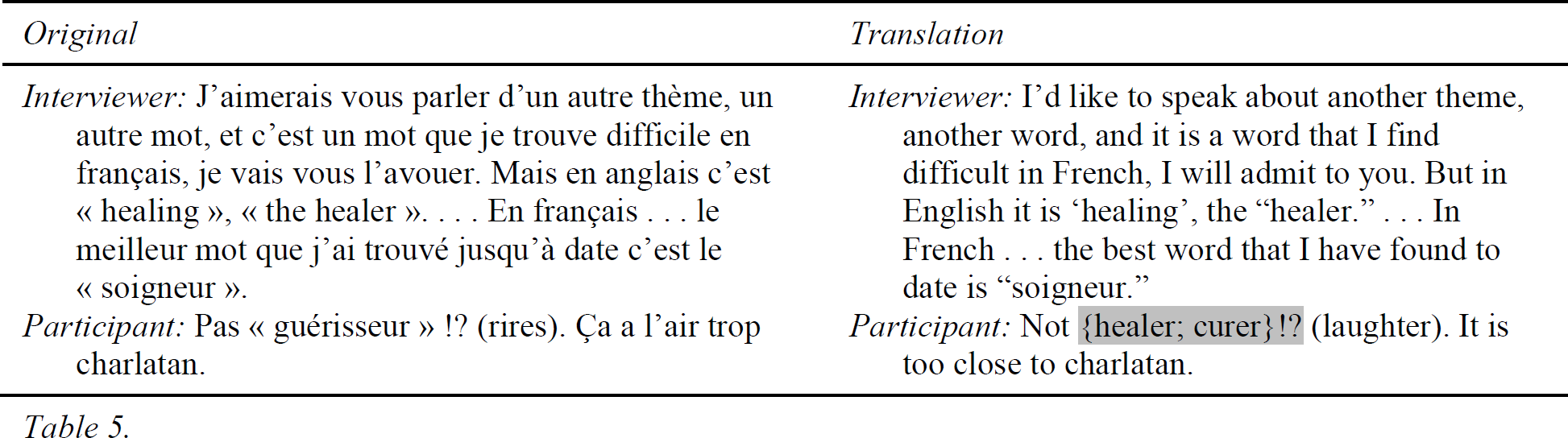
These two participants, when prompted to consider a French equivalent of the word healer, immediately mentioned the word guérisseur. This word is linked etymologically to the verb guérir, which is generally translated as both “curing” and “healing.” Although both terms, guérisseur and soigneur, were related to the concept of healer, neither was adequate in describing the healer role. For some French speakers, the concept of soigner lacked a sense of decision-making authority, which was deemed necessary for the doctor's role. Guérisseur, on the other hand, implied a definition of healing that was clearly outside the positive image of the doctor. Many viewed this word with suspicion or derision; examples of descriptions included “les société primitives” (primitive societies), “charlatan” (quack), and “sorcier Africain” (witch doctor).
In response to this linguistic challenge, we felt that asking them to find linguistic equivalents in French for the terms healing and curing could help to clarify the translation difficulties. However, questions aimed at elucidating the putative difference between healing and curing were met with confusion during French interviews. The following discursive exchange with a patient (who appeared to speak French and English equally well) and his spouse (who appeared to be more fluent in French than English) demonstrates the overlap in French between the concepts of curing and healing.
During this exchange between the interviewer, participant, and his spouse, the interviewer initially asked the question in English, to which the participant responded by translating the question into French for his spouse. He initially translated curing as “soigner” and healing as “guérir” but then decided that guérir encapsulates the meanings of both healing and curing.
After experiencing numerous instances of linguistic confusion during the French interviews, we decided to consult with multilingual health care workers for their perspectives on the language discrepancy. Four physicians, one psychologist, and two nurses were consulted. Five were bilingual (three had French as the maternal tongue, whereas for the other two it was English), and two were trilingual (English/French/Spanish and English/French/Armenian). We asked them to define the words curing and healing and propose translations in French, to define guérisseur and soigneur, and to reflect on the linguistic equivalence of these commonly used terms. The findings, which are summarized in Table 6, were congruent with the patterns that had emerged from interviews with patients. There was a greater tendency in English than in French to view healing and curing as distinct concepts. Although each term was polysemous, there appeared to be less variability with the term curing than with healing. The former was held to be something definitive and linked to disease. Healing was less clear cut, although for one person it evoked a surgical approach, and was associated with the person having a sickness rather than the disease. In French, the two terms were conflated and generally captured with the word soigneur. The term guérisseur was not imbued with much respect in the opinion of these health care professionals. Table 7 shows illustrative results from the consultative exercise with health care workers.


A perspective on cultural differences
Although it was beyond the scope of our study to explore in-depth the cultural differences related to the concept of healing, a few insights emerged concerning the relevance of the linguistic context of our research setting. For one, Hall's (1978) and Boyacigiller and Adler's (1991) observation that English North America has a low-context culture is helpful in interpreting our findings. As we already noted, their insight suggests that the language-meaning dyad is not as rigidly structured in the culture of English North America as it is in other cultures, including
Quebec. Interpreting the findings in this way would simply suggest that the words soigner and guerriseur in French have greater specificity of meaning than do the words curing and healing in English. English participants did not associate physician with healer on their own terms during interviews, but they typically accepted the association when it was presented to them by the interviewer. Alternatively, the French culture having a high (or at least higher) context might mean that the terms soigner and guerriseur in French could not be associated with the concept of the physician because it was imbued with greater specificity of meaning (midwife, allied health professional, etc.).
Another contextualizing factor is the fact that the concept of the physician-as-healer has only recently been reintroduced into medical education (Boudreau, Cassell, et al., 2007) despite the historically established association of the terms from ancient Greek conceptions of doctoring (Kearney, 2000). As the history of modern medicine unfolded, the concept of the physician healer fell out of favor. Thus, this history of association (in the ancient context), the de-association (during the era of modernity) and now the reassociation (in postmodernity) of the healer concept in medicine provides a tentative interpretation concerning the mixed reaction to the concept among participants of our study. For some, healer invoked the idea of a practitioner who operates outside the framework of modern science. Those who put their faith in the scientific aspects of modern medicine might find the association of physician with healer as contradictory or undesirable. Alternatively, those who believe that the mindset of the doctor should incorporate a way of thinking which is beyond the application of medical science and technique might be more apt to be sympathetic to introducing the idea of the physician-as-healer in medical education. However it is beyond the scope of the analysis here to suggest that the linguistic discrepancies between French and English speaking patients indicate a cultural divide of this nature. Further ethnographic and survey research would be needed to support such a claim.
Conclusion: Theoretical and methodological implications
Reflecting on the ecological approach to translation methodology, we view the nontransferability of language in our study as a research finding rather than a research failure. Although initially causing communication difficulties with French-speaking participants, it was humbling to discover that our terminology for curricular reform was grounded in a particular cultural worldview that could not be universally applied. The translation findings opened the door to new and unexpected possibilities for research inquiry. This has also been the experience in ethnographic research; in this context it has been stated, “Translation is neither of nuisance value nor strictly a technical problem but is the very essence of ethnographic research” (Kleinman, 1987, p. 451).
Given the insights provided by the translation issue, we have reflected on the implications of training physicians under the banner of physicianship within a bilingual clinical setting. One issue is the fact that the students accepted to the McGill Faculty of Medicine are culturally diverse, with many identifying themselves as members of the French-speaking community. Alongside their English-speaking counterparts, these students are required to learn about the concept of the professional and healer and reflect on their own development toward that end. Our research findings lead us to question whether there might be a difference in the way students of different linguistic heritages comprehend, attach meaning to, or develop professional identity though the healer concept. Although francophone students complete the bulk of their undergraduate training in English, it would be worthwhile investigating the extent to which particular linguistic and cultural references to the word healer determine outcomes in professionalization, enculturation, or the achievement of specific learning objectives. In addition, given this multicultural context, features of the Patients' Perspectives Study could be conducted with international students and with students of diverse ethnic origins to explore the multitude of connotations of the healer concept beyond the English/French context. Preliminary results of recent unpublished research with clinician-educators have indicated that the implications of our findings on patient communication is not an issue for educators, as the terms or labels “professional” and “healer” rarely arise in conversation with patients (Jagosh, 2009). Notwithstanding, the findings described in this article raise the question of whether or not it is appropriate for clinician-educators and their students to use the word healer when communicating with patients during visits to the teaching hospitals.
Although some variation exists among patients in terms of their expectations of the doctor-patient relationship, the macro-level findings of our study suggested that a core set of physician attributes and behaviors have common value among patients regardless of particular linguistic origin of patients. These include such ideas as the doctor's skill and willingness in listening to the patient's story, the doctor's respect for the patient's unique goals and desires, and the baseline expectation that doctors will diagnose and treat with up-to-date medical knowledge. This consensus about the vision of ideal doctor attributes is congruent with the general goals of the physicianship curriculum. Yet, despite the consensus on attributes, the professional/healer labels used to organize these attributes for teaching purposes might remain a terrain of contestation in the multicultural and bilingual patient population of the MUHC.
Through our experience, we adopted the ecological approach to translation theory. Had we operated through a positivist approach to back-translation methodology, expecting to eventually find linguistic equivalency, we could have spent unnecessary resources on an aspect that would have possibly led us to conclude failure in our efforts. For our purposes, discovering that the overarching framework for the physicianship curriculum had linguistic limitations was a significant finding. Further investigation of the healing concept could be undertaken to explore the deeper meaning in the French context.
Much of the literature on translation in qualitative research focuses on understanding the influence of third-party translators on the interview process (Temple, 1997) and outlining a method to incorporate translators in the preparation, collation, and interpretation of multilingual data (Larkin & Dierckx de Casterlé, 2007). In comparison to most published research on translation, our experience was unique in that no translators were used in the interview process and no translation of the data was undertaken after transcription. Our methodological issues, thus, were limited to translating and testing the terminology of the interview script. Because of the bilingual competencies of the research team, our collaborative analysis was not confined to one language, so the bilingual research process spanned the entire duration of the study, from initial design to final analysis. Yet in hindsight, piloting a number of French interviews using the translated interview script would have been helpful to identify the language discrepancy before data collection began. This would have prepared us for the possibility of language resistance and/or confusion in subsequent interviews. With an awareness of that reality, we could have included a set of unique prompts for French interviews appropriate to the discrepancy.
Our experience also suggests that self-reflexivity should be practiced among the research team concerning the particular cultural and linguistic backgrounds of the investigators. Despite the fact that most members of the team had a working knowledge of French, no one on the committee realized that the translated term for healer would be met with resistance. Had we reflected on the linguistic and cultural composition of the research team, it may have become clearer at the outset that piloting the French interview script was necessary. Given our unique context, our decision to consult with health care professionals midway through the study proved to be a valuable exercise. Having bilingual hospital staff of French Canadian heritage reiterate the same confusion as patients was indication that the language discrepancy could be generalized beyond a particular class or education-level demographic of the French-speaking study participants.
The ecological model for translation theory suggests that more important than finding language equivalency is pretesting research instrumentation to allow language discrepancies to emerge organically from the process. Once uncovered, these discrepancies should be treated as points of cultural learning. Our work revealed a number of considerations involving the cultural foundation and the linguistic limitations of the physicianship framework. We hope that our reporting on the lessons we learned and the steps we took concerning our dual-language research will be beneficial for other researchers who are engaged in multilingual research and must address issues involved in instrument translation and language equivalency.