
Abstract
Background
Intracranial aneurysms are increasingly detected incidentally due to broader use of neuroimaging. Intrasaccular devices are frequently used to prevent rupture, yet standardized follow-up and retreatment strategies remain undefined. We performed a scoping literature review and DELPHI consensus to gauge current practice patterns and expert opinions on managing intracranial aneurysms that were previously treated with intrasaccular devices.
Methods
A DELPHI consensus was conducted during an invite-only meeting of international neurointerventional experts. The process was informed by a scoping literature review and included three iterative rounds of structured questionnaires to establish consensus on follow-up imaging timing, modality, and retreatment decision-making.
Results
Twenty-four experts participated. The literature review identified 16 key studies, which were presented to the panel. For completely occluded aneurysms, MRA at 6 months was preferred by 58% of participants, with annual imaging favored thereafter. For incompletely occluded aneurysms, 6-month DSA followed by annual imaging was recommended. No consensus was reached on the imaging modality for annual follow-up. Retreatment decisions were primarily driven by aneurysm growth (>2 mm). Endovascular retreatment was preferred over open surgery, with risks such as ischemia and rupture identified as key concerns.
Conclusion
This DELPHI consensus highlights current practice trends and open questions in the follow-up and retreatment of aneurysms treated with intrasaccular devices.
Introduction
Unruptured intracranial aneurysms are present in approximately 3% of the general population, with higher prevalence among individuals with a positive family history or specific comorbidities. 1 Smaller aneurysms are less likely to rupture, and factors such as location and morphology also influence rupture risk. 2 Rupture can result in devastating consequences, with high morbidity and mortality rates.3,4
Asymptomatic unruptured intracranial aneurysms (UIA), especially smaller ones, are being increasingly detected due to more frequent use of neuroimaging to investigate common conditions such as headache or cognitive decline. The increase in incidentally discovered, small UIA warrants careful evaluation and management strategies to balance risk of rupture vis-à-vis treatment complications. Both over- or under-treatment should be avoided, and patient concerns and anxiety need to be managed appropriately. 5
Over the past decades, endovascular therapies have emerged as a safe and effective alternative to surgical clipping for treating ruptured and unruptured aneurysms.6,7 Intrasaccular devices are preferred in most centres to avoid long-term antiplatelet medication, which is needed when devices are left permanently in the vessel lumen as is the case in stent-assisted coiling or flow diversion. Newer intrasaccular devices, such as the Woven Endo Bridge (WEB), have expanded the therapeutic landscape and now allow for safe intrasaccular treatment of wide-necked aneurysms that previously required stent-assisted coiling or flow diversion.
While re-treatment is generally considered safe in cases of recurrence or progression after endovascular treatment with such intrasaccular devices,8–10 there is still a lack of standardized guidelines for follow-up imaging and retreatment decisions in these cases. 11 To address these challenges, a DELPHI consensus was initiated at the 5T Think Tank annual conference 2024. Leading experts in aneurysm treatment using intrasaccular devices collaborated to develop recommendations and explore key questions regarding the follow-up regimen, necessity, and timing of retreatment for aneurysms previously treated with intrasaccular devices. We aimed to provide insights into current practice patterns, summarize current evidence and expert opinions, and highlight critical knowledge gaps.
Methods
5T Think Tank attendees and sponsorship
The DELPHI consensus was conducted as part of the 5T Think Tank, held in September 2024 in Banff, Alberta, Canada. This annual three-day, in-person meeting brings together international experts in neurology and neurointervention, including neurologists, radiologists, and neurosurgeons. The 2024 meeting focused on discussing the latest research and future advancements in interventional stroke and aneurysm therapy, with a particular emphasis on areas with insufficient evidence and scarce data. Attendance is by invitation only, with careful attention to assembling a diverse panel representing various specialties, countries, and genders. Sponsorship for the 5T Think Tank was equally provided by Medtronic, Stryker, Terumo, Cerenovus/J&J MedTech, and Penumbra; however, the sponsors had no influence over the guest list, discussion topics, or presentation content. The preparation and analysis of the DELPHI rounds were conducted independently by 5T Think Tank participants unaffiliated with the sponsors.
Delphi methodology
The DELPHI method is a systematic approach designed to gather and refine expert opinions through an iterative process, making it particularly useful in situations where robust evidence is lacking. In medicine, it is used to establish interim guidelines and standardize patient care until more definitive evidence becomes available. 12 A panel of experts who respond to a series of structured questions. Their responses are anonymized and summarized after each round, allowing participants to reconsider their opinions in light of the group's feedback. This iterative refinement continues until a consensus is reached or the responses stabilize. 13 By ensuring controlled feedback and anonymity, the method minimizes bias and ensures a balanced contribution from all participants, resulting in recommendations that reflect collective expertise. We applied the DELPHI methodology to address complex decision-making scenarios for follow-up and re-treatment of intracranial aneurysms previously treated with intrasaccular devices. A flow chart of the methodology is illustrated in Figure 1.
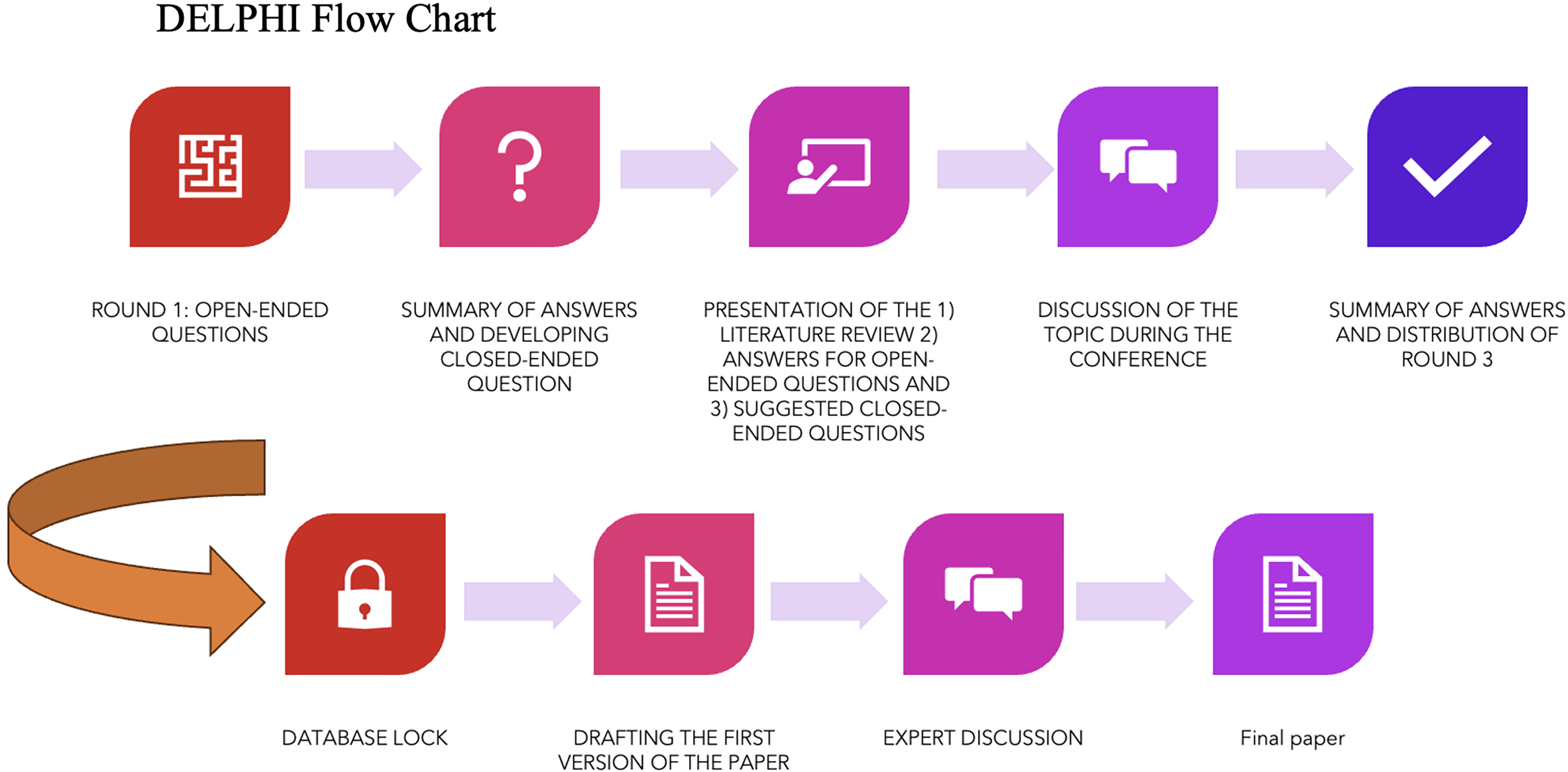
DELPHI flow chart. This figure shows the DELPHI process from developing the open-ended questions to presentations and summary to the final expert discussion and manuscript writing.
Literature review
As a part of the DELPHI consensus devising, a scoping literature search was performed to identify key publications on intracranial aneurysm treatment with intrasaccular devices. The purpose of the literature search was to identify high-quality retrospective cohort studies and meta-analysis focused on the recurrence, retreatment and rebleeding or late bleeding rates in treated aneurysms and to identify factors associated with recurrence/retreatment. Due to the heterogeneity of the studies, the literature review included both ruptured and unruptured aneurysms. One of the co-authors (PC) summarized and presented the results of this search during the live session.
Delphi rounds
Following the review of the literature, the first round of the DELPHI consensus was initiated with four open-ended questions focusing on the management and re-treatment of intracranial aneurysms previously treated with intrasaccular devices. The four questions were as follows:
In your opinion, what are the current best practices for follow-up imaging after intrasaccular treatment (i.e., coiling or intrasaccular flow disruptor), and how often should imaging be performed to effectively monitor patients? Do you think it should be standardized or an individual approach? If you favor an individualized approach, what factors would you take into account for decision-making? What factors should be considered when deciding whether to retreat a residual or recurrent aneurysm detected on follow-up imaging after initial treatment with intrasaccular devices (i.e., coiling or intrasaccular flow disruptor)? What are the potential risks and benefits of retreating residual or recurrent aneurysms endovascularly? How should clinical and angiographical outcomes be measured and reported for patients undergoing retreatment for residual or recurrent aneurysms following intrasaccular treatment? Comment on both clinical and angiographic outcomes.
Based on the responses from round 1, closed-ended questions were formulated for rounds 2 and 3. The questions were identical in rounds 2 and 3. A total of 21 questions were developed, addressing key topics related to follow-up, retreatment, and outcomes. Initial questions focused on determining the optimal timing and modality for imaging follow-up. To identify factors prompting closer follow-up, participants ranked factors such as patient age, comorbidities, smoking status, functional status, and aneurysm characteristics according to their importance. Retreatment criteria were examined through both aneurysm-specific and patient-related factors. Further questions explored procedural aspects, including the safety and feasibility of retreatment, risks such as ischemic events, aneurysm rupture, and technical challenges. Lastly, questions were asked on appropriate and relevant clinical and angiographic outcome measures for assessing treatment success. The detailed questionnaire is displayed in Supplementary Material 1.
Data collection and analysis
The data collection process was conducted using an online survey tool (Qualtrics.com), with respondents’ email addresses recorded to prevent duplicate submissions. The first round of the survey was sent out to the attendees before the 5T meeting on August 22, 2024, and closed on September 15, 2024. The closed-ended questions were distributed to attendees on September 16, 2024, allowing them to review all responses prior to the meeting. During the 5T think tank, current evidence on the topic and a summary of the first-round responses were presented, followed by a 90-min group discussion. The second-round survey remained open after the meeting until October 3, 2024. Responses were summarized and shared with all participants. These results, along with the literature review and discussions, informed the third and final round. Participants were explicitly instructed to review the second-round results carefully before completing the third-round survey, which included the same questions as round two. Once the final round was completed, the database was locked on December 20, 2024, and two independent attendees who did not participate in the consensus (SLB and AS) analyzed the data. Consensus was pre-specified as ≥70% agreement for questions with multiple options or ≥50% agreement for single-option questions, identical to prior DELPHI consensus studies in neurointervention.14–16
Results
Data collection was from August 30 to December 20, 2024. A total of 24 participants contributed to the DELPHI consensus. A list of all participance of the DELPHI questionnaire and discussion is shown in Supplementary Table 1. An overview of the round 1 answers can be found in Supplementary Material 2. Key results of the consensus are shown in Figure 2.
Literature search results
Sixteen key publications were identified (see Table 1 and Supplementary Material 3).
Key publication results of the literature search.
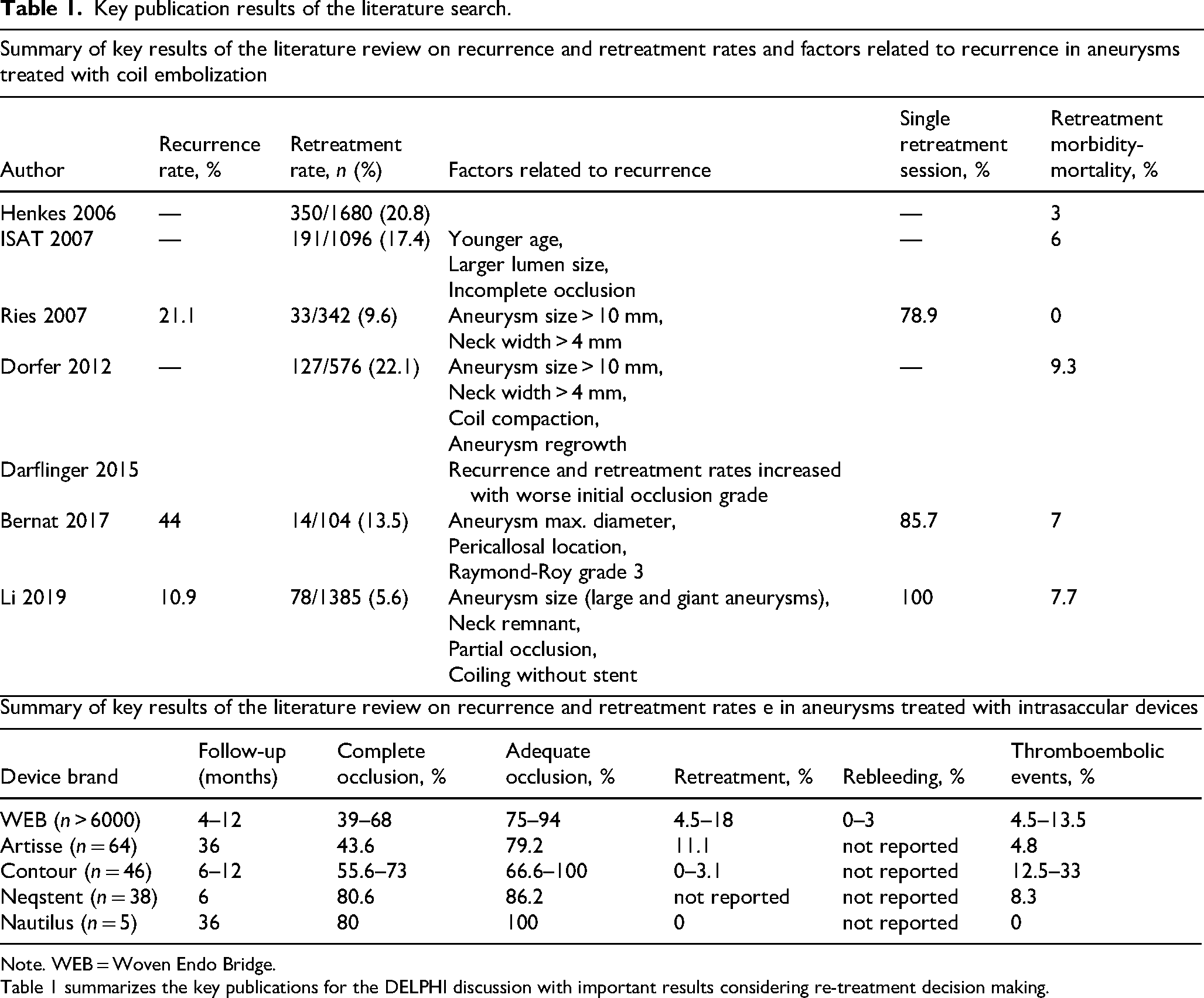
Note. WEB = Woven Endo Bridge.
Table 1 summarizes the key publications for the DELPHI discussion with important results considering re-treatment decision making.
Follow-up of completely occluded aneurysms
The panel achieved consensus that the most appropriate time point for reimaging of a completely occluded, unruptured aneurysm treated with an intrasaccular device is 6 months (14/24, 54% experts, Supplementary Figure 1). There was consensus on MRA as the preferred imaging modality for the first follow-up (16/24, 58% /experts, Supplementary Figure 2). A 1-year interval was identified by consensus as the preferred timeline for subsequent follow-up imaging (12/24, 50% experts, Supplementary Figure 3).
No consensus was reached on the preferred imaging method for subsequent follow-ups, although Three-Dimensional Time-of-Flight (3D TOF) (10/24, 42%) and Contrast-Enhanced Magnetic Resonance Angiography) (CE-MRA) (8/24, 33%) were the most favored options (Supplementary Figure 4). Although there was no consensus on when a Digital Subtraction Angiography (DSA) should absolutely be performed, the most commonly chosen answers were “before considering retreatment” (10/24, 42%), followed by “when reperfusion is suspected” (7/24, 29%) (Supplementary Figure 5).
Follow-up of incompletely occluded aneurysms
There was consensus that the first follow-up imaging of an incompletely occluded aneurysm should be performed at 6 months (15/24 [63%]) (Supplementary Figure 6), and that the imaging modality used in this case should be a DSA (12/24, 50%) (Supplementary Figure 7).
Consensus was also achieved on annual subsequent follow-ups in case no re-treatment is performed (12/24, 50%) (Supplementary Figure 8). However, there was no consensus on the imaging modality, with 11/24 (46%) experts being in favor of 3D TOF MRI and 9/24 (38%) opting for CE-MRA (Supplementary Figure 9).
The top 5 picked factors for closer follow-up imaging considerations (other than suboptimal occlusion or rupture) were “large/giant aneurysm” (20/24, 83%), “other comorbidities” (18/24, 75%), “packing density” (16/24, 67%), “type of device” (14/24, 58%) and patient age (13/24, 54%) (Supplementary Figure 10). Previous SAH/rupture (17/24, 71%) and extent of recurrence/recanalization (13/24, 54%) were considered strong indications for re-treatment by most experts (Supplementary Figure 11).
In terms of aneurysm morphology, “new saccular portion/daughter sac” (18/24, 75%) and “change to Raymond-Roy III grade” (16/24, 67%) were considered the most important indications for re-treatment (Supplementary Figure 12). For patient-related factors in terms of retreatment indications, family history of SAH (18/24, 75%) and polycystic kidney disease (17/24, 71%) were considered most critical (see also Supplementary Figure 13).
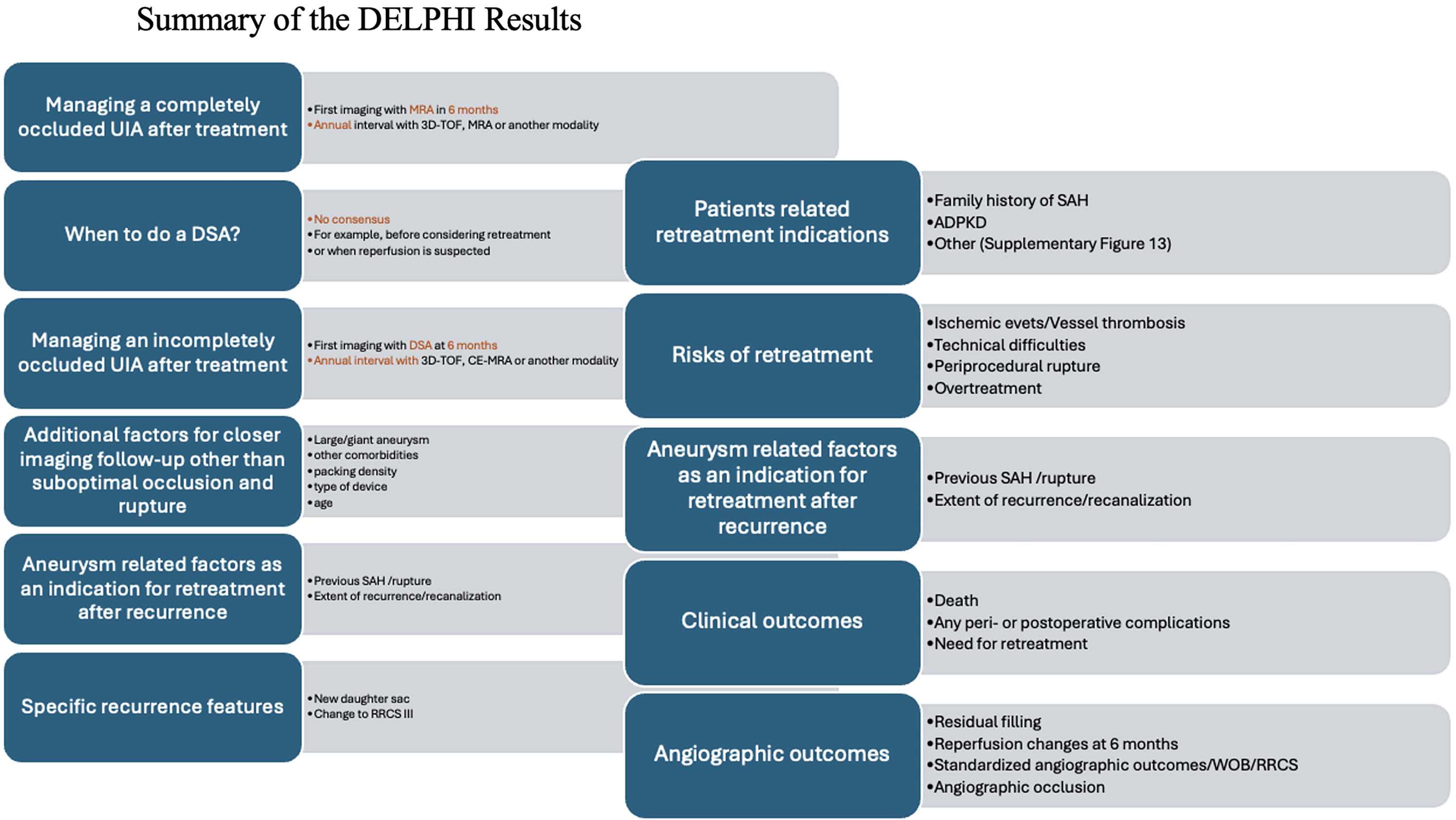
Summary of the DELPHI results. This figure summarizes answers and statements for various questions that were attempted to answer during the DELPHI discussion.
Priorities and outcome measures for re-treatment
All participants agreed that safety and feasibility should be of the highest priority for retreatment (Supplementary Figure 14). Risks to be taken in the account when considering retreatment were ischemic events (24/24, 100%) and parent vessel thrombosis (23/24, 96%), platelet aggregation (22/24. 92%) and technical difficulties (22/24, 92%) periprocedural rupture (21/24, 88%), as well as risk of overtreatment (21/24, 88%) (Supplementary Figure 15).
Most experts thought that the risk of re-treatment differs from the risk of the first treatment (Supplementary Figures 16 and 17). Potential benefits for endovascular retreatment were re-rupture prevention (24/24, 100%), stopping further growth (23/24, 96%), and avoiding craniotomy (18/24, 75%) (Supplementary Figure 18). All participants agreed that endovascular re-treatment is superior to open surgery (24/24, 100%) (Supplementary Figure 19).
All participants agreed on the importance of clinical outcomes to measure re-treatment success, specifically death (24/24, 100%), mRS (19/24, 79%), and patient-reported outcome measures (PROMs) (18/24, 75%) (Supplementary Figure 20). Angiographic outcome measures such as residual filling of the aneurysm or aneurysm neck at the end of the procedure (23/24, 96%) and at 6 months (23/24, 96%) were also deemed important.
The WEB occlusion scale (WOS) as an angiographic outcome measure after WEB treatment was supported by 22/24 participants (92%), and the modified Raymond-Ray classification scale (RRCS) for coiled aneurysms was agreed upon by 20/24 participants (84%) (Supplementary Figure 21).
Discussion
Key take-home messages from this DELPHI consensus on managing patients after treatment of intracranial aneurysm with intrasaccular devices are as follows:
For completely occluded aneurysms, the first follow-up imaging was considered at 6 months using MRA, with the following at 1 year, though the method for later imaging achieved no consensus. For incompletely occluded aneurysms, DSA is recommended at 6 months, followed by annual reimaging. Retreatment decisions focused on factors like aneurysm size, recurrence features, and patient comorbidities, with agreement on retreatment risks of ischemic events. Important clinical and angiographical outcomes included: death, any peri- or postprocedural complications, assessing residual filling and aneurysm occlusion at specific time points.
The recommendations for follow-up imaging generally reflect what is discussed in the literature, with emphasis on early imaging at 3–6 months. 17 Several studies have emphasized the importance of early imaging to detect complications or incomplete occlusions. 18
The lack of consensus in the panel on long-term follow-up modalities underscores the highly nuanced decision-making based on patient and physician preferences and center-specific protocols. MRA is a non-invasive and reliable option for follow-up in many cases, but DSA is generally still considered the gold standard for detecting recurrence or complications.19,20
The panelists’ opinions with regard to re-treatment decisions also align well with findings from previous studies, which have demonstrated that larger aneurysms, wider necks, and higher Raymond-Roy Occlusion Classification (RROC) scores are significant predictors of recurrence.10,21,22 Their preference for endovascular retreatment over surgical approaches reflects current trends in neurovascular treatment practices, supported by data showing lower complication rates and shorter recovery times with endovascular treatment.23,24 That being said, re-treatment rates after surgical clipping as a first-line treatment are lower than those for endovascular therapy. 25
The strong focus on angiographic outcomes in many studies is another point of controversy. While assessing angiographic occlusion rates and residual filling provides valuable insights into treatment success, there is growing recognition of the need to integrate long-term clinical outcomes and patient reported quality of life. This was also reflected in the DELPHI panel, where experts deemed long-term clinical outcomes and patient-reported outcome measures more important than angiographic outcome scales. 26
Limitations
This study has several limitations: (a) The conference addressed multiple topics over three days, and there may have been some fatigue from long and intense discussions. (b) The questions for round 2 were developed by the 5T organization committee based on round 1 responses, and this required narrowing down a broad range of topics to fewer closed-ended questions. As such, some interesting aspects that were mentioned only by a few attendees in round 1 may have been omitted from subsequent rounds.
Conclusion
The findings of the DELPHI consensus emphasize the complexity and multifaceted nature of real-life decision-making in managing intracranial aneurysms that were previously treated with intrasaccular devices. While consensus was reached on key aspects of follow-up timing and key decision drivers for retreatment, the panel also highlighted the wide variability in clinical scenarios that render standardized approaches challenging or perhaps even impossible.
Footnotes
Abbreviations
Acknowledgments
None.
ORCID iDs
Author contributions
Alexander Stebner: received a stipend for his Research Fellowship in Calgary from the Swiss Society of Radiology. M. Moreu: Regarding this paper: None, Consultant: Stryker, Medtronic, Balt, Inspire, iVascular, Accandis, Investigation: Anaconda, Cerenovus, iVascular, Stryker, Stocks: Basecamp. A. Paul: Consultant for Microvention and Medtronic. S. Yoshimura: received speakers’ bureau/honoraria from Daiichi Sankyo, Bristol-Meyers Squibb, Stryker, Medtronic, Kaneka Medics, Terumo, Boehringer-Ingelheim, Bayer, Johnson & Johnson, Nxera, and Eisa. Johanna M Ospel: is a consultant for Nicolab.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The 5T Think Tank Conference was financially supported equally by Medtronic, Stryker, Terumo, Cerenovus, and Penumbra, covering expenses for the venue, accommodation, and meals.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.