
Abstract
Background and objectives
Fetal posterior cerebral artery (fPCA) is a common anatomical variant where the P1 segment is hypoplastic or absent, and the posterior communicating artery supplies the posterior cerebral artery (PCA) territory. Aneurysms in this setting often form at the internal carotid artery (ICA)–posterior communicating artery junction and are poorly defined. This study introduces a novel classification to address the fPCA variant, treatment challenges, and outcomes.
Methods
This registry-based study included fPCA aneurysms treated endovascularly at the Medical University of South Carolina (2013–2024). Aneurysms are classified into type-1 (shared neck with ICA and fPCA), type-2 (neck arises from ICA, and fPCA originates from the aneurysm), and type-3 (neck originates entirely from fPCA). Aneurysm type, treatment strategy, and outcomes were compared.
Results
Forty fPCAs, consisting of 20 type-1, 15 type-2, and five type-3 aneurysms, were analyzed. For type-1 aneurysms, recurrence on admission was higher (40%, p = 0.03, V = 0.34 [95% CI: 0.22–0.56]). In addition, maximum diameter (p = 0.02, η2 = 0.17) and neck size (p = 0.001, η2 = 0.32) were larger in type-2 aneurysms. Treatment modalities included coiling alone (55%), stent-assisted coiling (17.5%), and flow diversion (FD) (27.5%). All coil-alone treatments were performed in newly presented ruptured aneurysm cases (p < 0.01, V = 0.57). FD was mainly used in aneurysm recurrence (54.5%), with adequate occlusion in all patients at one-year follow-up. The lowest occlusion rate was seen in type-2 (86.7% vs. 96%, p = 0.54, RR = 0.3 [95% CI: 0.03–3.03]) in one-year follow-up.
Conclusion
A personalized approach is needed to improve outcomes, particularly in wide-neck bifurcation fPCA aneurysms. Endovascular treatment should be individually adapted to each type to achieve optimal outcomes.
This is a visual representation of the abstract.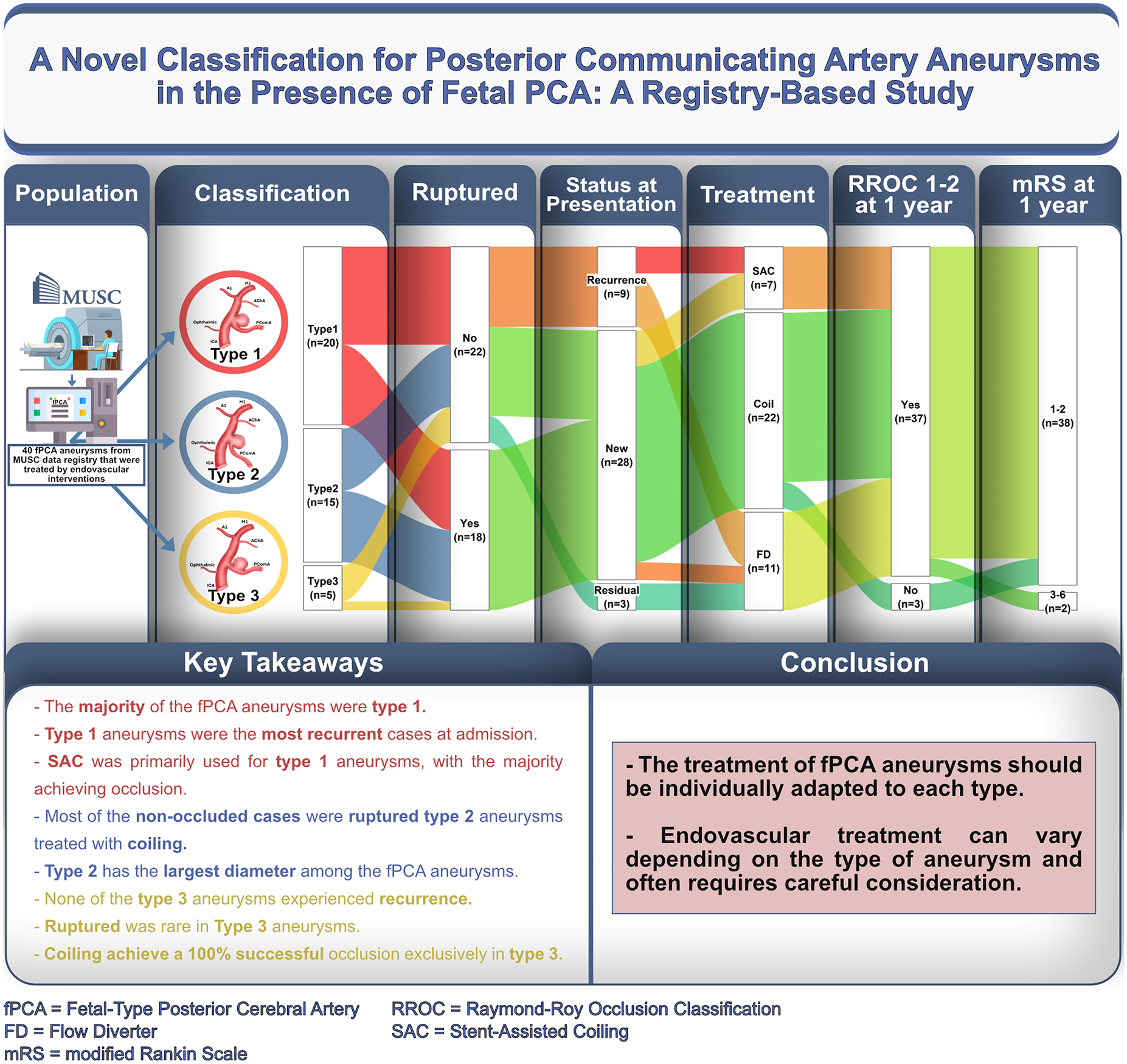
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.