
Abstract
Background
Intracranial high-flow vascular malformations greatly alter neonatal cerebral hemodynamics and can cause significant morbidity and mortality. X-ray digital subtraction angiography (DSA) is the standard of care to assess angioarchitecture and plan for intervention, but exposes patients to radiation and procedural risks, and only allows for subjective interpretation. Objective noninvasive assessment of hemodynamics could improve prognostication. Data on normal or abnormal cerebral hemodynamics in neonates is limited due to the lack of readily available and validated methods. 4D flow MRI may offer noninvasive quantitative assessment of hemodynamic metrics to gain a better understanding of pathophysiology and may one day help to guide endovascular intervention. Here, we explore the feasibility of 4D flow MRI for the assessment of high-flow vascular malformations and present our initial experience.
Methods
Retrospective analysis of 4D flow MRI studies was performed for five children with high-flow vascular malformations before and/or after embolization of their lesions. Two raters independently performed the 4D flow measurements: flow rate and peak speed. We compared quantitative measurements with qualitative angiographic findings.
Results
Interrater reliability of flow measurements was high (intraclass correlation coefficient 0.959). Quantitative changes in arterial and venous 4D flow measurements after embolization corresponded with qualitative changes on DSA.
Conclusions
4D flow MRI is a feasible and precise tool for studying high-flow intracranial vascular malformations in children with safety advantages over DSA. Standardized acquisition protocols and postprocessing methods could facilitate adoption across multiple centers.
Introduction
High-flow intracranial vascular malformations—including arteriovenous malformations (AVM), dural arteriovenous fistulas (DAVF), vein of Galen malformations (VoGM), and nongalenic pial arteriovenous fistulas (NGPAVF)—are associated with significant morbidity and mortality when presenting in the first months of life. 1 These shunting lesions provide a low-resistance pathway for arterial blood to enter the venous system, driving an increase in cardiac output and an associated higher proportion of total cardiac output directed to the brain and also contributing to venous hypertension.
In a healthy neonate, approximately 17% of total cardiac output is directed to the brain and this number increases steadily into adulthood where it reaches approximately 25% of total blood flow despite representing only 2% of total body mass. 2 Additionally, in early life, intracranial circulation changes rapidly. Within the first five days of life, cerebral blood flow velocity was noted to increase by approximately 35% in a cohort of full-term neonates. 3 Further sonographic studies have demonstrated a continued increase over the first three years of life. 4 With high-flow shunting lesions, a higher total amount and proportion of overall cardiac output are directed through the brain, which can be especially problematic in the pediatric setting given that neonatal cerebrovascular autoregulation is limited. 2
Hemodynamic parameters may hold significant insight into this disease process and others. However, historical data were generally derived using either invasive physiologic testing in animal models and extrapolating to humans or with limited ultrasonographic methods combining Doppler velocity measurements in relevant vessels with approximations of cross-sectional area calculated based on the observed radius of the vessel on imaging.2,3,5 While these methods provide a helpful foundation for our understanding of the basic physiology, they rely on assumptions that may not be accurate. More recently, more advanced ultrasound imaging methods are being explored, but can only provide estimates of flow velocities and lack other hemodynamic parameters. 6
Clinically, digital subtraction x-ray angiography (DSA) is the current gold standard for imaging of these lesions and serial imaging is typically used in the context of surveillance, treatment planning, and endovascular intervention. 7 While DSA provides important structural information relevant for diagnosis and treatment, the method is limited by lack of quantitative hemodynamic parameters and introduces procedural risks including exposure to ionizing radiation, intraarterial administration of iodinated contrast material, and need for arterial access. Conversely, MRI is noninvasive and does not expose the patient to ionizing radiation. In addition, phase-contrast magnetic resonance angiography, such as “4D flow” sequences, may provide a method to noninvasively and quantitatively extract hemodynamic parameters to better characterize these high-flow AVFs or other vascular lesions. 8
Herein, we seek to evaluate the feasibility and reproducibility of 4D flow MRI for quantitative assessment of hemodynamics in fives neonates/infants with high-flow intracranial vascular malformations.
Methods
Participants
Patients with 4D flow MRI before and/or after embolization were selected retrospectively from our institution's database of pediatric patients with high-flow intracranial vascular malformations for further analysis in accordance with institutional review board exempt status. This study focused on pediatric patients and extracted imaging studies and reports of patients with DAVF, VoGM, and NGPAVF who had undergone endovascular intervention.
Patients with high flow vascular malformations who underwent endovascular treatment with preoperative and/or postoperative 4D flow MR imaging between January 2021 and January 2022 were included within the study. Five patients met criteria, two with both pre- and postembolization data and three in whom a preembolization scan could not be completed due to hemodynamic instability. Scans for patients with only one available imaging timepoint were assessed for reproducibility of 4D flow data processing whereas scans for patients with both pre- and postembolization imaging were assessed for agreement with qualitative interpretation of DSA before and after intervention. In this study, one patient with DAVF, two patients with a VoGM, and two patients with a NGPAVF were evaluated. In total, seven imaging series were assessed for these five patients.
Imaging and intervention
4D flow MRI was acquired on a GE SIGNA architect, GE Discovery MR750, or Phillips Ingenia MRI scanner at 3 Tesla before or after embolization of the high-flow fistula. 4D flow MRI was acquired at a matrix size of 180 × 180 × 52, flip angle of 15°, repetition time of 5 ms, echo time of 2.78 ms, velocity encoding gradient of 60 cm/s, with 20 cardiac frames. Following MRI studies, DSA imaging and embolization under fluoroscopic guidance for Patients 1 and 2 were performed on a Siemens Axiom-Artis Q biplane angiography system optimized for pediatric neuroangiography. Embolization was performed with standard endovascular surgical techniques employing a combination of detachable platinum embolic coils (Balt Optimax, Stryker Target) and n-butyl cyanoacrylate (n-BCA) liquid adhesive (Cerenovus Trufill). In Patients 3, 4, and 5, embolization prior to imaging was achieved with a combination of the above coils and adhesives and liquid embolic agents (Medtronic Onyx).
Image processing
4D flow images were imported into Arterys software v27.9 (Arterys, Inc.) for postprocessing. Two independent raters, trained in the use of the software, measured the flow through designated vessels using a standardized method by defining the boundaries of the lumen of the vessel of interest in a plane orthogonal to the direction of flow through the vessel. Vessels examined include the straight sinus and the bilateral internal carotid arteries, vertebral arteries, and sigmoid sinuses as well as several vessels specific to each intervention.
For each vessel of interest, net flow (L/min) and peak speed (cm/s) were recorded. For each of these quantities, the mean and standard deviation between both raters were calculated and reported in Tables 1 and 2.
Patient 1 underwent embolization of a vein of Galen malformation on day 152 of life. Average 4D flow MRI measurements were acquired both pre- (Day of life 152) and post- (Day of life 153) embolization.
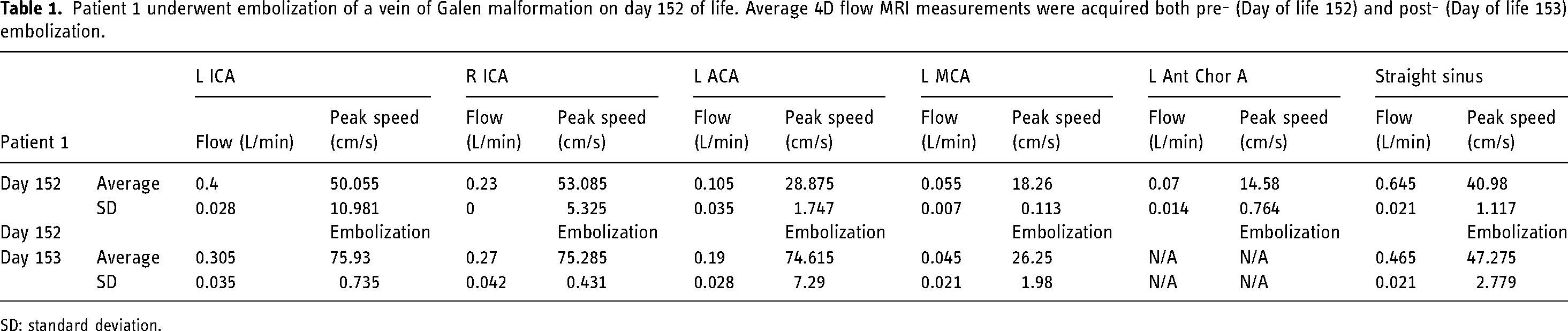
SD: standard deviation.
Patient 2 underwent embolization of a nongalenic pial arteriovenous malformation on day 1 of life. Average 4D flow measurements were acquired pre- (Day of birth = Day 0) and post- (Day of life 141) embolization.

SD = standard deviation.
Placement of regions of interest was confirmed by experienced interventional neuroradiologists. The measured flow in the bilateral sigmoid sinuses was summed to estimate total intracranial venous drainage (excluding collateral circulation) as a surrogate measure for total flow. Raters were blinded to the interventions and chronological order of imaging studies when taking measurements.
Statistical analysis
Comparison of interrater reliability for 4D flow data processing was assessed with the intraclass correlation coefficient (ICC). Flow and peak speed values are reported as the mean value and standard deviation between the two independent raters. Differences between pre- and postembolization flow measurements are reported as absolute and percent changes. Graphs for the figures were made in Tableau Desktop software v2021.4 (Salesforce, Inc.) and figures were designed in Microsoft Powerpoint (Microsoft, Inc.).
Results
Background on patient population
The five patients were studied between July 2020 and June 2022. Patient 1 was 152 days old at the time of the VoGM embolization event examined. 4D flow MR images were captured on days 152 and 153 of life. This was the third embolization treatment for this patient. For Patient 1, embolization was performed under fluoroscopic guidance using a combination of detachable coils and n-BCA in the left anterior choroidal artery and a left middle cerebral artery cortical branch supplying the fistula.
Patient 2 was one day old at the time of the NGPAVF embolization event examined. 4D flow MR images were captured on days 0 and 141 of life. For Patient 2, embolization was performed under fluoroscopic guidance using n-BCA adhesive in the left posterior inferior cerebellar artery and bilateral superior cerebellar arteries.
Patients 3, 4, and 5 were 13 years, 25 months, and 13 months old, respectively at the time of MRI. Each of these patients had at least one embolization prior to 4D flow scan.
Quantitative analysis of derived flow measurements
Measured hemodynamic parameters, including flow rate and peak speed, for Patients 1 and 2 both pre- and postembolization can be found in Tables 1 and 2, respectively. Representative images of DSA and 4D flow MRI before and after embolization for Patient 1 are included in Figure 1. Figure 2 demonstrates changes in flow rate measurements in relevant arteries and veins following embolization for Patient 1. Representative images of DSA and 4D flow MRI before and after embolization for Patient 2 are shown in Figure 3. Figure 4 demonstrates changes in net flow measurements in relevant arteries and veins following embolization for Patient 2.
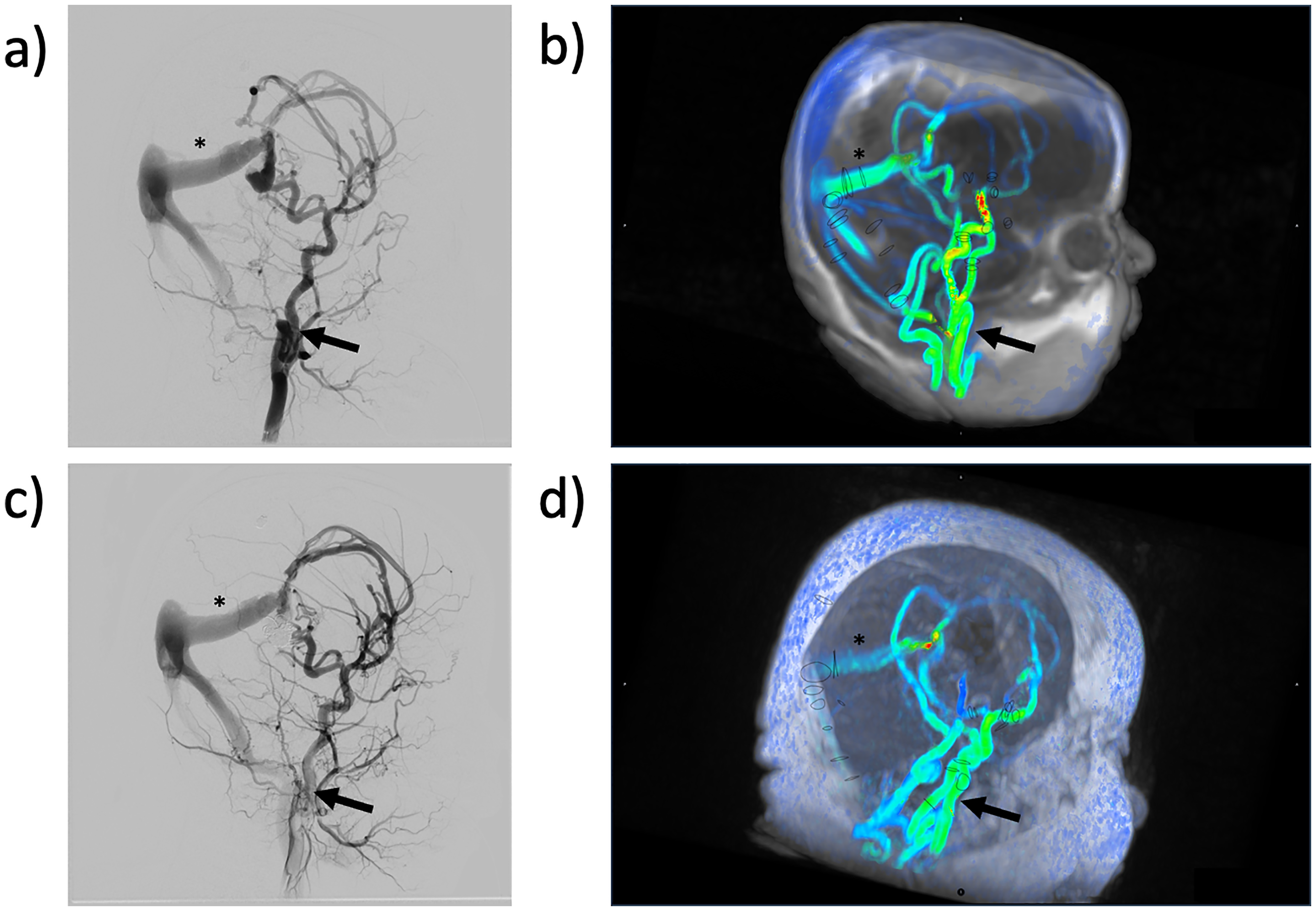
(a) Representative angiography image demonstrating the presence of vascular malformation prior to intervention for Patient 1. (b) 4D flow MRI demonstrating vascular malformation for Patient 1 prior to intervention, discs represent vessel contours drawn by readers for flow calculations. (c) Representative angiography image demonstrating the presence of vascular malformation after intervention for Patient 1. (d) 4D flow MRI demonstrating vascular malformation for Patient 1 after intervention, discs represent vessel contours drawn by readers for flow calculations.
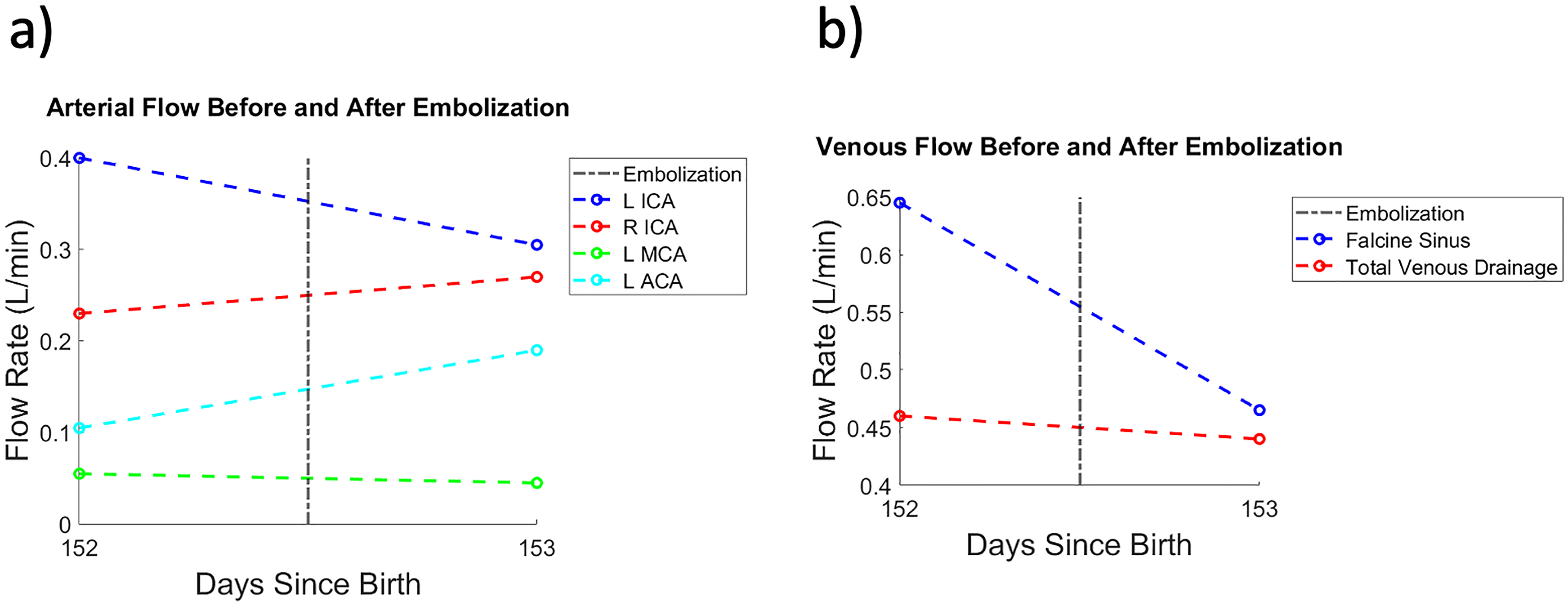
(a) Graph demonstrating calculated flow in several arteries before and after intervention with embolization for Patient 1. (b) Graph demonstrating calculated flow in several veins before and after intervention with embolization for Patient 1.
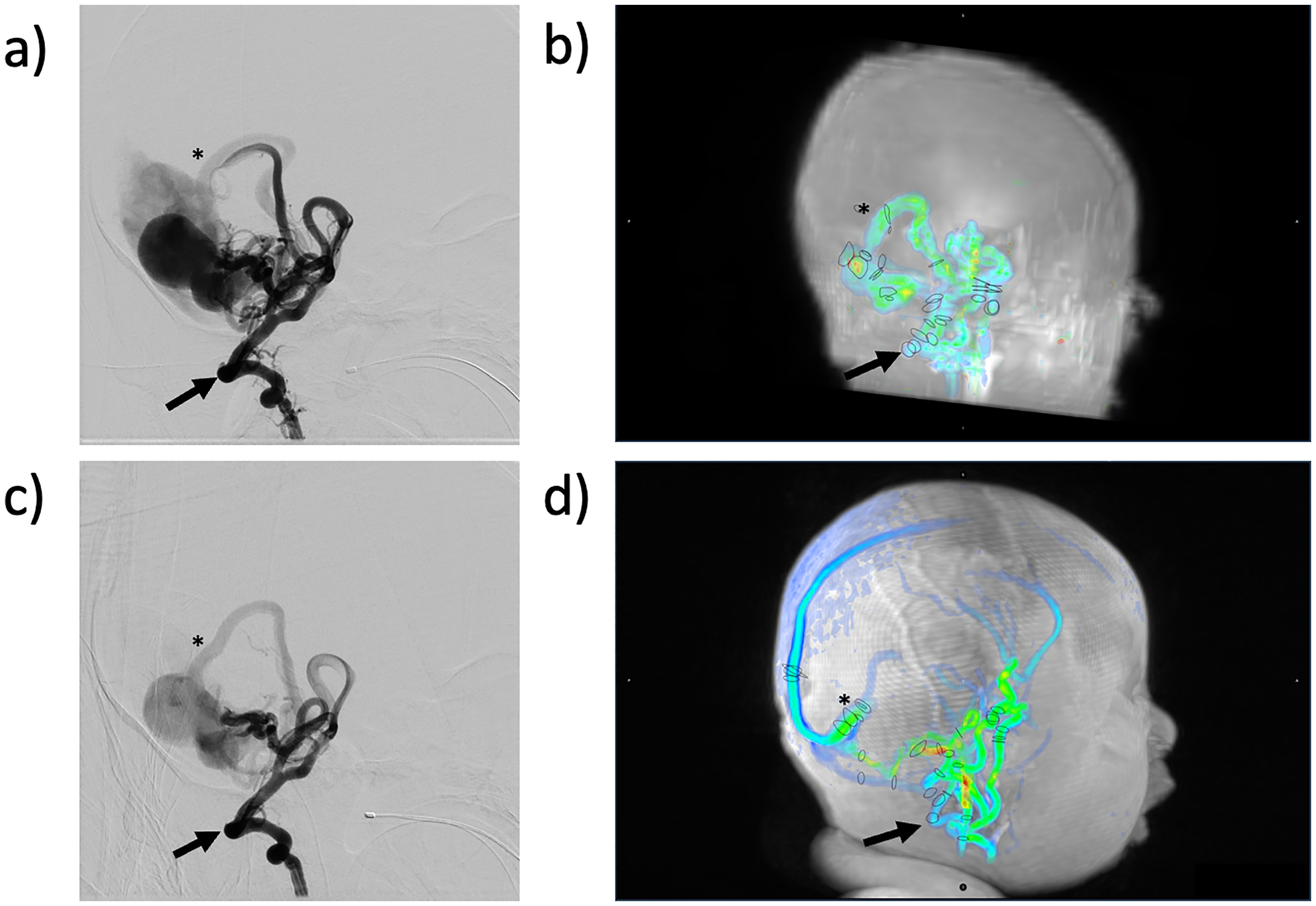
(a) Representative angiography image demonstrating the presence of vascular malformation prior to intervention for Patient 2. (b) 4D flow MRI demonstrating vascular malformation for Patient 2 prior to intervention, discs represent vessel contours drawn by readers for flow calculations. (c) Representative angiography image demonstrating the presence of vascular malformation after intervention for Patient 2. (d) 4D flow MRI demonstrating vascular malformation for Patient 2 after intervention, discs represent vessel contours drawn by readers for flow calculations.
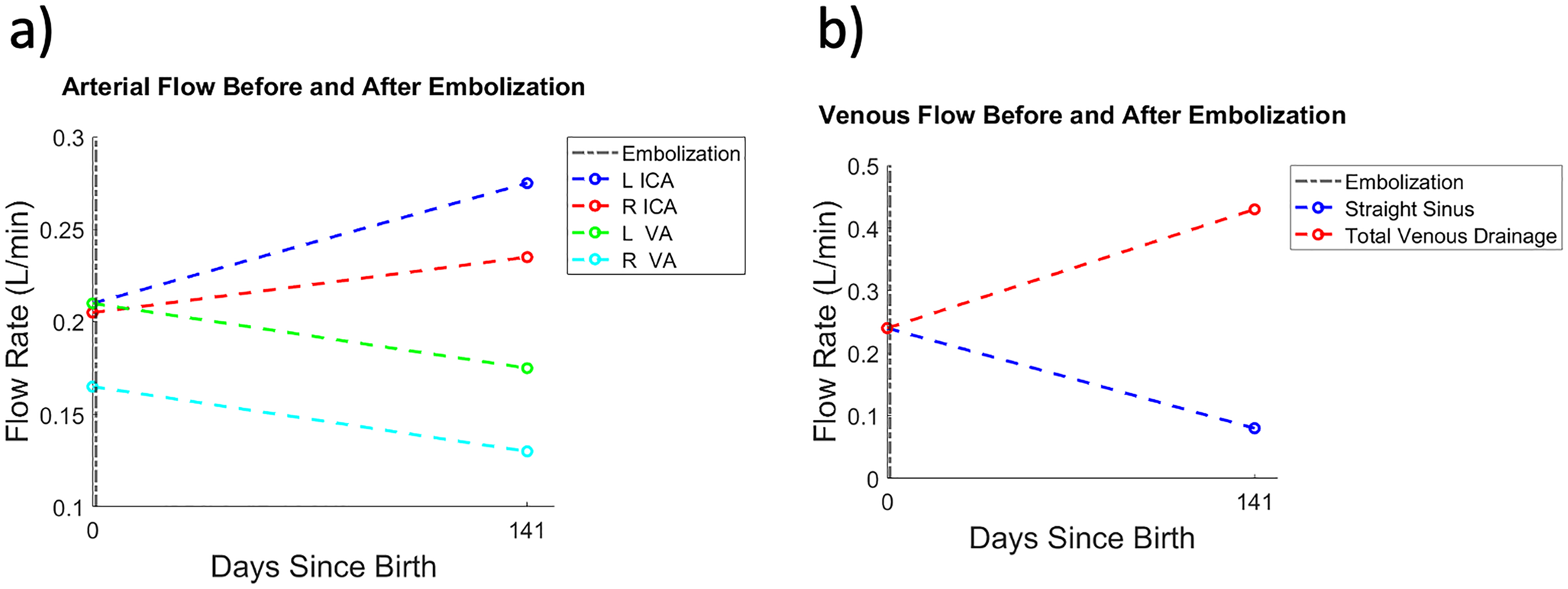
(a) Graph demonstrating calculated flow in several arteries before and after intervention with embolization for Patient 2. (b) Graph demonstrating calculated flow in several veins before and after intervention with embolization for Patient 2.
Flow rates
After embolization of multiple left anterior circulation arterial pedicles (arising from the left middle cerebral and left anterior cerebral arteries) in Patient 1, the flow rate in the left internal carotid artery and falcine sinus decreased (Figure 2). After embolization of multiple posterior intracranial circulation arterial pedicles (arising from both superior cerebellar arteries and the left posterior inferior cerebellar artery) in Patient 2, the flow rate in the right vertebral artery, the left vertebral artery, and the straight sinus decreased (Figure 4).
Superimposed physiologic changes in hemodynamics associated with normal growth of children
For Patient 1, given the short time between imaging studies, no physiologic changes are anticipated to play a role in hemodynamic properties. However, for Patient 2 given the separation between the first and second MRI studies, some physiologic change in flow is anticipated separately from the contribution of the embolization. Studies of intracranial blood flow in neonates and infants shows that the most rapid increase in blood flow occurs during the first six months of life, concurrent with the time period between these two studies (140 days). 4 Although an earlier study was performed on day 14 of life (13 days after the embolization event), interpretation was limited by imaging technique as optimal parameters for this sequence had not yet been identified.
As a result of this separation between imaging sessions in our study, the measured flow in all of the intracranial arteries and veins would be anticipated to increase between these two time points. Given that the flow in the straight sinus declined so appreciably, this decrease in flow is likely attributable to the impact of the embolization. Similarly, observed decreases in flow in the left and right vertebral arteries are likely attributable to embolization in the posterior circulation. The observed increases in total venous drainage and flow in the bilateral internal carotid arteries are likely physiologic and represent the increased demand for oxygen of the developing brain.
Reproducibility of flow data processing
Interrater reproducibility of 4D flow measurements was evaluated with ICC, a descriptive statistic utilized to assess conformity of quantitative measurements, specifically data clusters, made by multiple observers. Notably, ICC is a measure of agreement or reproducibility, which is related to correlation, however, demonstrates key differences. While correlation can assess the relationship between variables of interest, agreement also evaluates the degree of concordance between two or more assessments of the variable of interest. ICC is superior to alterative measures of correlation, such as the Pearson correlation, given the additional ability to account for differences in means of the measurements being considered.
Flow measurements, obtained from the Arterys software, were analyzed utilizing ANOVA two factor tests without replication, ICC measurements were calculated both in aggregate as well as grouped by patient (Figure 5). Flow measurements were found to be reproducible between independent raters. Interrater reliability of 82 flow measurements across all five patients demonstrated a high degree of agreement with ICC = 0.959.
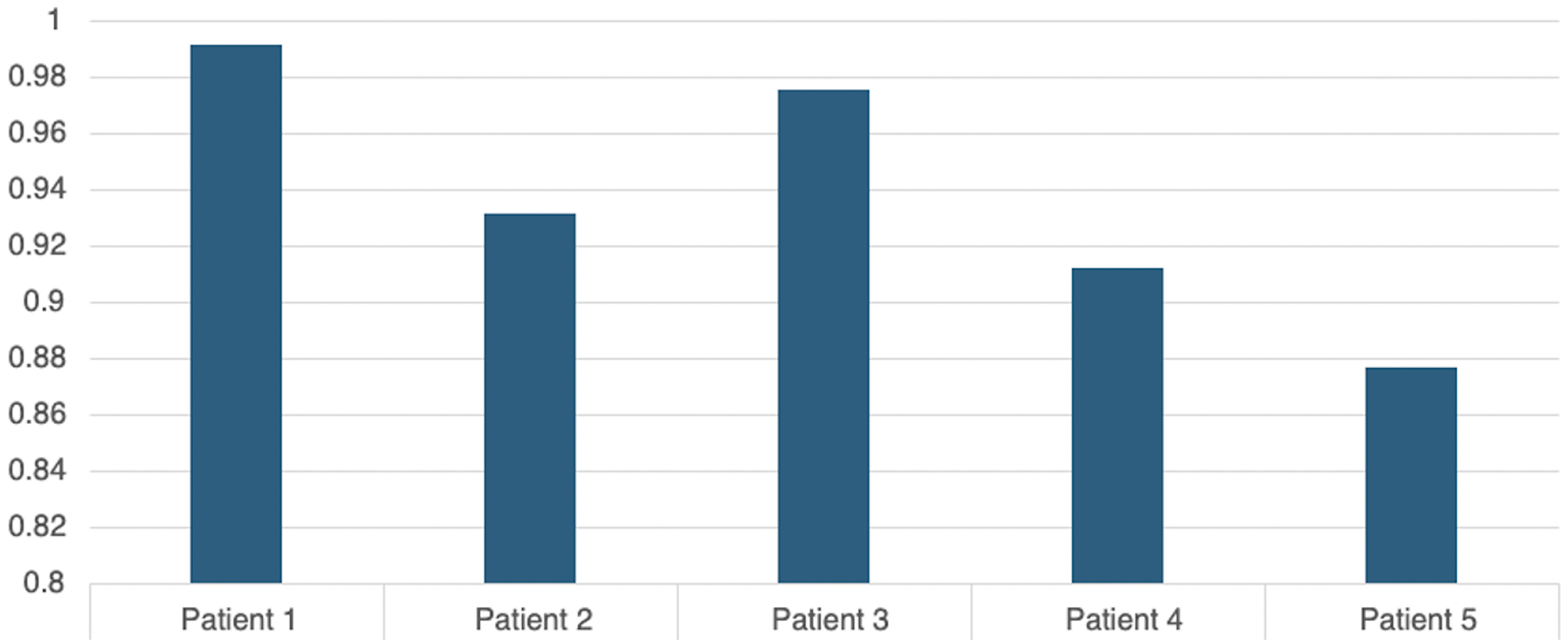
Graph demonstrating the intraclass correlation coefficient for flow measurements per patient denoting excellent agreement between the two raters.
Discussion
4D flow MRI is a powerful modality for quantification of vascular flow in the brain. Neonates and infants are particularly sensitive to the effects of ionizing radiation due to their age and are prone to arterial injury due to small arterial size. Therefore, neonates and infants with high-flow intracranial vascular malformations such as VoGM and NGPAVF could benefit from noninvasive hemodynamic assessment and avoidance of DSA. Another potential advantage of 4D flow MRI over DSA is that by providing additional quantitative hemodynamic parameters, such as wall shear stress, better characterization of these lesions may improve long-term management strategies. Recently, 4D flow has been used to demonstrate a significant difference in hemodynamic properties between nidal and extranidal circulation in AVMs 9 or treatment effects of stereotactic radiosurgery prior to the development of angioarchitectural changes on structural imaging. 10
One of the main practical challenges of 4D flow MRI in the clinical setting is the need for postprocessing to obtain hemodynamic parameters, involving software with user-dependence. We sought to assess the reproducibility of 4D flow MRI measurements given these practical constraints, and found a strong degree of interrater reliability across the 82 measurements collected by each rater; therefore we feel that the estimates of blood flow generated by this method have acceptable precision for clinical use. The accuracy of these measurements remains unknown, as quantification of intracranial flow in neonate is not part of routine clinical practice. However, these findings do correspond with qualitative interpretation of angiographic imaging.
4D flow MRI could potentially be used as an imaging biomarker of endovascular treatment success. For example, one patient (Figure 2) had decreased flow through the straight sinus following embolization, suggesting reduced pressure in the deep venous system. Additional flow measurements indicate a decrease in flow in the left internal carotid artery with relatively preserved flow through the left middle cerebral artery and left anterior choroidal artery and increased flow in the left anterior cerebral artery, suggestive of occlusion of arteries feeding the vascular malformation while still maintaining adequate perfusion to the surrounding vascular territories. The increase in flow observed in the right internal carotid artery and left anterior cerebral arteries may indicate the involvement of collateral circuits and the circle of Willis in maintaining perfusion of the brain following embolization.
Limitations of the study include a small sample size, a retrospective study design and single institution data collection. Our sample size of five patients further is limited by unavailable preembolization imaging in three patients, this limitation must be interpreted in the context of investigated a rare vascular condition. Additional technical imaging-related limitations encountered in the process of performing this investigation were primarily related to specifying imaging parameters such as velocity encoding (Venc). This parameter must be selected carefully to prevent aliasing of flow that exceeds this threshold. From our experience, and as seen in other studies, Venc is optimally selected to be of the order of 20% greater than the maximum flow velocity to be measured. In the case of our studies, we initially explored a Venc of 60 cm/s but found that in our patients there were several flow velocities measuring greater than this Venc, resulting in aliasing. Given this initial finding, the Venc was raised to 100 cm/s to appropriately capture higher velocities. An excessively high Venc is undesirable as it reduces the sensitivity to the full range of presenting velocities.
4D flow MRI can provide a noninvasive method of quantitatively assessing hemodynamic parameters with high interrater reliability in the setting of high-flow intracranial vascular malformations in neonates and infants. The observed changes in flow through vessels also appear to correspond with subjective angiographic findings. Future work with larger sample sizes, as well as standardized acquisition and postprocessing protocols, may help to guide future work and could help establish which hemodynamic parameters are the most predictive of clinical outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.