
Abstract
Introduction
Extracranial internal carotid stenosis (EICS) is a well-established cause of stroke. Carotid near-occlusion (CNO), either distally collapsed or not, is a rare sub-type of EICS with conflicting data regarding the necessity for treatment. The aim of this study is to evaluate the results of carotid artery stenting (CAS) for patients with symptomatic CNOs.
Material and methods
Institutional review board (I06-420-23) approval was obtained for this retrospective study. Consecutive data from January 2019 to January 2023 was obtained. Sixty-five patients underwent 66 procedures for symptomatic CNOs. Diagnosis of CNOs were made with DSA images. Treatment decisions were made by a multidisciplinary team. Patient data including age, gender, clinical presentation, affected side, complications (initial/ follow-up), and pre and post mRS scores were recorded and analyzed.
Results
There were 22 female and 43 male patients with symptomatic CNOs (mean age: 71.52 ± 9.32 years). The mean time from symptom-to-treatment was 3.91 weeks ± 3.74 weeks (ranging from 0 to 20 weeks). There were eight events recorded in the 30 days period after CAS; five (7.7%) were cerebral hyperperfusion syndrome (one causing haemorrhage) and three (4.5%) ischemic complications. Permanent neurologic deficit rate was 6% and 61 patients (94%) mRS scores were unchanged during last follow-up. Mean follow-up period was 22.94 ± 16.67 months (ranging from 0.5 to 60 months).
Conclusion
Our study demonstrated that in the complex population of patients with symptomatic CNOs, CAS is a feasible option with acceptable rate of permanent neurologic deficits. Further studies are needed to assess its safety and long-term efficacy.
Keywords
Introduction
Extracranial atherosclerotic carotid stenosis (EICS) is responsible for 8–20% of ischemic strokes.1–3 Carotid near-occlusion (CNO) is a rare sub-type of EICS defined by severe internal carotid artery stenosis with significant reduction of its distal lumen. Although carotid ultrasound (CUS) is a valuable tool for the imaging of carotid disease, it may be inconclusive in CNO cases. 4 On the other hand, CT angiography has a higher sensitivity and specificity, compared to the CUS imaging and DSA is the gold standard.3–5
The prevalence of significant carotid stenosis is approximately 3% for women and 5% for men with a risk of stroke of 18–29% in this population. 6 CNOs account for approximately 10% of patients with significant carotid stenosis. 7 The optimal management of CNOs is still a matter of debate since no definitive evidence is available for guidance. Besides, these patients are usually excluded from larger trials. 8 Despite conflicting data in the literature regarding the treatment of this entity, a recent meta-analysis demonstrated better results for carotid endarterectomy (CEA) and/or carotid artery stenting (CAS) in contrast to the best medical treatment. 9 Furthermore, CEA and CAS have reached similar results in respect to the 30-day stroke risks and restenosis rates in the long-term follow-up.8,9
The aim of this retrospective study is to evaluate the feasibility, safety and outcomes of CAS in the treatment of symptomatic CNO patients.
Materials and methods
Our institutional database was retrospectively reviewed. Sixty-five consecutive patients (22 women, 43 men) with symptomatic CNOs were treated with CAS between January 2019 and January 2023. All patients were older than 18 years of age (18–91 years) and informed consents were obtained. Institutional review board approval was granted for this study (I06-420-23) and patients’ data were anonymized.
The diagnosis of CNO was suggested using CUS, CTA or MRA; DSA imaging was obtained for definitive diagnosis before any treatment was performed.
The diagnosis of CNO was made according to the criteria described in detail previously in the literature 10 (Figure 1). Patients with CNO-like appearance related to carotid dissections or post-radiation changes with no signs of atherosclerotic disease were not included in this study.
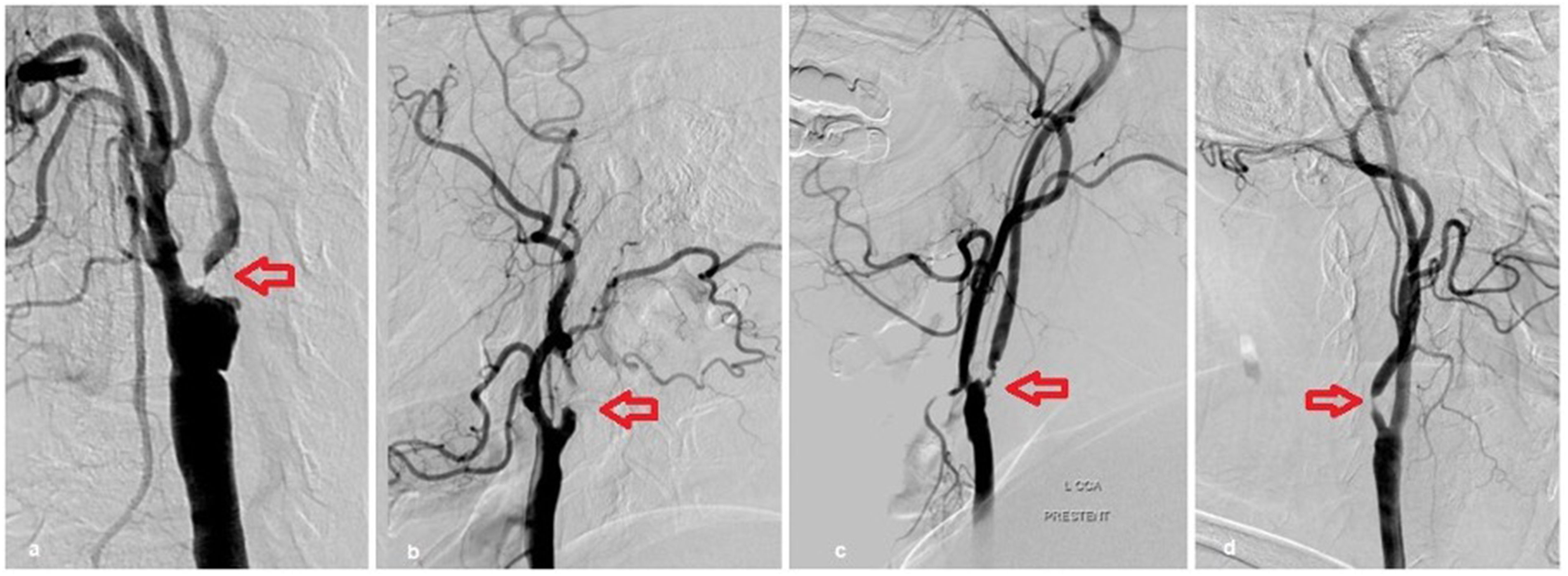
Images of carotid near-occlusions. (a, b) Left-sided carotid near-occlusions with full collapse in two different patients. (c, d) Left- and right-sided carotid near-occlusion in two different patients without full collapse.
The decision to proceed with CAS for the treatment of patients with CNOs was made by our institutional multidisciplinary team consisting of neurologists, neurosurgeons, vascular surgeons and interventional radiologists. Patients’ data including age, gender, clinical presentation, affected side, access, number of stents used, balloon sizes used during pre and post dilatations, protection device usage, neurologic status of the patients (initial/ follow-up), time passed from the symptom onset to CAS, antiplatelet regimens, re-stenosis/occlusion rates during the follow-up, and complications (initial/ follow-up) were recorded and analyzed. Technical complications were recorded. All neurological events from the time of the procedure to 30 days post procedure (30-day period) were considered complications. All patients treated by CAS were discharged from the hospital 4–6 h after the endovascular procedures unless neurological or access complications were noted as per our protocol. Patients were advised to present to our Institution's emergency department (ED) in case neurological deterioration or arterial access issues after their discharge from the hospital. Patients that needed longer period of hospitalization or returned to the ED after their initial discharge were also recorded. Patients were scheduled for a CUS at 3–6 months and 12 months. Afterwards they were controlled annually and if there was concern of stenosis/occlusion during CUS follow-up, a DSA was performed.
CAS technique
Arterial accesses were performed via femoral or brachial artery using local anaesthesia. Arterial punctures were made with either manual palpation or under ultrasound guidance according to the operators’ preferences with an 18 G needle. Patients were started on aspirin 100 mg and clopidogrel 75 mg at least 5 days before and continued dual antiplatelet regimen for six months after the endovascular procedures followed by a single antiplatelet therapy indefinitely unless indicated otherwise. For the patients with history of valve replacement requiring oral anticoagulants, a single antiplatelet (clopidogrel 75 mg) was used along with the oral anticoagulant.
Different embolic protection devices (EPD) (FilterWire, Boston Scientific, USA, SpiderFX, Medtronic, USA, Emboshield, Abbot Vascular, USA) were used for distal protection during the treatments and all patients were treated with closed cell stents (WALLSTENT, Boston scientific, USA). Pre-dilatation was performed using 3–5 mm balloons (Sterling, Boston Scientific, USA) when there was difficulty in advancing the EPD or the stent system. Post-dilatation after stent deployment was performed if there was a residual stenosis of >30% using a 5 or 6 mm balloon (Sterling, Boston Scientific, USA).
All patients in this study were monitored by the anaesthesia team using a two channel near infrared spectroscopy (NIRS) device (Medtronic, USA) to better understand and monitor the cranial flow changes after stent implantations.
Statistical analysis
IBM-SPSS 20.0 was used to perform statistical analysis. Descriptive data for age are presented as average standard deviation (±), whereas categorical data representing the number of participants (angiographies) are indicated as percentage (%). Student's t test was used in this study to compare ages in different gender groups. For the descriptive statistics average, standard deviation (±), median, minimum and maximum values were used while numbers and percentages were used for discrete data. The relationships among the categorical variables were analyzed using Pearson's chi-squared test. For results with p < 0.05, we assessed the statistical significance of the findings.
Results
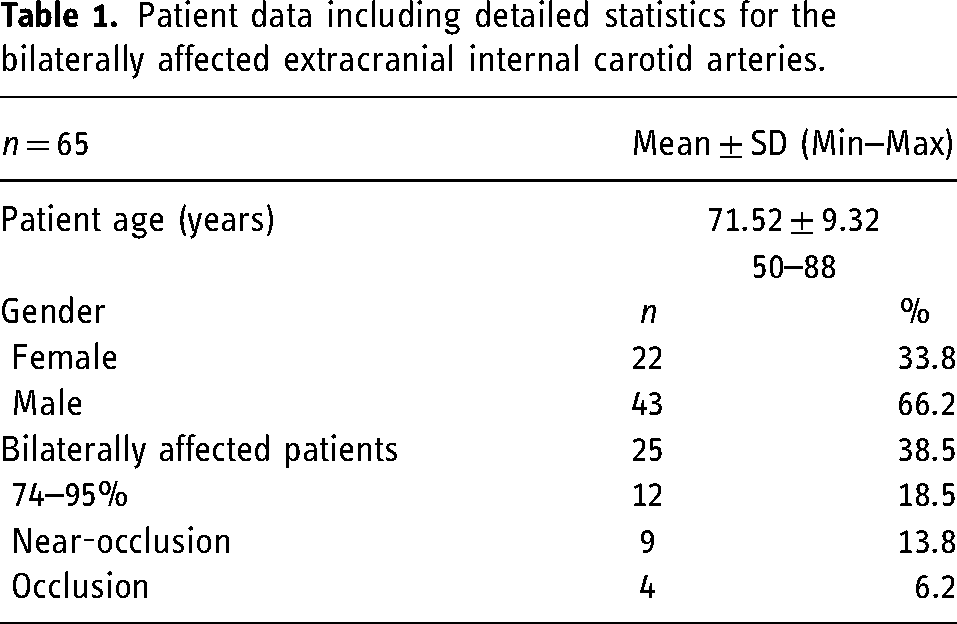
Sixty-five patients (22 female and 43 male) with 74 CNOs were included; 66 (89.2%) of the CNOs were treated in a single session and analyzed. The mean age was 71.52 ± 9.32 years (50–88 years). Twenty-five of the patients (38.5%) were bilaterally affected; 13 of the bilaterally affected patients (52%) had either near-occlusions (9 patients) or occlusions (4 patients) at their contralateral internal carotid arteries (Table 1).
Patient data including detailed statistics for the bilaterally affected extracranial internal carotid arteries.
All patients’ symptomatic ICA stenoses were confirmed with non-invasive imaging within three months prior to the interventional treatment. Thirty-three patients (50.8%) had CTA, 45 patients (69.2%) had CUS and 19 patients (29.2%) had MRA. All CNOs were diagnosed and confirmed with DSA. They were stented for the right side in 32 patients (49.2%), left side in 32 patients (49.2%) and bilaterally in one patient (1.6%). Eighteen of the 66 CNOs treated had collapsed distal ICA pre procedure (27.3%).
One stent was used in 92.3% of the patients (60 patients) and two stents were used in five patients. Four were due to operator preference and one was due to bilateral treatments at the same session. Pre-dilatation was needed in 26 lesions (39.4%) due to unsuccessful primary crossing of the lesions with the EPD or stent system; there was no need for balloon pre-dilatations for the majority of the patients (n = 40) during the filter and stent passages and therefore patients were only post-dilated after stent deployments (100% of the patients). Pre-dilatation before stent deployment was not statistically significant between male and female patients (p = 0.087).
EPDs were used in all treatments. Filterwire EZ was used in 50% (n = 33), Spider FX was used in 42.4% (n = 28) and Emboshield was used in 7.6% (n = 5) cases. Left brachial artery access was used in two patients and right femoral artery access was used in all others. The mean time passed from symptom-to-treatment was 3.91 weeks ± 3.74 weeks (0–20 weeks); 61.4% (n = 40 patients) were treated 3 to 20 weeks after initial diagnoses. There were no technical complications. All patients in this cohort had less than 30% residual stenosis after CAS with an improved distal ICA caliber compared to the initial diameter.
Neurologic status of the patients before CAS was recorded: 63 (96.9%) patients had an mRS of 0, and the other 2 patients (3.1%) had an mRS of 1 and 2 before treatment. There were eight neurological events (12%) recorded in the 30-day period. Five (7.7%) patients developed cerebral hyperperfusion syndrome and another three (4.5%) had ischemic complications. One of the patients was admitted to the ED of our institution at the night of the procedure due to face numbness and MRI confirmed a stroke with micro-embolic areas on the treated side of the patient requiring 10 days of hospitalization. One patient (1.5%) had a stroke at day 15 due to non-compliance to antiplatelet agents. Another patient with a 75% of stenosis on the contralateral ICA (right) diagnosing a watershed infarct two weeks prior to the endovascular treatment of her symptomatic side had a stroke (1.5%) after initial treatment and reached to an mRS of 2 at 90-day control.
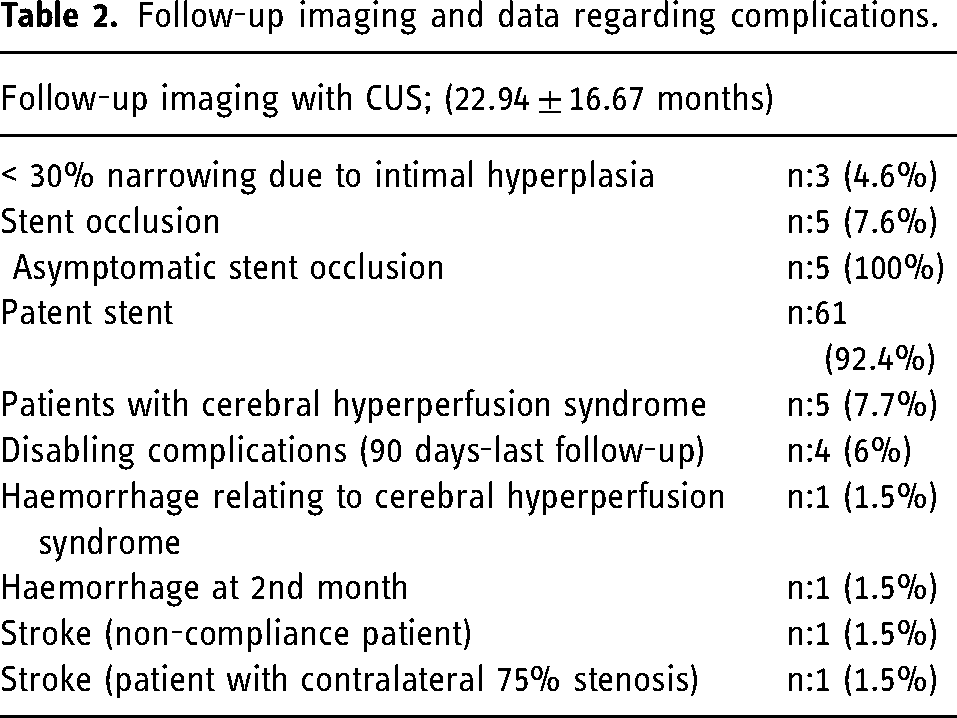
Clinical suspicion of cerebral hyperperfusion syndrome was confirmed by cerebral monitoring (NIRS) test and radiologic imaging including perfusion MRI (Figure 2). All diagnoses of cerebral hyperperfusion syndrome were made during the immediate post-op follow-up period during the first 6 h post-procedure. No patient developed late hyperperfusion syndrome. Patients who developed hyperperfusion syndrome were managed by strict blood pressure control. There were no sustained hypotensive episodes recorded related to balloon angioplasty or stent implantation. Six percent of the patients (n = 4 patients) were worse at 90-day follow-up. One patient (1.5%) died (mRS 6) due to haemorrhage related to cerebral hyperperfusion syndrome. Another patient (1.5%) had a parenchymal haemorrhage diagnosed two months after the treatment and had an mRS of 3 at 90-day control. Four patients with cerebral hyperperfusion syndrome (6%) and one patient with minor stroke (1.5%) were symptom free at 90-day follow-up. In 61 patients (94%) the mRS scores were unchanged in the last follow-up. Follow-up imaging with CUS (mean 22.94 ± 16.67 months, ranging from 1 to 60 months) demonstrated < 50% narrowing due to intimal hyperplasia in three patients (4.6%) and in five patients (7.7%) the stents were occluded at their last follow-up confirmed on DSA. All patients with occluded stents on follow-up were asymptomatic (Table 2).
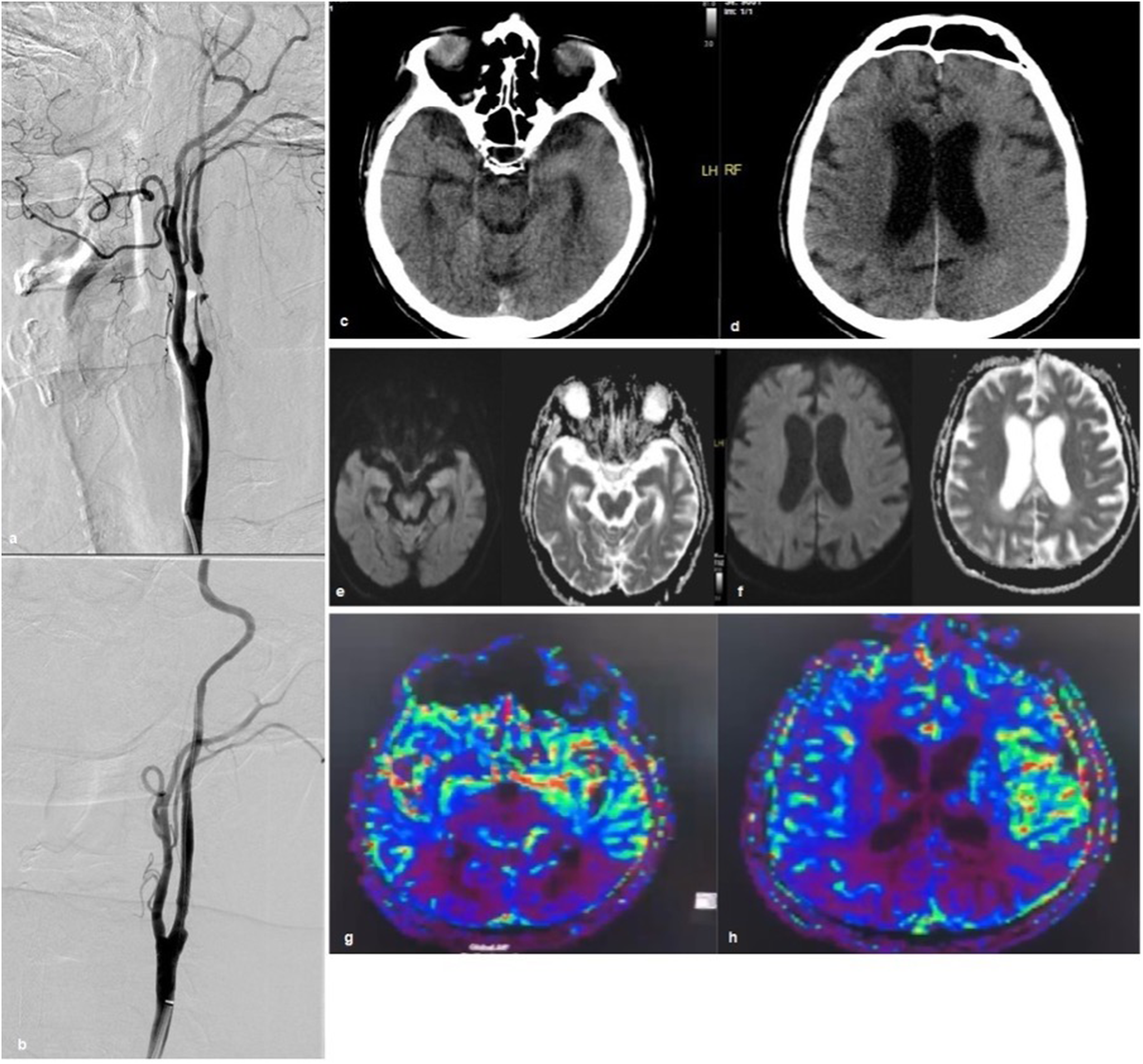
Radiologic images obtained during and after carotid stenting procedure in a patient with cerebral hyperperfusion syndrome diagnosed immediately after balloon angioplasty and stent implantation discharging from hospital one week after intervention without any sequela. (a, b) DSA images of a patient's extracranial ICA indicating a carotid near-occlusion with full collapse prior to and after stent implantation. (c, d) CT images of the same patient demonstrating oedema. (e, f) Diffusion MR images of the patient obtained at similar level with the CT images did not demonstrate any diffusion restrictions. (g, h) Perfusion images and colour maps at the same level.
Follow-up imaging and data regarding complications.
No other strokes or deaths were recorded during the follow-up period for this study. Therefore, permanent neurologic event rate was 6% with 95% demonstrating good outcome with an mRS 0 to 2.
Discussion
Our results demonstrated that CAS for treatment of symptomatic CNOs is technically feasible with acceptable complications rate and good mid-term clinical outcomes. Despite that it is important to note that five patients (7.7%) developed hyperperfusion syndrome and five stents were occluded at the last imaging follow-up demonstrating that further studies are needed to assess the safety and long-term efficacy of this strategy.
Atherosclerotic disease affects male individuals more often; moreover, usually older patients with concomitant comorbidities are treated with endovascular stenting.2,11 Similar to the existing literature, the age distribution of the patients with symptomatic CNOs were similar but male gender was predominant (p < 0.05). Furthermore, most of the study population had coexisting comorbidities such as coronary artery disease with high surgical risks.
CNOs are uncommon affecting approximately 10% of the patients with significant carotid stenosis. 7 Its consequences, however, can be devastating with the risk of stroke. Treatment of this disease by surgical or endovascular strategies remains controversial. The prevalence of the CNO is very low amongst the general population, with an estimated rate of 0.3% for women and 0.5% for men. The management of this vascular pathology has not yet been determined.6,9,12 Management of this group of patients can be very challenging. Neurologic risks causing mortality and morbidity, are higher for the patients with CNOs.3,13–15 Patients with symptomatic >50–70% carotid stenosis have higher risks and the risk of in-hospital stroke or death could be as high as 6%, reaching to 9%, at one month after CAS.3,14 Two studies reported the risk of recurrent stroke after the endovascular revascularization procedures for a heterogeneous group of patients with CNOs to be 3.4% and 10.6%, which are in-line with our study.6,16 In addition, Akkan et al. showed that CNOs can be treated with low complication rates in a heterogeneous population including symptomatic and asymptomatic patients. 17 Our data included only symptomatic patients with CNOs treated with CAS, and demonstrated a rate of 6% of death or permanent neurologic event. It is important to note that one of our complications happened after the patient deliberately stopped the antiplatelet agents resulting in a stroke. Excluding this patient, our rate of death or permanent neurologic event rate would decrease to 4.5%. This demonstrates that CAS in symptomatic patients with CNOs could be beneficial with an acceptable complication rate.
The use of distal EPD device during CAS is standard of care although there is still some debate regarding the safety of CAS without EPD.3,18–22 In our series all cases were performed with distal EPD even though sometimes it is difficult to precisely choose the correct EPD size since the distal cervical carotid lumen is usually collapsed. Balloon dilatation using different techniques have been extensively studied for CAS and the data demonstrate mixed results.21–24 A widely accepted option for balloon angioplasty technique in CAS is predilatating the lesion with a suboptimal dilatation without a post stent dilatation when possible. 3 Plaque rupture is an important complication of balloon angioplasty with unstable atherosclerotic lesions leading to acute thrombosis. Harada et al. demonstrated the potential benefits of post-stent dilatation in their study using an optical coherence tomography device and concluded that early in-stent stenosis or occlusion could be related to skipping the post-dilatation after CAS. 23 Additionally, as mentioned by other authors, plaque rupture can cause devastating complications like acute thrombosis or distal embolus.25–27 We hypothesised that the use of closed-cell stents may decrease the risks of distal embolism from post balloon dilatation due to its less aggressive impingement on the plaque surface; therefore, it is our preferred technique to cross the lesion with the stent prior to any balloon angioplasty unless necessary. In our series, most patients underwent stenting without the need of pre-balloon dilatation. All our patients were treated with closed cell stents and all of them underwent post balloon angioplasty. There were no acute stent occlusions reported in our series and our results regarding complications were in-line with the existing literature for this difficult cohort of patients.
Some of the articles evaluating the results of CAS for asymptomatic CNO point out that these interventions have no benefit for these patients, and they are a matter of debate.16,28 Therefore, some suggest that pre-procedural hemodynamic imaging and tests indicating insufficiency in the intracranial circulation is required to select the patients that will benefit from revascularization.29–33 Another important point is that the risk of cerebral hyperperfusion syndrome after CAS in CNO is higher, and the potential risk for harming patients should be considered. 16 All patients in this study were diagnosed with CNOs, on their prior radiologic imaging, and they were stented from their clinically symptomatic lesion side after reaching a multi-specialty clinical consensus. Patients were monitored with NIRS device during the procedures for cerebral monitoring. We tried to understand cerebral alterations and changes in the cerebral circulatory haemodynamics better using the NIRS device. Using this technique, clinical suspicion of cerebral hyperperfusion syndrome after CAS can be supported with the data from the NIRS device and confirmed with radiologic imaging such as perfusion MRI.
Treatment timing for patients with symptomatic CNO has not been established. These lesions can be treated either acutely (within the first two weeks) or after three weeks on a patient-by-patient basis.2,3 Our median symptom to treatment period was nearly four weeks and nearly half of our population (43%) were treated acutely in the first two weeks. Some authors claimed that CNOs with distally collapsed ICAs should be treated more aggressively because they may have higher risks of neurologic events, if not treated. 34 However, there is non-negligible data demonstrating that the risk of cerebral hyperperfusion syndrome after CAS treatment could be as high as 20% for these patients, with significant morbi-mortality in nearly half of these patients.6–9 The rate of cerebral hyperperfusion syndrome in our study is 7.7% with 20% haemorrhage rate (resulting in mortality) amongst the patients with cerebral hyperperfusion syndrome, which is lower than the existing literature.7,9 The permanent neurologic deficit rate in this study excluding the antiaggregant drug non-compliant patient was 4.5%. Additionally, patients with CNO have a significant risk of ipsilateral stroke which may justify intervention.8,9,16,17 CAS has similar patency rates, and long-term results compared to endarterectomy in CNOs. 35 In our study, the rate of asymptomatic stent occlusion was 7.6% (5 patients). Stent occlusions were slightly more common in distally collapsed ICAs (3 out of 18 patients) comparing to the non-collapsed ICAs (2 out of 48 patients), at a median 22.94 ± 16.67 months of follow-up.
This study has important limitations. Its retrospective nature, lack of a table including a control group from our institution including symptomatic carotid stenosis without near-occlusions or asymptomatic CNOs and/or any data obtained through the existing literature. The relatively small number of patients also preclude a definitive statistical answer regarding the nuances of the disease and of the treatment performed. Nevertheless, due to the uncommon nature of the disease and the treatment performed, this manuscript may provide help in guiding treatment decisions for these patients. Lastly, we only used dual antiplatelet drugs for the patients in our cohort; therefore, there is no comparison group including patients treated with anticoagulant drugs which could be pointed as a limitation for some experts.
Conclusions
Our study demonstrated that in the complex population of patients with symptomatic CNOs, CAS is a technically feasible strategy with acceptable rate of permanent neurologic deficits and good mid-term clinical outcomes. However, the risks of hyperperfusion syndrome and asymptomatic carotid occlusion in follow-up are not negligible. Further studies are needed to assess its safety and long-term efficacy.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical standards and patient consent
We declare that this study has been approved by the Ankara University Clinical Research Ethics Board on 11 July 2023 (İ06-420-23) and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. We declare that all patients gave informed consent prior to inclusion in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.