
Abstract
Background
We evaluated the association of reperfusion quality and different patterns of achieved reperfusion with clinical and radiological outcomes in the ESCAPE NA1 trial.
Methods
Data are from the ESCAPE-NA1 trial. Good clinical outcome [90-day modified Rankin Scale (mRS) 0–2], excellent outcome (90-day mRS0–1), isolated subarachnoid hemorrhage, symptomatic hemorrhage (sICH) on follow-up imaging, and death were compared across different levels of reperfusion defined by expanded Treatment in Cerebral Infarction (eTICI) Scale. Comparisons were also made between patients with (a) first-pass eTICI 2c3 reperfusion vs multiple-pass eTICI 2c3; (b) final eTICI 2b reperfusion vs eTICI 2b converted-to-eTICI 2c3; (c) sudden reperfusion vs gradual reperfusion if >1 pass was required. Multivariable logistic regression was used to test associations of reperfusion grade and clinical outcomes.
Results
Of 1037 included patients, final eTICI 0–1 was achieved in 46 (4.4%), eTICI 2a in 76 (7.3%), eTICI 2b in 424 (40.9%), eTICI 2c in 284 (27.4%), and eTICI 3 in 207 (20%) patients. The odds for good and excellent clinical outcome gradually increased with improved reperfusion grades (adjOR ranging from 5.7–29.3 and 4.3–17.6) and decreased for sICH and death. No differences in outcomes between first-pass versus multiple-pass eTICI 2c3, eTICI 2b converted-to-eTICI 2c3 versus unchanged eTICI 2b and between sudden versus gradual eTICI 2c3 reperfusion were observed.
Conclusion
Better reperfusion degrees significantly improved clinical outcomes and reduced mortality, independent of the number of passes and whether eTICI 2c3 was achieved suddenly or gradually.
Keywords
Background
Endovascular treatment (EVT) has become standard of care in patients with acute ischemic stroke (AIS) after its efficacy and safety was repeatedly demonstrated in clinical trials in the past eight years.1–7 The goal of AIS treatment, be it mechanical or pharmacological, is reperfusion of the ischemic tissue via recanalization of the occluded blood vessel. Thus, it is not surprising that early and successful reperfusion has shown to be an independent predictor of good clinical outcome.8–10 Continuous technical developments in EVT techniques over past years have enabled us to achieve higher rates of successful reperfusion and have broadened the population that can benefit from EVT.7,11,12
First-pass reperfusion 13 is a common and routinely used measure to demonstrate angiographic success which has shown to be associated with improved clinical outcomes. Thus, the current perception among interventionists is that achieving complete or near-complete reperfusion with a single pass should be the primary EVT goal. 14
In this study, we evaluated the association of reperfusion quality and first-pass reperfusion with clinical outcome and presence of hemorrhage on the follow-up scan. The aim of this study was to confirm the previously described impact of reperfusion measures such as first-pass recanalization in a large EVT treated population.
We also hypothesized that those patients with improved final expanded Treatment in Cerebral Infarction (eTICI) 2c3 reperfusion grade had a better clinical outcome than those with the final TICI 2b reperfusion grade. Since previous papers showed that sudden recanalization is associated with improved clinical outcomes, 15 we aimed to confirm these results on multicenter dataset.
Methods
Patient selection
The ESCAPE-NA1 trial (registered with ClinicalTrials.gov, NCT02930018) was approved by the local ethics boards at each participating center. Enrollment occurred from March 2017 to August 2019. Eligible patients underwent EVT for AIS, were above 18 years of age presenting with a disabling ischemic stroke at the time of randomization (baseline National Institutes of Health Stroke Scale [NIHSS] > 5) within 12 h from last known well and who were functioning independently in the community (Barthel Index score > 90) prior to the stroke. Patients with proximal intracranial artery occlusion, defined as an occlusion of the intracranial internal carotid artery (ICA), the first segment of the middle cerebral artery (MCA), or both, that was confirmed on noncontrast CT and multiphase CT angiography, with ASPECTS of 5–10 and moderate-to-good collaterals were included. Detailed inclusion and exclusion criteria have been published previously. 16 Patients with cervical ICA occlusion, patients with spontaneous recanalization, and patients with observed thrombus fragmentation/clot migration on the initial digital subtraction angiography (DSA) into distal branches of MCA (M3 segment and beyond) were excluded. Cases with unavailable final eTICI score or missing procedural information were excluded.
Procedures
The procedural details were published previously. Briefly, patients were randomly assigned to receive a single intravenous dose of nerinetide or saline placebo. All patients were treated with EVT using available devices and techniques including stent-retriever thrombectomy, contact aspiration, or combination of the techniques (the choice of technique was at the discretion of the interventionalist). Patients received intravenous alteplase, according to usual care following national or regional guidelines, before or during EVT at a primary hospital before transfer or at an endovascular center.
Image analysis
Periprocedural DSA series were retrospectively evaluated by a core team consisting of two radiologists (PC and JO), two neurointerventional radiologists (MA and NK), and two neurologists (MM and NS). The core team was blinded to the clinical presentation, outcome, and any demographic data. Evaluation of each pass (defined as every endovascular maneuver targeting the intracranial vessel occlusion) was performed, and the following information was collected: target vessel occlusion for each pass, grade of reperfusion after each pass, and final reperfusion grade using the eTICI scale.
The majority of EVT procedures (967/1105, 87.5%) were completed within three passes. Therefore, detailed evaluation of the first three passes was performed, and the following reperfusion variables were recorded for each patient: first-pass eTICI 2c–3 reperfusion, multiple-pass (final) eTICI 2c3 reperfusion, eTICI 2b reperfusion that was subsequently converted to final eTICI 2c–3 reperfusion with additional passes, sudden eTICI 2c3 reperfusion (eTICI 0 after the first and/or second pass that suddenly changes to eTICI 2c or 3 on the final pass), gradual eTICI 2c3 reperfusion (eTICI 0–2b after the first/second pass, which gradually improved to eTICI 2c or 3 after each pass).
Outcome assessment
The primary outcome of interest was good clinical outcome, defined as 90-day modified Rankin Scale (mRS) 0–2. Secondary outcomes were excellent functional outcome, defined as 90-day mRS 0–1, symptomatic hemorrhage (sICH, defined according to the Heidelberg classification 17 as any intracranial hemorrhage associated with clinical evidence of neurological worsening with the hemorrhage judged to be the principal cause of neurological decline by 4 or more points in NIHSS) on follow-up imaging, isolated subarachnoid hemorrhage without parenchymal hemorrhage on follow-up imaging, and death.
Statistical analysis
Patient angiographic and procedural characteristics were summarized using descriptive statistics. Proportions of primary and secondary outcomes were reported for each eTICI category. Multivariable analyses were performed to derive effect estimates for primary and secondary outcomes using logistic regression with adjustment for patient age, sex, baseline NIHSS, baseline ASPECTS, interaction of alteplase and nerinetide (given the observed interaction effect in ESCAPE-NA1 16 ), and time from groin puncture to reperfusion.
To assess the impact of the following variables, different models were obtained:
First versus multiple pass—within the subgroup of patients with final eTICI 2c3, outcomes were compared between patients with first-pass versus multiple-pass eTICI 2c3 reperfusion and effect estimates were derived for primary and secondary outcome using logistic regression. The models were adjusted for patient age, sex, baseline NIHSS, baseline ASPECTS, interaction of alteplase and nerinetide, and time from groin puncture to reperfusion. eTICI 2b reperfusion grade was used as a reference. Final eTICI 2b versus patients with eTICI 2b that was converted to eTICI 2c3 in a subsequent pass(es). Primary and secondary outcomes were compared. The models were adjusted for patient age, sex, baseline NIHSS, baseline ASPECTS, interaction of alteplase and nerinetide, time from groin puncture to reperfusion and the number of passes. eTICI 2b reperfusion grade was used as a reference. Sudden eTICI 2c3 versus gradual eTICI 2c3 reperfusion. Primary and secondary outcomes were compared. Models were adjusted for patient age, sex, baseline NIHSS, baseline ASPECTS, interaction of alteplase and nerinetide, time from groin puncture to reperfusion, and the number of passes. Sudden eTICI 2c3 reperfusion was used as a reference.
Missing primary outcomes (n = 9) were imputed as mRS 6 (as the worst possible outcome). All statistical tests were two-sided and conventional levels of significance (two-sided alpha < 0.05) were used for interpretation. All analyses were performed in Stata 16.1.
Results
Of 1105 patients that were enrolled into the trial between March 2017 and August 2019, 15 patients with cervical ICA occlusion, 6 patients with spontaneous recanalization, and 25 patients with thrombus migration into peripheral branches were excluded. Final eTICI could not be assessed in 7 cases and the procedural information about the performed EVT was missing in 16 patients, leaving 1037 patients for the analysis.
Patient baseline characteristics were reported in detail previously. 16 The primary occlusion sites on the first DSA run were terminal ICA (n = 199, 19.2%), M1 segment of the MCA (n = 676, 65.2%), or M2 segment of the MCA (n = 162, 15.6%). The median time from groin puncture to reperfusion was 37 min [interquartile range (IQR) 22–56 min]. The median number of passes was 1 (IRQ 1–2). Digital subtraction angiography and procedural characteristics are listed in Table 1.
Patient DSA and procedural characteristics.
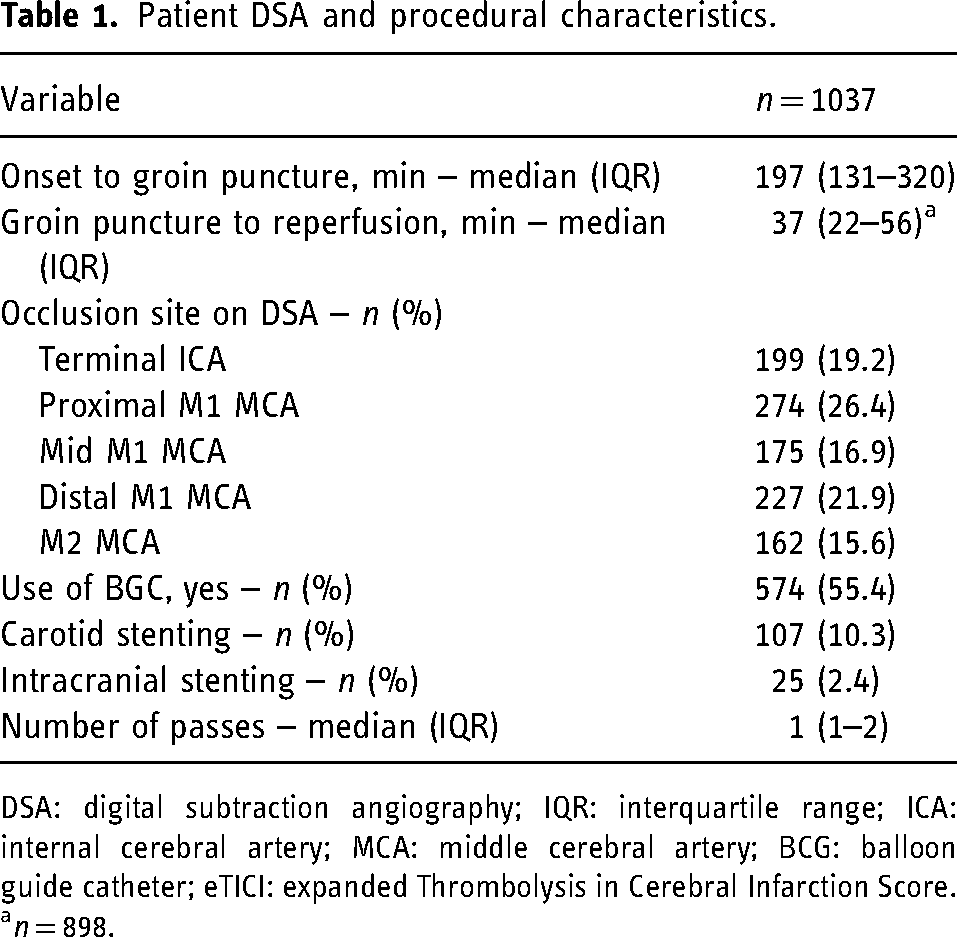
DSA: digital subtraction angiography; IQR: interquartile range; ICA: internal cerebral artery; MCA: middle cerebral artery; BCG: balloon guide catheter; eTICI: expanded Thrombolysis in Cerebral Infarction Score.
an = 898.
Expanded treatment in cerebral infarction and clinical outcome
Final eTICI 0–1 was achieved in 46 patients (4.4%), eTICI 2a was achieved in 76 patients (7.3%), eTICI 2b in 424 patients (40.9%), eTICI 2c in 284 patients (27.4%), and eTICI 3 in 207 patients (20%). The median number of passes was 3 (IRQ 2–4) for eTICI 0–1 reperfusion grade, 2 (IQR 1–4) for eTICI 2a reperfusion grade, and 1 (IRQ 1–2) for reperfusion grades eTICI 2b, eTICI 2c, and eTICI 3 [similarly, the median number of passes for combined eTICI 2c–3 subgroup was 1 (IRQ 1–2)]. Independent of reperfusion status, good clinical outcome was achieved in 627/1037 patients (60.5%) and excellent clinical outcome in 421/1037 patients (40.5%). Isolated SAH was present in 19 patients (1.8%) and sICH in 33 patients (3.2%). The frequency of good and excellent clinical outcome consistently improved with each point improvement in grade of reperfusion in comparison to eTICI 0–1 (Table 2).
Primary and secondary outcomes in the study subgroups (treatment group vs. control group) based on the grade of reperfusion defined as eTICI.
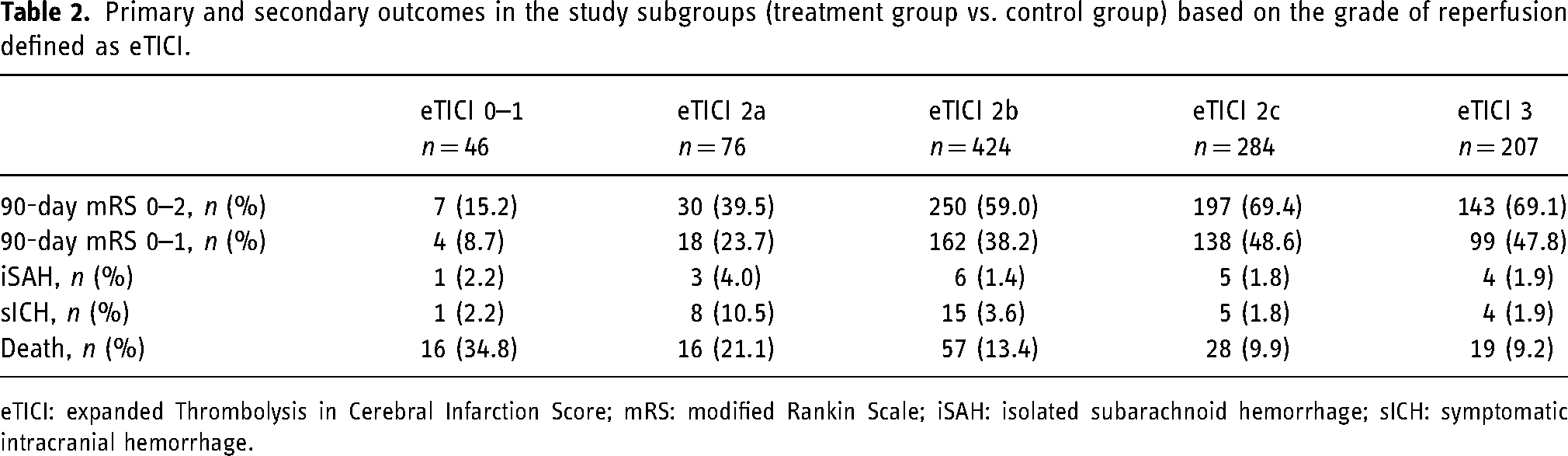
eTICI: expanded Thrombolysis in Cerebral Infarction Score; mRS: modified Rankin Scale; iSAH: isolated subarachnoid hemorrhage; sICH: symptomatic intracranial hemorrhage.
When assessing the effect of eTICI in the adjusted analysis, every 1-point improvement in eTICI increased the likelihood for achieving good and/or excellent outcome compared to no reperfusion (eTICI 0), with the highest odds for complete eTICI 3 reperfusion [adjOR 29.3; 95% confidence interval (CI) 11.2–77.1 and adjOR 17.6; 95%CI 5.7–54.2, respectively], Supplementary Table 1. Results for the mortality were similar with gradually decreasing odds with improved reperfusion grade (Supplementary Table 1). (Of note: adjusted analysis was not performed for isolated SAH and sICH due to low numbers in each category.) The proportions of the 90-day clinical outcome based on the grade of reperfusion are graphically depicted in Figure 1.
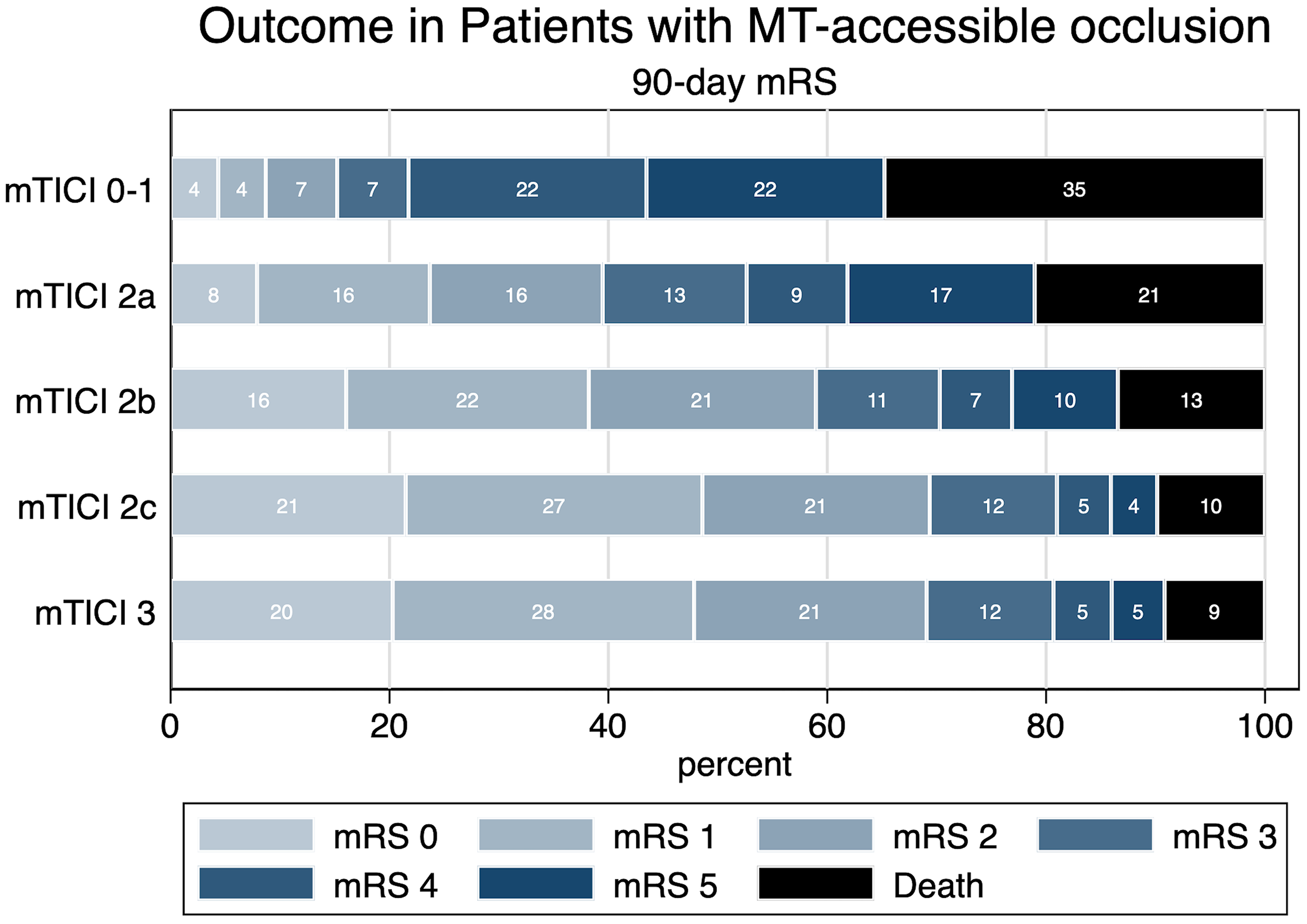
Graphical illustration of 90-day clinical outcome expressed as modified Rankin Scale based on the eTICI reperfusion grade. mRS categories are shown in ascending order from left to right. Numbers in the bars represent percentages of patients in each mRS category.
First-pass effect versus multiple-pass eTICI 2c3 and clinical outcome
First-pass eTICI 2c3 reperfusion was achieved in 318/1037 (30.7%) patients, and multiple-pass eTICI 2c3 reperfusion in 173/1037 (16.7%) patients. The median time from groin puncture to reperfusion was 26 min (IQR 18–38 min) for first-pass eTICI 2c3 and 49.5 min (IQR 36–70 min) for multiple-pass eTICI 2c–3 (p ≤ 0.001). The median number of passes in multiple eTICI 2c–3 reperfusion was 2 (IQR 2–3)
Good clinical outcome was achieved in 217/318 patients (68.2%) with first-pass eTICI 2c3 and in 123/173 patients (71.1%) with multiple-pass eTICI 2c3. Excellent clinical outcome was achieved in 159/318 patients (50.0%) with first-pass eTICI 2c3 and in 78/173 patients (45.1%) with multiple-pass eTICI 2c3. Isolated SAH and sICH occurred in 3/318 (0.9%) and 4/318 (1.3%) patients with first-pass eTICI 2c3, and in 6/173 (3.5%) and 5/173 (2.9%) patients with multiple-pass eTICI 2c3. Twenty-eight of 318 patients (8.8%) with first-pass eTICI 2c3 and 19/173 patients (11.0%) with multiple-pass eTICI 2c3 died within 90 days. In the adjusted analyses, there was no significant association of clinical outcome with first-pass eTICI 2c3 versus multiple-pass eTICI 2c3, Table 3.
Multivariable logistic regression analysis for clinical and radiological outcomes in patients with first-pass versus multiple-pass eTICI 2c3, patient eTICI 2b subsequently converted to eTICI 2c3 and in patients with sudden versus gradual eTICI 2c3 reperfusion.
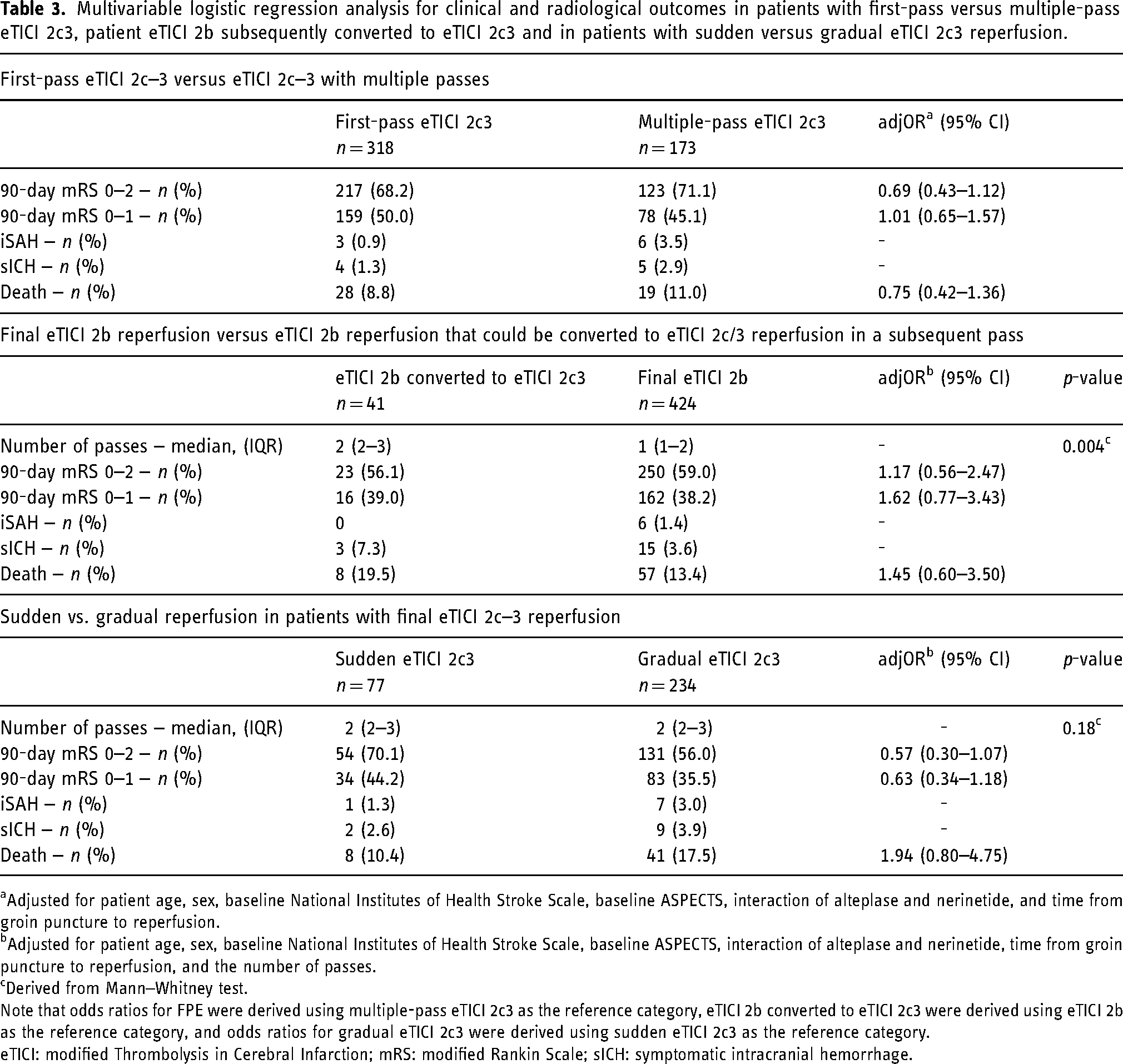
aAdjusted for patient age, sex, baseline National Institutes of Health Stroke Scale, baseline ASPECTS, interaction of alteplase and nerinetide, and time from groin puncture to reperfusion.
bAdjusted for patient age, sex, baseline National Institutes of Health Stroke Scale, baseline ASPECTS, interaction of alteplase and nerinetide, time from groin puncture to reperfusion, and the number of passes.
cDerived from Mann–Whitney test.
Note that odds ratios for FPE were derived using multiple-pass eTICI 2c3 as the reference category, eTICI 2b converted to eTICI 2c3 were derived using eTICI 2b as the reference category, and odds ratios for gradual eTICI 2c3 were derived using sudden eTICI 2c3 as the reference category.
eTICI: modified Thrombolysis in Cerebral Infarction; mRS: modified Rankin Scale; sICH: symptomatic intracranial hemorrhage.
Final eTICI 2b versus eTICI 2b converted to eTICI 2c3
Expanded Treatment in Cerebral Infarction 2b was achieved in 424/1037 (40.9%) patients and among those, eTICI 2b was converted to eTICI 2c3 in a subsequent pass in 41 (3.9%) patients [with the median of 2 (IRQ 2–3) passes in total].
Good clinical outcome was achieved in 23/41 patients (56.1%) with eTICI 2b converted to eTICI 2c3 and in 250/424 patients (59.0%) with eTICI 2b. Excellent clinical outcome was achieved in 16/41 patients (39.0%) with eTICI 2b converted to eTICI 2c3 and in 162/424 patients (38.2%) with eTICI 2b. Isolated SAH and sICH occurred in 0/41 and 3/41 (7.3%) patients with eTICI 2b converted to eTICI 2c3, and in 6/424 (1.4%) and 15/450 (3.6%) patients with final eTICI 2b. Eight of 42 patients (19.5%) with eTICI 2b converted to eTICI 2c3 and 57/24 patients (13.4%) with eTICI 2b died within 90 days.
In the adjusted analyses, there was no significant association of clinical or radiological outcomes and eTICI 2b converted to eTICI 2c3 versus final eTICI 2b reperfusion, Table 3.
Sudden versus gradual eTICI 2c3 reperfusion
In 311 patients with eTICI 2c3 who required multiple passes, the target occlusion remained unchanged until eTICI 2c3 reperfusion was achieved in 77 (24.8%) patients, and gradual reperfusion was observed in 234 (75.2%) patients.
Good clinical outcome was achieved in 54/77 patients (70.1%) with sudden eTICI 2c3 and in 131/234 patients (56.0%) with gradual eTICI 2c3. Excellent clinical outcome was achieved in34/77 patients (44.2%) with sudden eTICI 2c3 and in 83/234 patients (35.5%) with gradual eTICI 2c3. Isolated SAH and sICH occurred in 1/77 (1.3%) and 2/77 (2.6%) patients with sudden eTICI 2c3, and in 7/234 (3.0%) and 9/234 (3.9%) patients with gradual eTICI 2c3. Eight of 77 patients (10.4%) with sudden eTICI 2c3 and 41/234 patients (17.5%) with gradual eTICI 2c3 died within 90 days.
In the adjusted analyses, there was no significant association of clinical or radiological outcomes with gradual eTICI 2c3 reperfusion versus sudden eTICI 2c3 reperfusion, Table 3.
Discussion
In this post hoc analysis of the randomized controlled ESCAPE-NA1 trial, better reperfusion grade as measured by the eTICI Score significantly improved clinical outcomes and reduced mortality, independent of the number of passes, and speed of achieving eTICI 2c3 (sudden vs. gradual). The fact that higher degrees of reperfusion results in better post-EVT outcomes makes intuitive sense and is well known from the existing EVT literature.18–20
Previous studies have suggested that first-pass eTICI 2c3 (so-called “first-pass effect” or FPE) is associated with better outcomes compared to no FPE, perhaps because of a reduction of hemorrhagic complications, less vessel injury, and reduced procedure times/shorter time to reperfusion. FPE has therefore been suggested as a new outcome metric and quality indicator in EVT.13,21 In line with previous results, outcomes in patients with FPE were nominally slightly better compared to multiple-pass eTICI 2c3 in the current study, except for excellent outcome. However, after adjusting for baseline characteristics, we did not observe any significant differences in outcomes of patients with FPE compared to multiple-pass eTICI 2c3. Possible explanations for the lack of such associations in multivariable analysis may include confounding by baseline characteristics, imbalanced group sizes in our study, whereby twice as many patients had FPE compared to multiple-pass eTICI 2c3. Furthermore, EVT tools and techniques have evolved since the impact of FPE has first been described, and thus, fewer passes may have been required in the non-FPE group compared to previous studies (with the median of one additional pass in the multiple-pass eTICI 2c–3 group). Indeed, Tonetti et al., 22 which performed a multivariable analysis as well, found that the benefit of eventually achieving successful reperfusion outweighs the risk conveyed by additional passes that are necessary to achieve it.
We also evaluated the impact of sudden versus gradual eTICI 2c–3 reperfusion. Data from the cardiac literature suggest that gradual reperfusion may be favorable when performing percutaneous coronary intervention for ST-segment elevation myocardial infarction, possibly because it results in greater preservation of microvascular integrity and less reperfusion injury. 23 In contrast to that, Requena et al. 15 demonstrated the association of the sudden reperfusion with the higher likelihood of improved functional outcome in their single-center study. In this multicenter dataset, we were not able to repeat their results as we did not find significant differences between sudden and gradual eTICI 2c3 reperfusion, despite numerically higher number of patients achieving favorable and excellent outcome in the group of sudden eTICI 2c–3 reperfusion. Possible reasons for this nonsignificant trend may be a shorter time to complete reperfusion (particularly when sudden reperfusion is achieved early on, in the first or second pass) or reduced risk of distal embolization (i.e., the clot “comes out in one piece” as opposed to retrieval of the clot “piece by piece” with iatrogenic clot fragmentation and potential embolization of the most distal parts). Of note, these considerations are purely hypothetical and further studies are therefore warranted to prove or discard them.
The potential effect of improved reperfusion that can be achieved with additional EVT passes on clinical outcome is the matter of ongoing investigation. Although Flottmann et al. 24 reported the higher frequency of favorable outcome among patients with mTICI 3 reperfusion compared to mTICI 2b patients while the outcomes were compared separately after the first, second, and third pass, the effect of achieved TICI 3 reperfusion on favorable outcome could no longer be observed after 3 or more passes. In agreement with these results, we were not able to demonstrate a benefit of improved reperfusion after additional passes in patients with prior eTICI 2b that was eventually converted to final eTICI 2c3, despite the fact that eTICI 2c3 reperfusion group had better outcome than eTICI 2b group when the whole dataset was analyzed. A possible explanation for such a discrepancy may be a low number of patients in the converted eTICI 2c3 group (41 out of 491 patients with final eTICI 2c3 reperfusion).
Similarly to our findings, in the recent report by Winkelmeier et al. 25 on patients with large volume infarcts, the authors did not show an additional benefit of eTICI 3 reperfusion compared to eTICI 2b. 25 This, however, could be a specific finding for the large infarct volume group of patients, while the remaining eTICI 2b perfusion defect may reflect perfusion through the already infarcted brain. In contrast, in a more detailed analysis of eTICI 2b patients 26 was reported that patients with potentially targetable residual occlusions had worse clinical outcome that those with more peripherally located/multiple nontargetable perfusion defects on the final DSA. 26 All these findings suggest that there remains a need to better understand the pathophysiology behind the residual perfusion defects and to identify patients who could most benefit from additional endovascular attempts or other adjunctive therapies.
Limitations
Our analyses are all post hoc, nonrandomized observations that need to be interpreted in that context. The main aim of the trial was to study the effects of NA-1 in stroke and not to investigate the various procedural steps and techniques.
Although high-quality data were collected prospectively from multiple centers around the world, there was not set up a uniform procedural approach or material use, and this choice was left on the operator's decision based on local (personal) customs and preferences.
In conclusion, better reperfusion degrees overall improved clinical outcomes and reduced mortality, irrespective of how many passes were required and whether eTICI 2c3 was achieved suddenly or gradually. Although we were not able to prove that FPE or subsequent passes lead to better outcome, eTICI 2c3 reperfusion still seems to be the most relevant technical EVT outcome and should be of high priority when performing EVT in AIS.
Supplemental Material
sj-docx-1-ine-10.1177_15910199241288874 - Supplemental material for Effects of reperfusion grade and reperfusion strategy on the clinical outcome: Insights from ESCAPE-NA1 trial
Supplemental material, sj-docx-1-ine-10.1177_15910199241288874 for Effects of reperfusion grade and reperfusion strategy on the clinical outcome: Insights from ESCAPE-NA1 trial by Petra Cimflova, Johanna M Ospel, Nishita Singh, Martha Marko, Nima Kashani, Arnuv Mayank, Andrew Demchuk, Bijoy Menon, Alexandre Y Poppe, Raul Nogueira, Ryan McTaggart, Jeremy L Rempel, Michael Tymianski, Michael D HILL, Mohammed A Almekhlafi and Mayank Goyal in Interventional Neuroradiology
Supplemental Material
sj-doc-2-ine-10.1177_15910199241288874 - Supplemental material for Effects of reperfusion grade and reperfusion strategy on the clinical outcome: Insights from ESCAPE-NA1 trial
Supplemental material, sj-doc-2-ine-10.1177_15910199241288874 for Effects of reperfusion grade and reperfusion strategy on the clinical outcome: Insights from ESCAPE-NA1 trial by Petra Cimflova, Johanna M Ospel, Nishita Singh, Martha Marko, Nima Kashani, Arnuv Mayank, Andrew Demchuk, Bijoy Menon, Alexandre Y Poppe, Raul Nogueira, Ryan McTaggart, Jeremy L Rempel, Michael Tymianski, Michael D HILL, Mohammed A Almekhlafi and Mayank Goyal in Interventional Neuroradiology
Footnotes
Consent to participate
Signed informed consent to participate in the trial was obtained from the patients, their legally authorized representative, or, if required by applicable national laws or regulations for obtaining consent, from the investigator after consultation with an independent physician who was not otherwise participating in the trial.
Contributorship
PC, JO, NS, MM, NK, AM, MA, and MG contributed to the study conception and design. Material preparation, data collection, and analysis were performed by PC, JO, NS, MM, NK, AM, and MA. The first draft of the manuscript was written by PC and JO. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data availability
Data used in the current study are available from the author upon reasonable request.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Financial interests: PC reports honoraria from ESMINT, outside the submitted work. JO reports consultancy fee from NicoLab. ADM received grants from NoNO; honoraria from Medtronic; patent Circle NVI. MT is CEO of NoNO; patents owned by NoNO. BKM has stock options in Circle NVI and has consulted for Biogen and Boehringer Ingelheim. AYP has received a project research grant from Stryker and honoraria from BMS-Pfizer. MDH has received consulting fees from Sun Pharma and Brainsgate and has stock options in Circle NVI. MG reports consultancy for Medtronic, Stryker, Microvention, GE Healthcare, Mentice, outside the submitted work. All other authors have nothing to disclose. Nonfinancial interests: ADM is a member of the editorial board at International Journal of Stroke (Editor). AYP is PI of EASI-TOC study. BKM is a member of the editorial board at Stroke (Assistant Editor). MDH is Director, Board of Circle Neurovascular, Director, Board of the Canadian Neuroscience Federation, and Director, Board of the Canadian Stroke Consortium. MG is a member of the editorial board at Stroke (Consulting Editor).
Ethical considerations
This study was approved by the local ethics committee of the University of Calgary (ID: ESCAPE-NA1, REB-19-3029).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: The ESCAPE-NA1 trial was funded by the Canadian Institutes for Health Research, Alberta Innovates, and NoNO Inc. (Grant number: 389143).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.