
Abstract
Background
Wide-necked bifurcation aneurysms (WNBA) of the middle cerebral artery (MCA) present significant therapeutic challenges. Flow-diverter stents have been increasingly adopted for their management, though they may give rise to adverse outcomes such as in-stent stenosis (ISS). This study explores the association between stent oversizing and the incidence of ISS following flow-diverter stent placement in MCA bifurcation aneurysms.
Methods
A retrospective study included 34 patients who underwent flow-diverter stent placement for MCA bifurcation aneurysms between 2020 and 2023. Data on patient demographics, aneurysm morphology, and stent sizing were collected. ISS was evaluated through follow-up imaging at 6-month post-procedure. Stent oversizing was determined by calculating the difference between the stent diameter and the proximal and distal parent vessel diameters. Statistical analyses included Pearson correlation and chi-square tests, with significance established at p < 0.05.
Results
The studied group had a mean age of 57.8 years, with 81.6% female patients. The average aneurysm neck size was 3.6 mm, with a mean dome-to-neck ratio of 1.6. ISS was detected in 64.7% of cases proximally and 88.2% distally. A statistically significant negative correlation (r = −0.496, p = 0.003) was observed between stent oversizing and ISS, indicating that increased stent oversizing was associated with a higher incidence of ISS, particularly in the distal vessel segments.
Conclusion
The findings indicate that stent oversizing is significantly associated with the development of ISS in MCA bifurcation aneurysms treated with flow-diverter stents. Careful consideration of stent sizing, particularly minimizing oversizing in distal segments, may mitigate the risk of ISS and improve clinical outcomes. These results underscore the importance of meticulous stent selection and procedural planning in neurointerventional practice.
Introduction
Despite the significant technological progress in the endovascular treatment of brain aneurysms, a large part of them still pose a challenge for the modern interventionalist. Such types of aneurysms include wide-necked bifurcation aneurysms (WNBA) especially located on the middle cerebral artery (MCA). 1 To overcome the obstacles in treating this type of pathology, flow-diverter implants are increasingly being used with contradictory results.2,3 These stents have previously been established for treating aneurysms with wide necks located mainly along the course of the internal carotid artery, with satisfactory safety and efficacy profiles. Compared to currently available techniques, such as balloon or stent-assisted coiling, flow-diverter treatment for MCA bifurcation aneurysms is associated with a technically easier procedure. However, the rate of observed complications should not be disregarded. 4
The main complications after flow-diversion treatment of bifurcation aneurysms are acute hemorrhagic and ischemic incidents, with the latter being more often described. Regardless of the applied dual antiplatelet therapy, late complications are represented by covered side branch occlusion, caliber reduction, and in-stent stenosis (ISS). 5 The reporting of ISS is often overlooked due to its tendency to have a relatively benign nature and undergo regression, either spontaneously during follow-up or after prolonged usage of either single or dual antiplatelet therapy. However, it is not entirely certain whether the condition always has a favorable course, and investigating the potential mechanisms for its onset would contribute to a better understanding of the process.6,7 Some of the proposed mechanisms leading to ISS may involve processes like microthrombus formation, endothelial cell hyperplasia and growth, smooth muscle cell proliferation, vessel remodeling, changes in shear stress, disruptions in the balance of vasodilator and vasoconstrictor factors, stent oversizing, and sub-acute stent deformities. These factors collectively contribute to the narrowing or constriction of the diameter of the blood vessel at the site of the stent placement, leading to ISS. The exact mechanisms may vary depending on individual patient factors and clinical context.8,9
Because of the lack of a unified grading system for ISS and a non-insignificant discrepancy in the results of different authors, we can surmise that this phenomenon is largely underappreciated by the endovascular community.
We set out to evaluate the existence of a correlation between stent oversizing and ISS after flow diversion of MCA bifurcation aneurysms.
Materials and methods
We conducted a retrospective study using our prospectively collected database for the period from 2020 to 2023 regarding patients with MCA aneurysms treated at our institution with a flow-diverter stent.
To include patients in the current study, we used the following criteria:
At least one treated MCA bifurcation aneurysm through flow diversion. At least one follow-up was performed with a minimum time period of 6 months after the procedure. Adequate compliance with the prescribed dual antiplatelet therapy (DAPT). No immediate adverse effects were observed after the procedure.
Characteristics of patients and aneurysms
For the purposes of this study, basic demographic data (gender and age), data regarding the characteristics of the aneurysms (location, neck size, aspect, and dome-to-neck ratios), and the geometric characteristics of the parent vessel into which the implant was delivered were collected. The geometric characteristics of the aneurysm and the adjacent vessels were assessed based on images obtained during 3D rotational angiography or 2D images from digitally subtracted angiography (DSA).
Endovascular procedures—general considerations
All procedures were performed under general anesthesia using a bi-plane angiographic system, Philips-Azurion. The arterial access used was the right femoral with a 6F sheath. After performing a four-vessel panangiography, a guiding catheter was introduced into the target internal carotid artery. 3D rotational angiography was performed for aneurysms with more complex geometry and those that were difficult to differentiate from the local vascular anatomy. The subsequent steps involved selective catheterization of the MCA and successful deployment of the implant.
Follow-up and flow-diverter assessment
To assess the treatment effect, follow-up was conducted at an average of 6 months after the procedure using magnetic resonance imaging or DSA. Data were collected regarding the type and size of the used stent and the oversizing of the implant (measured in millimeters) relative to the proximal and distal parent vessel diameter into which the stent was delivered. ISS from the implanted device was assessed in percentages by measuring the proximal and distal diameters of the parent vessel at the 6-month follow-up (Figure 1).
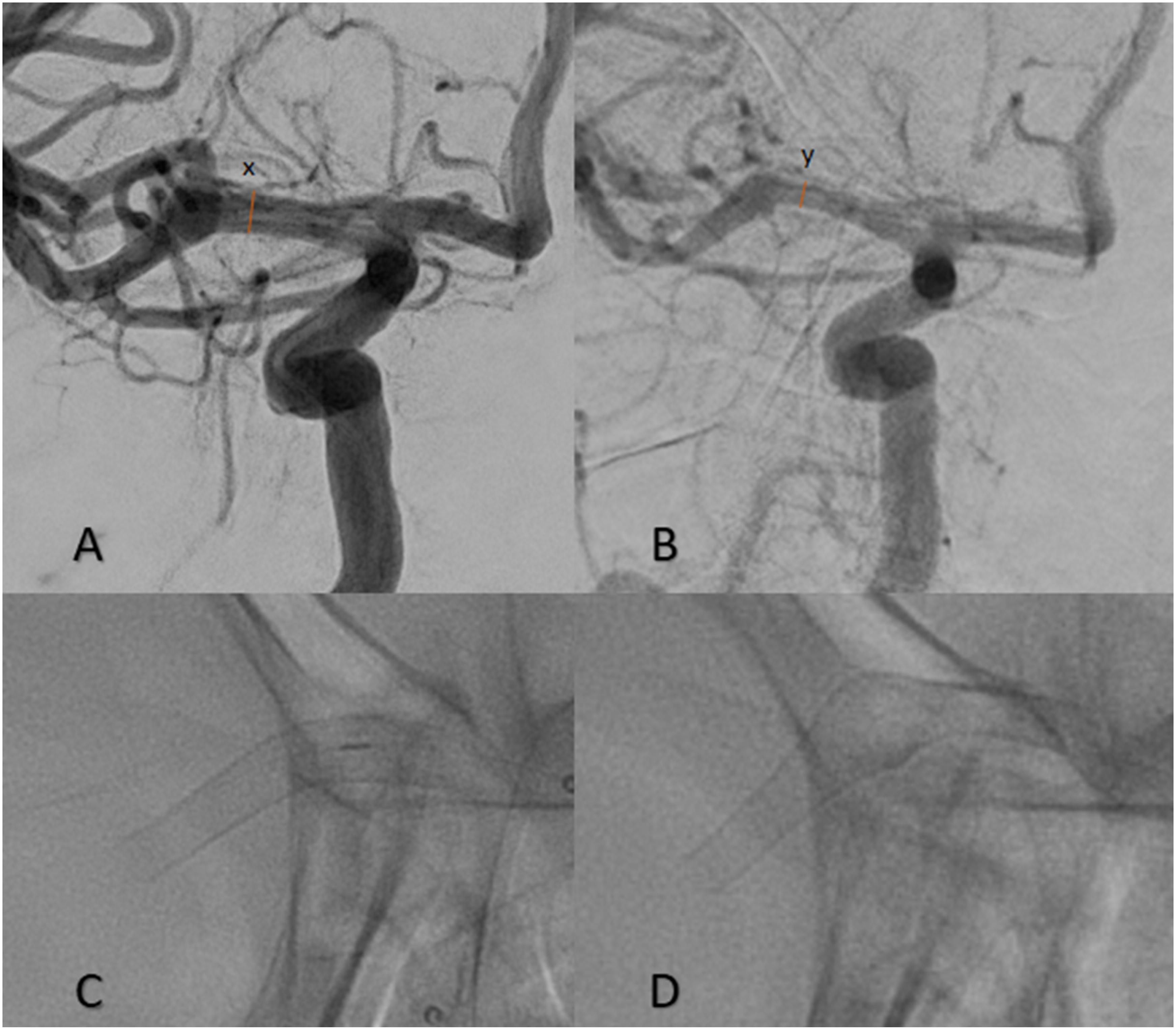
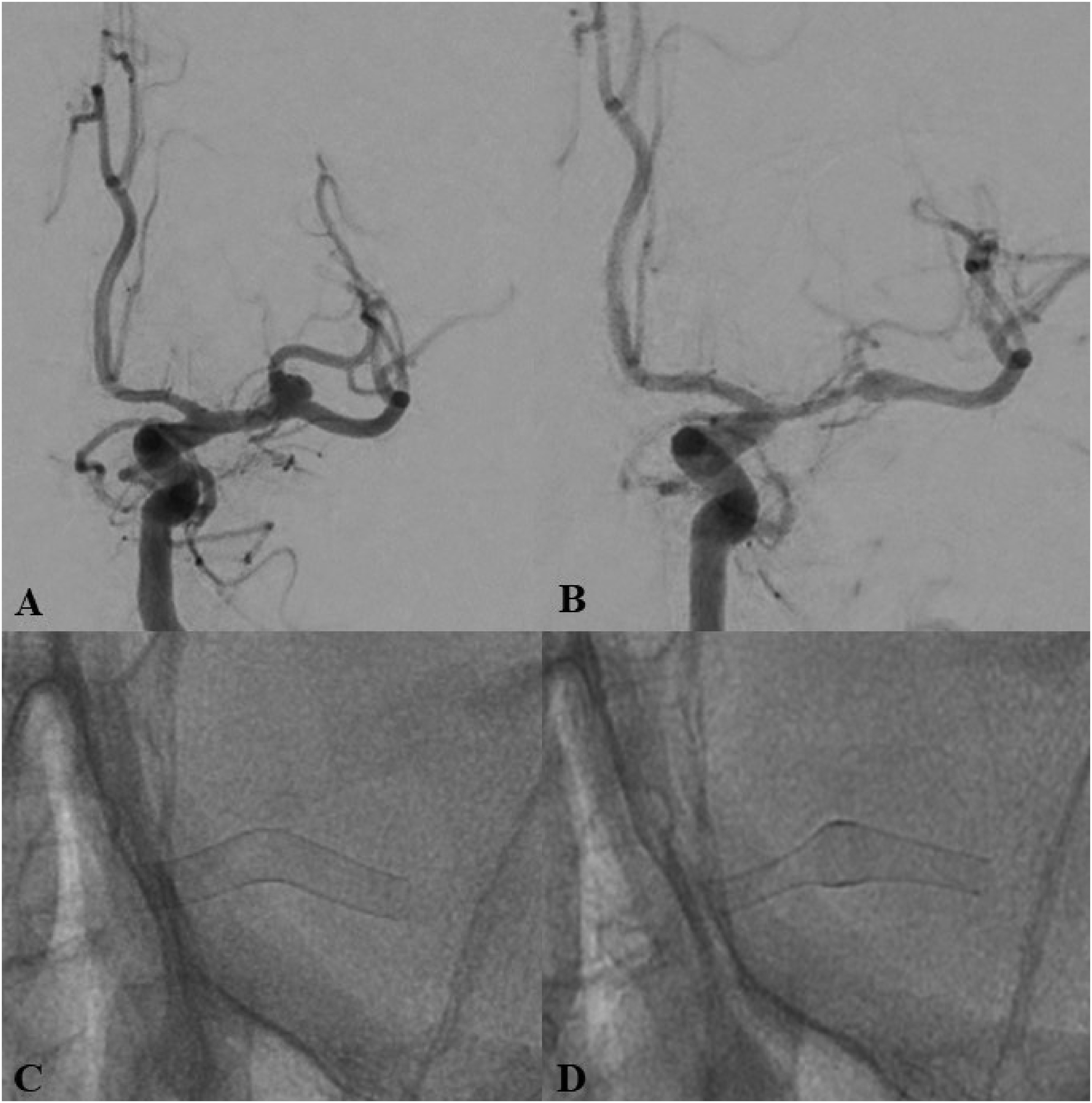
DSA imaging of a patient with a treated right MCA aneurysm intra-procedurally (A) and post-procedurally (B). Single-shot images were taken during the procedure (C) and at follow-up (D). The measurements acquired from both images were used to determine the percentage of in-stent stenosis, which occurred after the treatment during the mid-term follow-up (sixth month). The formula by which we calculated the percentage reduction of the vessel segment caliber was x–y/x.
Statistical methods
For the purpose of the study, the following methods were employed: descriptive statistics, chi-square test (to examine dependencies between categorical variables with two or more categories), and correlation analysis.
The accepted significance level was α = 0.05, with statistical significance defined as p < 0.05. The data analysis was conducted using the specialized statistical software package SPSS (Statistical Package for the Social Sciences), version 29.0.
Results
Characteristics of patients and aneurysms
The specified criteria were met by 34 patients treated at our institution from 2020 to 2023. The mean age of the patients is 57.8 years (SD ± 8.9), with a predominance of females at 81.6% (n = 31). All treated aneurysms were located at the bifurcation of the MCA. The aneurysms have the following characteristics: mean neck size—3.6 mm (SD ± 1.5), mean dome-to-neck ratio—1.6 (SD ± 0.6), and mean aspect ratio—1.4 (SD ± 0.6). Prior coiling was performed in 11.8% of the aneurysms (4/34). The mean proximal vessel diameter into which the flow-diverter stent was placed was 2.6 mm (SD ± 0.3), with a minimum of 2.15 mm and a maximum of 3.42 mm. The distal vessel diameter of the same parent vessel had mean values of 2.3 mm (SD ± 0.32), with a minimum of 1.5 mm and a maximum of 3.27 mm (Table 1).
Demographics, aneurysm, and vessel characteristics of the 34 treated patients.
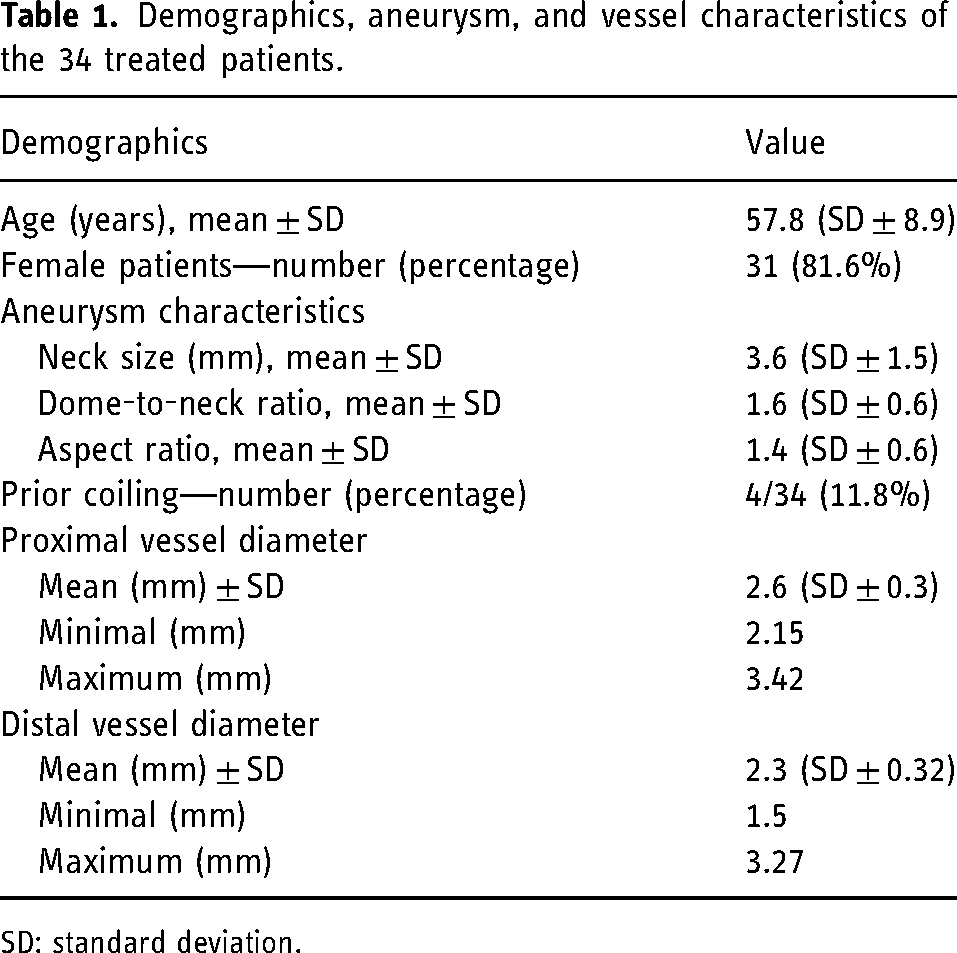
SD: standard deviation.
Characteristics of the used flow-diverter stents
Aneurysms in the population were treated using two types of devices: p48 and p64 (Phenox, Bochum, Germany), along with their variants: p48 MW and p48 HPC, p64, p64 MW, and p64 HPC. Patients treated with p48 and p64 were evenly distributed, each comprising 50% of the cases. Among the p48 group, the p48 MW variant predominated in 88.2% (15/17) of cases, while in the p64 group, p64 HPC was most frequently used in 53% (9/17) of cases. The used implants had sizes of 3, 3.5, and 4 mm, with the most common size between the two groups being 3 mm.
Upon analyzing the results regarding implant oversizing, we found the following values: proximal oversizing was performed with an average of 0.74 mm (SD ± 0.6), and distal oversizing with an average of 0.96 mm (SD ± 0.32; Table 2).
Technical details regarding the procedure—devices used and oversizing.
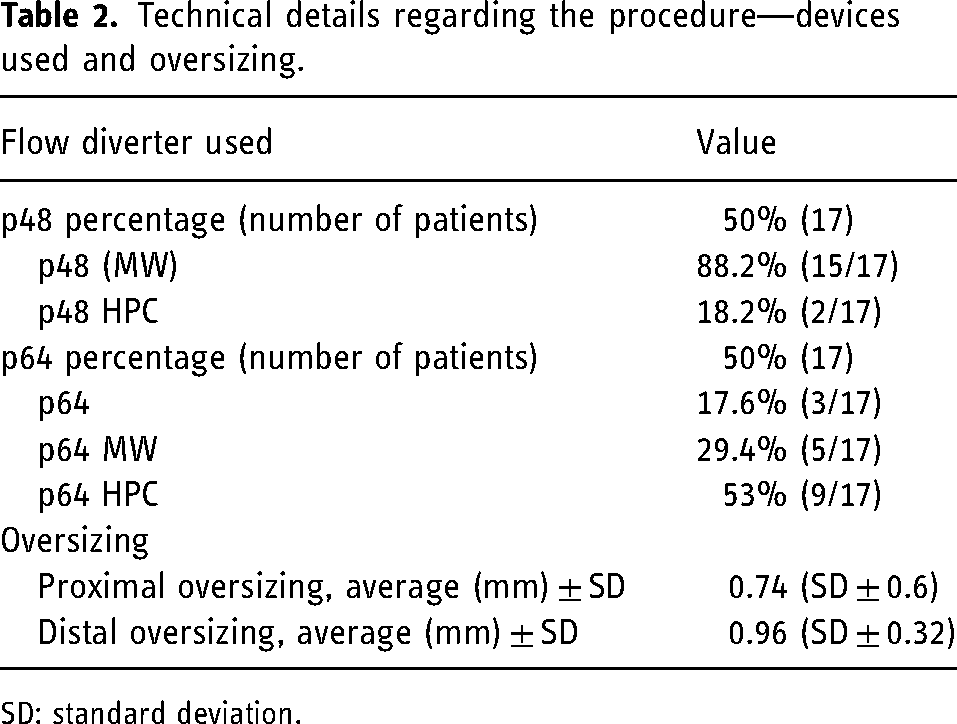
SD: standard deviation.
Safety profile
We did not observe any symptomatic peri- and post-procedural events directly related to the procedure. During one of the interventions, a thromboembolic complication (2.6%) was observed, which regressed completely without any clinical symptoms after the intra-arterial administration of a GpIIb/IIIa inhibitor.
Follow-up and assessment of the parent vessel stenosis
The first follow-up imaging study was conducted on an average of 6 months after the procedure: DSA in 44.1% (15/34) of cases and magnetic resonance imaging (MRI) in 55.9% (19/34) of cases. ISS was assessed with respect to the proximal and distal parts of the vessel in which the stent was placed. Proximally, ISS was not observed in 26.5% of cases (9/34), in 64.7% (22/34) of cases, ISS was observed to be <25%, and in 8.8% (3/34) of cases, ISS limited the vessel lumen between 25% and 50%. Regarding the distal vessel, ISS was not detected in 11.8% (4/34) of cases, in 44.1% (15/34) of cases, ISS with <25% reduction in lumen was observed, and in another 44.1% (15/34) of cases, ISS led to lumen reduction in the range of 25%–50%. Expressed in percentages, ISS proximally averaged 12% (SD ± 7.5) and distally averaged 24% (SD ± 10.9).
To assess the impact of oversizing on the occurrence of ISS and for the purposes of statistical analysis, we examined the following dependencies: the influence of the type of stent used on ISS, the size of the implant used on ISS, and the effect of oversizing on ISS. We did not find any statistically significant relationship between the type and size of the implant used and the likelihood or severity of ISS (p > 0.05).
To determine the oversizing, we used the following steps (Figures 2, 3 and 4). We identified three values of the vessel diameter, measured at equal distances from each other, namely proximal, middle, and distal portions where the stent would be deployed. The arithmetic mean of the obtained values was compared to the same measurements taken during the control imaging study at 6 months after the procedure, following the implant placement. We conducted a correlation analysis to examine the relationship between oversizing and ISS. The Pearson correlation coefficient (r) was calculated to be approximately −0.496, indicating a moderate negative linear relationship between oversizing and vessel diameter. This negative correlation was statistically significant with a p-value of 0.003. The negative correlation coefficient suggests that as oversizing of the stent increased, there was a tendency for vessel diameter to decrease. We also investigated the impact of oversizing separately in the proximal and distal portions of the vessel and its relationship to the development of ISS. The correlation analysis between proximal oversize in mm and ISS, revealed a positive Pearson correlation coefficient of r = 0.339 (p = 0.050), indicating a positive relationship between the two variables. This suggests that as proximal oversizing increases, there tends to be an increase in ISS. While the p-value is marginally significant, further investigation and a larger sample size may be needed to confirm this relationship.
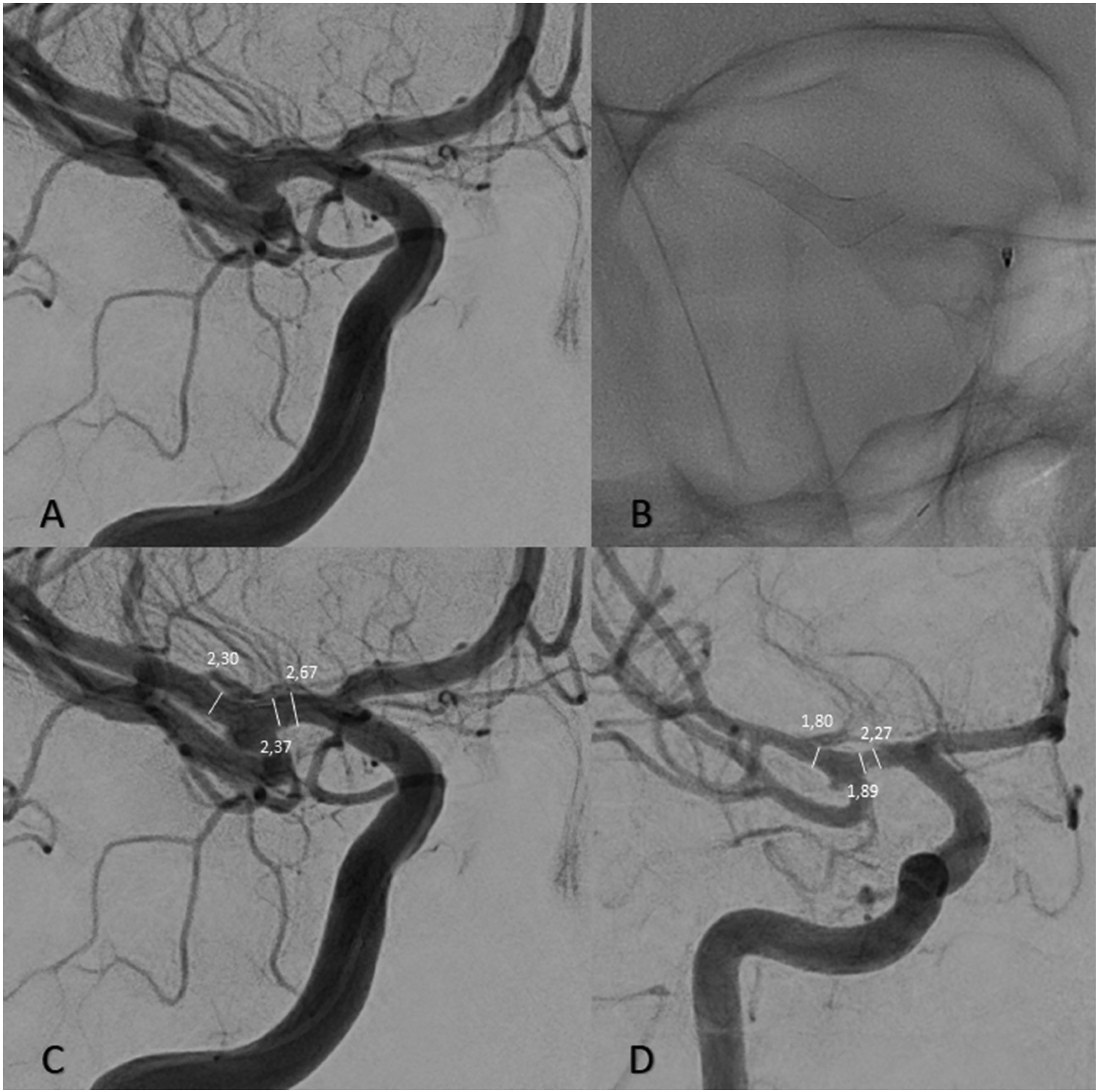
A representative case of a patient treated through flow diversion for an aneurysm of the right MCA bifurcation. (A) intra-operative DSA in a working projection. (B) A single-shot image of the implanted stent. (C) We made measurements of the proximal, bifurcation, and distal parts of the vessel in the area of the implant (in millimeters). (D) Control DSA on the sixth post-procedural month, again measuring the vessel at the same points. The figure showcases our approach toward the measurements taken into account for the statistical analysis of all patients included in the study.
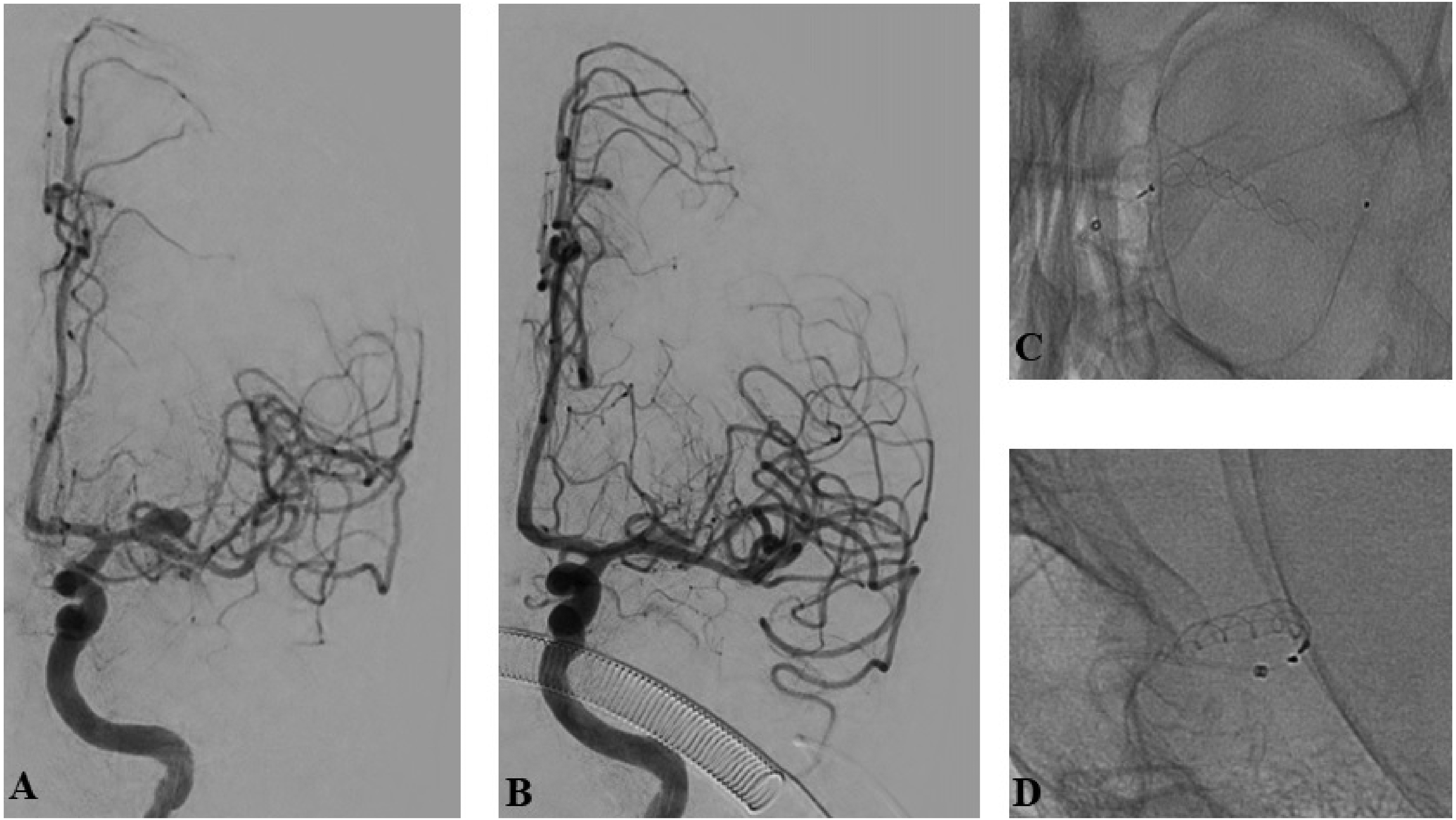
A representative case of a patient with a complex left middle cerebral artery aneurysm, treated with a p64 flow-diverter stent. (A) Left internal carotid artery injection demonstrating the aneurysm; (B) intraprocedural DSA after stent placement, showing almost complete absence of contrast filling of the aneurysmal sac; (C, D) frontal and lateral projection of the implant.
Case example of a patient with a bifurcational left MCA aneurysm. Given the width of the aneurysmal neck and its morphology, the placement of an FD into the inferior MCA trunk was considered an appropriate treatment strategy. Radiological follow-up of the patient demonstrated the complete occlusion of the aneurysm, along with notable changes in the MCA vasculature and the tubular structures of the FD implant. (A) DSA in working projection before implant delivery; (B) DSA in working projection at 6-month follow-up, demonstrating asymptomatic reduction of the lumen of the middle cerebral artery; (C) configuration of the implant at the end of the procedure; (D) deformation of the implant in its proximal part, as well as in the area of the aneurysmal sac.
Discussion
Our results show a significant difference in the occurrence of ISS after flow diversion when considering the sizing of the intra-luminal implant. Due to the nature of oversizing, we cannot account for the diameter of both the proximal and distal landing zones of the stent. Usually, the distal landing zone is a non-negligible value smaller in diameter compared to the proximal one, which we measure for the choice of the device. This fact can lead to what we can call a disproportionate sizing of flow-diverters simply because of arterial vessel divergence in physiological conditions.
Several factors can be taken into account as to why this would be meaningful and have an impact on follow-ups. The most important one, perhaps, is the fact that the implant has active properties, determined by its sizing and oversizing, compared to the parent vessel. In a study from 2009, Chen et al. 10 showed that wall-shear stress, wall-shear stress gradient, and the oscillatory shear index all change when going through different sizing options for a given vessel diameter. In their study, the authors also point out that the struts of the implant lead to damage of the endothelial cells, which contributes to the underlying pathological cascade that is about to occur. Furthermore, the stress exerted by the implant and the difference in the force gradients between the struts’ marginal zones and the uncovered endothelium monolayer kick-starts an inflammatory reaction in the vessel, which benefits intimal hyperplasia. 11 The iatrogenic creation of microscopic flow disturbances and small spatial gradients at the lumen interface are at the core of the development of intimal dysfunction. 12
The altered mural stress caused by the radial force of the implant is also an important part of the process. An oversized implant exerts more radial stress on the vessel until it reaches its nominal diameter. 13 The wall reaction to these forces can be surmised by activating the smooth muscle cells and the derived growth factors associated with intimal hyperplasia. 14
What is also interesting is the fact that some authors point out age as an independent factor that determines the possibility of the development of intimal hyperplasia. 15 Brandes et al. 16 concluded that apart from the higher cardiovascular risk, older age is associated with a reduction of the regenerative capacity of the endothelium. The cell senescence and subsequent stagnant functions of the endothelium can perhaps partly explain the paradoxical phenomenon that is observed.
A large problem concerning the topic is a lack of unified criteria to describe the incidence of ISS. Different authors cite an occurrence anywhere between 10% and 50%.17–20 This fact could lead us to the conclusion that its rate is still relatively undisclosed and underappreciated. As in our cases, ISS in the MCA segments could be more detrimental due to the smaller caliber of treated vessels. A small narrowing in the case of internal carotid artery ISS would be significant in the territory of the MCA and can have detrimental consequences for the patient. A preexisting collateral network for the hemisphere or rapid development of leptomeningeal collaterals can become a protective factor, but the risk remains high. 21
Again, making a parallel between the internal carotid artery (ICA) and MCA flow-diversion therapy, we can also conclude that what seems to be a small oversizing for the ICA (0.5 mm) can be seen as an exaggerated stent oversizing in the M1 and M2 segments. Choosing an optimal branch of the M2 segment, where the flow diverter (FD) would be positioned, with minimal size discrepancy compared to the M1 segment, could lead to more favorable outcomes.
Flow diversion for MCA aneurysms to this day still faces some controversy. Despite its relatively high occlusion rates, with different authors citing numbers over 80% on long-term follow-up,22–24 the complication and mortality rates in the same studies and retrospective analyses also show non-negligible values of around 10% and 1%–2%, respectively. The symptomatic cases are often linked with thromboembolic and stenotic complications, associated with ISS and jailed side branches occlusion and reduction of blood-flow velocity. As in typical cases of bifurcation aneurysms, oftentimes the M1 and M2 segments of the MCA can be incorporated in the aneurysmal neck or even arise from the sac, which further increases the risk of occlusion of the incorporated side branches, as well as decrease the pace of occlusion. 25 The choice of the correct device size can, in turn, remedy some of the complications. Stent oversizing should account for three things: higher porosity to keep the jailed branches patent for as long as possible, adequate wall apposition, and as small as a discrepancy between the parent M2 branch diameter and stent oversizing.
Considering the nature of MCA bifurcation aneurysms, a thorough evaluation of the local vascular anatomy is necessary to pick a correct form of treatment. Aneurysms with favorable dome-to-neck ratios without incorporated side branches may not present difficulty for simple or assisted coiling techniques, but appreciation of the occlusion and recanalization rates of the different methods is also vital. In cases of complex, wide-necked aneurysms, flow diversion remains a simple solution to a complicated problem.
Conclusion
Flow diversion is a vital treatment option for MCA bifurcation aneurysms in the arsenal of neurointerventional radiologists. The benefits and drawbacks of the method should be carefully taken into account before treatment. Our study found a positive correlation between stent oversizing and the ISS of the treated vessel on the conducted control imaging methods. Based on the presented data, we can conclude that minimal oversizing of the flow diverter of both the proximal and distal portions of the MCA can yield better results when concerning the phenomenon of ISS. The choice of the distal landing zone bifurcation vessel should be based on minimal discrepancy compared to the M1 segment.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.