
Abstract
Purpose
Contact aspiration mechanical thrombectomy (CAMT) with 0.088-inch catheters may improve first-pass success rates, but delivery of such catheters can be challenging and limit effectiveness. This study examines the initial multicenter experience using the FreeClimb 88 catheter paired with the Tenzing 8 delivery catheter.
Materials and Methods
Retrospective analysis was performed of consecutive patients with large vessel occlusion (LVO) of the internal carotid artery (ICA) or M1 segment of the middle cerebral artery treated with off-label CAMT using the FreeClimb 88 and Tenzing 8 at eight sites participating in the early limited release for these devices. Demographic and procedural variables were collected and analyzed with descriptive statistics and multivariable analysis.
Results
Fifty-three consecutive patients were treated. Large vessel occlusion was located in the ICA in 19/53 (35.8%) patients; 34/53 (64.2%) were in the M1 segment. FreeClimb 88 was successfully delivered to the site of occlusion in 50/53 (94.3%) of patients. First-pass TICI 2c or 3 was achieved with FreeClimb 88 delivered by Tenzing 8 in 36 (67.9%) cases. Among cases with successful FreeClimb 88 delivery 9/50 (18.0%) required additional smaller devices to perform thrombectomy of distal occlusions after recanalization of the initial LVO. No complications or symptomatic hemorrhages occurred following thrombectomy.
Conclusion
Contact aspiration mechanical thrombectomy performed for ICA or M1 LVOs using FreeClimb 88 delivered with Tenzing 8 was safe, effective, and efficient in this early experience, with first-pass TICI 2c or 3 was achieved in 68% of patients without procedural complications occurring in any cases.
Introduction
Contact aspiration mechanical thrombectomy (CAMT) is an efficacious, efficient, and cost-effective means of rapidly restoring perfusion in stroke patients with large vessel occlusion (LVO).1–3 Clinical trials have shown similar rates of successful reperfusion and clinical outcomes when comparing CAMT to stent retriever (SR) thrombectomy for LVOs.1,2 Proposed advantages of first-line CAMT over SR include faster time to first pass, less need to select distal artery branches with a microwire or microcatheter beyond an embolus, decreased endothelial damage, decreased vessel traction during device withdrawal for a thrombectomy pass, decreased clot fragmentation, and decreased cost.4,5 In spite of these advantages, in the ASTER trial, first-line CAMT was associated with 32.8% crossover rates to SR thrombectomy or combined SR with local aspiration, either due to inability to deliver the aspiration catheters to the target occlusion or unsuccessful thrombectomy after the initial attempt. 1 Additionally, incomplete ingestion of thrombus by the aspiration catheter can be a source of distal emboli. 6
Aspiration catheter design improvements have permitted increased suction force through larger inner diameter (ID) at the tip and improved catheter trackability. Use of larger bore catheters for CAMT is associated with increased aspiration flow rates, first-pass effect (FPE), faster recanalization, reduced procedure time, and better reperfusion rates.7,8 Recently, super large-bore catheters (SLBC) with distal IDs of 0.088 inches have been developed to reach the middle cerebral artery (MCA) M1 segment. In vitro studies have shown better ingestion of clots, including challenging fibrin-rich clots, and these findings have been borne out in reports of early clinical experience.9–14
Recently, a novel full-length 0.088-inch distal ID catheter, FreeClimb 88 (Route 92 Medical, San Mateo, California, USA), was introduced for access to the cerebral vasculature. This catheter is available in two working lengths, 132 cm or 125 cm, with braided nitinol construction. Additional 0.088 distal ID catheters have recently been developed, including Zoom 88 (Imperative Care, Campbell, California, USA) and Sofia 88 (MicroVention, Inc., Aliso Viejo, California, USA).
Concurrent to development of the FreeClimb 88, a specialized delivery catheter, Tenzing 8 (Route 92, San Mateo, CA), was developed to assist the tracking of SLBCs to the target site. The Tenzing 8 ledge-reducing delivery device occupies the entire lumen of the FreeClimb 88 catheter to facilitate delivery.15,16 Compared to traditional aspiration catheter delivery using a microwire and microcatheter, Tenzing 8 significantly reduces the ledge or space between itself and the tip of the FreeClimb 88 catheter, which is especially important with increasing caliber of aspiration catheters that have a greater tendency to catch on the ophthalmic artery or anterior cerebral artery origins and encounter increased friction in tortuous anatomy. In an in vitro study, Tenzing device enabled delivery of aspiration catheters to the proximal M1 in half the time compared to leading with a microwire and microcatheter. 15 The Tenzing may provide a more robust rail in the center of the vessel lumen that avoids need for a SR. It may also be less disruptive to the clot and less likely to induce thrombus fragmentation and distal embolization. Initial reports have shown the technical feasibility of CAMT with SLBC, as well as with Tenzing 8 combined with the HiPoint catheter (Route 92, San Mateo, CA), a novel 0.088-inch ID catheter-on-a-wire.17–19
In this case series, the initial multicenter clinical experience is reported for use with the full-length FreeClimb 88 catheter delivered using Tenzing 8 for CAMT of internal carotid artery (ICA) terminus and M1 segment MCA occlusions. It is hypothesized that the Tenzing 8 and FreeClimb 88 combination is associated with consistent and rapid access to the clot, increased FPE, and diminished use of a stent-retriever. 20
Methods
Consecutive patients undergoing CAMT for LVO using the Tenzing 8 delivery catheter and FreeClimb 80 access catheter at eight different stroke centers from May 2022 to April 2024 were retrospectively reviewed from prospectively collected institutional databases. Eligible patients received intravenous thrombolytic therapy according to American Heart Association (AHA) Guidelines. 21 All patients who received MT had LVO of the ICA or M1 identified on computed tomography (CT) angiogram. Patient selection for thrombectomy was based on the most recent AHA Guidelines using advanced imaging with noncontrast head CT, CT angiography, and CT perfusion. 21 Since this study is observational in nature with no patient contact by virtue of its retrospective collection of prospectively gathered anonymized data, informed consent was not required by participating centers. Data collection and analysis were performed under an institutional review board approved protocol at the principal investigator's institution (CPMCRI protocol 2.16.17). During the study period, FreeClimb 88 was not FDA approved as an intracranial aspiration catheter for mechanical thrombectomy; the cases included in this study involve off-label use.
Study variables
Data collected for each patient included age, biological sex, stroke severity on arrival measured by the National Institutes of Health Stroke Scale (NIHSS), baseline functional status as measured by modified Ranking Scale (mRS) before symptom onset, IV thrombolytic use, and time of arterial access. Patient imaging, including admission CT and CT angiography, was reviewed to document the admission Alberta Stroke Program Early CT score (ASPECTS), and the location of the vascular occlusion. Angiography, clinical and procedural reports, and follow-up CT or MRI were reviewed to document outcome variables: number of passes, reperfusion time, procedural complications, rate of symptomatic intracerebral hemorrhage, and procedural complications. Reperfusion score using the modified Thrombolysis in Cerebral Ischemia (mTICI) grading scale was used to document prethrombectomy occlusion and postthrombectomy revascularization. Symptomatic intracerebral hemorrhage was defined using the European Australian Cooperative Acute Stroke Study II definition: any intracerebral hemorrhage on any posttreatment imaging after the start of tissue plasminogen activator and increase of ≥4 points on the NIHSS points. 22
Technique
Thrombectomy procedures were performed by one of 21 experienced neurointerventionalists. In brief, transfemoral vascular access was obtained using a 9F or 10F femoral arterial sheath. A Base Camp (Route 92 Medical, San Mateo, CA) 0.106-inch ID guide catheter or 8F Shuttle sheath (Cook Medical, Bloomington, IN) was advanced into the proximal cervical segment of the ICA or distal common carotid artery over Berenstein tip Nav Cath (Route 92 Medical, San Mateo, CA) or comparable inner catheter.
The Free Climb 88 and Tenzing 8 are shown in Figure 1. Delivery with Tenzing was employed in all cases. In brief, this technique involves positioning the Tenzing 8 delivery catheter within the FreeClimb 88 catheter so that the distal tip of the FreeClimb catheter was immediately proximal to the proximal marker of the Tenzing 8 where its tip tapers. The Tenzing 8 was locked in this position with the rotating hemostatic valve on the hub of the FreeClimb catheter. Loading a 0.014–0.016-inch microwire inside the Tenzing is optional. These catheters were then advanced as a single unit until the distal tip marker of the Tenzing 8 reached the angiographic limit of contrast at the site of the LVO (Figure 2). The Tenzing 8 was then pinned and the Freeclimb 88 catheter advanced over the Tenzing 8 to the angiographic limit of contrast (Figure 2, Supplemental Videos). During this maneuver, Tenzing 8 tip movement was concurrently observed to ensure that the angiographic limit of contrast is not excessively crossed by the proximal marker of the Tenzing 8 tip. In some cases, subtle back-and-forth movements of the Tenzing 8 during FreeClimb advancement assisted in reducing the static friction between catheters and vessel wall to assist delivery of the FreeClimb to the target. Once the FreeClimb 88 catheter reached the angiographic limit of contrast, the Tenzing 8 delivery catheter was removed, and the Freeclimb 88 catheter was allowed to advance passively into the occlusion, as the vacuum created by Tenzing 8 removal may assist with clot ingestion (Supplemental Videos).16,19 Vacuum aspiration was then applied to the FreeClimb catheter with a Penumbra pump (Penumbra, Inc., Alameda, California, USA) for 2–5 min or upon return of free-flowing blood in the aspiration tubing indicating complete ingestion of the clot. The Freeclimb 88 was then slowly withdrawn (Figure 2). Infrequently, a microwire (0.014–0.016 inch) was utilized when the tip of the Tenzing 8 device engages a side branch of the parent artery such as the ophthalmic, posterior communicating, or anterior communicating artery. Following this technique, if incomplete recanalization was identified, additional aspiration thrombectomy attempts were made. In some cases, if accessible distal emboli were present, or rescue therapy was necessary, additional devices were used to perform thrombectomy additional passes. Types of additional devices used were left to individual operator discretion.
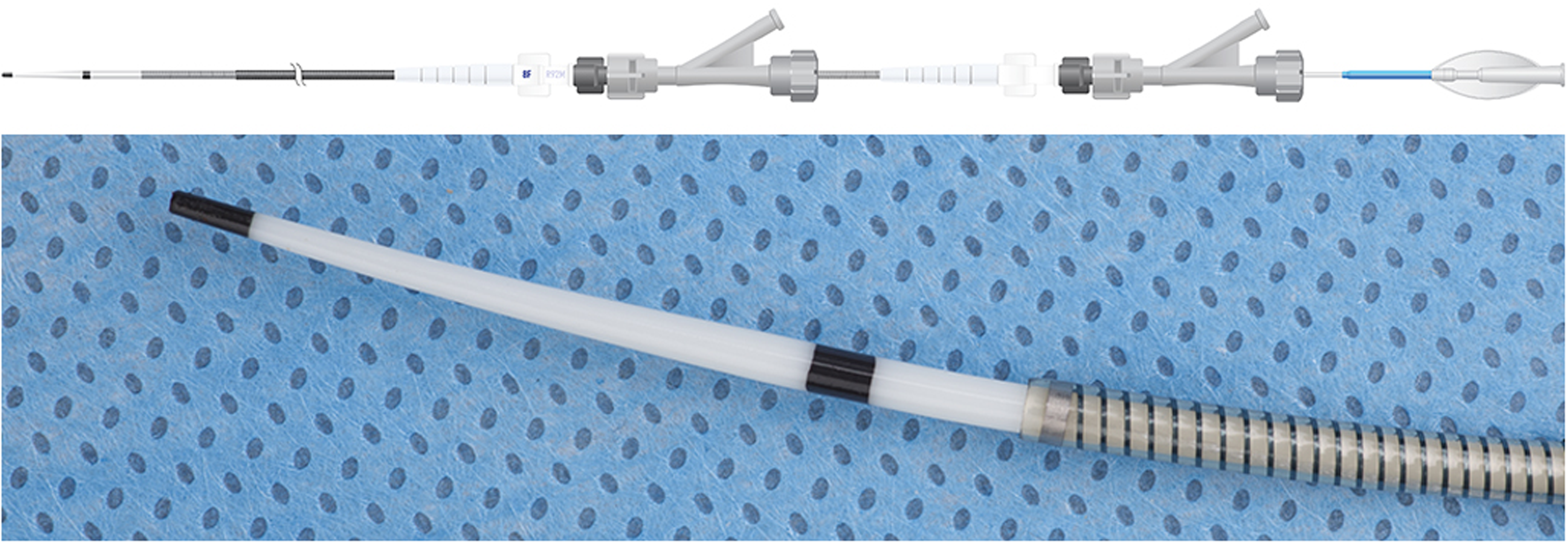
(a) Schematic representation of the Tenzing 8 device in the FreeClimb 88 full-length catheter and Basecamp guide catheter, which both have rotating hemostatic valves. (b) Photograph of the tip of the Tenzing 8 device beyond the tip of the FreeClimb 88. The tapered portion of the Tenzing 8 is demarcated by black radiopaque markers.
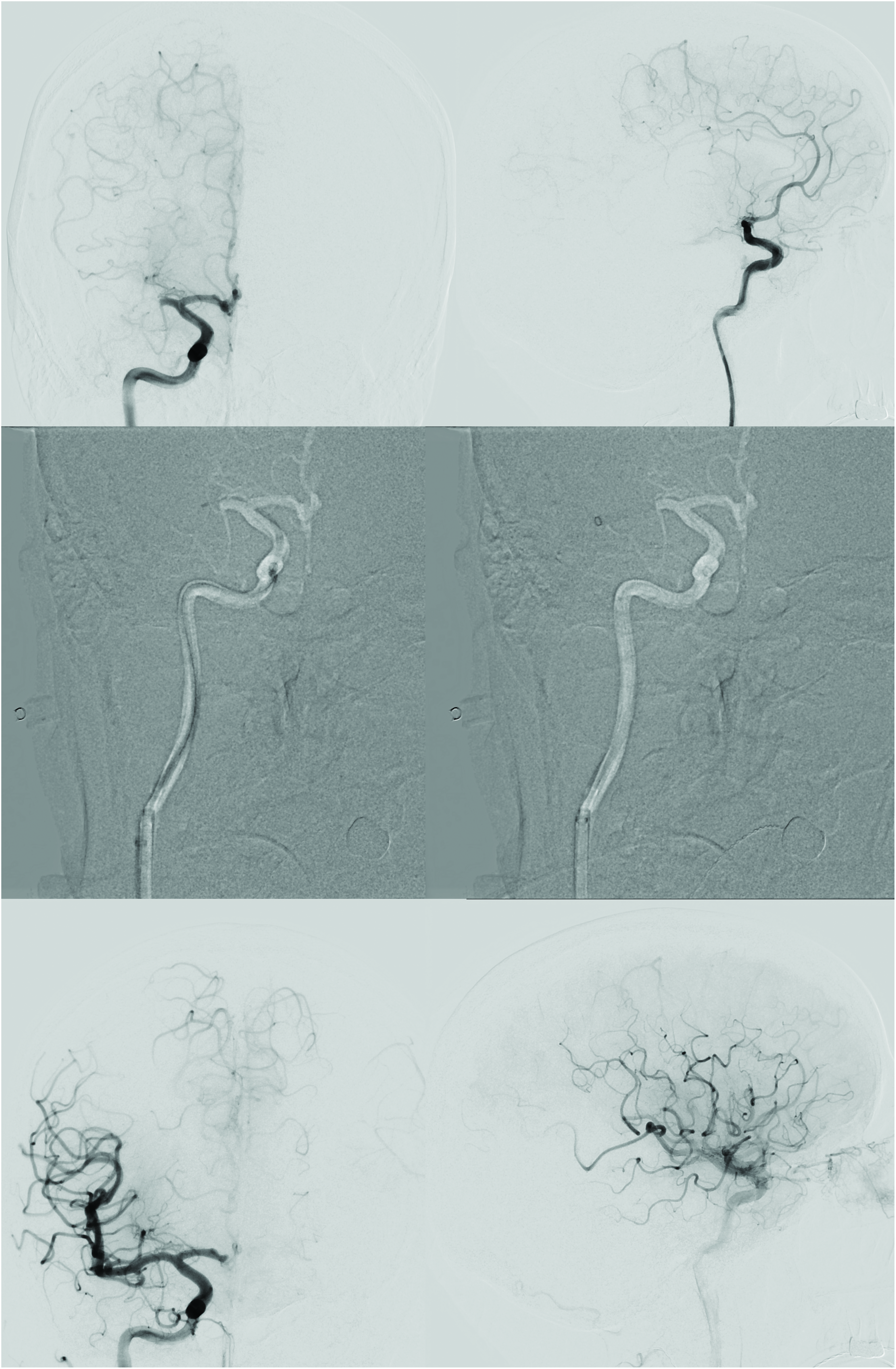
CAMT performed in a patient with right M1 occlusion seen on (a) frontal and (b) lateral projection angiography. (c) Frontal and (b) lateral stored roadmap images demonstrate the tip of the Tenzing 8 device (white arrowhead) just beyond the angiographic limit of contrast (black arrowhead). (e) Frontal and (f) lateral stored roadmap images following removal of the Tenzing device demonstrate the FreeClimb 88 catheter after it has passively moved downstream with its tip (white arrowhead) beyond the angiographic limit of contrast (black arrowhead), facilitated by passive from the plunger effect from Tenzing removal. Video of the stored fluoroscopy from this technique is provided in Supplemental Video 1. (g) Frontal and (h) lateral spot films over the head demonstrate the FreeClimb 88 catheter. (i) Frontal and (j) lateral angiograms following one pass of CAMT demonstrate mTICI 3 recanalization, confirming FPE. Note faint opacification of the anterior cerebral artery compared to initial angiography due to competitive flow from the contralateral ICA across the anterior communicating artery.
Statistical analyses
Descriptive statistics were used to report patient demographic and clinical characteristics in the included patients. Univariable analysis was performed with Fisher's exact test for dichotomous predictor variables and the Fisher–Freeman–Halton test for predictor variables with three or more measures to assess association of these variables with TICI 2c/3 recanalization, FPE, inability to deliver the FreeClimb 88 to the targeted vessel, or procedural complication. To identify predictors for each of these outcome variables, mixed effects logistic regression was performed, eliminating any confounders with p > 0.20 in univariable analysis account for possible residual confounding. 23 Analysis was conducted using R version 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
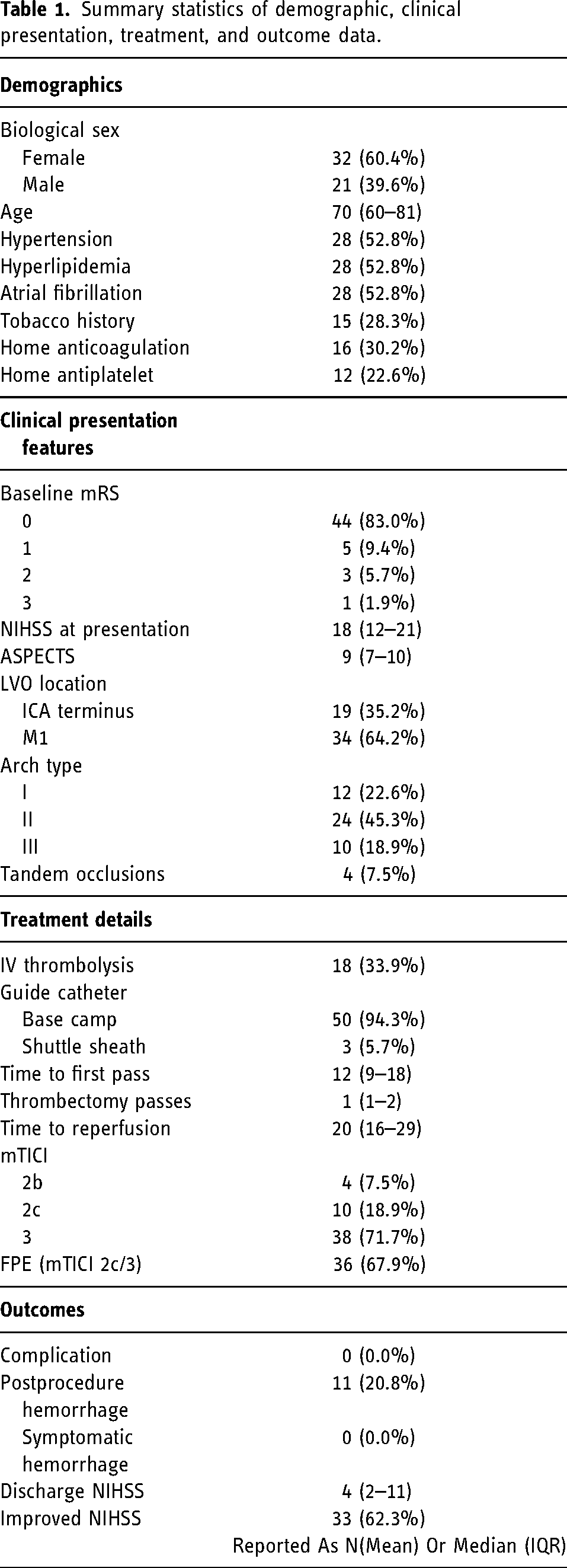
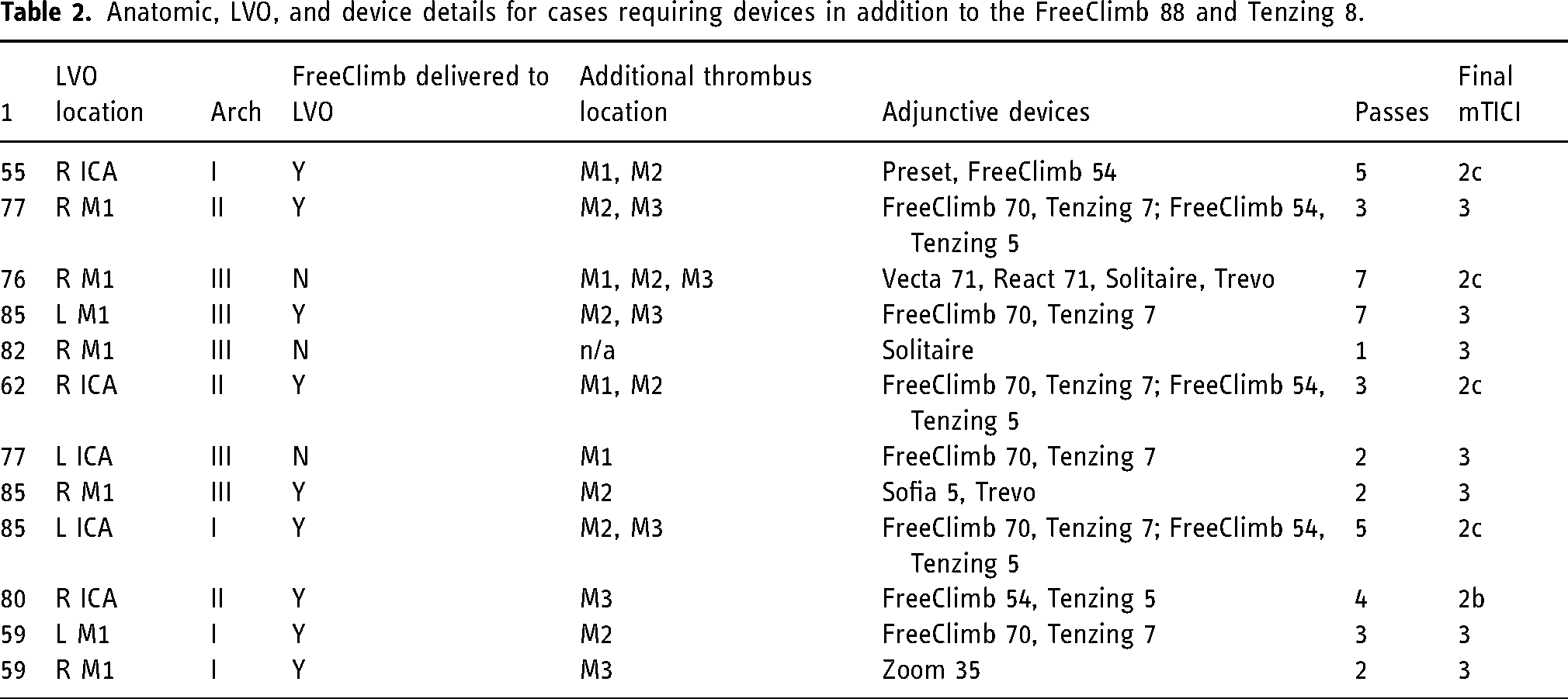
Fifty-three consecutive patients underwent first-line CAMT using the FreeClimb 88 and Tenzing 8 catheter system at eight different institutions during the study period. Table 1 summarizes demographic, procedural, and outcome characteristics of the study cohort. Median age was 71 years (IQR 59–81). 32 patients were female (60.4%). The median presenting NIHSS and ASPECTS were 18 (IQR 12–21) and 9 (IQR 7–10), respectively. Baseline mRS was 0 in 44 patients (83.0%), 2 in 5 (9.4%), 2 in 3 (5.7%), and 3 in 1 (1.9%). Tandem occlusions were present in 4 patients (7.5%). Eighteen (34.0%) patients received IV thrombolysis. Using Tenzing 8, the Freeclimb 88 catheter was successfully delivered to the target LVO in 50/53 (94.3%) patients. A microwire was required to avoid arterial branches in 11/53 patients (20.8%); 1/53 (1.9%) patient required a stent-retriever to deliver the FreeClimb 88 to the targeted vessel. Median time from groin puncture to first pass was 12 (IQR 9–17) minutes. Median time from groin puncture to recanalization was 1915–29 minutes. Modified Thrombolysis in Cerebral Ischemia 2c/3 was achieved in 49/53 (92.5%) patients, including the 3 (5.7%) in which FreeClimb 88 was not successfully delivered to the target vessel. Modified Thrombolysis in Cerebral Ischemia ≥ 2B was achieved in all 53 patients. Of those in which the FreeClimb 88 was successfully delivered to the LVO, mTICI 2c/3 was achieved in 47 (94.0%), with mTICI 2c/3 FPE achieved in 36 (72.0%) cases. Modified Thrombolysis in Cerebral Ischemia 2c/3 FPE was achieved in 36/53 (67.9%) among all patients. Adjunctive devices were needed to perform thrombectomy for residual distal occlusions in 9/53 (17.0%) patients. Embolization to new territory was not identified in any case. Details of adjunctive devices and cases with distal occlusions are provided in Table 2. Among cases in which a microwire was used to deliver the Free Climb 88 over the Tenzing 8, the wire was advanced beyond the angiographic limit of contrast in 3/11 (27.3%). Among cases during which the Free Climb 88 was successfully delivered to the target vessel, the Tenzing 8 device crossed the angiographic limit of contrast in 18/50 (36.0%). There were no adverse events or postprocedural symptomatic hemorrhages. In multivariable analysis, the use of adjunctive devices was associated with lower rates of FPE (OR = 0.12, p = 0.031). This was the only statistically significant finding among multivariable models prospectively planned prior to analysis; no statistically significant associations were identified for TICI 2c/3 recanalization, inability to deliver the FreeClimb 88 and Tenzing 8 to the targeted vessel, or complications.
Summary statistics of demographic, clinical presentation, treatment, and outcome data.
Anatomic, LVO, and device details for cases requiring devices in addition to the FreeClimb 88 and Tenzing 8.
Discussion
This early experience demonstrated consistent rapid and effective access to LVOs in the ICA and M1 to perform CAMT using the Tenzing 8 with FreeClimb 88 catheter with no procedure-related complications. Using the Tenzing delivery catheter in CAMT significantly reduces the ledge between the inner delivery device and outer aspiration catheter, likely reducing the tracking force necessary to advance an aspiration catheter.15,16,24,25 This is especially important with increasing caliber of aspiration catheters, which can catch on branch artery origins or experience increased wall friction in tortuous anatomy. The Tenzing delivery catheter provides a robust rail for aspiration catheter delivery by virtue of its caliber, mechanical properties, and central position in the vessel lumen. In an in vitro study, Tenzing was capable of delivering aspiration catheters to the proximal M1 segment in half the time compared to a leading microwire and microcatheter combination. 15 Another potential advantage of the Tenzing is that it may facilitate avoidance of crossing and potentially fragmenting the clot. 26 Additionally, once at the face of the clot, the FreeClimb 88 catheter is advances passively due to a plunger effect created by vacuum from removal of the Tenzing device from the aspiration catheter lumen; this initiates ingestion of the thrombus by the catheter tip (Supplemental Videos). 19
In the present study, the median (IQR) time from groin puncture to first pass was 129–16 minutes. The median (IQR) time from groin puncture to reperfusion12,9–17 minutes is faster than previous reports using 0.070–0.074″ ID large bore aspiration catheters delivered with microcatheters or using a stent-retriever as an anchor and rail.27–35 Previous studies have shown the Tenzing delivery catheter is highly effective for tracking large (0.070–0.074″) as well as “super large” (0.088″) bore aspiration catheters to an intracranial LVO.14,16,18,30 In a prospective trial, Caldwell et al. reported Tenzing 8 facilitated delivery of a HiPoint 88 catheter (Route 92 Medical, San Mateo, CA). 18 The HiPoint 88 catheter-on-a-wire is composed of a distal catheter segment with the same dimensions as the distal portion of the FreeClimb 88, with the catheter connected to a wire to serve as its proximal end. In all 20 (100%) cases in their study in which the Tenzing 8 delivery catheter was used with the HiPoint 88 catheter, the catheter was successfully delivered to the target occlusions in the ICA and M1. 18 Caldwell et al. reported a FPE mTICI ≥2C of 55%, which is less than the rate (68%) reported in this series. 18 In the first-in-human HiPoint 88 experience, 25% of cases required adjunctive devices to recanalize more distal occlusions to improve final reperfusion, compared to 17.0% in this present series. 18 In another multicenter study by Massari et al., a Tenzing 8 was used to successfully deliver HiPoint 88 in 33/33 (100%) consecutive patients with 34 LVOs (17 M1, 17 ICA). 19 In addition, 93% of cases required only one thrombectomy pass with a FPE for mTICI ≥2C-3 rate of 86%. 19 In a previous study of the smaller Tenzing 7 and FreeClimb 70 system for aspiration thrombectomy, the FPE mTICI 2C-3 was 55% for ICA and M1 LVOs. 16 In the current study, rapid groin puncture to mTICI ≥2B recanalization was achieved (19 min), which is in line with and faster than previous HiPoint 088 studies from Caldwell et al. (26 min) and Massari et al. (20 min).18,19 The median time from groin puncture to clot contact with the FreeClimb 88 catheter system was 12 min (IQR 9–17), similar to that seen in Massari et al., 14 min (6–31 min). 19 Compared to results in early reports of CAMT use with the Zoom 88 catheter, FPE mTICI ≥2C rates were superior with FreeClimb 88 and Tenzing 8 (68% vs. 40%). 11 Compared to preliminary results of The Imperative Trial, Zoom 88 had lower rates of successful delivery to the clot face (55.8% vs. 94.3%), higher rates of stentriever use to achieve successful recanalization (5.5% vs. 1.9%), and higher rates of complication (1.2% vs. 0%) compared to FreeClimb 88 in the present cohort. 36
Several studies comparing larger aspiration catheters to those with a smaller bore have shown improved outcomes, shorter procedure times, and lower likelihood of needing additional devices with larger ID, with no impact on complication rates.7,36 This relates not only to increased suction force at the clot with larger ID but also increased aspiration flow rate with decreasing catheter size to vessel diameter ratio. 8 In the ASTER and COMPASS trials, the first-line CAMT cohorts used older generation 0.064–0.068″ aspiration catheters.1,2 Comparative efficacy studies of first-line CAMT with SLBC to first-line SR technique would be of interest. Furthermore, comparative studies between SR technique and CAMT technique using ledge-reducing delivery catheters, such as Tenzing 8, are also lacking.
It is important that operators using an aspiration catheter of this size for CAMT that in patients with significant intracranial atherosclerotic disease or native diminutive arterial caliber, caution should be used to avoid arterial injury. Smaller caliber devices should be considered in such circumstances. The outer diameter of the FreeClimb 88 is 2.6 mm (0.101 inch). This is appropriately sized for most ICA terminus calibers and M1 segments, which tapers with a typical range of diameter from 2.4 to 3.1 mm; the size of this catheter allows for a higher catheter-to-vessel ratio.8,11,37 The angle of interaction between the aspiration catheter and the clot has also been found to affect the efficacy of CAMT. 38 Moreover, in some cases utilizing CAMT as a first-line approach, the combination of SR and aspiration catheter may be necessary to retrieve emboli that are resistant to initial direct aspiration passes. The low number of passes, high FPE, and infrequent use of adjunctive devices in this current study suggest that Tenzing 8/FreeClimb 88 CAMT may offer cost savings compared to other approaches or devices. Further investigation into cost impacts would on thrombectomy procedures going forward will be of interest.
This study is limited by its modest number of patients included in the early release period for these paired devices. Lack of a control group and its retrospective design are also limitations. Additionally, there was no independent core lab adjudication of angiographic results. Since most patients were recently treated, longer term follow-up data are lacking. Larger scale studies are needed to corroborate these initial findings and detect potential complications of using Tenzing 8 and FreeClimb 88 catheters.
Conclusions
In this early experience with the Tenzing 8 and FreeClimb 88 catheters, delivery to the M1 and ICA LVOs to perform CAMT was achieved in 94% of cases, with infrequent need for use of adjunctive devices for delivery to the LVO. This delivery catheter and aspiration catheter combination permitted rapid access to LVOs with better reperfusion performance than seen with CAMT using existing SLBCs without procedural complications. Larger studies are needed to further assess the efficacy and safety of this technology.
Supplemental Material
Supplemental Material
Footnotes
Author contributions
Concept and design (FS, MDA, JDE), analysis and interpretation (MDA, FS, JDE), data collection (all authors), writing the article (MDA, FS), critical revision of the article (MDA, FS, JC, SL, WTK, JDE), final approval of the article (all authors), statistical analysis (MDA, FS), and overall responsibility (MDA, FS, JDE).
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MDA: Consultant fees, Route 92 Medical. Stock or stock options, Certus Critical Care, Route 92 Medical, Piraeus Medical. JC: Consultant fees and travel/meeting Support, Route 92 Medical. SL: Consultant fees and travel/meeting Support, Route 92 Medical. WTK: Consultant fees, Stryker Neurovascular; Consultant fees, Travel reimbursements, and Stock Options, Route 92 Medical. JDE: Consultant fees, Stryker Neurovascular; Consultant fees, Travel reimbursements, and Stock Options, Route 92 Medical, Co-founder and Chief Medical Officer, Route 92 Medical. JAG: Consultant fees, Imperative Care, Route 92, Cognition; Grant Support, Emory Medical Care Foundation, Neurosurgery Catalyst, Department of Defense-Surgical Critical Care Initiative, Georgia Research Alliance. DT: Consultant fees Route 92, Scientia; Speaker fees, IRRAS. RP: Consultant fees, Stryker, Medtronic, Route 92 Medical; Grant Support, Phenox. FS: Consultant fees, Stryker Neurovascular and Route 92 Medical; Honoraria for lectures, Stryker Neurovascular; Travel, Medtronic; Research Grants: Microvention, Stryker. Stock or Stock Options: Route 92 Medical
Ethics statement
All data were deidentified and unlinked to any identifiers. The pseudonymized data of each subject were collated by one author for statistical analysis. The institutional review board of each participating center approved the study and waived the need for patient consent given the retrospective study design.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.