
Abstract
Purpose
The contour neurovascular system (CNS) is an intrasaccular flow-disrupting device designed for the treatment of intracranial wide-necked bifurcation aneurysms. Metal artifacts limit magnetic resonance imaging (MRI) accessibility after implantation. The purpose of this in vitro study was to evaluate non-invasive imaging alternatives to digital subtraction angiography (DSA).
Material and methods
Three aneurysms of patients originally treated with CNS were three-dimensional (3D)-printed (one at the basilar tip and two at the middle cerebral artery bifurcation). CNS devices were implanted under fluoroscopic control into the 3D models. Post-implantation two-dimensional-DSA, flat panel computed tomography angiography (CTA), MRI, and spectral CTA were performed.
Results
Time of flight angiography and T1 weighted sequences showed large susceptibility artifacts at the detachment zone of the devices. A thin-sliced T2 weighted sequence in cross-sectional orientation to the aneurysm allowed visualization of the aneurysm dome, but the aneurysm neck and parent vessel could not be assessed. Focused spectral CTA, especially a 40 keV reconstruction with a metal artifact reduction algorithm (orthopedic metal artifact reduction (OMAR)), showed only minor artifacts at the detachment zone. This approach achieved a very similar result to DSA and flat panel computed tomography, enabling the assessment of the device structure, aneurysm perfusion, and parent vessel perfusion.
Discussion and conclusion
For non-invasive follow-up of CNS, focused 40 keV CTA with OMAR seems to be a valuable option. MRI can be valuable for larger aneurysms to assess the aneurysm dome, but was not suitable for evaluating the parent vessels and aneurysm neck after CNS implantation in this study.
Background
The contour neurovascular system (CNS)
The CNS (Stryker, USA) is an intrasaccular flow-disrupting device for the treatment of intracranial wide-neck bifurcation aneurysms. By the end of 2019, Akhunbay-Fudge et al. 1 published a case series of 11 patients treated with this system. Since then, more publications have followed, including a small prospective multicentric trial analyzing the safety and effectiveness of the device.2–7
The sizing of the CNS requires an assessment of the aneurysm's neck and base width/depth, whereas the height and dome morphology only need to be considered in very shallow aneurysms. The CNS should be placed in the aneurysm base within the equatorial plane. The aneurysm neck should be completely covered, and the detachment marker is supposed to be in the parent vessel, outside the aneurysm. The CNS can be fully re-sheathed. The device can be detached electrolytically.
Purpose of this study
Besides the gold standard digital subtraction angiography (DSA), magnetic resonance imaging (MRI) is a valuable non-invasive alternative for follow-up examinations of endovascularly treated aneurysms. 8 The purpose of these examinations is to detect early aneurysm recanalization or regrowth, as well as narrowing of the parent vessels by secondary intimal hyperplasia, thrombus, or the implanted devices themselves. After CNS treatment of the first patients, difficulties with MRI follow-up examinations were noticed. Severe susceptibility artifacts at the region of the radiopaque marker of the CNS complicated the assessability of the treated aneurysms. Comparable findings were described by Akhunbay-Fudge et al. 1 before. This experimental in vitro analysis was set up to evaluate alternative non-invasive imaging options using three-dimensional (3D)-printed aneurysm phantoms.
Material and methods
No consent or ethics approval was needed by local standards because it is an in vitro study.
Aneurysm phantoms
Three patient-derived intracranial aneurysm flow models were produced using a 3D printing technology (Form 3, Formlabs, USA). 9 First, the vessel lumens were segmented from the patient's 3D-rotation angiography datasets using a threshold-based region-growing algorithm 10 followed by marching cubes 11 (MevisLab 3.0.1, MeVis Medical solution, Germany). Next, the resulting lumens were optimized for 3D printing by cutting the branches smaller than 1 mm in diameter (Meshmixer 3.5, Autodesk, USA). At last, an outer layer was added to form a vessel wall (3 mm), and flow connectors (Fusion 360 2.0, Autodesk, USA) were added to integrate the models in a flow loop.
Implanting CNS in the aneurysm phantoms using DSA
The phantoms were connected to silicon pipes. A short 6F-sheath (Terumo, Japan) was used as an access to the system. Circulation was maintained by a roller pump (Ismaltec MCP Standart, Cole Parmer, USA). Physiological saline solution was used as fluid. A 3D-rotation-angiogram was made by manual injection of 20 ml iodine contrast (Imeron 300, Bracco Imaging, Italy) under fluoroscopy (Allura Xpert FD, Philips, The Netherlands). A microcatheter (Headway 27, Microvention, USA) was placed into the aneurysm, for additional stabilization an intermediate catheter was used (SOFIA EX 5F, Microvention, USA). According to the manufacturer’s recommendation, 1 suitable sized devices (CNS 7 mm, 9 mm, and 11 mm) were deployed inside the aneurysm models. By pulling back the microcatheter, the device was placed in the neck and base of the aneurysm, and a wine-glass-like configuration was achieved. For ensuring that there is adequate wall apposition and device stability a manual test was performed by pushing the wire slightly. In case of a device movement CNS was repositioned. The proximal marker was placed in the parent vessel to avoid residual basal perfusion. Unlike in a patient, an additional microwire (Transend, Boston Scientific, USA), which touched the CNS, was needed to release the CNS due to low conductivity in the model. The plus electrode was attached to the pusher wire of the device, and the minus electrode to the microwire. CNS was detached using a Solitaire Detachment Device (ev3 Neurovascular/Medtronic, USA). After detachment, two-dimensional (2D) and flat panel angiograms were made.
MRI imaging protocol and experimental setup
Prior to the MRI examination, the phantoms were embedded in an agarose solution (3% by volume). The glycerol–water mixture was used as blood-mimicking fluid. The phantoms were placed in a head coil (32 channels) in 3 Tesla MRI (Ingenia, Philips, The Netherlands).
The MRI protocol comprises the following sequences:
Time of flight (TOF) angiography, gradient echo, echo time (TE)/repetition time (TR) 5.76/25 ms, matrix 800 × 407, field of view (FOV) 200 × 200 × 74 mm3, voxel size 0.23 × 0.23 × 0.5 mm3, acquisition time 4:05 min:s. T2 weighted (T2w) sequence, spin echo, TE/TR 100/3436, matrix 400 × 226, FOV 220 × 175 × 33 mm3, voxel size 0.43 × 0.43 × 1 mm3, acquisition time 3:40 min:s. T1 weighted (T1w) sequence, spin echo, TE/TR 3/144, matrix 400 × 255, FOV 220 × 175 × 26 mm, voxel size 0.43 × 0.43 × 1.5 mm3, acquisition time 3:41 min:s. T1 weighted Dixon sequence (T1dixon), spin echo, TE/TR 6/0, matrix 132 × 150, FOV 120 × 151 × 55 mm3, voxel size 0.43 × 0.43 × 0.46 mm3, acquisition time 2:39 min:s.
To distinguish the signal voids caused by the blood suppressing from the signal void arising due to the metal artifacts, T2w sequence was acquired without flowing fluid (the pump was turned off).
Computed tomography (CT) protocol and experimental setup
The phantoms were filled with iodine contrast (Imeron 300, Bracco Imaging, Italy) solution 10% by volume and sealed. The attenuation was conformed to clinical CT angiography. The phantoms were placed into a clay vase with a wall thickness of 10 mm filled with sacharid solution (97 g sacharid/l) to match the attenuation of the skull and brain parenchyma. Spectral CT was performed (iQon, Philips, The Netherlands): 80 mAs, 120 kV, spiral, pitch 1.046, scan time 1.4 s, scan length 40 mm, volume computed tomography dose index (CTDIvol) 7.2 mGy, dose length product 68.4 mGy*cm.
Data analysis
CT, MRI, and DSA images were rated by the authors. The aneurysm dome, aneurysm neck, and parent vessel were assessed. The results were categorized as completely, partially, and not assessable. Disagreements were solved by consensus.
Results
Three different aneurysm models were successfully 3D-printed. The correct morphology and measures of the aneurysms were verified by DSA pre-implant. The aneurysm dimensions and corresponding sizes of contour devices are summarized in Table 1. All three CNS were successfully implanted. Post-implant 2D DSA and flat panel CT were made (Figure 1). The aneurysm dome, aneurysm neck, and parent vessel could be assessed completely.
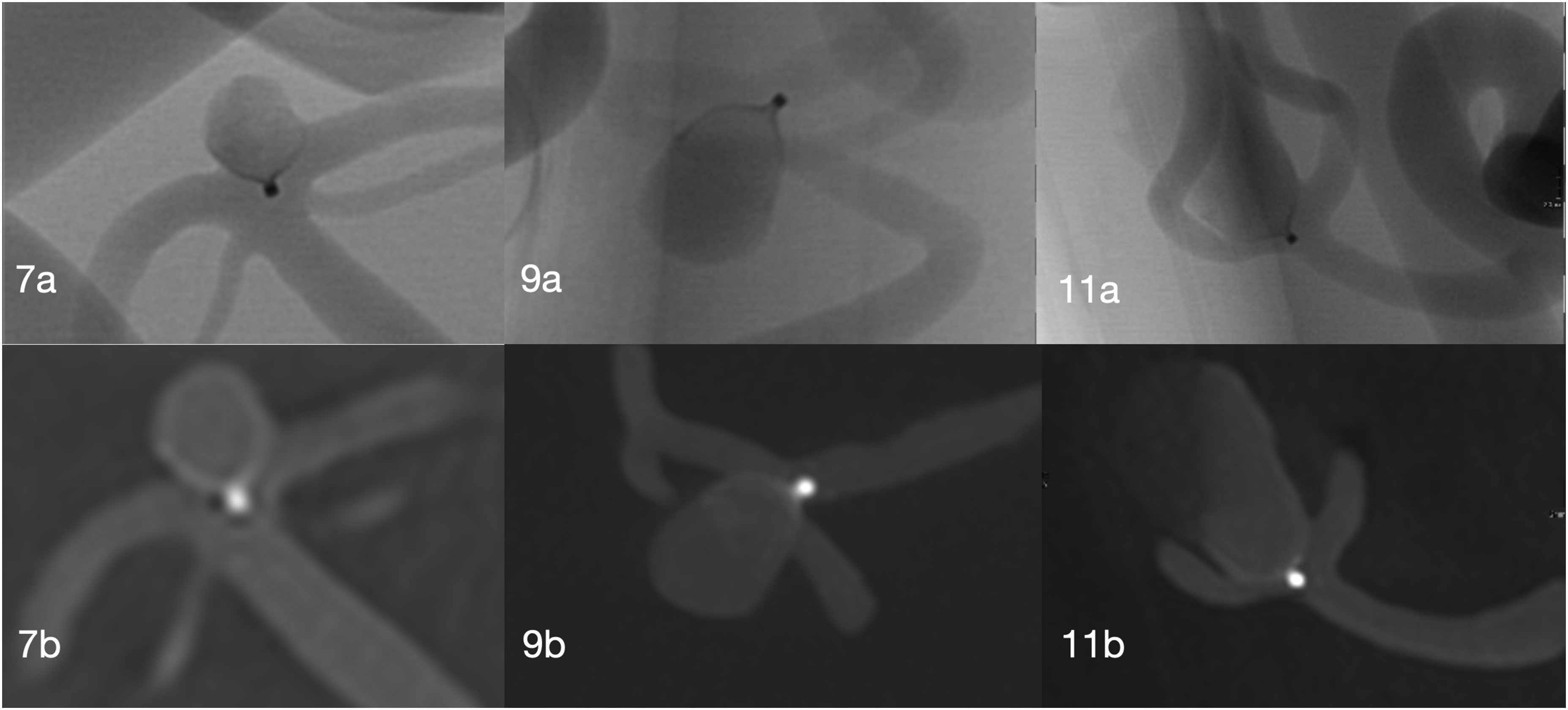
2D DSA (a) and flat panel CT (b). Basilary tip aneurysm with 7 mm Contour Neurovascular System (7a, 7b); MCA bifurcation aneurysm with 9 mm contour neurovascular system (9a, 9b), MCA bifurcation aneurysm with 11 mm contour neurovascular system (11a, 11b).
The specification of aneurysms and corresponding implanted contour devices.

MCA: middle cerebral artery.
Magnetic resonance imaging
In all sequences, significant artifacts at the radiopaque marker could be found. In the TOF-angiography (Figure 2: 7a, 9a, and 11a) the aneurysm dome could be partially assessed in the 7 mm CNS Aneurysm, and completely in the 9 and 11 mm CNS aneurysms. The parent vessel and aneurysm neck could not be assessed in any aneurysm (Table 2).
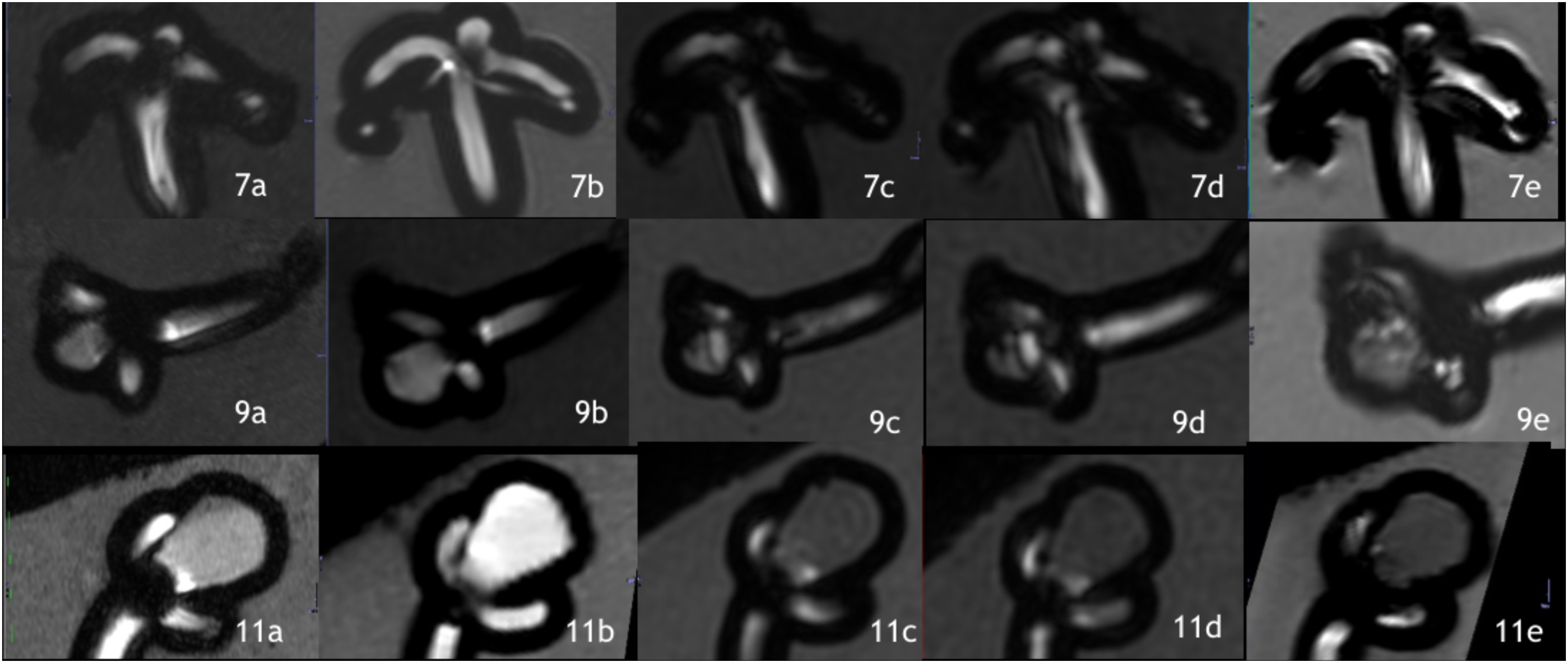
Magnetic resonance imaging (MRI) of aneurysm models with implanted 7 mm, 9 mm, and 11 mm contour endovascular systems. 7a, 9a, 11a: Time of flight angiography (gradient echo). 7b, 9b, 11b: T2 weighted sequence (spin echo). 7c, 9c, 11c: T1 weighted Dixon sequence with fat saturation (spin echo). 7d, 9d, 11d: T1 weighted Dixon sequence no fat saturation (spin echo). 7e, 9e, 11e: T1 weighted sequence (spin echo).
Assessibility of the aneurysm and parent vessel in MRI, spectral CT, and DSA after implantation of contour neurovascular system.
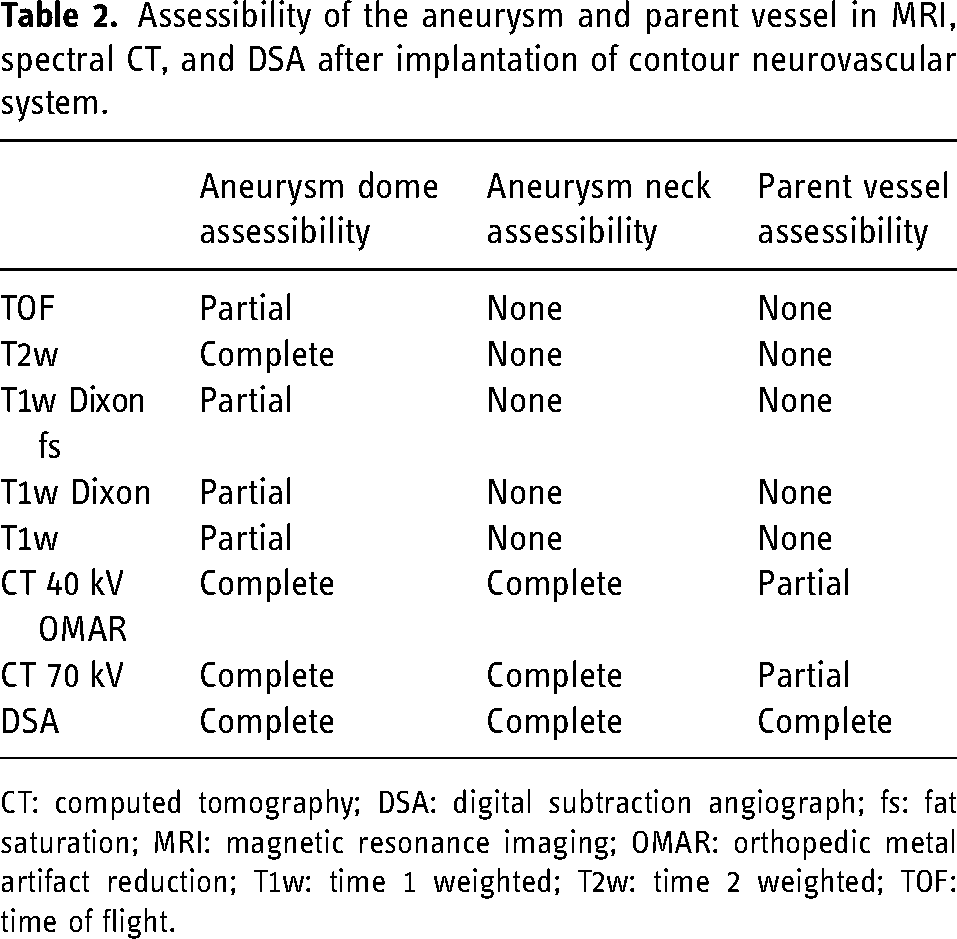
CT: computed tomography; DSA: digital subtraction angiograph; fs: fat saturation; MRI: magnetic resonance imaging; OMAR: orthopedic metal artifact reduction; T1w: time 1 weighted; T2w: time 2 weighted; TOF: time of flight.
T1 weighted sequences (both Dixon and conventional spin echo) were similar artifact prone such as the TOF-angiography: The aneurysm dome could be assessed in the 11 mm CNS aneurysm, but only partially in the smaller aneurysms. Both the aneurysm neck and the parent vessel could not be assessed.
The least susceptibility artifacts were found using the T2 weighted sequence (Figure 2: 7b, 9b, and 11b): The aneurysm dome was completely assessable in all aneurysms, the aneurysm neck could be assessed partially, the parent vessel could not be assessed (Table 2).
Spectral CT
Using the Philips Intellispace Portal (Philips, The Netherlands) different monoenergetic reconstructions were acquired with and without orthopedic metal artifact reduction (OMAR). The best results (authors` consensus) could be achieved at 40 kV with OMAR. OMAR leads to a less blurry appearance of the device. The radiopaque marker caused only minor artifacts. Additionally, a conventional 70 kV—a standard energy CT angiography (CTA) was performed—reconstruction was made, which also showed good results. At 40 and 70 kV, the aneurysm dome and neck could be completely assessed, the parent vessel partially.
Discussion
DSA is the gold standard imaging modality for follow-up examinations after endovascular aneurysm treatment. It offers high sensitivity and specificity, but it is an invasive procedure. In many endovascular centers, repetitive follow-ups after intracranial aneurysm treatment are done by MRI. For the CNS strong MRI metal artifacts from the device detachment zone were described in the literature and observed in daily practice. 1 In this study, different imaging modalities were compared in 3D-printed aneurysm models to identify non-invasive alternatives to DSA. Different MRI sequences showed strong artifacts caused by the proximal marker of the CNS—most severe when T1 weighted—and reducing the assessability of the treated aneurysms. However, spectral CTA revealed to be very precise in the delineation of the treated aneurysm models, the implanted CNS devices, and the parent arteries.
A prospective study from 2012 showed an inter-modality agreement of magnetic resonance angiography (MRA) with DSA of 0.51 at 3 T and 0.47 at 1.5 T. 12 Evaluating flow-diverting stents in MRI, especially the stent lumen, remains difficult with MRA regardless of the sequence used. 13 Regarding Woven EndoBridge (WEB) treated aneurysms, a clinical study showed that contrast-enhanced-MRA and TOF-MRA have low sensitivity for aneurysm remnant detection and concluded that DSA remains the gold standard for follow-up. 14 CTA proved to be a reliable technique for the follow-up of aneurysms treated with the WEB device, high agreement with DSA findings could be shown. 15 It was described that metal reduction algorithms significantly reduced metal artifacts from intracranial aneurysm coiling and improved visualization of anatomical structures and arteries around the coil, and depiction of the status of coiled aneurysms on post-interventional cerebral CT. 16 In another study using metal artifact reduction in patients with predominately clipped aneurysms, the degree of the streak artifacts and surrounding vessel depiction were not significantly improved compared with conventional CTA. 17 Acquisition of monochromatic images using spectral CT and metal artifact reduction software have been shown to reduce metal artifacts with preserved or increased vessel contrast in patients, who underwent coiling of intracranial aneurysms. 18
Akhunbay-Fudge et al. 1 showed an artifact at the detachment zone in the TOF-MRI, which could not be seen in DSA (Figure 3). In this examination, the result of the CNS pilot study could be confirmed: TOF-angiography showed major susceptibility artifacts of 7 mm diameter at the detachment zone, regardless of which CNS size was used. The dome was still possible to assess (Figure 2, 11a), but it depended on the aneurysm size. In small aneurysms, TOF would have no value. In T1w sequences (spin echo), CNS showed even larger artifacts. T2w sequences (spin echo) showed fewer susceptibility artifacts (around 5 mm diameter). Because of the flow voids, it would be possible to detect high-flow reperfusion. Also, aneurysm size monitoring at the region of the dome might be possible. In our 3D models, the signal of the aneurysm wall was hypo-intense and the aneurysm wall was rather thick. Having flow in the model it was not possible to differentiate between flow-void, artifact, and wall. Therefore we made the T2w images with no flow simulating a total aneurysm occlusion.
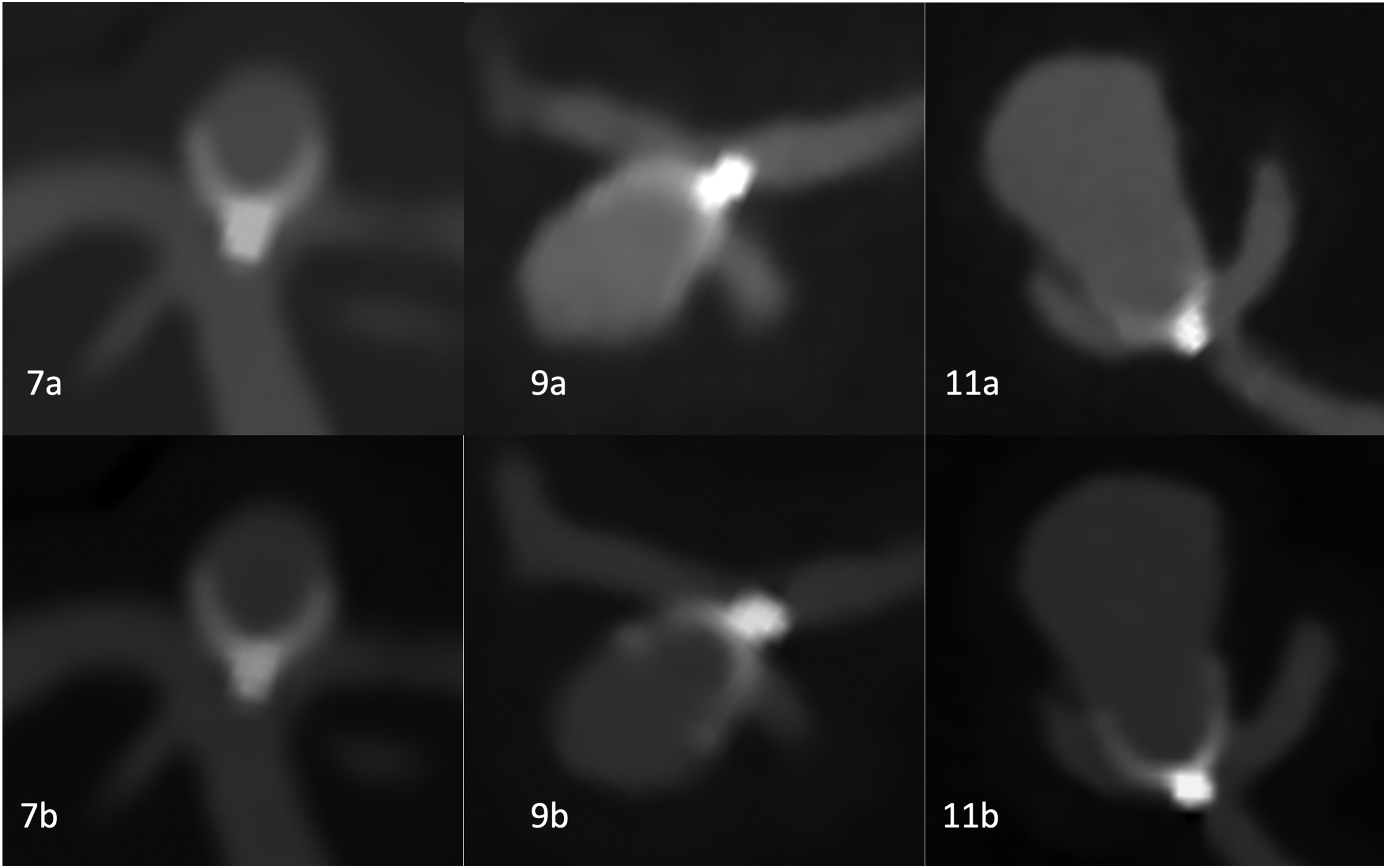
Spectral computed tomography (CT) angiography of aneurysm models with 7 mm, 9 mm, and 11 mm contour neurovascular systems. Both conventional 70 kV scans (a) and 40 kV scans with orthopedic metal artifact reduction reconstruction (a).
CTA (Figure 3) showed results very similar to flat panel CT (Figure 1). Although there were some metal artifacts at the detachment zone of CNS (<1 mm), the results were better than in any MRI sequence used. Adding spectral reconstruction at 40 keV and a metal reduction algorithm, the artifact could be slightly reduced and the contrast-enhanced. The aneurysm base, the shape and alignment of CNS, and the parent vessel could be assessed in very good quality. Despite the slightly worse imaging quality compared to DSA or flat panel CT, CTA might be easier accessible to the majority of patients. New generation spectral and dual-source CT and improved metal artifact reduction algorithms might improve imaging in the future.
We used materials and methods, which are easily reproducible. The models are made publicly available. Such a standardized test stand allows to develop or refine imaging techniques for this intrasaccular device or other devices.
The low number of cases is a limitation of this study: The results cannot be generalized, but the concept could be proved. In further steps larger in vitro studies and clinical studies can follow with an already tailored protocol.
Conclusion
CTA, especially using spectral reconstruction and metal artifact reduction algorithm, seems to be a valuable radiological follow-up option after CNS implantation. MRI can be valuable for larger aneurysms to assess the aneurysm dome (T2w sequence), but is not suitable for evaluating the parent vessels and aneurysm neck after CNS implantation in this study.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics committee or institutional review board approval
By local standards no consent or ethics approval is needed, because it is an in vitro study with no biological material.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.