
Abstract
Although rare, cerebral arterial fenestration may present challenges in diagnosis and treatment. Here we present a case of a supraclinoid internal carotid artery (ICA) fenestration adjacent to an ICA aneurysm, successfully treated with balloon-assisted coil embolization. A female in her 50's presented with an acute subarachnoid hemorrhage from a ruptured left ICA-ophthalmic artery (OA) aneurysm. Digital subtraction angiography revealed a focal ICA fenestration distal to the posterior communicating artery (Pcom). The patient underwent successful coil embolization of the aneurysm using the balloon-assisted technique. No immediate hemorrhagic, thromboembolic, or neurological complications were observed. The patient was discharged in good condition after 2 weeks of hospitalization. A comprehensive literature review of 33 cases was subsequently performed to understand the characteristics of this condition. Cases involving the cranial division of the ICA forming the fenestration exhibited caliber differences significantly more frequently (p = 0.02). Embryological insights revealed distinctions between the cranial divisions of the ICA, influencing fenestration morphology and associated aneurysm formation. Endovascular treatment poses the risk of vascular injury, necessitating the identification of this variation and procedural planning.
Keywords
Introduction
Cerebral arterial fenestration is rare, with an incidence of only 2.1% in the general population, and is notably more common in the posterior circulation. 1 Approximately 90% of cases occur in the basilar artery (BA), vertebral artery, or anterior cerebral artery (ACA), while fenestration of the internal carotid artery (ICA) occurs in only 1.3% of cerebral arterial fenestration cases. Haryu et al. conducted a review of 16 cases of supraclinoid ICA fenestration, categorizing them into three groups 2 : Type A (where the ICA appears to be a duplicate (equal caliber)), type B (where the smaller limb of the fenestration fused to the ICA at the origin of the posterior communicating artery (Pcom)), and Type C (the smaller limb of the fenestration is fused to the Pcom itself or appears as a duplicated Pcom) (Figure 1A–D). It is noteworthy that while some Type C cases exhibit fenestrations extending beyond the Pcom (Figure 1D), ICA fenestrations between the Pcom and anterior choroidal artery (AChA) are not included in this classification (Figure 1E), with only two such cases being reported in the past.3,4
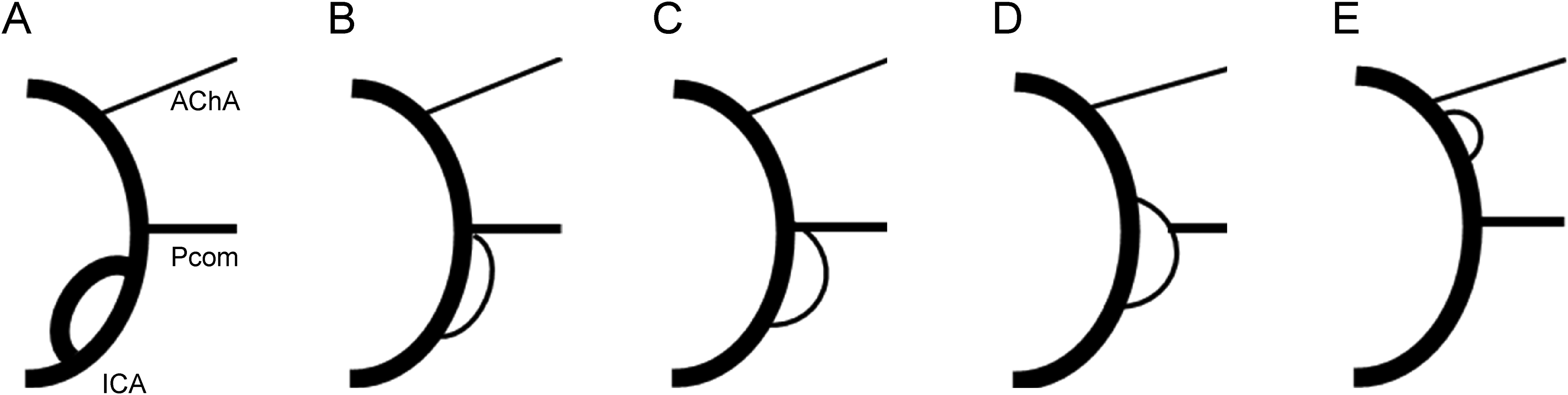
Illustrations depicting the location of the supraclinoid fenestration. A: The internal carotid artery (ICA) appears to be duplicated (equal caliber); B: Smaller limb fenestration fused to the ICA at the origin of the posterior communicating artery (Pcom); C: Smaller limb of fenestration fused to the Pcom itself; D: Smaller limb of fenestration appearing as a duplicated Pcom; E: Fenestration between the Pcom and anterior choroidal artery (AChA). Haryu et al. categorized supraclinoid ICA fenestration into three groups 2 : Type A (A), Type B (B), and Type C (C and D). Cases were assessed based on available images and descriptions in the literature. In this study, we divided the patients into two groups: one comprising the cranial division (cranial division group) (D and E), and the other located in the ICA segment proximal to the Pcom (proximal group) (A-C).
Generally, the etiology of cerebral arterial “fenestration” can be attributed to a lack of fusion of embryologically paired arteries (segmentally unfused arteries), two embryologically different vessels that fuse during development (duplication), or a partial residual of the embryological rete of perforators (extracerebral anastomoses between perforators).2,5 However, the cause of the supraclinoid ICA fenestration remains unclear. Herein, we present a case of a supraclinoid ICA fenestration located between the Pcom and AChA, accompanied by an ICA aneurysm, which was successfully treated with balloon-assisted coil embolization. This case report aims to elucidate the embryology of ICA fenestration based on a literature review and discuss the technical considerations when considering the endovascular treatment of aneurysms associated with this condition.
Case presentation
A female in her 50's was admitted to our hospital with an acute subarachnoid hemorrhage caused by a ruptured left ICA-ophthalmic artery (OA) aneurysm. On arrival, she presented with a Glasgow Coma Scale (GCS) score of 15, and no focal neurological deficits. Digital subtraction angiography revealed a ruptured left ICA-OA aneurysm incorporating the origin of the OA into the neck. Focal fenestration of the left supraclinoid ICA was observed between the Pcom and the AChA (Figure 2). A notable discrepancy in the caliber of the two limbs of the fenestration was observed, with the posterolateral limb being smaller in caliber. The patient was treated with balloon-assisted coil embolization of the ruptured left ICA-OA aneurysm (Figure 3), achieving satisfactory occlusion. A trace residual flow was noted at the proximal neck of the aneurysm at the site of origin of the OA, with flow preserved along the OA. Baseline postprocedural magnetic resonance imaging showed no thromboembolic complications. The patient was prescribed 81 mg of aspirin for 3 months following the procedure, and was discharged in good condition after 2 weeks of hospitalization, with no neurological deficits.
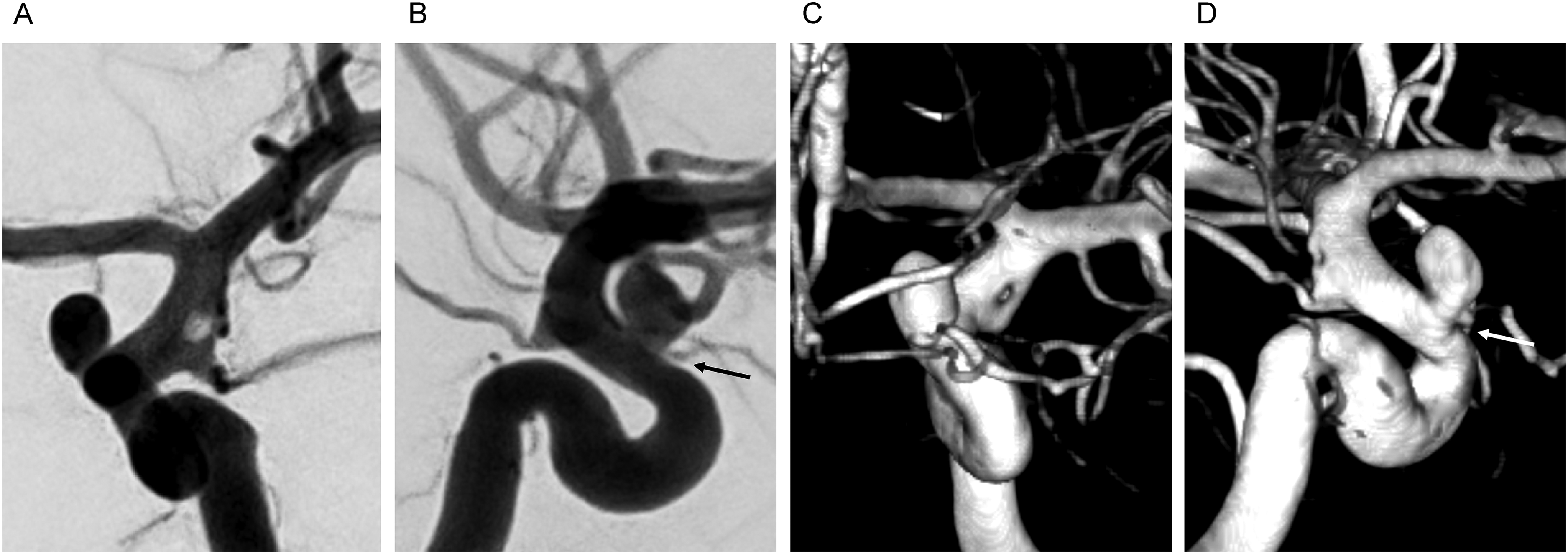
Digital subtraction angiography (DSA) with 3D reconstruction, antero-posterior (A, C), and lateral (B, D) views, demonstrating focal fenestration of the supraclinoid internal carotid artery (ICA), distal to the posterior communicating artery (Pcom), and proximal to the anterior choroidal artery (AChA) origin. The disparity in the caliber of the fenestrated vascular limbs is notable, with the posterolateral limb being smaller in caliber. The ruptured ICA-ophthalmic artery (OA) aneurysm is located distant to the fenestrated ICA segment. The OA (arrow) is incorporated into the neck of the aneurysm.
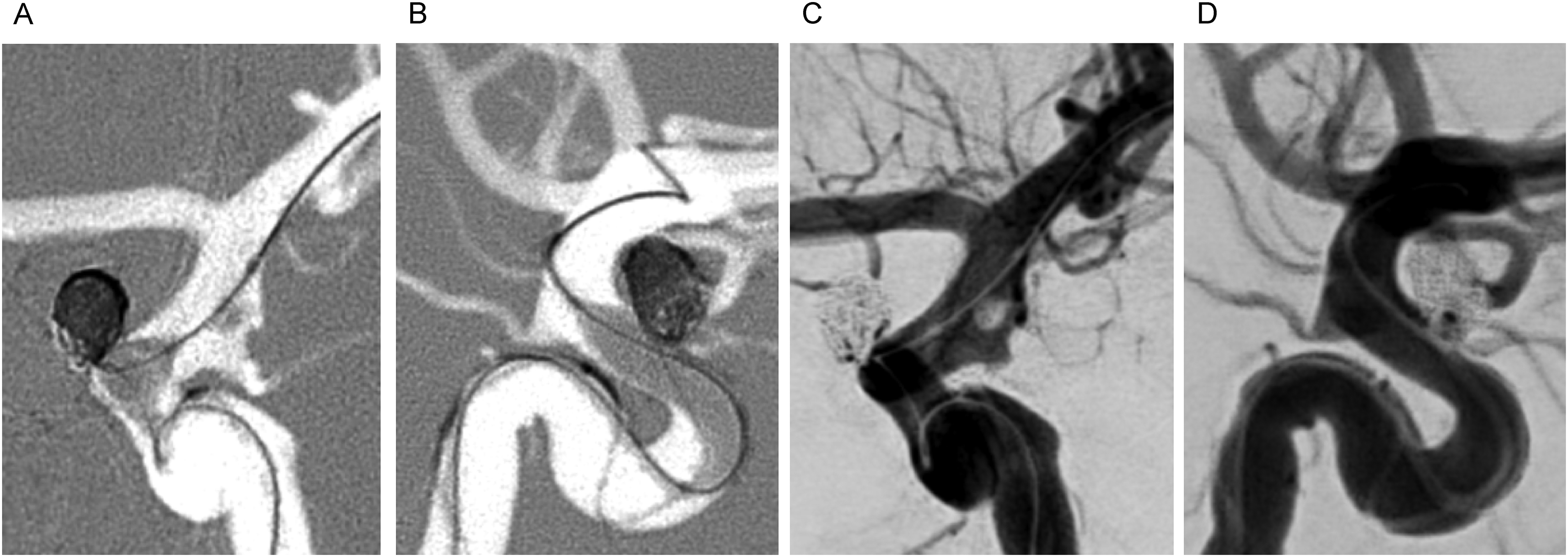
Digital subtraction angiography (DSA), antero-posterior (A, C) and lateral (B, D) views of the balloon-assisted coil embolization of the ruptured ICA-ophthalmic artery (OA) aneurysm. The balloon is positioned and inflated over the aneurysm neck, carefully sparing the fenestrated segment, with a micro guidewire through the larger fenestrated limb. Post-embolization angiogram (C, D) demonstrating near complete occlusion of the aneurysm, with flow in the OA preserved.
Literature review
Table 1 summarizes the characteristics of 33 reported cases of supraclinoid ICA fenestration, including the current case and 32 additional cases identified by a literature review conducted via PubMed, using search terms including “internal carotid artery,” “posterior communicating artery,” and “fenestration.” One case was excluded because it was classified as having a duplicate origin of the Pcom. Cases were assessed based on available images and descriptions in the literature. Furthermore, considering the embryological distinction between the ICA beyond the Pcom, which originates from the cranial division of the ICA, and that proximal to the Pcom of the ICA 33 , the cases were divided into two groups: one comprising the cranial division (cranial division group) (Figure 1D and E) and the other located in the ICA segment proximal to the Pcom (proximal group) (Figure 1A–C).
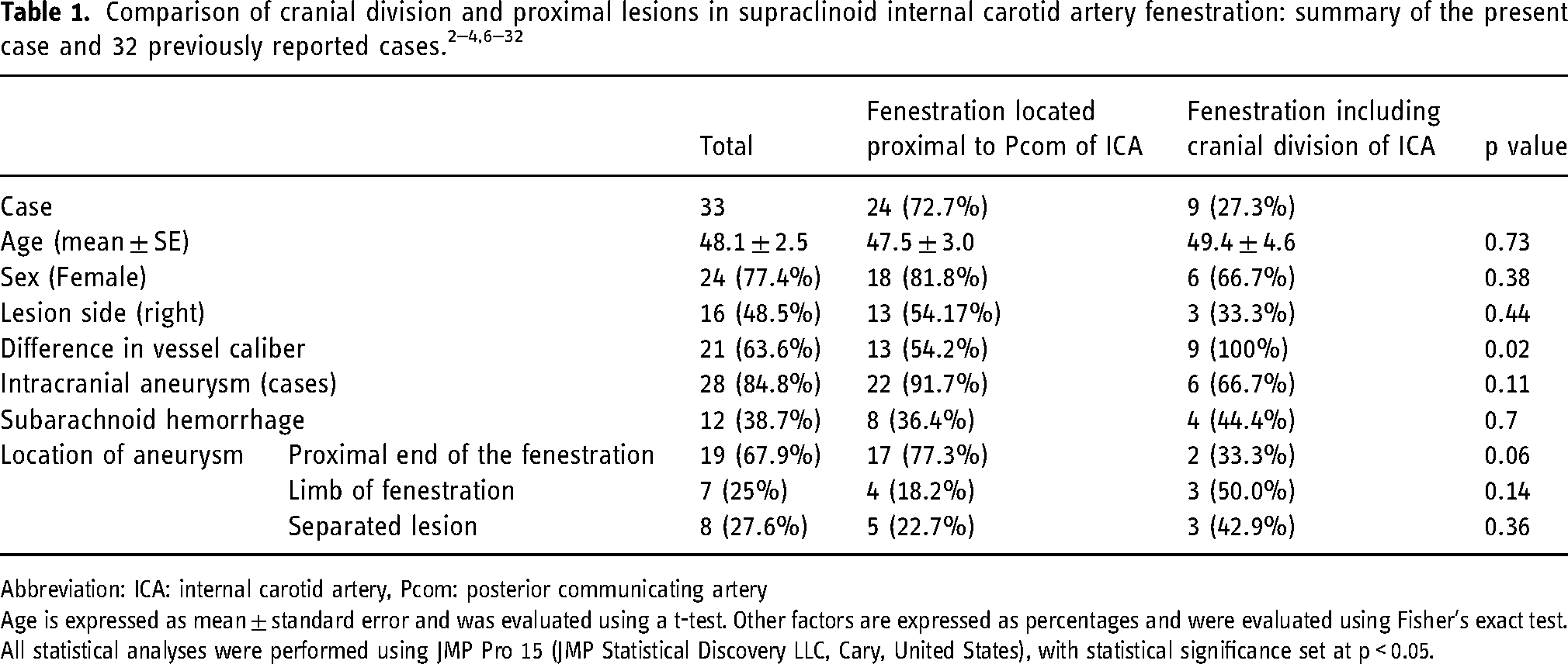
Abbreviation: ICA: internal carotid artery, Pcom: posterior communicating artery
Age is expressed as mean ± standard error and was evaluated using a t-test. Other factors are expressed as percentages and were evaluated using Fisher's exact test. All statistical analyses were performed using JMP Pro 15 (JMP Statistical Discovery LLC, Cary, United States), with statistical significance set at p < 0.05.
The mean age of patients with supraclinoid ICA fenestration was 48.1 years, with a female predominance (77.4%), while no significant difference was observed between the sides. Additionally, 84.8% of the cases were associated with intracranial aneurysms, and 38.7% presented with aneurysmal subarachnoid hemorrhage. The cranial division group was noted in nine cases (27.3%), with no discernible differences in age, sex, or side between the groups. However, caliber differences between the two limbs forming the fenestration were significantly more common in the cranial division group (p = 0.02). There were no notable differences in the occurrence of intracranial aneurysms or subarachnoid hemorrhages between the groups (p = 0.11, 0.7, respectively), although a trend toward aneurysms forming at the proximal end of the fenestration in the proximal group was observed (p = 0.06).
Discussions
Herein, we present the case of a woman with a ruptured left ICA-OA aneurysm proximal to the focal fenestrated ICA segment successfully treated with balloon-assisted coil embolization. Further, our literature review constitutes the largest compilation of previous reports using statistical analyses. Our review demonstrated notable caliber differences between the two fenestrated limbs if the cranial ICA division was involved. Further, our findings suggest that aneurysms related to fenestrations located proximal to the Pcom tend to develop at the proximal end of the fenestration.
Embryological hypothesis
Embryologically, the ICA is divided into cranial and caudal segments at the 4–5 mm stage2,33, with the cranial division developing into the anterior circulation and the caudal division into the Pcom. Therefore, the ICA beyond the Pcom is embryologically derived from the cranial divisions of the ICA, and is distinct from the segment proximal to the Pcom. In this study, fenestrations involving the cranial division were observed to have caliber differences between the two limbs forming the fenestration; this discrepancy/asymmetry was also observed in the present case. Because cerebral arterial fenestration is considered a congenital condition 2 , the differences in the morphology of the limbs forming the fenestration can be hypothetically explained embryologically.
Generally, cerebral arterial fenestration is considered to be caused by the failure of the fusion of two equivalent vessels, such as paired ventral longitudinal neural arteries that eventually form the BA.5,34 In such cases, the two arteries forming the fenestration have equal caliber. 35 Extracerebral anastomoses between perforators, in which the embryological rete of the perforators is partially residual, have also been proposed. 5 Although rare, fenestration of the middle cerebral artery (MCA) is thought to be caused by a failure of confluency in the extinction of the plexiform arteries. 36 In such cases, there is a difference in caliber between the two arteries that form the fenestration. Based on the two mechanisms of fenestration formation, the caliber differences in fenestrations, including cranial divisions, may be related to the presence of a plexiform stage in the formation of the AChA and MCA during ICA cranial division development. 2 Just as the temporopolar artery bifurcations are thought to be related to the formation of smaller fenestrations in the MCA 36 , it is also possible that the AChA and perforating arteries are related to fenestration formation. The presence of a smaller posterolateral fenestration at this site supports this hypothesis.
On the other hand, if the fenestration is located proximal to the Pcom, the two limbs forming the fenestration are comparable, suggesting that arteries of comparable sizes may fuse during fetal development. The segment between the OA and the Pcom is thought to be derived from the third aortic arch during embryonic life 33 , and there are no major branching vessels in this segment. Further, the cranial and caudal divisions are thought to be of equal caliber. This suggests that fenestration in the ICA segment proximal to the Pcom occurs during development when the Pcom is formed by caudal division. The caudal division that branches off from the proximal part of the ICA fuses to a more distal portion during development, which may have caused fusion failure.
In this case, confluence failure in the plexiform extinction of the cranial division of the ICA may have contributed to the ICA fenestration. Anatomically, the oculomotor nerve is located inferolateral to the ICA, and an aneurysm in this region can cause compression of the oculomotor nerve and, in rare cases, fenestration of the oculomotor nerve. 37 Since the oculomotor nerve runs along the dura mater between the posterior clinoid process and the oculomotor triangle, 38 it is not thought to penetrate the ICA.
Intracranial aneurysm formation
Cerebral arterial fenestrations are often associated with aneurysm formation. 6 There are two main theories to explain the formation of an aneurysm in the presence of arterial fenestration: the fragility of the vascular structure in the fenestrated vessels and the hemodynamic stress at the site of fenestration. 2 Although some studies have shown that the fragility of the vessel wall can be attributed to the loss of the muscular layer 2 , this has yet to be proven histologically in ICA.
Given that the ICA is a high-flow artery, narrowing caused by fenestration and turbulence may lead to hemodynamic stress. The high reporting rate of ICA fenestration compared to its prevalence suggests that ICA fenestration may be more prone to aneurysm formation than other sites 1 , potentially due to the high flow characteristics of the ICA. Computational fluid dynamics with the fenestration model have shown that stress on the vessel wall is localized at the proximal end of the fenestration and the distal lateral part of the limb 35 , which could explain the multifocal formation of aneurysms.
In this study, approximately 40% of supraclinoid ICA fenestrations with associated aneurysms presented with subarachnoid hemorrhage. However, as this literature review was heavily based on case reports, it is likely that the incidence of ICA fenestration and associated aneurysms was underestimated. This study also highlighted a higher tendency for aneurysms to form at the proximal end of the fenestration proximal to the Pcom group, which is presumably related to hemodynamic stress. Further research is required to study the differences in hemodynamic stress based on the location of fenestration and morphological characteristics, such as vessel caliber and incorporated arterial branches.
Endovascular treatment
It is important to recognize ICA fenestration on preprocedural cross-sectional and initial diagnostic angiographic images, as this focal filling defect may mimic a focal thrombus or air bubble. 39 To avoid complications, we suggest that in cases where balloon remodeling is deemed necessary, the balloon microcatheter—micro guidewire assembly should be navigated through the larger limb of the fenestration, with precise positioning of the balloon and gentle inflation over the aneurysm neck, sparing the fenestrated ICA segment to avoid vessel injury. In cases in which endovascular treatment is deemed too risk, for example because of the presence of fenestrated or deformed vessels, open surgical treatment should be considered. Vigilant post-treatment follow-up may be required because of the potentially higher risk of aneurysm recurrence or de novo aneurysm formation.
Conclusions
Supraclinoid ICA fenestration, particularly in the cranial division, may pose diagnostic and therapeutic challenges. Embryological origins and hemodynamic stress may contribute to fenestration morphology and associated aneurysm formation. Although effective, endovascular treatment requires meticulous planning to mitigate the risk of vascular injury. Our findings further underscore the importance of a precise diagnosis and careful procedural execution in managing this rare but clinically significant condition.
Footnotes
Abbreviations
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Written consent was obtained from the patient.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Krings acknowledges receiving research support from UMIC and the Dan Andrea and Patricia Holt-Hornsby Endowment.
This study did not receive any specific grants from funding agencies in the public, commercial, or non-profit sectors.