
Abstract
Background
Studies investigating endovascular therapy in vertebro-basilar stroke have led to controversial results in the past, but recent randomized trials seem to show an effectiveness superiority of endovascular therapy versus best medical treatment. However, uncertainty remains concerning many aspects of thrombectomy in acute basilar artery occlusion, notably technical considerations. This study compared the first-pass effect of direct thromboaspiration and combined thrombectomy in the setting of distal basilar occlusion.
Methods
An in-vitro experimental set-up was used, consisting of a vascular phantom model and thrombus analogs of different consistencies to mimic human clots. Thrombus analogs were injected into the model through the vertebral artery and flowed to the basilar distal third to mimic a distal basilar occlusion. Ten procedures were performed for each thrombus analog stiffness and technique (direct thromboaspiration versus combined thrombectomy).
Results
Direct thromboaspiration showed an overall first-pass effect rate of 83.3% (25/30) and was particularly effective for ultra-soft and soft clot analogs, but decreased for hard clot analogs. Combined thrombectomy had an overall first-pass effect rate of 56.7% (17/30). The effect rate for ultra-soft and soft clot analogs was 60% and 50% for hard clot analogs. In the softer clot analogs, the stent-retriever device used for the combined thrombectomies tended to deviate the clot analog from a co-axial trajectory with the aspiration catheter.
Conclusions
In the context of distal basilar occlusion, our in-vitro results showed that higher first-pass effect rates were achieved with direct thromboaspiration compared to combined thrombectomy in all types of thrombus analogs.
Introduction
Studies investigating the influence of endovascular therapy in vertebro-basilar stroke have led to controversial results in the past, but recent randomized studies, such as the ATTENTION 1 and BAOCHE trials, 2 have showed the benefit of endovascular therapy in terms of effectiveness versus best medical treatment.1–3
The main recommended endovascular strategies for acute basilar artery occlusion (ABAO) and, more generally, posterior circulation large vessel occlusion, are stent-retriever and aspiration-based thrombectomy. 4 Although previous studies have compared different aspects of these techniques,5–8 uncertainty remains concerning many aspects of thrombectomy in ABAO notably regarding technical considerations. In particular, which thrombectomy technique should be optimally used for which localization or with which thrombus type.9,10 Complete recanalization after a single pass, that is, first-pass effect (FPE) should be aimed at as it has been clearly associated with improved clinical outcome. 11 The purpose of this in-vitro study was to compare FPE and embolic complications in direct thromboaspiration (DTA) and combined thrombectomy for distal basilar occlusion by clots of differing stiffness.
Materials and methods
In-vitro set-up
The study was performed using a vascular phantom model and thrombus analogs (TAs) of different consistencies. Figure 1 summarizes our experimental set-up.
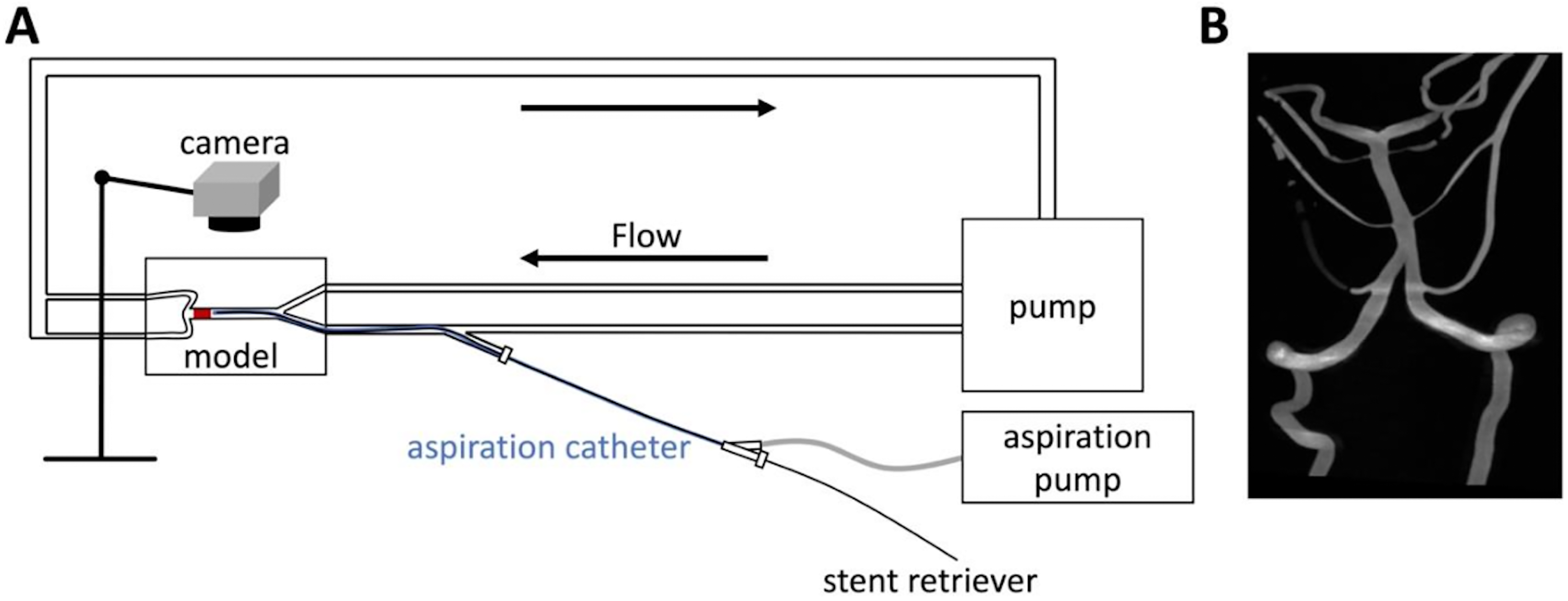
(A) Schematic representation of the experimental setup. (B) 3D RA representation of the vascular phantom.
TA production
TAs were produced using mixtures of guar, borax, and water to mimic human clots of different stiffness, according to the procedure reported by Bernava et al. 12 Guar and borax were added to water in different concentrations to obtain softer or harder clots. Cylindrical samples with a 10 mm height and a 5 mm diameter were extracted from the mixtures to measure their stiffness by compression tests with a vertical compression machine (Sauter FL10, Sauter GmbH, Wutöschingen, Germany). Samples were compressed to 50% of their initial height. Hard, soft, and ultra-soft TAs originated from mixtures requiring compression forces equaling 9.24, 3.27, and 1.72 mN/mm2, respectively. These mechanical properties are within similar ranges to ones described in previous in-vitro studies.12,13 TAs of 6 mm diameter and 5 mm height were produced.
Flow model
The vascular phantom consisted of a silicon model (Elastrat Sarl, Geneva, Switzerland) derived from a real patient-specific anatomy corresponding to an ectasic basilar artery. 14 The phantom was continuously flushed with water heated at 37 °C using a steady-state pump. A canister was installed at the system outlet to collect distal emboli. TAs were injected into the model through the vertebral artery and flowed to the basilar distal third to mimic a distal basilar occlusion. All experiments were recorded.
In-vitro mechanical thrombectomy experiments
Two operators experienced in mechanical thrombectomy (MTB) performed MTB experiments as described below. Ten procedures were performed for each TA stiffness and technique.
DTA: a large bore aspiration catheter (AC) (SOFIA 6F, MicroVention, Aliso Viejo, CA, or React 71, Medtronic, Irvine, CA) was introduced into the phantom vertebral artery via a standard 9F guide catheter (Cordis vista brite, Miami, FL) and advanced up to the proximal edge of the TA. An automated vacuum system performed aspiration (Stryker Medela AXS; Stryker, Kalamazoo, MI). DTA was performed according to the following procedure. Once placed in contact with the proximal edge of the TA, the AC was connected to the pump by a tube, which was clamped for around 90 s until a vacuum pressure of around −90 kPa was obtained. The connecting tube was then unclamped to suddenly transmit negative pressure through the AC. Anterograde flow through the phantom was not arrested in order to avoid positive interference with DTA efficacy. Effective DTA was defined as aspiration of the TA through the AC into the vacuum system canister or the TA remaining corked at the distal end of the AC during retrieval, with ingestion of the TA occurring during the retrieval process or when entering the guiding catheter.
Combined thrombectomy: a stent-retriever device (Solitaire X 4 × 40 mm, Medtronic, Irvine, CA, or Solitaire 2, 4 × 40 mm, Medtronic) was introduced through the ACs positioned at the level of the antero-inferior cerebellar arteries and placed at the occlusion site through a 0.021 inches microcatheter (Phenom 21, Medtronic, or Trevo 18, Stryker). Stent-retrievers were delivered over and beyond the TA using a standard technique. 15 After a 3-to-5-min time lapse after stent deployment for interaction with the TA, the stent was gently completely retrieved coaxially in the AC. Machine aspiration was performed simultaneously. An effective combined thrombectomy FPE was defined as the ingestion of the TA in the AC after complete or during retrieval of the stent.
For both techniques, failure was defined as non-retrieval of the TA at first-pass. FPE and the presence of embolic complications according to clot stiffness and technique were evaluated.
Statistical analysis
As a categorical variable, FPE rate was analyzed using a Pearson's chi-squared test after ensuring that its assumptions were met. For this variable, we compared DTA with combined thrombectomy and with the different types of TA (ultra-soft, soft and hard). Statistical analysis was performed with SPSS, version 29 (IBM, USA) with significance set to p < 0.05 (one and two-sided).
Results
Table 1 summarizes the results of our study.
Summary of results.
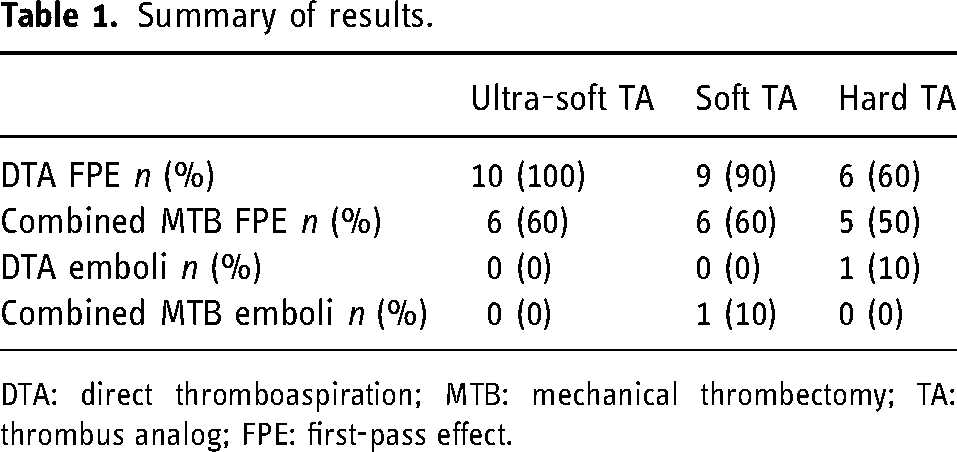
DTA: direct thromboaspiration; MTB: mechanical thrombectomy; TA: thrombus analog; FPE: first-pass effect.
Direct thromboaspiration
Overall, DTA resulted in FPE success in 25/30 (83.3%) cases. Ultra-soft TA: DTA resulted in completely ingested TAs at first-pass in all 10 cases (100%) directly after the connection between the AC and the vacuum system was unconstrained. Soft TA: FPE was achieved in 9/10 (90%) cases. They were mostly completely ingested when the connection between the AC and the vacuum system was unconstrained. Eight of 10 (80%) TAs were completely ingested at first-pass. Two (20%) remained corked at the AC distal tip. In 1/10 (10%) cases, the corked TA was finally aspirated by the AC just a few centimeters cranially to the guiding catheter's distal end, located in a region of the phantom that can be likened to the V2/V3 junction. In the remaining case, the TA was first corked at the AC tip, but was lost at the vertebro-basilar junction.
Hard TA: FPE was achieved in 6/10 (60%) cases. Two different scenarios could be distinguished. First, complete TA ingestion occurred in 4/6 (67%) cases. Second, the TA remained corked at the AC tip in 2/6 (30%), with 1/6 (16.7%) being aspirated when the AC arrived at the vertebro-basilar junction and the remaining one (16.7%) at the region of the phantom, which can be likened to the V2/V3 junction a few centimeters cranially to the guiding catheter's distal end. In 4/10 (40%) cases, FPE failed. In two cases, the TA clogged at the AC tip and was lost at the vertebro-basilar junction and in one case, the TA clogged at the AC tip, but fragmented at the vertebro-basilar junction and was only partially removed. The remaining fragment embolized at the basilary middle third. In 1/4 first-pass failure cases, the TA was first clogged at the AC tip and then lost at the basilary middle third.
Combined thrombectomy
Overall, combined thrombectomy resulted in FPE success in 17/30 (56.7%) cases.
Ultra-soft TA: the procedure resulted in TA removal at first-pass in 6/10 (60%) cases with direct TA ingestion when brought at the tip of the AC by the stent. In 4/10 (40%) cases resulting in first-pass failure, the TA was brought at the AC tip, but could not be ingested as the stent tended to deviate the TA from a co-axial trajectory with the AC (Figures 2 and 3). Soft TA: complete TA removal at first-pass was observed in 6/10 (60%) cases. In 3 (30%) cases, the TA was clogged at the AC tip and aspirated at the portion of the phantom corresponding to the V4 segment at first-pass. In another 3 (30%) cases, it was directly ingested when brought at the AC tip by the stent. TA clogging until the V4 portion was also observed in 2/10 (20%) cases, but was eventually lost at V4 level. In 1/10 cases, the TA was partially ingested by the AC when brought to its tip by the stent at the anterior inferior cerebral artery level. The residual non-ingested TA embolized to the basilary middle third. In 1/10 cases, the TA remained blocked at the vertebro-basilar junction. Deviation of the TA by the stent-retriever device from a co-axial trajectory with the AC was observed in a similar way to the ultra-soft TAs.
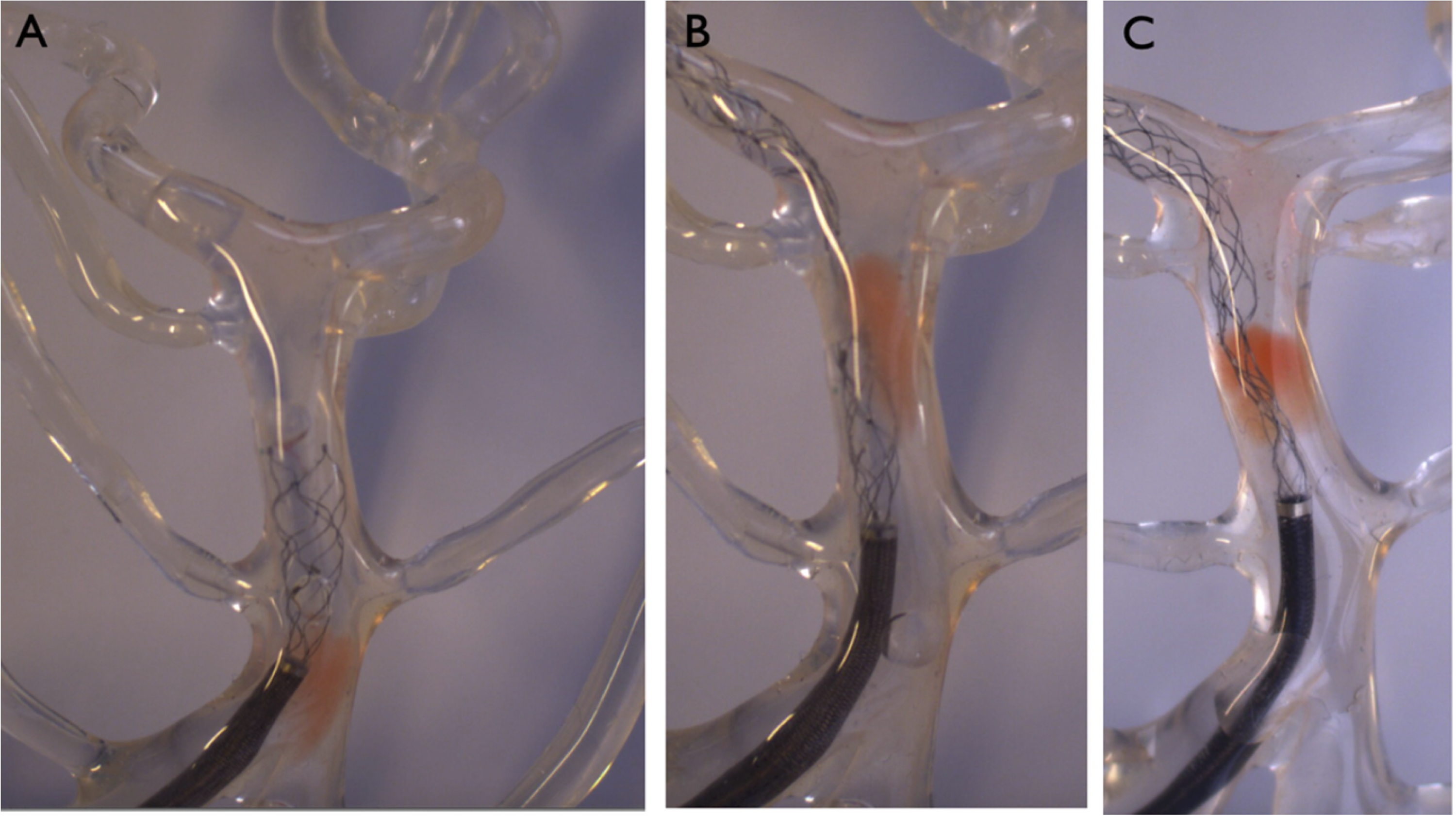
Interaction between thrombus analog and stent-retriever in combined thrombectomy. Particularly in situation A (ultra-soft TA), but also in situation B (soft TA), we can observe a deviation of the TA by the stent-retriever from the axis of the AC. In situation C (hard TA), there is no deviation of the TA from a coaxial direction with the AC.
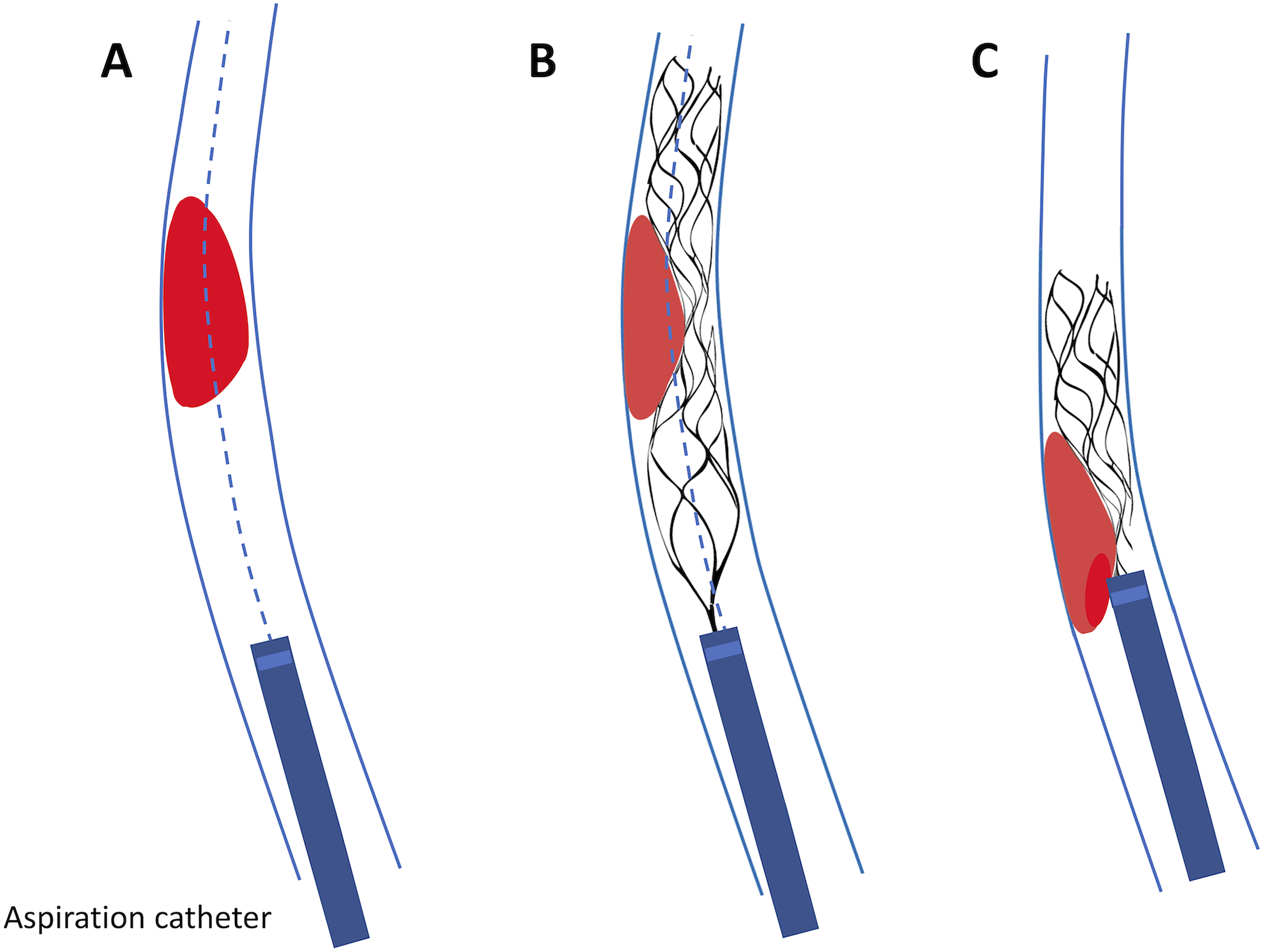
Schematic view of the phenomenon described in Figure 2. Soft and ultra-soft TAs (in red) tend to be deviated from a co-axial trajectory with the AC by the stent-retriever.
Hard TA: FPE was achieved in 5/10 (50%) cases. In 2/10 (20%) cases, it resulted in removal of the TA via direct ingestion by the AC when the TA was brought at the AC tip by the stent-retriever. The TA was clogged at the AC tip and aspirated at the portion of the phantom corresponding to the V4 segment in 1/10 (10%) cases and at the level of the guiding catheter in 2/10 (20%). In 1/10 cases, the TA was brought by the stent-retriever at the level of the AC tip, but it was unable to interact with the TA. In our last case (10%), the TA was clogged to the AC tip and lost at the vertebro-basilar junction. In 2/10 (20%) cases, the TA remained blocked at the vertebro-basilar junction and in 1/10 (10%) at the basilary middle third. TAs tended to stay coaxial to the AC, contrary to what was observed with softer TAs.
Overall, DTA achieved a statistically significant higher FPE rate than combined thrombectomy (p(two-sided) = 0.047. p(one-sided) = 0.024. 83.3% (25/30) vs 56.7% (17/30) FPE rate).
A trend for higher FPE rate was found for DTA compared to combined thrombectomy for the ultra-soft TA subgroup (p(two-sided) = 0.087 (trend level), p(one-sided) = 0.043. 100% (10/10) vs 60% (6/10) FPE rate).
Discussion
Our study showed higher effectiveness of DTA in terms of FPE for distal basilar occlusions than combined thrombectomy across all clot consistencies. In the vast majority of combined procedure failure, the stent deviated the clot from co-axial trajectory with the AC. As previously reported, one of the main factors related to aspiration success is the angle of interaction between the AC and the clot. During combined thrombectomy, the stent-retriever tended to create a unfavorable angle between the AC and the TA, which limited the technique's efficacy. 12 Alexandre et al. highlighted that combined techniques were associated with the highest number of passes in ABAO. 16 This finding could be corroborated by our finding that the stent-retriever device during the combined technique tended to deviate the TA. Moreover, the AC flow rate could be reduced when the stent-retriever and microcatheter devices were in certain positions inside the AC, 17 which may also provide additional explanations for this finding.
Concerning clot composition, previous studies that investigated if a particular technique was superior to another for fibrin-rich (i.e. in the stiffer range) or red blood cell-rich (i.e. in the softer range) clots10,18 led to non-consensual results. In ABAO, clots tend to have a higher red blood cell composition compared to anterior circulation, and therefore are more often in the softer range. 18 Our results suggest that it would seem advisable to first start with DTA for distal third basilar occlusions, especially knowing that clot consistency would most probably be soft.
An interesting aspect is also the influence of the basilar diameter. Patients with larger basilar diameters have a higher risk of posterior circulation stroke of cardio-embolic origin, which is also the most frequent reported etiology of distal basilar occlusions.19,20 Some studies highlighted that distal ABAO had the worst outcomes, hypothesizing that the mostly cardio-embolic etiology does not allow collateral creation.21,22 Previous studies also demonstrated that larger basilar diameters correlated with increased stroke-related mortality and cardiovascular events23,24 or even stroke recurrence if the basilar artery diameter was superior to around 5 mm. 14 These aspects also motivated us to use a basilar phantom in the larger diameter range, which was based on the anatomy of a real patient. Kyselyova et al. also suggested that a high catheter-to-vessel ratio was favorable in DTA, 25 permitting increased TICI (≥2b) grades and a lower pass number. Similarly, Pampana et al. reported that a vessel-to-catheter ratio ≤1.51 maximized a mTICI ≥2b in isolated middle cerebral artery occlusion. 26 As our phantom had a large diameter, we could consider it as a worst clinical scenario due to catheter-to-vessel ratio reduction. However, despite this, our results showed a higher FPE with DTA compared to combined thrombectomy.
Previous studies have highlighted the advantages of DTA in the setting of posterior and basilar stroke compared to stent-retriever or combined techniques, notably concerning outcomes, complication rates and procedure time, although never focusing on a particular localization within the basilar artery.5,27 These findings could be corroborated by our results, as the overall FPE rate was statistically higher with DTA compared to combined thrombectomy, with additionally a trend for higher FPE rate in the ultra-soft TA subgroup. This highlights the advantages of DTA for distal basilar occlusions. The clinical complexity, possible disastrous consequences, and the distal basilar occlusion's unique nature motivated us to conduct this study in a highly reproducible setting, with a focus on FPE for this type of occlusion.9,20,28,29 Combined thrombectomy has been presented as possibly limiting embolic complications. 30 However, these were only observed once for both techniques with a soft TA during combined thrombectomy and a hard TA during DTA. Thus, our study does not show the superiority of either technique on this aspect.
Our study has some limitations. The MTBs were realized in a silicone model. The model, filled with water, which has a different viscosity than blood, but was considered adequate to compare both MTB techniques. The interactions between the thrombectomy devices, the vessel wall, and the TAs do not fully replicate in-vivo conditions. For example, TA adhesion to the vessel wall is a difficultly predictable factor, which may have limited the efficacy of thrombectomy, particularly when a stent retriever was used during combined thrombectomy. Our phantom simulated an ectasic basilar artery to demonstrate a worst-case clinical scenario.
Conclusions
Our in-vitro study showed the efficacy and high FPE rate of DTA in the context of distal basilar occlusion and, overall, DTA FPE rates were higher than those of combined MTB. The use of a stent-retriever device during combined thrombectomy tended to deviate the TA from a co-axial trajectory with the AC, leading to a negative influence on clot removal.
Footnotes
Author Contributions
All authors were substantially involved in the study design and interpretation, as well as manuscript revision and final approval. RS and PM were involved in the conception of the study, acquisition and analysis of the data, and initial manuscript draft.
Data availability statement
Data are available upon reasonable request.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PM is consultant for Medtronic and Stryker.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (grant numbers 320030_188942 and 32003B_182382).