
Abstract
Objective
Carotid artery webs are an underappreciated cause of recurrent ischemic stroke, and may represent a significant portion of cryptogenic stroke. Evidence-based guidelines for the management of symptomatic carotid webs do not exist. The goal of this study is to audit our local experience for patients with symptomatic carotid artery webs undergoing carotid stenting as a treatment option, along with describing the hypothesized dynamic physiology of carotid webs.
Methods
All patients undergoing stenting for symptomatic carotid artery web at two comprehensive regional stroke centers with high endovascular thrombectomy volume from January 1, 2012 to March 1, 2021 were included. The modified Rankin Scale (mRS) score was used to define functional outcome at 3 months after stenting.
Results
Fourteen consecutive patients with symptomatic carotid artery webs underwent stenting. Twelve patients were female (86%), with a median age of 54 (IQR, 48–64) years across all patients. Stroke was the qualifying event in 12 (86%) patients and TIA in 2. Eleven patients (11/14, 79%) achieved a mRS score of 0–2 at 90 days, 2 (14%) were mRS 3–5, and one patient was lost to follow-up. The median follow-up was 12 months (IQR, 10–12). There was no recurrent stroke or TIA like symptoms in any patients.
Conclusions
Carotid stenting appears to be safe at preventing recurrent stroke/TIA with a median follow-up of 12 months in this retrospective multicenter observational study.
Introduction
Stroke is a leading cause of disability and the fifth-leading cause of death in the developed world. 1 The majority of strokes are ischemic in etiology, accounting for 80–90% of all strokes. Cryptogenic strokes are those stokes for which no probable cause is identified after diagnostic evaluation, and account for 30% of all ischemic strokes. 2 Carotid artery webs may be an underappreciated cause of recurrent ischemic stroke, and may represent a potentially causative portion of cryptogenic strokes.3,4 Histologic examination of surgically resected carotid webs reveals an atypical form of fibromuscular dysplasia, most commonly affecting the intimal layer of the vessel wall. 5 This intimal hyperplasia can project into the vessel lumen as a web-like structure. 5 The web can alter laminar flow, causing blood stasis and predicating the formation of thrombus within the carotid bulb. 6 Radiographically, webs are located on the posterior wall of the carotid bulb and appear as a thin shelf-like filling defect on sagittal or oblique images, and as a thin septum on axial imaging. 6
Evidence-based guidelines for the management of symptomatic carotid webs do not exist, and a comprehensive systematic review of the literature in 2018 identified only 135 reported patients with symptomatic carotid webs, the majority of which (70%) were of African race. 7 Treatment options for symptomatic webs include medical management (anticoagulant or antiplatelet medication) and carotid revascularization with carotid artery stenting (CAS) or carotid endarterectomy (CEA). A recent study by Wojcik et al. 2019 of subspecialist across multiple neurologic disciplines revealed that single (25%) and dual (26%) antiplatelet therapy was the preferred treatment following acute stroke secondary to carotid web, followed by CAS/CEA (21% combined). 8
However, the rates of recurrent stroke or transient ischemic attack (TIA) on antiplatelet or anticoagulant medication can be as high as 30%, and therefore initial surgical interventional may be warranted in patients with symptomatic carotid webs.4,9,10 Surgical intervention was more heavily favored in patients with recurrent stroke, where 65% of clinicians were now split between CAS and CEA. 8 The aim of this study is to audit our local experience for patients with symptomatic carotid artery webs undergoing carotid stenting as a treatment option. The descriptive analysis explored patient characteristics, periprocedural medical management, endovascular stenting techniques, and radiographic and clinical outcomes.
Methods
Research ethics board approval was obtained for this multi-center retrospective observational study. All patients undergoing CAS for symptomatic carotid artery web at two comprehensive regional stroke centers with high endovascular thrombectomy volume (>150 cases/year) serving the Greater Toronto Area, from January 1, 2012 to March 1, 2021 were included. There were no exclusion criteria. Patient baseline characteristics retrieved included: age, sex, race, stroke risk factors (hypertension, smoking, dyslipidemia, coronary artery disease, diabetes, and atrial fibrillation), previous stroke or TIA, and baseline antithrombotic medication (antiplatelet or anticoagulant therapy).
Other presenting/treatment characteristics recorded include baseline National Institute of Health Stroke Scale (NIHSS) score, Alberta Stroke Program Early CT Score (ASPECTS), perioperative antithrombotic regimen, endovascular thrombectomy (EVT), carotid stenting timing and technique (stent type, balloon angioplasty, distal embolization protection device).
Carotid web imaging and diagnosis
On presentation, all code stroke activations at our centers undergo CT angiography of the head and neck. Therefore all carotid webs were initially diagnosed on CT angiography, and confirmed on catheter angiography during the CAS procedure. A diagnosis of carotid web was made when there was a luminal shelf-like filling defect on the posterior wall of the carotid bulb on sagittal/oblique images, and a thin membrane-like septum on corresponding axial images (Figure 1). 3 All images were reviewed by at least 2 fellowship-trained neuroradiologists or neurointerventionalists.
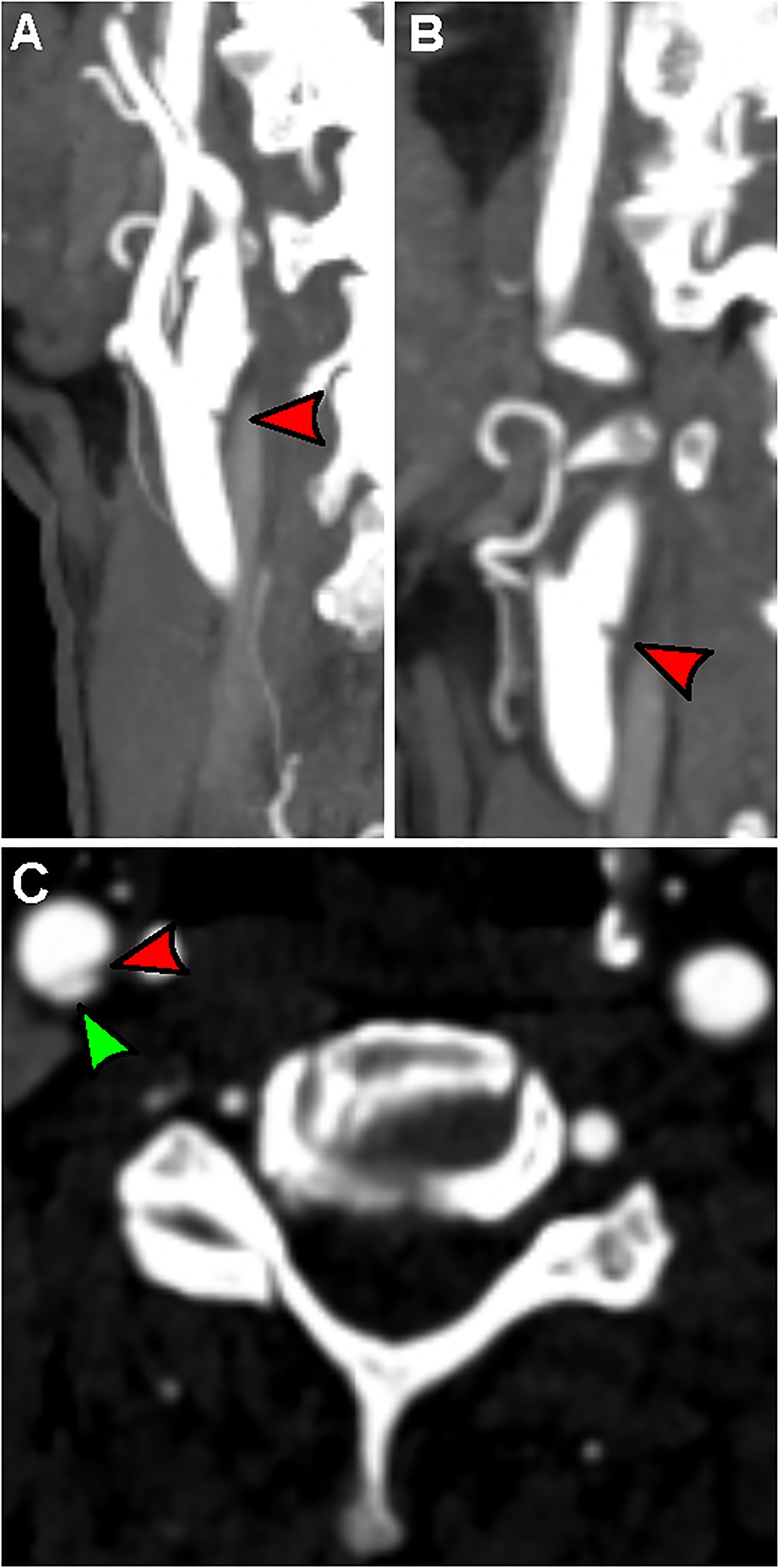
Computed tomography angiography (CTA) of a carotid artery web. (a) Oblique CTA displaying a shelf-life defect at the posterior carotid bulb (red arrow). (b) True sagittal CTA again displays the filling defect (red arrow). (c) Axial imaging shows the luminal filling defect, with a thin septum (red arrow) separating the carotid web (green arrow) from the carotid lumen.
Standard diagnostic evaluations to determine stroke etiology include hematologic testing (complete blood count, platelet count, international normalized ratio, and partial thromboplastic time), lipid prolife, glucose, CT angiography of the head and neck, MRI of the brain, transthoracic echocardiogram, and 12-lead electrocardiogram with inpatient cardiac telemetry. Attributing an ipsilateral stroke to a carotid web lesion required a negative stroke work-up by Trial of ORF 10175 in Acute Stroke Treatment (TOAST), and patients with >1 potential etiology were not classified as having a symptomatic carotid web. Therefore, patients were diagnosed as having a symptomatic carotid web when the following three criteria were met: (1) acute stroke or TIA in the corresponding vascular territory, (2) imaging criteria consistent with carotid web as observed on CT angiography, and (3) comprehensive stroke work-up identifying no other likely etiology for the stroke.
Clinical and radiographic outcome measures
The modified Rankin Scale (mRS) score was used to define functional outcome at 3 months after stenting, as measured by a stroke physician. For patients undergoing EVT, the modified treatment in cerebral infarction (mTICI) score was used to define reperfusion. All CAS periprocedural complications were recorded, along with post-procedural complications resulting from antithrombotic medication. All CAS patients undergo either CT angiography or carotid Doppler imaging at 3- and 6-months post-stenting, and annually thereafter, and any changes in degree of stenosis were recorded. Follow-up data on stroke or TIA recurrence after stenting was recorded as far as data was available for each patient. All continuous variables were recorded as medians with interquartile range, and categorical variables were recorded as counts with percentages.
Results
Patient baseline characteristics
Fourteen consecutive patients with symptomatic carotid artery webs underwent CAS. Twelve patients were female (86%), with median age of 54 (IQR, 48–64) years across all patients. Stroke was the qualifying event in 12 (86%) patients, and hemispheric TIA in 2 (14%) in the same vascular territory. With respect to atherosclerotic risk factors, 3 (21%) had hypertension, 5 (36%) had hyperlipidemia, 2 (14%) had diabetes, 4 (29%) were smokers, and none had atrial fibrillation. No patients were on anticoagulation and 4 (29%) were on Aspirin (ASA). Two patients had previous strokes; otherwise, there were no previous strokes/TIA.
The median NIHSS score at presentation was 4 (IQR, 2–16) and the median ASPECTS was 8 (IQR 7–10). Seven patients (50%) underwent EVT with mTICI grade 3 reperfusion achieved in all patients. All patients received ASA on stroke/TIA presentation and were placed on dual anti-platelets after repeat CT imaging showed no intracranial hemorrhage the next day. Twelve patients received Clopidogrel as a second anti-platelet agent and two received Ticagrelor.
Carotid artery stenting
All patients were on dual-antiplatelet therapy for a minimum of 3 days prior to the stenting procedure. The timing of the stenting procedure was based on patients’ clinical status. In the setting of preserved neurological function (mRS ≤ 2) in the affected neurological territory, stenting would be done during the same admission within 7 days. Two patients with initially disabling strokes (mRS > 2) returned at 3-months with substantial improvement in neurological function during rehabilitation and were subsequently stented. All stenting procedures were done under conscious sedation. Patients were heparinized after femoral puncture to achieve activated clotting time of 250–300 s. Diagnostic angiographic runs were performed to confirm the presence of the web (Figure 2).
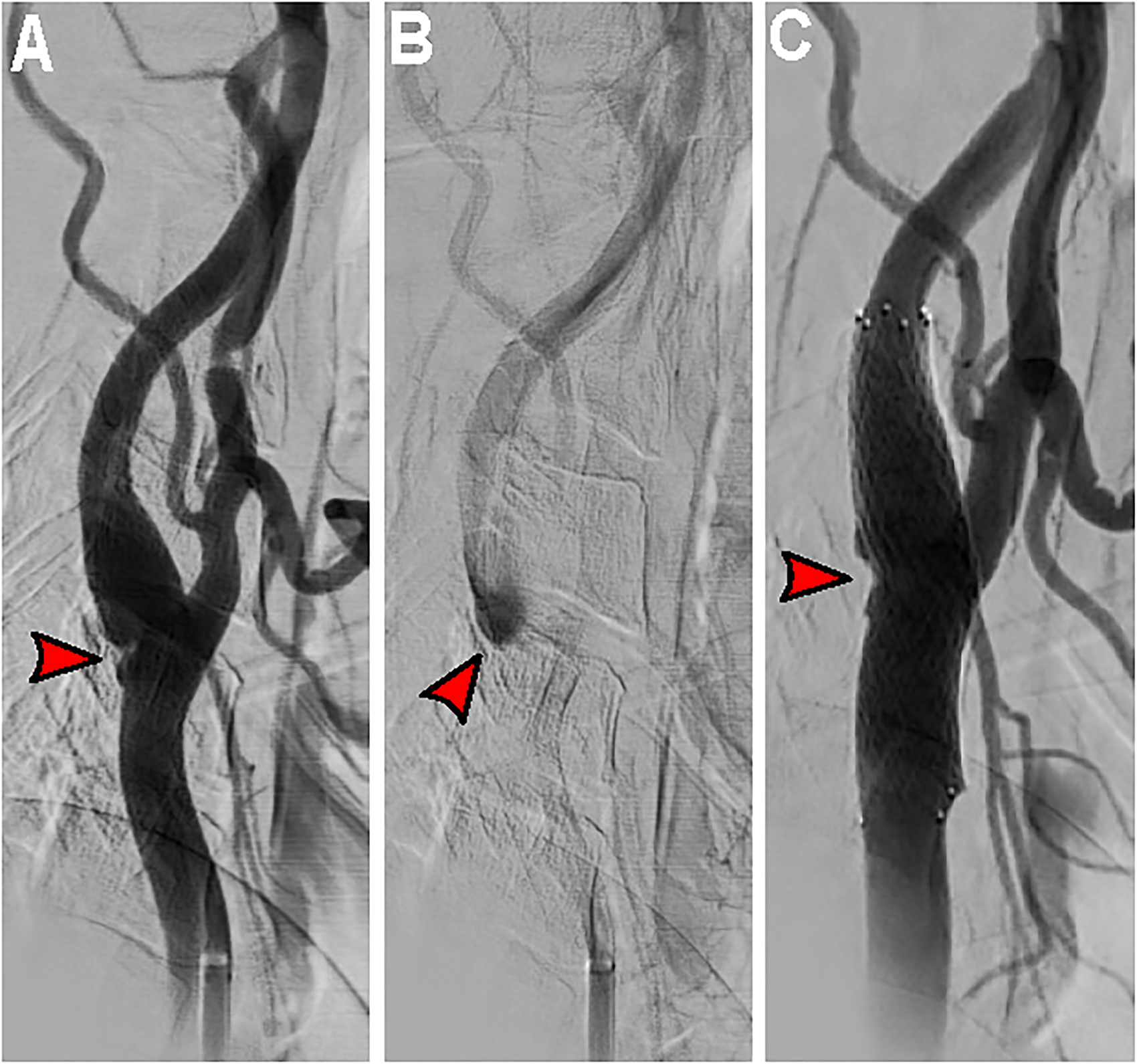
Patient two CAS. (a) Lateral common carotid artery injection reveals the shelf-like defect at the posterior carotid bulb. (b) Delayed lateral angiographic images displaying contrast stagnation within the web (red arrow) indicating blood stasis. (c) Angiogram after carotid stenting centered over the web (red arrow) with excellent stent-strut apposition and web flattening.
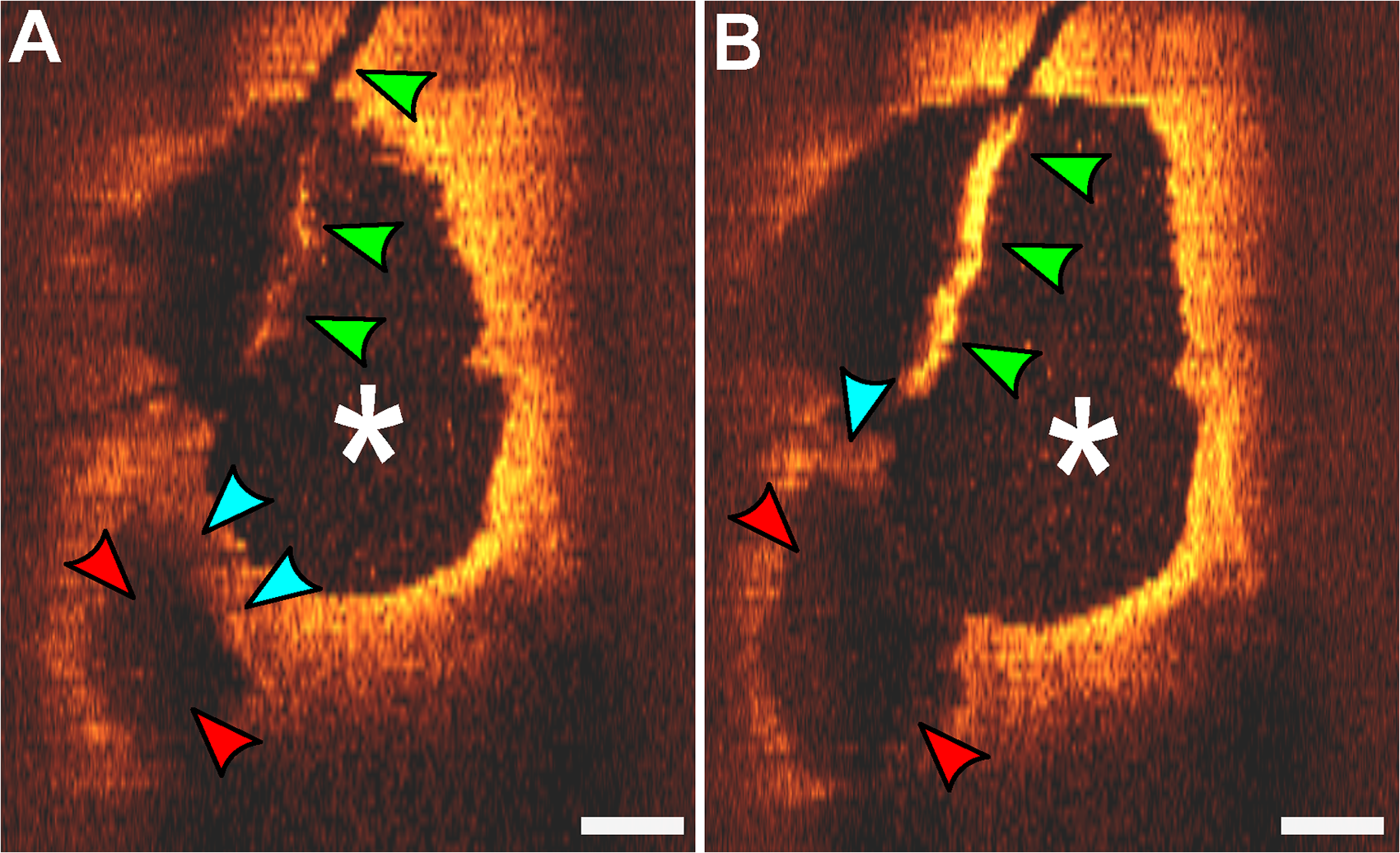
Endovascular OCT imaging of a carotid web. (a and b) The internal carotid artery lumen (white *) is appreciated along with the carotid artery web dysplastic septum (blue arrows), creating a pocket (red arrows) for blood stasis and thrombus formation. Artifact from the catheter is seen (green arrows). White bar = 1 mm.
Distal embolization protection devices were used in 9 (64%) of procedures, with 3 (38%) Emboshield NAV-6 (Abbott, Chicago, Illinois) devices, and 6 (43%) Spider-FX (Medtronic, Minneapolis, Minnesota) devices. With respect to stent type, six (43%) patients had Protégé (Medtronic, Minneapolis, Minnesota) open-cell stents implanted, four (28%) had XACT (Abbott, Chicago, Illinois), and four (28%) had Wallstent (Boston Scientific, Marlborough, Massachusetts) closed-cell stents implanted. Pre or post-stenting angioplasty was not performed for any patient. Only one stent was used for each patient. All patients were maintained on dual antiplatelet therapy for a minimum of 3 months, followed by monotherapy.
Clinical and radiographic outcomes
Eleven patients (11/14, 79%) achieved a mRS score of 0–2 at 90 days, 2 (14%) were mRS 3–5, and one patient was lost to follow-up. The median follow-up was 12 months (IQR, 10–12). There was no recurrent stroke or TIA-like symptoms in any patients. There was one periprocedural complication, a retroperitoneal hemorrhage, and no neurological complications for any patient. Follow-up routine carotid Doppler or CT angiography imaging did not show any adverse changes/in-stent stenosis for any patient. The median number of carotid dopplers completed for each patient was 3 (IQR, 2–3).
Discussion
The authors present multicenter retrospective observational data on CAS as a treatment option for patients with symptomatic carotid artery webs. Carotid stenting appears to be safe and efficacious at preventing recurrent stroke/TIA with a median follow-up of 12 months in this series. Our study has limitations, namely that this was a retrospective observational study and patient selection criteria for CAS for carotid web could be subject to selection bias. There was no standardization for patient and treatment selection.
Zhang et al. conducted the largest comprehensive systematic review for patients with symptomatic carotid artery webs finding that the majority of patients were young (median age 46 years) and 67% of the patients were female. Carotid webs are an atypical form of fibromuscular dysplasia, and fibromuscular dysplasia is significantly more prevalent in women (>80%) which could explain this gender imbalance. Zhang et al. found that 25/45 (56%) of patients managed medically with antiplatelet (91%) or anticoagulant (9%) medication had recurrent stroke with a median event time of 12 months. 7 Joux et al. similarly reported a stroke recurrence rate of 30% for patients treated with antiplatelet therapy. 10
The mechanism of thrombogenesis in carotid webs is likely complex. Haynes et al. resected six carotid webs during CEA for patients with symptomatic webs and found variable degrees of intimal fibrous hyperplasia with medial myxoid/fibrous thickening, proliferation of fibroblasts, neovascularization, and endothelial cells. 11 It is conceivable that these vessel wall changes and endothelial dysfunction can predispose to thrombogenesis at the site of the web. 12 Furthermore, one radiographic hallmark of carotid webs on angiography is blood stasis in the web (Figure 2(b)). The role of reduced blood flow and stasis in thrombogenesis is well documented, and therefore stasis in the web likely promotes thrombus formation.
Comparably, in patients with atrial fibrillation, the left atrial appendage (blind-ended passage) is the most common site of blood stasis and thrombus formation.13,14 Oral anticoagulants have proven to be superior to dual-antiplatelet therapy in preventing stroke in patients with atrial fibrillation. 15 It is hypothesized that platelet activation is not the predominant pathway of thrombogenesis in patients with atrial fibrillation. 15 Similarly, if platelet activation is not the primary driving force behind thrombus formation in carotid webs, this could help explain the high stroke recurrence rates in patients treated with antiplatelets.
The authors previously utilized endovascular optical coherence tomography (OCT) in a patient with a symptomatic carotid artery web, where the septum separating the internal carotid lumen from the web and the web pocket itself was visualized (Figure 3). 16 We hypothesize that the carotid web is dynamic, and its size and shape will vary depending on the amount of thrombus in the web pocket (Figure 4). Changes in the force on the wall of the web during systole and diastole may cause thrombus to be ejected from the web in the internal carotid artery causing strokes (Figure 4). We hypothesize that when no thrombus is present within the web pocket, the dysplastic segment of the web may be displaced against the vessel wall. In such a scenario imaging will not demonstrate the shelf-like filling defect and the web may go undiagnosed.
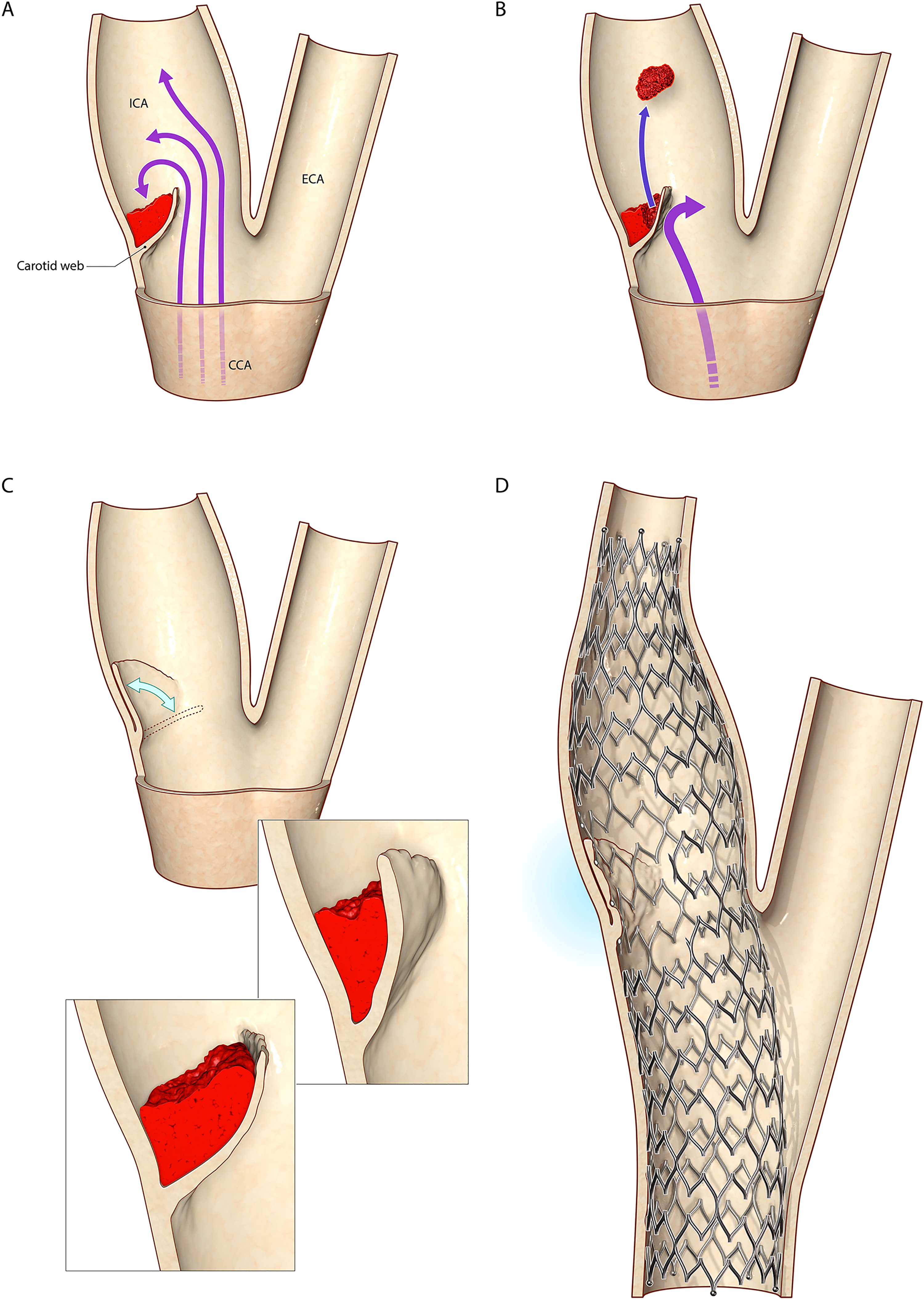
Representative dynamic illustration of a carotid web at the carotid bifurcation. (a) The carotid web is a form of fibromuscular dysplasia which forms a pocket with the posterior wall of the internal carotid artery distal to the carotid bifurcation. Thrombus is depicted within the pocket which forms from blood stasis/endothelial dysfunction. (b) Changes in the force on the wall of the web during systole and diastole causing thrombus to be ejected from the web in the internal carotid artery causing strokes. (c) If there is no/minimal thrombus within the web pocket, and the dysplastic segment of the web is displaced against the vessel wall, no shelf-like filling defect may be observed on imaging and the web may go undiagnosed. We hypothesize that the carotid web is dynamic, and its size and shape will vary depending on the amount of thrombus in the web pocket. (d) Carotid stenting displaces the dysplastic web segment against the vessel wall and promotes long-term neointimal formation along the stent, eliminating future thromboembolic events.
Furthermore, the duration of antithrombotics for patients with symptomatic carotid webs is unclear. Given there is no current evidence of the fibrotic webs remodeling or healing, lifelong therapy is likely indicated which can increase the risk of hemorrhage. In a study of more than 8000 cardiac patients undergoing stenting on dual-antiplatelet therapy, post-discharge bleeding was reported in 6.2% at a median time of 300 days. Even with an improved safety profile, novel oral anticoagulants carry a 2–3% yearly risk of major bleeding. 17 The median age of patients with symptomatic webs in our cohort was 59 years, and therefore the lifetime of risk of major bleeding is substantial.
Given the above, carotid remodeling as a first-line treatment for patients with symptomatic carotid webs may be reasonable. Joux et al. 2014 reported the largest series of 7 patients undergoing CEA for symptomatic web and reported no recurrent stroke/TIA with a median follow-up of 14 months. 18 More recently, Hayes et al. 2020 reported 6 cases of CEA for symptomatic web with no recurrent stroke/TIA at a mean follow-up of 6 months. 11
Haussen et al. 2018 reported the largest series of 24 patients with symptomatic webs undergoing CAS. 19 In their multicenter experience, the mean age was 47 years with 58% females. In a median follow-up of 12 months (IQR, 3–19) there were no new cerebrovascular events or perioperative complications. 19 Mathew et al. 2020 similarly reported on a single-center experience of 9 patients with symptomatic webs undergoing stenting and a mean follow-up of 5.5 months, with no reported cerebrovascular symptoms. 20
In this series, we report one complication of retroperitoneal hemorrhage and no neurological complications or recurrent stroke or TIA in follow-up. We hypothesize that the low stroke/TIA recurrence rate after CAS for carotid web is rooted in the immediate restoration of laminar flow in the internal carotid artery. It is apparent that the contrast pooling observed prior to stenting is reduced or eliminated immediately, and a well opposed carotid stent should promote near complete neo-endothelialization at 28 days covering the atypical dysplastic segment. 21 These events will eliminate both thrombogenic concerns of blood stasis and a dysplastic vessel wall.
Both CEA and carotid stenting appear efficacious in preventing future strokes in patients with symptomatic webs. We know that the CREST trial in 2012 showed that carotid stenting was effective and safe when compared to surgical endarterectomy for carotid artery stenosis. 22 Compared to CAS for atherosclerotic disease, CAS for carotid web is technically more straightforward, as the majority of patients with symptomatic carotid artery webs have minimal carotid stenosis. This reduction in stenosis leads to diminished need for pre and post-stenting angioplasty, and therefore a theoretical decrease in periprocedural stroke risk from showering thromboembolic material through the cells of the stent. Furthermore, long term stent restenosis rates may be lower in carotid web patients compared to atherosclerosis given risk factors for restenosis include high calcium content in plaques and smaller carotid diameters. The pathogenesis of stent restenosis is thought to include in part neointimal hyperplasia secondary to endothelial injury during stenting and angioplasty. Carotid web is a form of fibromuscular dysplasia as oppose to an atherosclerotic pathology, and stenting displaces the dysplastic web segment against the vessel wall, as oppose to the shearing forces during angioplasty and stenting required in atherosclerotic pathology, therefore theoretically decreasing endothelial injury.
Conclusion
CAS for symptomatic carotid web appears to be safe, technically feasible, and efficacious in preventing recurrent stroke. Future prospective studies are needed to determine the optimal treatment algorithm for these patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.