
Abstract
Background
In areas with high population spread such as Saskatchewan, it can be challenging to provide timely endovascular stroke treatment (EVT) to patients living far away from comprehensive stroke centres (CSC). We assessed the association of geography, stroke timing and weather conditions on EVT workflow times and clinical outcomes in Saskatchewan.
Methods
We included patients who underwent EVT between January 2017 and December 2022 in the province of Saskatchewan, Canada. Univariable and multivariable associations of time from last known well-to-CSC arrival, CSC arrival-to-reperfusion, and 90-day modified Rankin Score (mRS) with driving distance from patient home to CSC, transport mode, outdoor temperature and stroke timing (day & time) were assessed using descriptive statistics and multivariable regression.
Results
Three-hundred-three patients in the province of Saskatchewan underwent EVT between January 2017 and December 2022. Distance from patient home to CSC (beta-coefficient per 10 km increase = 0.02, 95% CI: 0.01–0.03) and direct to CSC transport (beta-coefficient = −0.76, 95% CI = −1.01–[−0.51]) were associated with last known well to CSC arrival time. In-hospital stroke (beta-coefficient = 0.37, 95% CI: 0.16–0.58), direct-to-CSC transfer (beta-coefficient = 0.27, 95% CI: 0.13–0.41) and daytime stroke onset (beta-coefficient = −0.15, 95% CI: −0.28–[−0.04]) were associated with time from CSC arrival to reperfusion. No association with 90-day mRS was seen.
Conclusion
Geographic factors and stroke timing were associated with EVT workflow times. However, no association with clinical outcomes was seen, suggesting that EVT patients living remote areas of Saskatchewan have similar benefit from EVT compared to urban areas. Every effort should be made to offer timely EVT to patients from remote areas.
Introduction
Acute ischemic stroke (AIS) is a severely disabling disease with a high mortality rate, particularly when caused by a large vessel occlusion (LVO). 1 Endovascular treatment (EVT), with or without intravenous thrombolysis, is a highly effective, but also highly time-dependent treatment for AIS due to LVO and has become standard of care in 2015.2–4 The rapid expansion of the EVT-eligible patient population constitute tremendous challenges for stroke systems of care, which need to adapt to this new situation. Saskatchewan is a sparsely populated Canadian province of 652,000 km2 with 1.2 million residents and temperatures that often stay below −20 °C for weeks during the winter months. As such, it faces additional unique obstacles when it comes to timely patient triage and treatment.
We assessed EVT workflow metrics and outcomes and their association with geographic factors, stroke timing and weather conditions in the province of Saskatchewan between January 2017 and December 2022.
Methods
This study was approved by the ethics committee of the Royal University Hospital, Saskatoon (REB 23-06). The data underlying analysis will be made available by the corresponding author upon reasonable request.
Patient sample
The current study included all patients who underwent EVT between January 2017 and December 2022 in the province of Saskatchewan, Canada. The Royal University Hospital of Saskatchewan is the only comprehensive stroke centre in the province; thus, all EVTs were performed at this centre. The primary stroke centres (PSCs) in Saskatchewan are as follows: St Joseph's hospital in Estevan, Lloydminster Hospital in Lloydminster, Dr FH Wigmore Regional Hospital in Moosejaw, Battlefords Union Hospital in North Battleford, Victoria Hospital in Prince Albert, Regina General Hospital in Regina (tertiary centre without EVT service), Cypress Regional Hospital in Swift Current and Yorkton Regional Health Centre in Yorkton. Note that not all these hospitals refer EVT candidates to Saskatoon, since some of the PSCs are close to the province border and refer EVT candidates to the neighbouring provinces (e.g. patients admitted to Lloydminster usually get transferred to Edmonton in Alberta for EVT).5–11
Data collection and curation
Clinical data of all acute ischemic stroke patients who underwent EVT between January 2017 and December 2022 in Saskatchewan are captured in the Canadian OPTIMISE registry, a national registry supported by the Canadian Stroke Consortium to ensure quality control for endovascular therapy and intravenous thrombolysis among patients with acute ischemic stroke. 12 Data for the OPTIMISE registry are captured using a web-based electronic data capture and reporting system and housed on a secure server at the Population Health Research Institute at McMaster University. OPTIMISE data were supplemented with patient data from administrative data sources (including patient homes’ postal codes, which were derived from the electronic medical records and then used as a proxy for patient location at the time of stroke onset). Imaging times at the PSC and CSC were derived from acute stroke imaging DICOM time stamps. The last intracranial run time, which was used as a surrogate for reperfusion time in case no eTICI 2b/3 reperfusion was achieved/documented, was also derived from DICOM time stamps.
Outcomes of interest
The main purpose of this study was to characterize EVT patients’ journey through the Saskatchewan stroke care infrastructure. As such, most analysis was descriptive in nature.
The three outcomes of interest in the multivariable analysis were:
the time from last known well to CSC arrival (capturing the pre-hospital and transfer phase of the patient journey until CSC arrival), the time from CSC arrival to reperfusion (capturing the in-hospital phase of the patient journey after CSC arrival). In case reperfusion could not be achieved (final eTICI 0-2a), the time of the last intracranial run, as derived from the DICOM time stamp), was used as a proxy for reperfusion time. modified Rankin Score (mRS) at 90 days.
Statistical analysis
Patient baseline characteristics, pre- and in-hospital workflow times as well as technical and clinical outcomes for the overall patient sample were reported using medians and interquartile ranges for continuous data and counts and frequencies for categorical data.
Univariable associations of primary and secondary outcomes with geographic factors (driving distance from patient home to CSC [km], transport mode [direct to CSC vs. PSC to CSC transfer vs. in hospital stroke], outdoor temperature [°C], since driving conditions are more challenging and air transport may not be possible during cold weather, and time factors (weekday of stroke onset [weekday vs. weekend], hour of stroke onset [8 a.m.–8 p.m. vs. 8 p.m.–8 a.m.]) were determined using Fisher's exact test, Wilcoxon rank sum test, Kruskal-Wallis test or Spearman correlation, as appropriate to the type of data.
We then built multivariable regression models for each outcome that included the abovementioned variables as independent variables, with patient age, sex and baseline NIHSS as additional adjustment factors. For time outcomes, linear regression was used and normal distribution of residuals was assessed visually and tested with the Shapiro–Francia-Wilk test. In case the residuals of dependent variables in linear regression were not normally distributed, logarithmic transformation of variables was attempted. For 90-day mRS, ordinal logistic regression was used. The parallel regression assumption for ordinal logistic regression was tested with the Brant test.
Since missing data were few, imputation for missing data was not performed.
All analyses were conducted using Stata 17.0 (Stata, LLC Corp), all statistical tests were two-sided and p-values <0.05 were considered statistically significant. Visualizations were generated using Microsoft PowerBI (Version 2.91).
Results
Between January 2017 and December 2022, 303 patients underwent EVT in the province of Saskatchewan at the Royal University Hospital. Of these, (144 [47.5%]) were women, median age 73 (interquartile range [IQR] 62–81). Baseline characteristics of the study sample are shown in Table 1. Figure 1A illustrates the patients’ journey from their homes to first hospital admission, Figure 1B shows the patients color-coded by time from last known well to CSC arrival. Supplemental Figure 1 provides an overview of outdoor temperature and additional environmental factors and workflow times throughout the study enrolment period. Median time from last known well to CSC arrival was 230 min (IQR 90–389), n = 275. Median time from CSC arrival to reperfusion was 106 min (IQR 79–144), n = 303. Median mRS at 90 days was 3 (IQR 1–6), n = 303. One-hundred-twenty-eight of 303 patients (42.2%) achieved a good outcome, while 88 (29.0%) died (see also Supplemental Table 1).
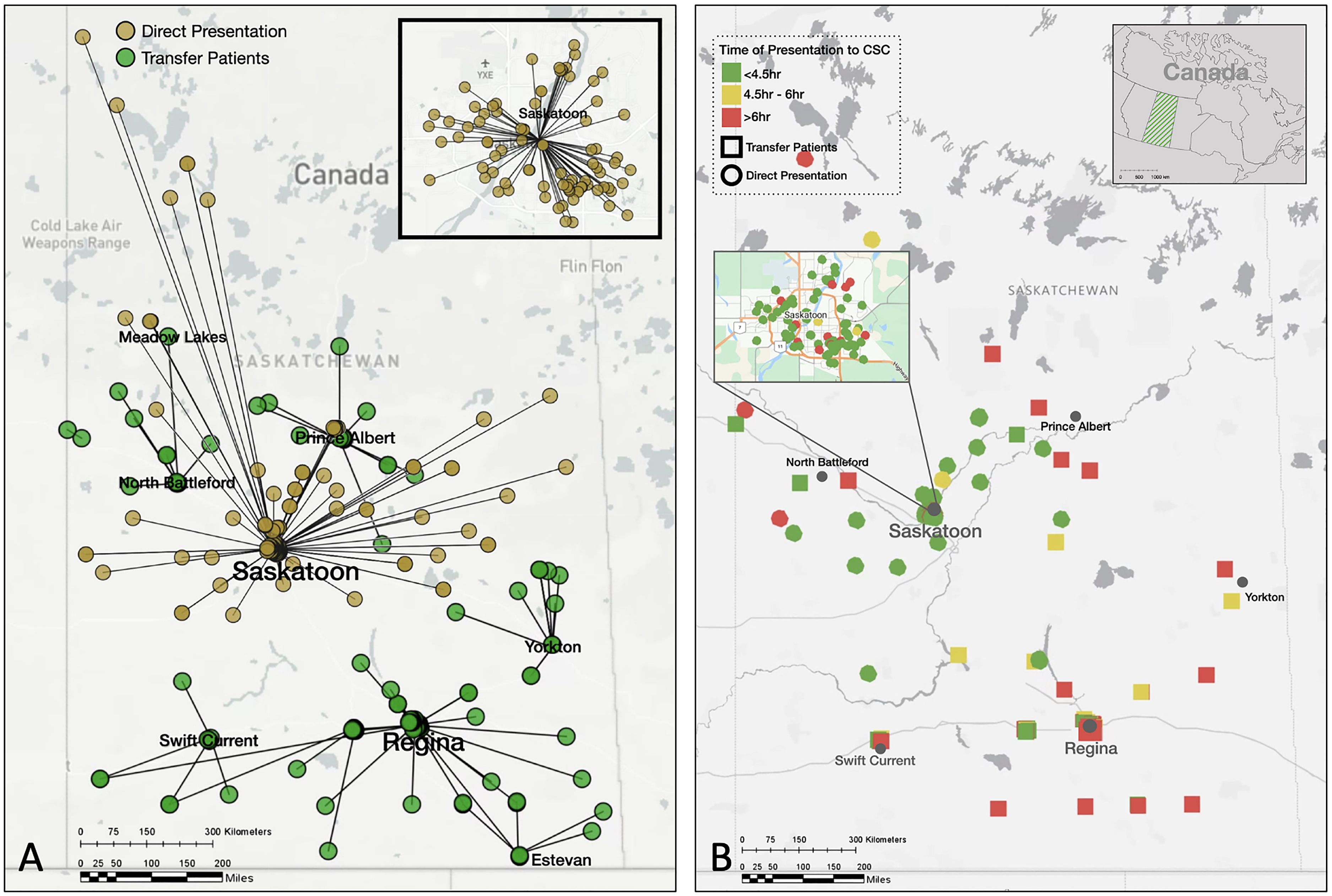
(A) EVT patients’ journey through Saskatchewan from their homes to first hospital admission. Green (dark grey) dots represent patients who initially presented to a PSC and were subsequently transferred to the Royal University Hospital (CSC, transfer routes not shown in this image). Brown (light grey) dots indicate patients who were directly admitted to the Royal University Hospital (CSC). Image in the right upper corner shows a magnified view of the city of Saskatoon. (B) Time from last known well to CSC arrival of EVT patients in Saskatchewan. Circles represent patients who were directly admitted to the CSC, while squares represent patients who were initially admitted to a PSC and subsequently transferred to the CSC. Green (medium grey) symbols indicate time from last known well to CSC arrival < 4.5 h, yellow (light grey) symbols 4.5–6 h, and red (dark grey) symbols > 6 h. Image in the right upper corner shows a magnified view of patients within the city limits of Saskatoon. Note that the position of the symbols has been slightly modified to ensure anonymity while keeping the distances to PSC and CSC accurate. Also note that not all dots may be seen individually since they may overlap. Distance from patient home to CSC did not differ significantly between the three groups (p = 0.58).
Baseline characteristics of the entire study sample (n = 303).
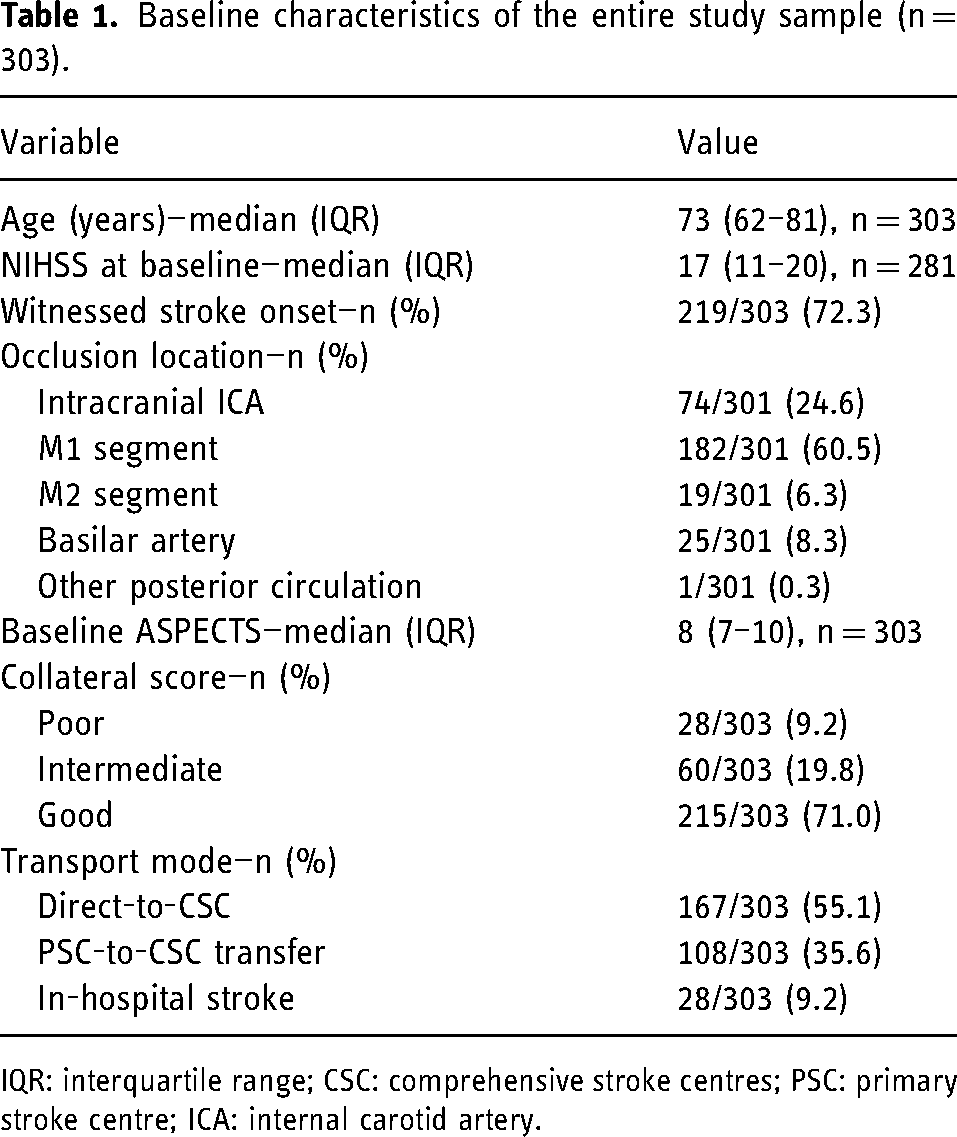
IQR: interquartile range; CSC: comprehensive stroke centres; PSC: primary stroke centre; ICA: internal carotid artery.
Univariable associations of geographic variables, stroke timing and temperature with outcomes
In univariable analysis, driving distance from patient home to CSC, outdoor temperature, stroke onset during daytime and transport mode were associated with time from last known well to CSC arrival (Table 2). Driving distance from patient home to CSC, outdoor temperature, stroke onset during daytime and transport mode were associated with time from CSC arrival to reperfusion (Table 2). None of the variables were associated with 90-day mRS in the univariable analysis.
Univariable association of geography, stroke timing and weather conditions on outcomes.
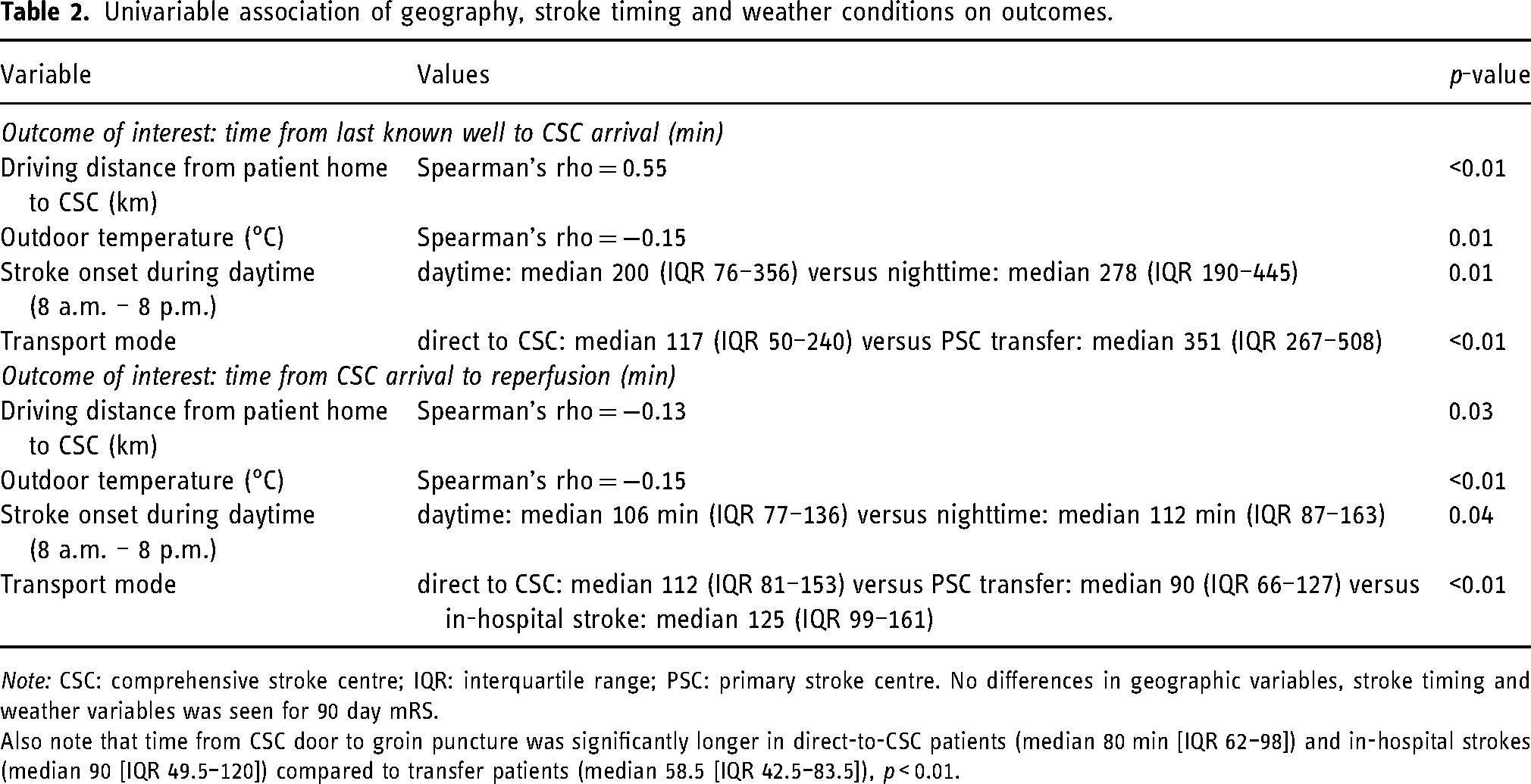
Note: CSC: comprehensive stroke centre; IQR: interquartile range; PSC: primary stroke centre. No differences in geographic variables, stroke timing and weather variables was seen for 90 day mRS.
Also note that time from CSC door to groin puncture was significantly longer in direct-to-CSC patients (median 80 min [IQR 62–98]) and in-hospital strokes (median 90 [IQR 49.5–120]) compared to transfer patients (median 58.5 [IQR 42.5–83.5]), p < 0.01.
In multivariable logistic regression, distance from patient home to CSC (beta-coefficient per 10 km increase = 0.02, 95% CI: 0.01 = 0.03) and direct to CSC transport as opposed to PSC-to-CSC transfer (beta-coefficient = −0.76, 95% CI = −1.01 – [−0.51]) were associated with log transformed last known well to CSC arrival time (p[Shapiro–Francia-Wilk = 0.12]). Note that patients with in-hospital stroke were excluded from this regression analysis.
In-hospital stroke (beta-coefficient = 0.37, 95% CI: 0.16 – 0.58) and direct to CSC transfer (beta-coefficient = 0.27, 95% CI: 0.13–0.41) as opposed to PSC-to-CSC transfer and daytime stroke onset (beta-coefficient = −0.15, 95% CI: −0.28 – [−0.04]) were associated with log transformed time from CSC arrival to reperfusion (p[Shapiro–Francia-Wilk = 0.04]), see also Figure 2.
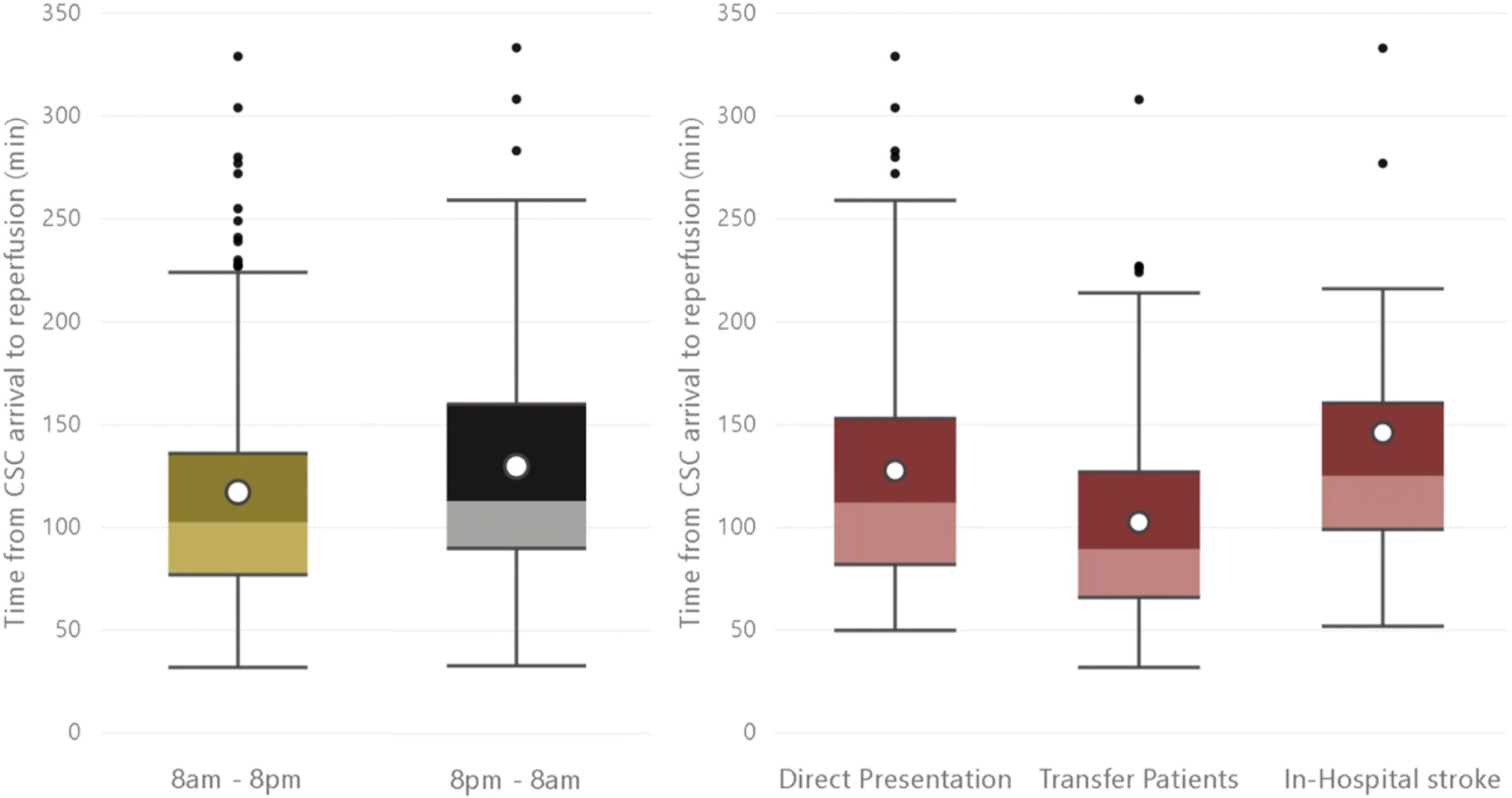
Left: Time from CSC arrival to reperfusion in minutes for patients with daytime (8 a.m. – 8 p.m.) versus night-time (8 p.m. – 8 a.m.) stroke onset/last known well time. Right: Time from CSC arrival to reperfusion in minutes for patients with in-hospital stroke versus direct-to-CSC transfer versus initial admission to PSC followed by PSC–CSC transfer. Note: CSC: comprehensive stroke centre; PSC: primary stroke centre. White dots in the boxplots represent means. Daytime presentation and transport mode were the only geographic/time factors that were significantly associate with time from CSC arrival to reperfusion in multivariable analysis.
None of the geographic and workflow factors were associated with 90-day mRS in the multivariable analysis (p[Brant] = 0.047).
Discussion
In this province-wide study of EVT patients in Saskatchewan, geographic variables and stroke timing well influenced pre-hospital and in-hospital EVT workflow times, but after adjusting for patient baseline characteristics, no association with clinical outcomes was seen among patients who received EVT. Our findings indicate that AIS patients in Saskatchewan living in remote areas far away from the hospital and presenting outside regular working hours may have a similar post EVT outcomes compared to patients living more closely to the CSC and presenting during working hours, despite slight delays in workflow time. One of the main reasons for this observation may be that Saskatoon has a uniform AIS pathway, whereby patients are directly brought to stroke centres (PSC or CSC), and hospitals that are unable to provide AIS care are bypassed. Of note, these findings may not apply to other geographies and jurisdictions.
Our multivariable analysis showed that time from last known well to CSC arrival increased with increasing driving distance of the patients’ home to the CSC, as has been reported before in a Spanish study, 13 as well as a study from Manitoba, a neighbour province of Saskatchewan that has a similar geography and population pattern. 14 Last known well to CSC arrival time was also decreased in patients who were directly admitted to the CSC, as opposed to transfer patients. Both these observations seem intuitively logical, but it is important to note that this prolongation of the pre-hospital phase did not translate into a statistical difference in clinical outcomes: it may well be that the advantage of receiving intravenous thrombolysis at the primary stroke centre somewhat balances out the EVT delay caused by PSC admission and subsequent inter-hospital transfer, and longer driving times to the CSC may allow the in-hospital team to prepare better for the patient. The fact that direct-to-CSC transfer was associated with significantly longer CSC-arrival to reperfusion times and longer CSC-arrival-to-puncture times supports this hypothesis: in direct transfer EVT candidates, there is less time for the neuro interventional team to prepare, and imaging still needs to be performed, thereby prolonging the procedure start. In transfer patients on the other hand, the CSC stroke team usually gets notified by the PSC to discuss the transfer, and the imaging obtained at the PSC is often sufficient for EVT decision making, so that repeat imaging at the CSC may not need to be performed. Stroke onset/last known well time during daytime (8 a.m. – 8 p.m.) as opposed to night time was also associated with decreased CSC arrival with reperfusion time, most likely because the neuro interventional team is already in the hospital, as opposed to during night time, when the team has to come in first.
Importantly, as opposed to some previous studies that report worse EVT outcomes in patients living in remote areas, 15 none of the geographic and time factors were associated with 90-day clinical outcomes in the current study. There are several potential reasons for this: first, our sample size may not have been large enough to detect a significant effect. Second, the effect of these factors on workflow times may have been too small to translate into a detectable difference in clinical outcomes. Third, factors unrelated to the EVT procedure may have influenced clinical outcomes. Such unrelated factors could be complications on the stroke unit like aspiration pneumonia, pulmonary embolism or urinary tract infections, post-stroke depression, and the inherent variability in patient resilience and their social support networks. Lastly, there may have been a selection bias, whereby among those patients living in remote areas with longer workflow times, only those with otherwise favorable baseline characteristics may have been deemed suitable for and treated with EVT. Since our sample does not include non-treated patients, we cannot rule out this possibility. Our group and others previously found that ASPECTS decay during inter-facility transfer is of the main reasons for not treating transfer patients with EVT.16,17 We suspect that this was the case for patients presenting with AIS in our 5-year study period as well. Since ASPECTS decay increases over time, it may well be that the delays we observed have resulted in a substantial number of AIS patients not being treated with EVT, and thus being excluded from the current analysis.
Limitations
Our study has several limitations. First, our patient sample included only patients who underwent EVT. Therefore, we were unable to investigate workflow times and outcomes in AIS patients who did not undergo EVT, and the reasons why these patients were not treated—it may well be that mostly patients with favorable baseline characteristics were chosen for EVT. Second, data are from a single Canadian province with unique geography and infrastructure, and the results may not necessarily be generalizable to other jurisdictions. In particular, local practice patterns related to repeat imaging as well as utilization of multimodality imaging vary considerably among hospitals and may influence patient selection for EVT. Third, there was evidence that the residuals in the multivariable model with CSC arrival to reperfusion time were not normally distributed despite log-transformation, and that the proportional odds assumption in the ordinal logistic regression was violated. Fourth, we did not have data on intravenous thrombolysis efficacy available and could therefore not assess how often thrombolysis-induced early recanalization of the target occlusion made EVT unnecessary. Lastly, the mRS score is a relatively crude outcome measure and may not capture the subtle declines in functional outcomes caused by slight delays in transport time.
Conclusion
In conclusion, geographic and time of stroke onset/last known were associated with pre-hospital and in-hospital workflow times in patients undergoing EVT in Saskatchewan, but after adjusting for patient baseline characteristics, no association with clinical outcomes were seen. Our findings indicate that EVT patients living in rural and remote areas of Saskatchewan may have similar benefit from EVT compared to those in urban areas in the setting of refined EVT workflows that reduce unnecessary delays. Every effort should be made to offer timely EVT to potential EVT candidates from remote areas.
Supplemental Material
sj-docx-1-ine-10.1177_15910199231196614 - Supplemental material for Influence of geography, stroke timing, and weather conditions on transport and workflow times: Results from a longitudinal 5-year Canadian provincial registry
Supplemental material, sj-docx-1-ine-10.1177_15910199231196614 for Influence of geography, stroke timing, and weather conditions on transport and workflow times: Results from a longitudinal 5-year Canadian provincial registry by Nima Kashani, Johanna Maria Ospel, Nishita Singh, Amy Zhou, Aravind Ganesh, Jessalyn Kathryn Holodinsky, Mohammed Almekhlafi, Saman Fouladirad, Adam Frost, Lotus Yang, Robert Otani, Braedon Newton, Amit Persad, Sanchea Wasyliw, Brett R Graham, Gary Hunter, Aaron Gardner, Regan Cooley, Syed Uzair Ahmed, Lissa Peeling and Michael E Kelly in Interventional Neuroradiology
Footnotes
Acknowledgements
The OPTIMISE investigators and Canadian Stroke Consortium.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JO: consultant (Nicolab). Aravind Ganesh reports grants from CIHR, the Canadian Cardiovascular Society, Alberta Innovates, Campus Alberta Neuroscience, Government of Canada – INOVAIT program and New Frontiers in Research Fund, Microvention, Alzheimer Society of Canada, Alzheimer Society of Alberta and Northwest Territories, Heart and Stroke Foundation, Panmure House, Brain Canada, MSI Foundation, consulting fees from MD Analytics, MyMedicalPanel, Figure 1, CTC Communications Corp, Atheneum, DeepBench, Research on Mind, Creative Research Designs, AlphaSights, 42mr, honoraria from Figure 1, Alexion, Biogen, Servier Canada, expert testimony payment from Grosso Harper Law, travel support from AAN, Association of Indian Neurologists in America, American Heart Association, University of Calgary, patents pending US 17/317,771, editorial board memebership Neurology:Clinical Practice, Neurology, Stroke, Frontiers in Neurology, stock options from SnapDx and Collavidence Inc., participation in several clinical trials. Johanna Ospel is a consultant to Nicolab. The remaining authors have nothing to disclose.
Ethics approval
This study was approved by the ethics committee of the Royal University Hospital, Saskatoon (REB 23-06).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.