
Abstract
Objective
In this systematic review and meta-analysis, we investigated the efficacy and safety of middle meningeal artery embolization (MMAE) using particle embolic agents to treat cSDH.
Methods
To retrieve articles investigating outcomes of patients following MMAE with particle agents and to compare their outcome with conventional treatment, Scopus, PubMed, Embase, and Web of Science were searched using relevant keywords. Original articles with more than 10 cases were included. The meta-analysis was carried out using the R studio and the random-effects model. Publication bias was assessed using Peter's test and quality assessment using NIH tools.
Results
Eleven studies with 359 patients were included. The analysis revealed a pooled recurrence rate of 5% (CI: 3–8%), a need for reoperation rate of 5% (3–9%), and a peri-procedural complication rate of 4% (CI:2–9%) following MMAE with particle embolic agents. The pooled rates of decrease in size or resolution of the hematoma were 85% (CI:66–94%) and 66% (39–86%), respectively. Comparing MMAE using particulate embolysate with conventional treatments, risk ratio (RR) of 0.10 (CI:0.04–0.27) was achieved for recurrence, 0.25(CI:0.13–0.49) for reoperation, and 0.34 (CI:0.16–0.27) for peri-procedural complications. 91% of cSDH cases responded to MMAE with particles in the way they showed either down-sizing or complete resolution of the hematoma on follow-up imaging. In comparison, this rate was found to be 63% following conventional treatment.
Conclusion
Middle meningeal artery embolization using particle embolysates is a safe and effective technique for the treatment of cSDH, whether as a standalone intervention or in combination with conventional treatments.
Introduction
Chronic Subdural Hematoma (cSDH) has an incidence rate of 1.7 to 20.6 per 100,000 annually. 1 The incidence rate of this condition has been increasing over the recent decades and is more prevalent among the elderly population. 2 It is believed that brain trauma, even if minor, may lead to cSDH. 1 Traumatic injuries to the brain can disrupt the integrity of the dural border, leading to extravasation and accumulation of blood and fluid in the subdural space. 3 Meanwhile, the secretion of inflammatory cytokines is induced by blood accumulation, leading to worsening local inflammation and increased vascular permeability. These cytokines include tumor necrosis factor-α (TNF- α), interleukin-6 (IL-6), and IL-8. 4 On the other hand, the release of vascular endothelial growth factor (VEGF) and angiopoietin-2 induce angiogenesis and the formation of new capillaries. 5 Since these capillaries are fragile, extravasation and micro-bleedings occur, which leads to a vicious cycle.3, 6 Additionally, the inflammatory cytokines stimulate the local secretion of tissue plasminogen activator (t-PA) which induces a hyper-fibrinolytic state causing the exacerbation of the bleeding. 3 These cascades explain the cycle of persistent subdural hematoma.
The conventional approaches for evacuating hematoma have been proven effective in decompressing the brain and alleviating the symptoms. 7 However, potential complications and risk for hematoma or hygroma reformation are the biggest concerns associated with these surgical interventions. 8 Since the introduction of the middle meningeal artery embolization (MMAE) technique in 2000, there has been a rising trend toward the use of such methods to cease the middle meningeal artery (MMA) blood supply for the treatment of cSDHs. 9 This endovascular technique comprises the use of coils or other agents, including liquid or particle materials, to embolize MMA.10, 11 Several studies have reported the efficacy of such endovascular procedures in reducing the recurrence rate of cSDH as well as decreasing the size of the hematoma along with a low complication rate.12, 13
Particle embolic agents were first introduced in the 1970s and since then, they have been increasingly used for the embolization of various lesions, such as hepatic malignancies and pulmonary hemorrhages.14, 15 Promising outcomes have been reported following MMAE with particle embolizing agents with low rates of complications and remarkable efficacy, even though the aggregate effects were not completely determined. 16 Herein, we aim to systematically investigate the articles reflecting the outcomes, complications, and need for re-intervention in patients with cSDH who underwent MMAE with particle embolic agents.
Method
This study follows Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)-2020. 17
Eligibility criteria
Studies that evaluated the effect of MMAE with the use of particle embolic agents for the treatment of cSDH and reported clinical outcomes either in comparison with conventional treatment or as sole intervention were included. Non-English manuscripts, editorials, case reports and case series with less than 10 cases, letters to editors, and preprints were excluded.
Information sources, search strategy
PubMed, Scopus, Embase, and web of science were searched using the words “subdural hematoma”, its synonyms, and relevant keywords in combination with “middle meningeal artery” and “embolization” on March 2022. The only filter that was used in the search process was the title/abstract.
Article selection and data collection process
Two independent co-authors (AS and YO) collected the articles from the above-mentioned databases. Next, all the articles were entered into an Endnote library 18 and duplicates were omitted manually. A two-step screening process was initiated by these two co-authors independently. In the first step, the title and abstracts were screened. In the second step, full texts were evaluated whether the included articles met our eligibility criteria. Final articles were discussed between two co-authors and in case any conflicts were raised, results were discussed with another researcher (MA). Following this process, data collection was carried out by two independent researchers (AP and YO) who entered the data into an excel sheet, and in case incongruence was noted, another researcher (FA) was asked to re-examine the data. No automated tool was used for these processes.
Data items and risk of bias
Characteristics of the studies such as publication year, age of the patients, the location where the study was carried out, type of embolization, and also the clinical outcome measures including mortality, recurrence rate(New hematoma or increase the size of previous hematoma), procedural success rate, change in the size of the hematoma, re-operation rate (Surgical interventions such as craniotomy and hematoma evocation), and peri-procedural complications for both MMAE and conventional treatment(Surgical evacuation) groups were retrieved. The risk of bias was assessed using the proper type of National Institute of Health(NIH) tools for quality and risk of bias assessment. 19
Statistical analysis
R Studio software version 1.2.5042 (RStudio Team (2020). RStudio: Integrated Development for R. RStudio, Inc., Boston, MA) was used for performing the analysis. Random-effects model and “meta” package were used throughout the analyses. In comparing outcomes of MMAE vs conventional treatment, the effect size was reported as risk ratio (RR) and 95% confidence interval(CI) and for analysis aimed to calculate a single pooled effect size, proportion, and 95% CI were computed. Finally, all effect sizes were illustrated as a forest plot. Heterogeneity was calculated using I2 and publication bias was determined using Peter's test In the case that significant publication bias was noted, the trim and fill test was carried out to adjust the effect size, and if applicable, sub-group analysis was performed to minimize heterogeneity.
Results
Following the exclusion of duplicates out of 628 articles in the endnote library, 224 studies remained for screening. In toto, 11 studies met our eligibility criteria (Figure 1). 359 and 875 patients underwent MMAE and conventional treatment, respectively. The mean age of the patients in the MMAE group was 74.2 ± 4.34 and 73.12 ± 3.58 in the conventional treatment group. Overall, patients were followed for 124 ± 74 days(Table 1). Six out of 11 studies investigated the combination of MMAE with particle and conventional treatment, four investigated coiling after embolization with particle, and at last, two studies utilized Subdural Evacuation Portal System (SEPS) technique for drainage of hematoma. Four out of 11 studies compared MMAE with conventional treatment in terms of different outcome measures. No study was excluded due to poor quality in the quality assessment process. Polyvinyl alcohol (PVA) was the most common agent used for embolization in nine articles, while two others used Embosphere. The most common size of PVA and Embosphere used in these studies were 150–250 and 300–500 microns in diameter, respectively. The type of anesthesia used for MMAE varied between patients due to the choice of physicians and wasn't strictly stated. However, the anesthesia used in each study is grossly stated in part C of supplementary materials. (Table 1 and supplementary materials).
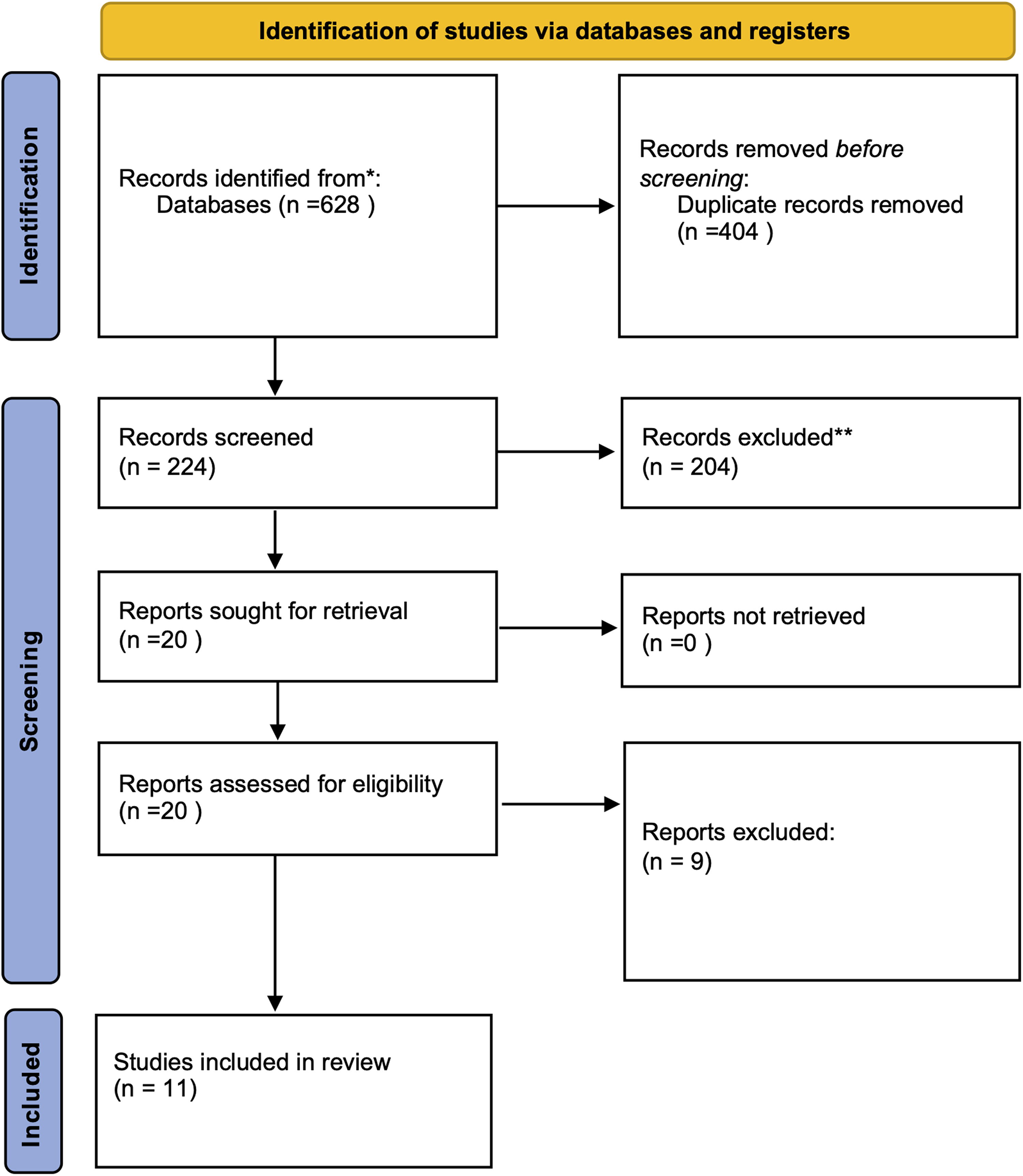
PRISMA flowchart of included studies illustrating the screening process.
Characteristics of included studies and their outcomes following treatment of SDH with particle embolization. .
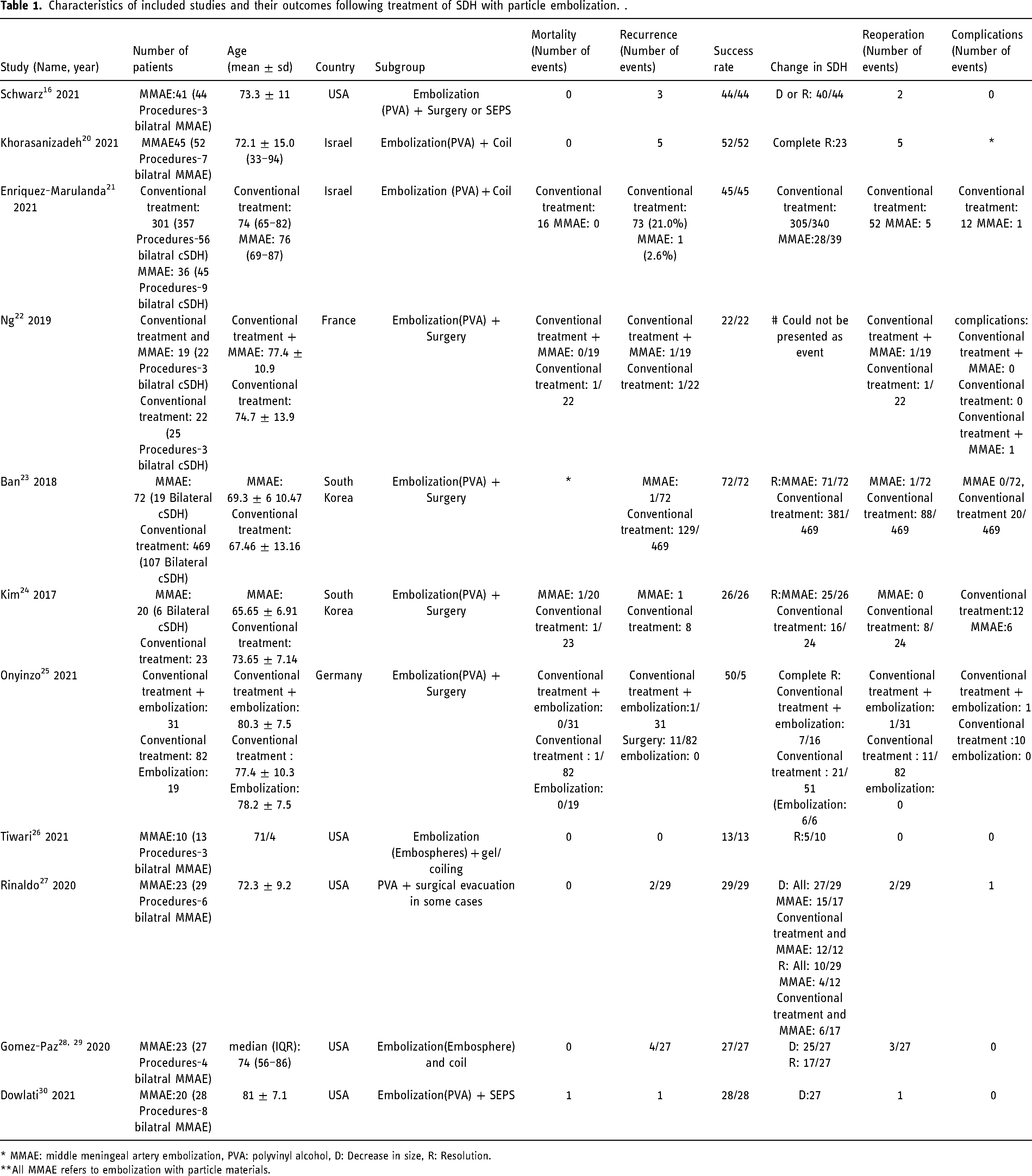
* MMAE: middle meningeal artery embolization, PVA: polyvinyl alcohol, D: Decrease in size, R: Resolution.
**All MMAE refers to embolization with particle materials.
In part 1, we have analyzed the outcome of patients who have undergone MMAE with particles as a single proportion. The pooled mortality rate was 1% (CI: 0–3%) along with a recurrence rate of 5% (CI: 3–8%), need for re-operation in 5% (3–9%) and peri-procedural complication rate of 4% (CI:2–9%). The overall procedural success rate of MMAE was 100% (CI:19–100%). The pooled rates of decrease in size and resolution of the hematoma following MMAE were 85% (CI:66–94%) and 66% (39–86%), respectively (Figure 2–4). Among the analyses, publication bias was significant for mortality and procedural success rates, which needed to be adjusted with the trim and fill test The mentioned adjusted rate was 3% (CI:0.2–4%) for mortality and 97% (CI:96–98%) for procedural success rate.
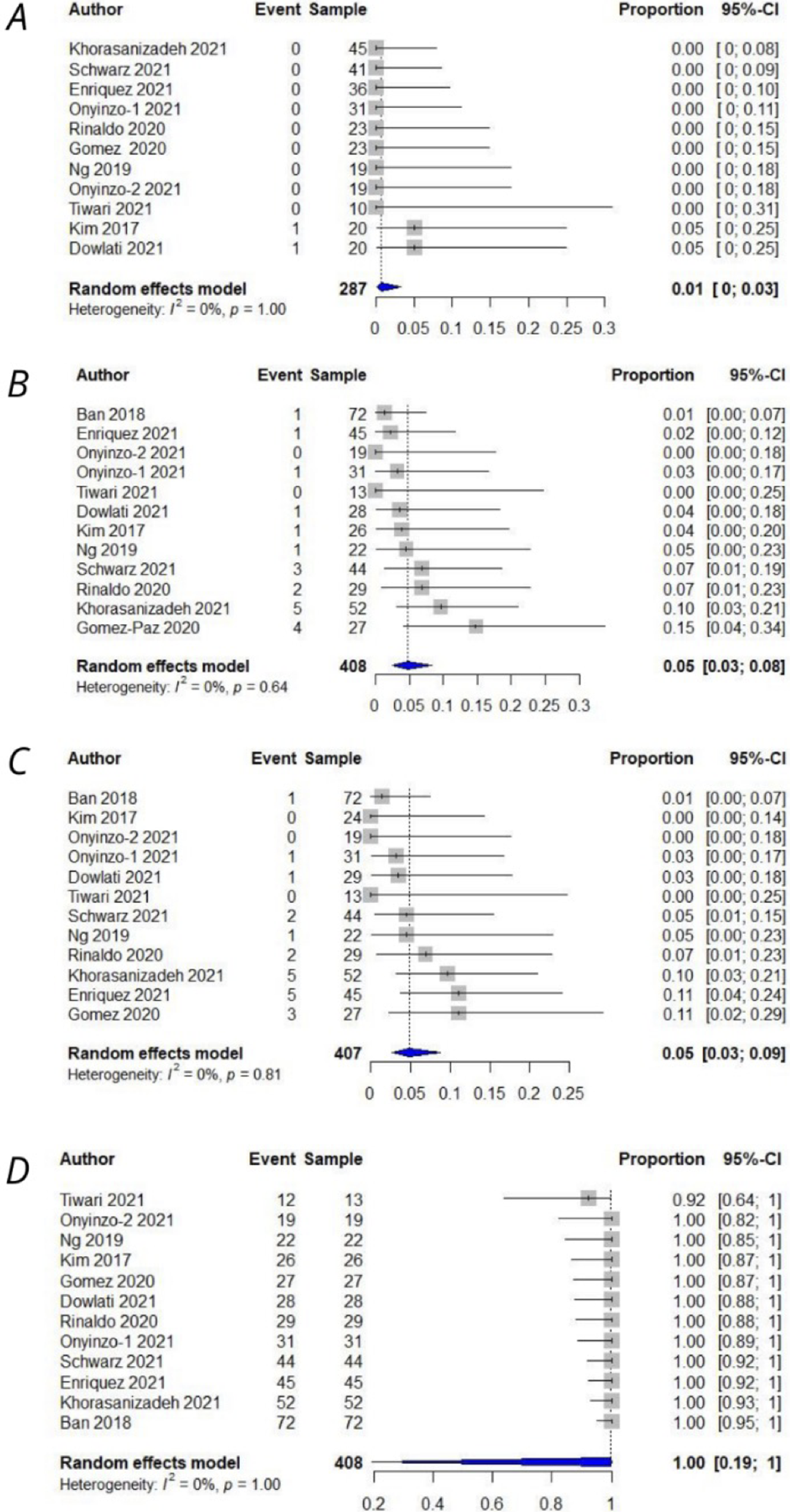
Meta-analysis of outcomes as a single proportion. A: Mortality rate (1%, CI:0–3%), B: Recurrence rate(5%, CI:3–8%), C: Reoperation rate(5%, CI:3–9%), D: Success rate(100%(CI:19–100).
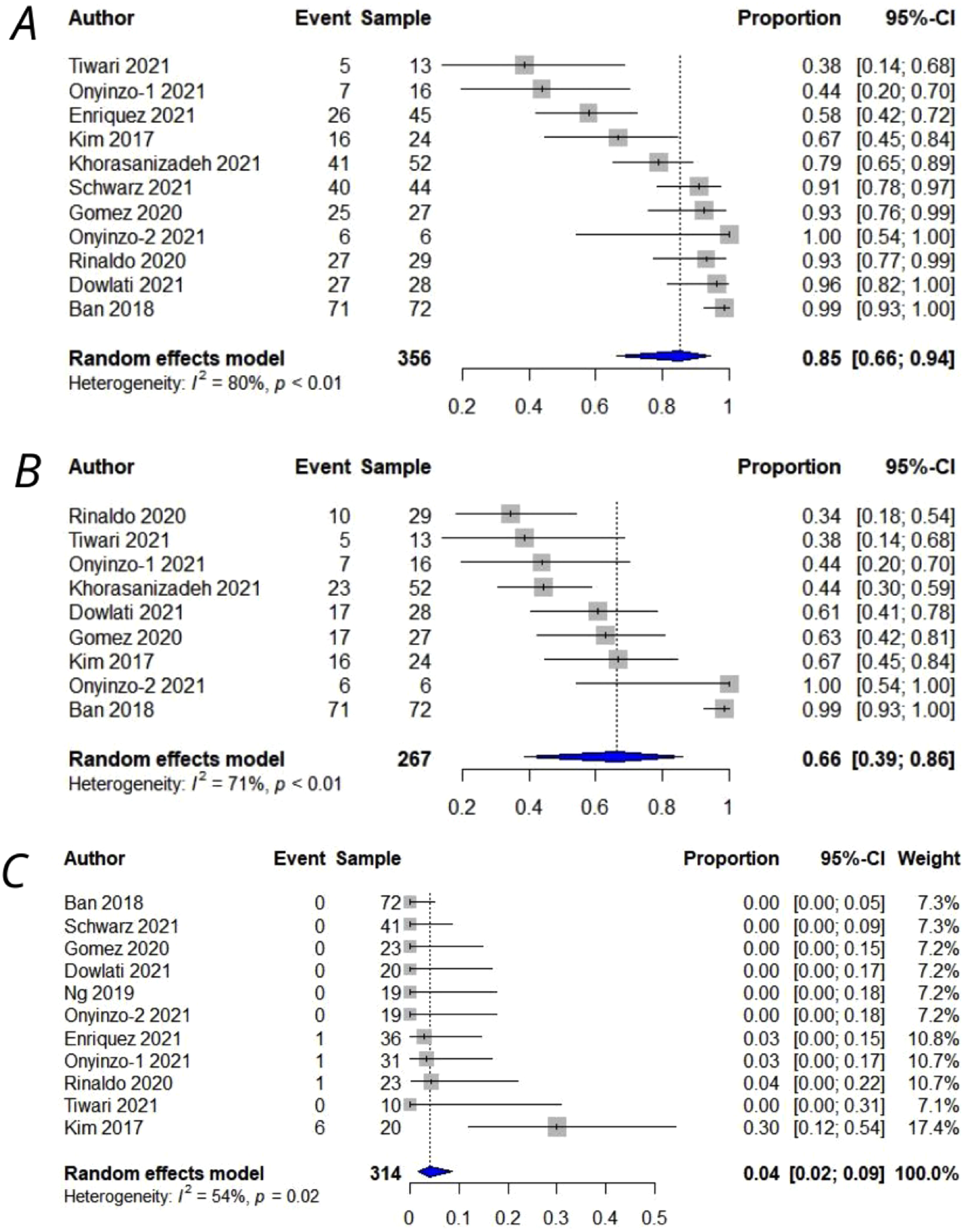
Meta-analysis of outcomes as a single proportion. A: Improve in the size of hematoma (85%, CI:66–94%), B: Resolution of hematoma (66%, CI:39–86%%), C: Complication rate (4%, CI:2–9%).
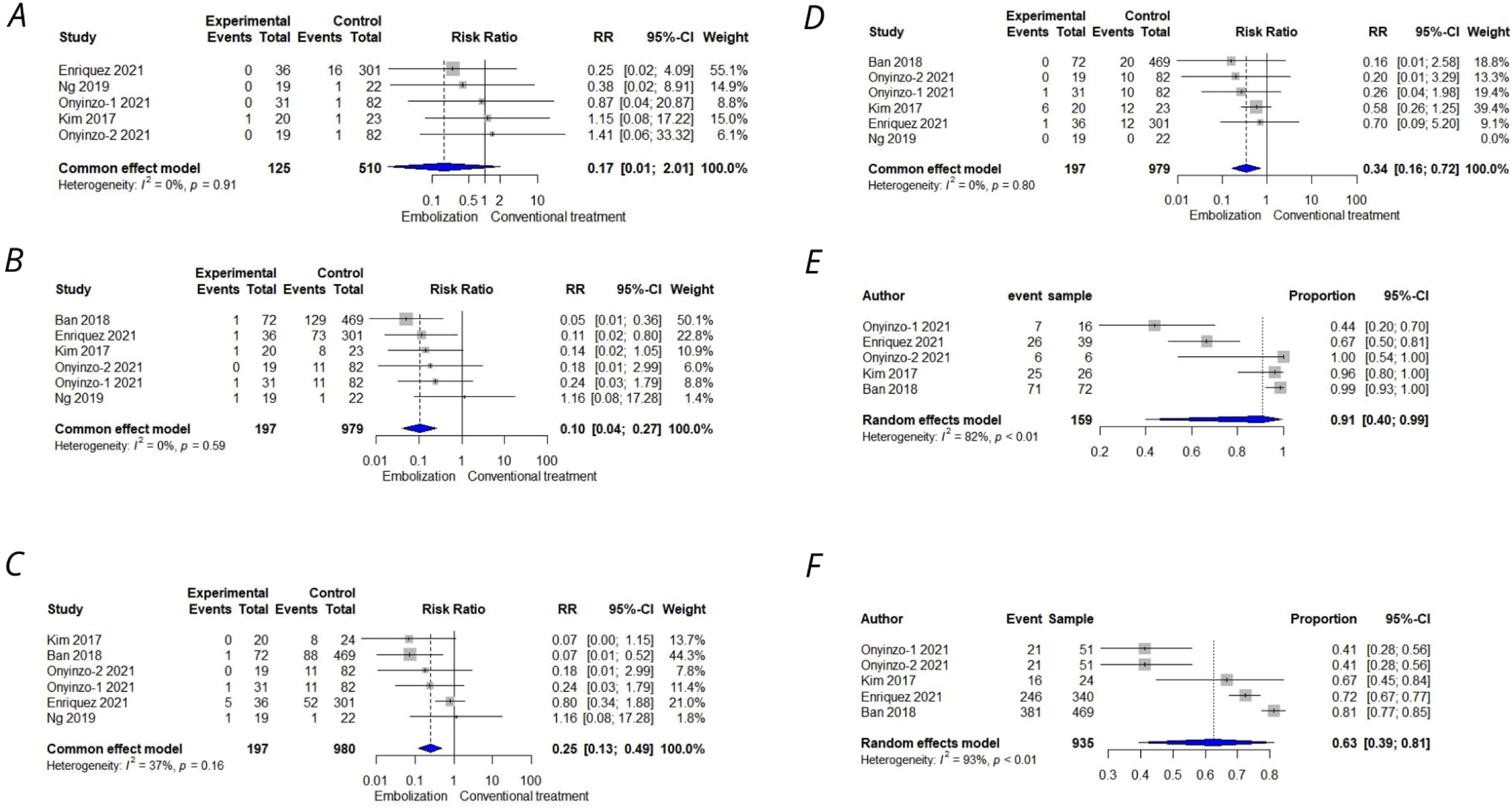
Meta-analysis of outcomes comparing MMAE to conventional treatment. A: Mortality(0.17, CI:0.01–2.01), B: Recurrence(0.10, CI:0.04–0.27), C: Reoperation(0.25,CI:0.13–0.49), D: Complication(0.34, CI:0.16–0.72), E: Decrease in size or resolution of hematoma following MMAE in studies comparing MMAE and Conventional treatment(91%, CI:40–99%), F: Decrease in size or resolution of hematoma following Conventional treatment in studies comparing MMAE and Conventional treatment(63%,CI:39–81%).
In part 2, when comparing particle MMAE with conventional treatment, all the following indices were analyzed amongst the two treatment modalities. RRs of 0.17(CI:0.01–2.01) for mortality, 0.10 (CI:0.04–0.27) for recurrence, 0.25(CI:0.13–0.49) for reoperation and 0.34(CI:0.16–0.27) for peri-procedural complications were calculated . The indices of decrease in hematoma size or the resolution of the hematoma were combined and analyzed for MMAE with particles and conventional treatment groups separately. This united index was reported 91% (40–99%) for MMAE for particles and 63% (39–81%) for conventional treatment.
Embolization procedure
Under general or monitored anesthesia care, femoral or radial artery access is obtained. A guide catheter is then advanced and placed into the external carotid artery.31, 32 Under the road mapping technique, a microcatheter preloaded with a microwire will be introduced and advanced into the guiding catheter, and the MMA will be selected with the microwire. Next, the microcatheter will be advanced selectively over the microwire and into the divisions of the MMA based on the decision of the physician. Then the microwire is removed, and the particles are infused slowly with caution until they reach the distal branches of the artery. Prior to the embolization, angiography is performed to assess dangerous anastomoses (e.g. ophthalmic artery anastomosis) to avoid unwanted embolization.33, 34 Also, before and after MMAE, angiography of anterior circulation is performed to ensure patency of cranial arteries. 34 MMAE is generally delayed or avoided in case the SDH is causing a significant midline shift requiring emergency neurosurgical evacuation. 31
Discussion
The present systematic review and meta-analysis is dedicated to evaluating the efficacy and safety profiles of MMAE using particle embolic agents to treat cSDHs. Our results indicate that MMAE with particle agents is a safe and effective procedure leading to lower chances of hematoma recurrence, particularly when compared to conventional neurosurgical treatments. 13
According to our findings, 91% of cSDH cases responded to MMAE with particles. They showed either down-sizing or complete resolution of the hematoma on follow-up imaging, while this rate was found to be 63% following conventional treatment. Therefore, MMAE with particles might be a more effective treatment option compared to conventional neurosurgical interventions in the management of cSDH. In contrast to our findings, Marulanda et al. reported no significant difference in terms of clinical outcomes between patients treated with MMAE (mostly using particles) and those who underwent conventional treatments. 21 However, definite conclusions may not be drawn from their study due to the small sample size.
The rates of peri-procedural complications and mortality were 4% and 1% among the patients who underwent MMAE with particles, respectively. These relatively low rates illustrate a reasonable safety profile for this endovascular procedure compared to conventional neurosurgical treatments, with reported complication rates ranging from 2.5% to 9.3%. 6 Seizure and stroke were among the reported complications occurring with MMAE with particles.
To validate our interpretations, we comparatively analyzed the incidence of complications among the patients who underwent MMAE with particles versus conventional treatment. Based on our analyses, the risk of mortality and peri-procedural complications decreased by 83% and 66%, respectively. These findings are not in line with a previously published meta-analysis by Srivatsan et al., who concluded that there is no significant difference in the peri-procedural complication rates between the two treatment methods. However, Srivatsan et al. did not categorize the use of liquid or particle embolic agents for MMAE. 13
The rate of recurrence of SDH was found to be 5% in follow-up imaging, with the need for reoperation in 5% of the cases. The reported estimated risk of recurrence was 2.4% and 3.6% in two previously published meta-analyses on MMAE.12, 35 However, the recurrence rate of SDH for various conventional neurosurgical treatments varied from 11.7% to 28.1%. 6 Based on RR calculation, we found out that the risk of recurrence decreased by 90% in patients who underwent MMAE with particles compared to those who underwent conventional treatments. This rate is 75% for reoperation. This finding might be explained by the fact that neurosurgical evacuation of the hematoma does not address the underlying pathology directly. On the other hand, MMAE prevents the reformation of hematoma by occluding the arterial feeding branches. Reducing the recurrence rate of cSDH is of substantial importance, as a 25-year retrospective cohort study showed recurrence of cSDHs is associated with an increased rate of neurological and non-neurological complications. 2
A recent meta-analysis by Jumah et al. on 11 studies and 177 cSDH patients showed that the incidence of peri-procedural complications of overall MMAE techniques was 1.2%, and treatment failure was 2.8%, which are relatively in line with our findings. 36 Furthermore, the risk of recurrence and peri-procedural complications with MMAE were reported to be 26% and 3.6% lower than conventional surgery, respectively 36
It is also noteworthy to know that since patients suffering from cSDH are usually the elderly with underlying comorbidities, they might not tolerate the invasive neurosurgical procedures and general anesthesia1, 37 MMAE could be a favorable treatment option for these patients, accordingly. Another advantage of MMAE is that this procedure might be feasible for the treatment of cSDH in patients with co-existing coagulopathy when conventional neurosurgical treatment would be too risky 32
Particle embolic agents treatment techniques
Particle embolic agents are the most widely used agents for MMAE. Polyvinyl alcohol (PVA) is the most commonly used particle for MMAE and is available in various sizes, ranging from 90 to 2800 µm. When PVA is infused into the artery, it causes inflammation, angionecrosis, and subsequent thrombosis, leading to vessel occlusion14, 38 PVA is generally cheaper and more cost-effective than liquid embolic agents11, 33 However, liquid embolic agents are generally infused faster and simpler. They can also penetrate the vessels more deeply compared to particles. Last but not least, the liquids’ effect persists longer because the tissue cannot reabsorb liquids, unlike particles 11
Although there are advantages and disadvantages to the use of liquid and particle embolic agents for MMAE, there is some evidence that there is no significant difference between the two in terms of efficacy, complications, procedure duration, and fluoroscopy radiation dose.12, 39, 40
Some studies carried out adjuvant treatment added to MMAE. If the patient has symptoms related to cSDH, performing hematoma evacuation may be inevitable. Twist drill, burr hole craniostomy, and a new, less invasive technique called Subdural Evacuation Portal System (SEPS) are among surgical hematoma drainage procedures. According to Lee et al., twist drill and burr hole craniostomy procedures showed no significant difference in outcomes for patients with cSDH. 1 For the first time, Dowlati et al. utilized SEPS in combination with MMAE as a primary treatment for cSDH patients. The authors of this study preferred this technique since it was less invasive with approximately equal outcomes compared to craniostomy. 2 Some studies investigated the simultaneous application of coiling with particle embolization. We found no previous studies comparing coiling after particle embolization and craniostomy or particle embolization alone.3, 4 Due to the insufficient number of studies, we could not compare particle embolization alone and in combination with surgery, SEPS, or coiling statistically. However, patients who have undergone surgical evacuation and embolization with particle agents may have better outcomes and fewer complications compared to others, even though not statistically proven. More studies are needed to consolidate these results.
Future direction
We found four ongoing clinical trials that aim to evaluate outcomes and complications of MMA embolization with particle agents. Three out of these four trials are randomized controlled trials (RCTs) and the other study is an open-label clinical trial. Including 154 patients in Germany, MEMBRANE trial is going to randomize patients into surgical evacuation and combined coiling and embolization with PVA in patients with newly diagnosed cSDH. 41 In another RCT, based in the Netherlands, ELIMINATE study is conducted on 170 patients divided randomly into two discrete groups of surgical evacuation and embolization with PVA. 42 EMMA-Can will evaluate the application of liquid or particle embolic agents in 200 patients randomly assigned into standard treatment groups (i.e. surgical drain or medical treatment) and MMA embolization in Canada. 43 The last trial investigates 600 patients in four arms that are Embolization with PVA, combined embolization and surgical evacuation, medical management, and surgical evacuation alone. 44 These aforementioned trials will be completed between July 2023 and December 2025 and afterwards, perhaps sufficient data could be available to consolidate our understanding of these embolic materials.
Limitation
The major limitation of this meta-analysis is the heterogeneity of our results. This is mostly due to differences between the included studies in terms of the cases, the duration of follow-up, and the techniques applied besides particle embolization (e.g. coiling). Another limitation of this study was the scarcity of studies to be used in subgroups analysis for comparing outcomes of patients who have undergone embolization with particle embolization agents alone and in combination with coil or surgical drain. It could be implemented from our analysis that reported outcomes were not similar. The development of unified indexes for reporting outcomes and complications of patients would be more helpful for deciding for patients. Regarding the technical aspects of embolization with particle agents, particle size, particle brand, microcatheter tip location, and sequence of embolization, whether frontal or parietal branches of MMA are embolized, all matter. Unfortunately, the included studies did not provide enough data to address these issues. We hope there'd be more thorough explanations in future studies.
Conclusion
The safety and efficacy of MMAE for the treatment of cSDH using particle agents such as PVA have been reviewed systematically, and a meta-analysis was performed. MMAE with particles leads to remarkable rates of hematoma size decline or resolution alongside low risks of complication. More importantly, the rate of recurrence, which is a significant challenge following treatment of cSDH with conventional surgeries, is lower.
Supplemental Material
sj-docx-1-ine-10.1177_15910199221125977 - Supplemental material for Particle embolic agents for embolization of middle meningeal artery in the treatment of chronic subdural hematoma: A systematic review and meta-analysis
Supplemental material, sj-docx-1-ine-10.1177_15910199221125977 for Particle embolic agents for embolization of middle meningeal artery in the treatment of chronic subdural hematoma: A systematic review and meta-analysis by Saeed Abdollahifard, Amirmohammad Farrokhi, Omid Yousefi, Adib Valibeygi, Pouria Azami and Ashkan Mowla in Interventional Neuroradiology
Footnotes
Contribution
All authors contributed to developing the idea, writing the draft, and finalizing the manuscript.
Disclosure,funding,and conflict of interest
Ashkan Mowla: Speakers Bureau/Consultant to Cerenovus, Stryker, Wallaby Medical, RapidAI, BALT USA,LLC. Others have no disclosure.
Supplemental material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.