
Abstract
Background
To identify an association between morphological parameters and the rupture risk of anterior communicating artery (ACoA) aneurysms using propensity score matching (PSM).
Methods
Data for 109 patients with ACoA aneurysms treated from January 2018 to October 2021 were reviewed; 94 patients were enrolled. The geometrical parameters of the ACoA aneurysms were measured and calculated using three-dimensional reconstructed digital subtraction angiography images. The aneurysms’ morphological parameters were analyzed using a propensity score for six factors (age, sex, excess alcohol intake, smoking, hypertension, diabetes mellitus). Univariate logistic regression was used to analyze the relationship between the aneurysms’ morphological parameters and rupture risk.
Results
Twenty-five patients each with or without ruptured aneurysms were selected. After matching, no statistically significant differences were seen between the groups in their baseline characteristics. Aneurysm neck size (p = 0.038) was higher in the unruptured group than that in the ruptured group, and the dome-to-neck ratio (D/N; p = 0.009) and aspect ratio (AR; p = 0.003) were higher in the ruptured group than those in the unruptured group. Univariable logistic regression analysis demonstrated that ACoA aneurysm rupture was associated with AR (odds ratio: 8.047; 95% confidence interval: 1.569–41.213; p = 0.012) and D/N (odds ratio: 4.253; 95% confidence interval: 1.228–14.731; p = 0.022). The areas under the receiver operating characteristic curves for AR and D/N were 0.746 and 0.715, respectively.
Conclusions
After PSM, ACoA aneurysms with higher AR and D/N, and smaller neck size were more likely to rupture. AR may be a much more important predictor of aneurysm rupture than other predictors.
Introduction
An increasing number of unruptured aneurysms have been identified with advancements in imaging technology.1,2 In the adult population, the incidence of unruptured intracranial aneurysms is 3%, and anterior communicating artery (ACoA) aneurysms account for the majority of intracranial aneurysms at approximately 30%.3,4 The incidence of spontaneous subarachnoid hemorrhage is approximately 0.0091%; however, ruptured intracranial aneurysms account for 85% of all cases. 5 Although the incidence of intracranial aneurysms does not appear high, the mortality rate associated with aneurysmal arachnoid hemorrhage can be higher than 30%. 6 Investigating the risk factors for ACoA aneurysm rupture is important because of the dismal outcomes secondary to rupture. 7
There is still insufficient evidence regarding which morphological parameters play critical roles in aneurysm rupture, and most previous studies did not consider the consistency of patients’ baseline data in group comparisons. Determining which morphological parameters are risk factors for aneurysm rupture will be beneficial in the selection of aneurysm treatment. In this study, we used propensity score matching (PSM) to reduce the impact of baseline data imbalances on the outcomes to identify the morphological factors related to aneurysm rupture.
Materials and methods
Ethics statement
This study was approved by our Hospital Institutional Review Board. The need to obtain written consent from the patients was waived by the Institutional Review Board.
Patient selection
Patients who were diagnosed as having intracranial aneurysm(s) in our Hospital Information System between January 2018 and October 2021 were retrospectively screened. All patients with ACoA aneurysms were included, and we excluded patients without digital subtraction angiography (DSA) images. Fifteen patients were excluded and, thus, 94 patients met the above criteria.
Definition and measurement of the morphological parameters
The morphological parameters of the aneurysms were measured from three-dimensional DSA images. Figure 1 shows the measured vascular parameters. We measured the aspect ratio (AR; defined as the ratio of the maximum perpendicular height to the cross-section of the aneurysm neck), flow angle (defined as the angle between the centerline of the parent artery and the line indicating the aneurysm size), aneurysm dome (defined as the maximum diameter of an aneurysm), neck size (defined as the maximum diameter of the cross-section at the neck of the aneurysm), and aneurysm width (defined as the longest line segment formed when the vertical line of the aneurysm size intersects the aneurysm wall). 8 We used the ratio of the length of the aneurysm to the mean diameter of the parent artery as the size ratio. The parent artery mean diameter was defined as the average diameter of the anterior cerebral artery on both sides of the aneurysm. Aneurysm size was defined as the maximum distance from the midpoint of the aneurysm neck to the apex of the aneurysm. We defined the aneurysm height as the maximum distance from a vertical line through the aneurysmal neck to the top of the aneurysm.
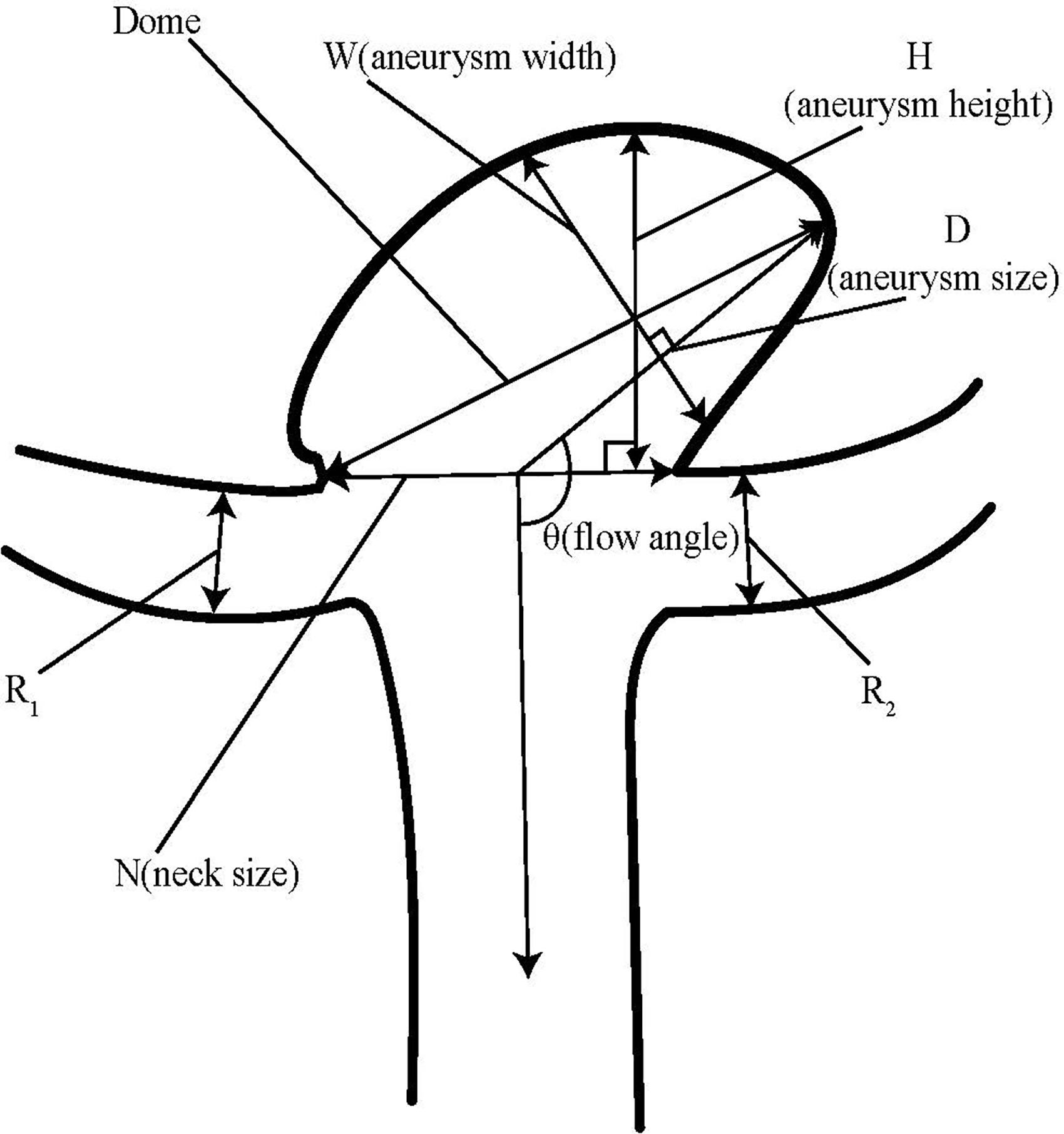
Diagram of the measured vascular parameters.
Statistical analysis
Categorical data, expressed as frequencies and percentages, were compared by Pearson's chi-square or Fisher's exact test All continuous variables are expressed as medians and interquartile ranges, and were compared by the Mann–Whitney U test PSM was performed using nearest-neighbor matching with a caliper width of 0.1. All statistical and PSM analyses were performed using R (version 4.1.2; www.r-project.org) and SPSS software (version 22.0; IBM Corp., Armonk, NY, USA).
After 1:1 matching for age, sex, excess alcohol use, smoking, hypertension, and diabetes mellitus, there were 25 patients in the ruptured aneurysm group and 25 in the unruptured aneurysm group. The effect of the morphological parameters on aneurysm rupture risk was analyzed using univariate logistic regression.
Results
Of the 109 patients with ACoA aneurysms treated between January 2018 and October 2021, 94 patients were enrolled. Table 1 and Table 2 show the patients’ demographic characteristics and clinical characteristics. After PSM, 25 patients each with or without ruptured aneurysms were selected (Figure 2). The patients comprised 30 females and 20 males, with a median age of 59.5 years. After we performed all propensity score matches, the baseline covariates (age, sex, excess alcohol use, smoking, hypertension, diabetes mellitus) were compared between the groups (Table 2). Among all clinical factors, P values after matching were >0.05.
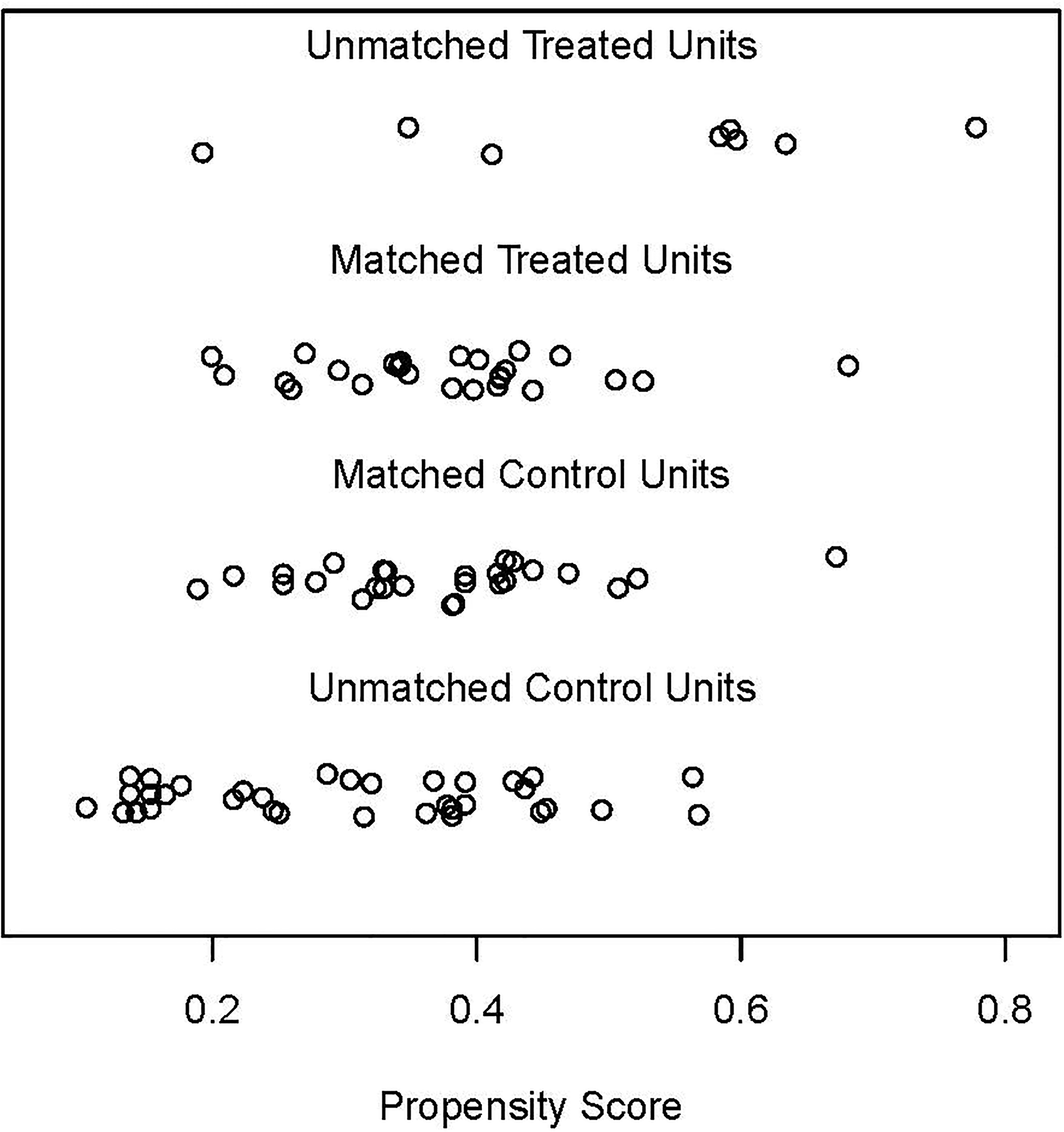
Distribution of propensity score matches for matched and unmatched patients.
Characteristics of 94 patients with ACoA aneurysms.
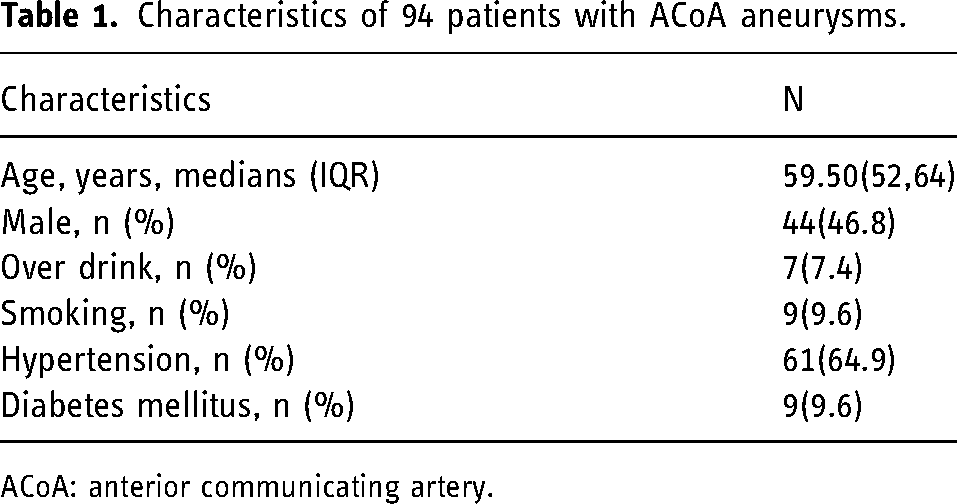
ACoA: anterior communicating artery.
Characteristics of 50 patients with ACoA aneurysms after propensity score matching.
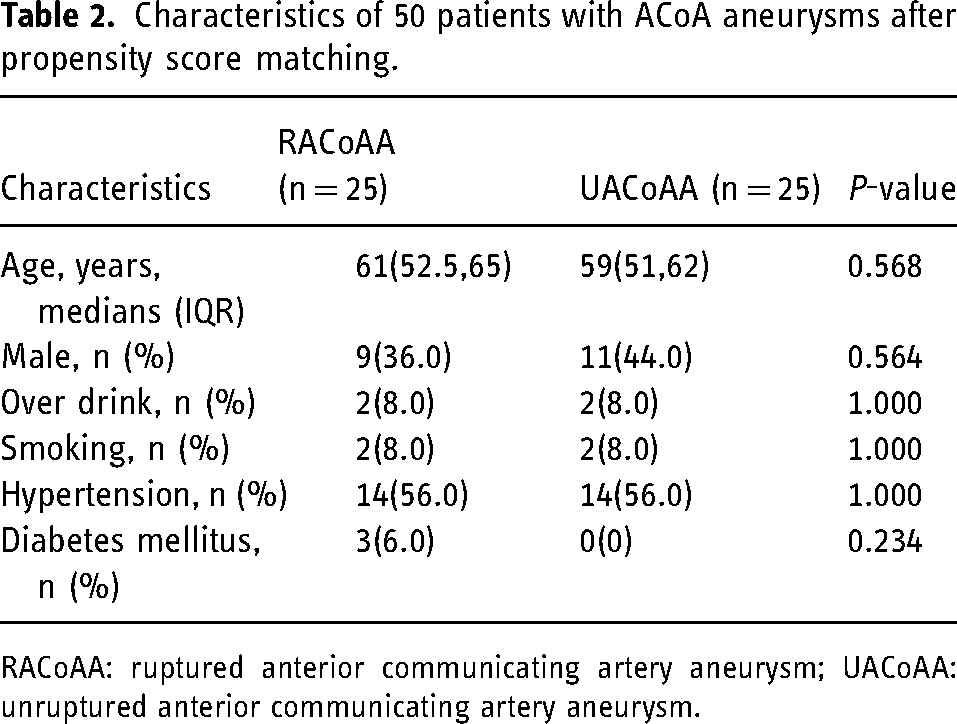
RACoAA: ruptured anterior communicating artery aneurysm; UACoAA: unruptured anterior communicating artery aneurysm.
Compared with the unruptured group, aneurysms had larger AR and D/N, and smaller neck size in the ruptured group that those in the unruptured group on the basis of the Mann–Whitney U test results (Table 3). The remaining morphological parameters showed no statistically significant differences between the two groups.
Morphological characteristics of the aneurysms after propensity score matching.
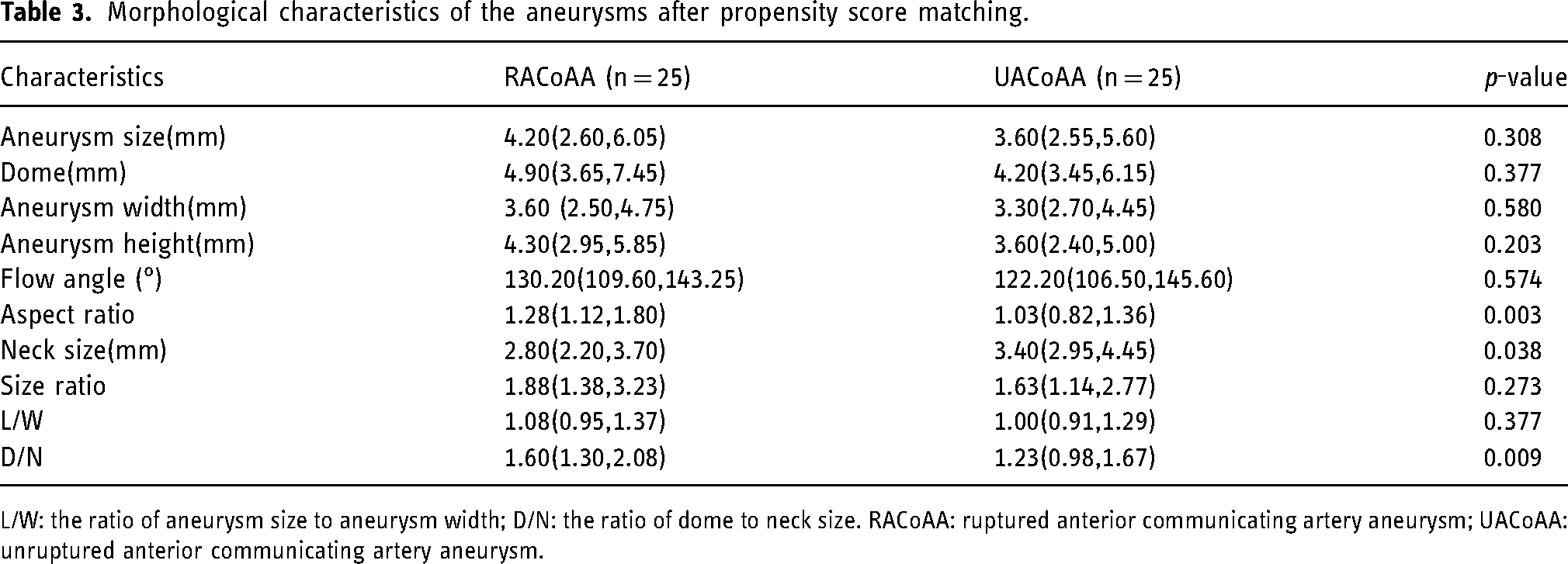
L/W: the ratio of aneurysm size to aneurysm width; D/N: the ratio of dome to neck size. RACoAA: ruptured anterior communicating artery aneurysm; UACoAA: unruptured anterior communicating artery aneurysm.
The results of the regression analysis for predicting aneurysm rupture are presented in Table 4. Univariable logistic regression analysis demonstrated that AR (odds ratio: 8.047; 95% confidence interval (CI): 1.569–41.213; p = 0.012) and D/N (odds ratio: 4.253; 95% CI: 1.228–14.731; p = 0.022), were significantly related to the rupture of ACoA aneurysms. Our results showed that the ratio of aneurysm size to aneurysm width, aneurysm width, aneurysm height, size ratio, flow angle, and aneurysm size were not statistically significantly associated with aneurysm rupture.
Univariate and multivariate logistic regression analysis of morphological parameters for aneurysm.
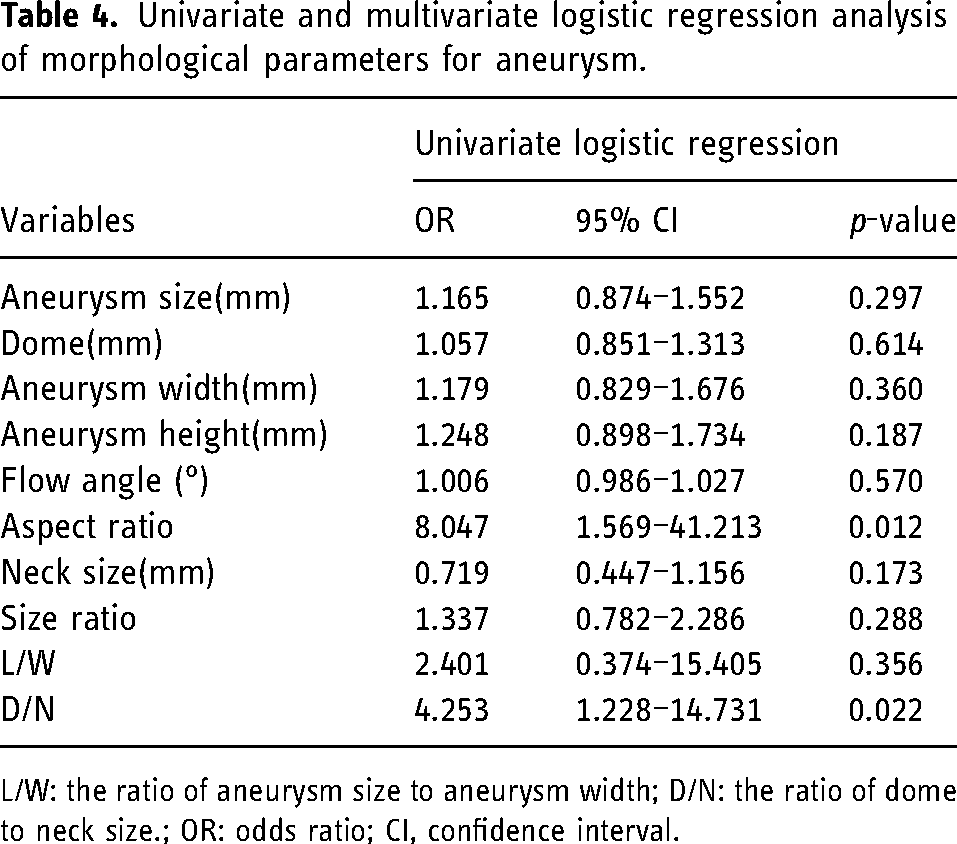
L/W: the ratio of aneurysm size to aneurysm width; D/N: the ratio of dome to neck size.; OR: odds ratio; CI, confidence interval.
The areas under the receiver operating characteristic curves for AR and D/N were 0.746 (95% CI: 0.610–0.881; p = 0.003) and 0.715 (95% CI: 0.573–0.858; p = 0.009), respectively (Figure 3). The cut-off values for AR and D/N were 1.089 (64% specificity and 80% sensitivity) and 1.289 (56% specificity and 80% sensitivity), respectively (Table 5).
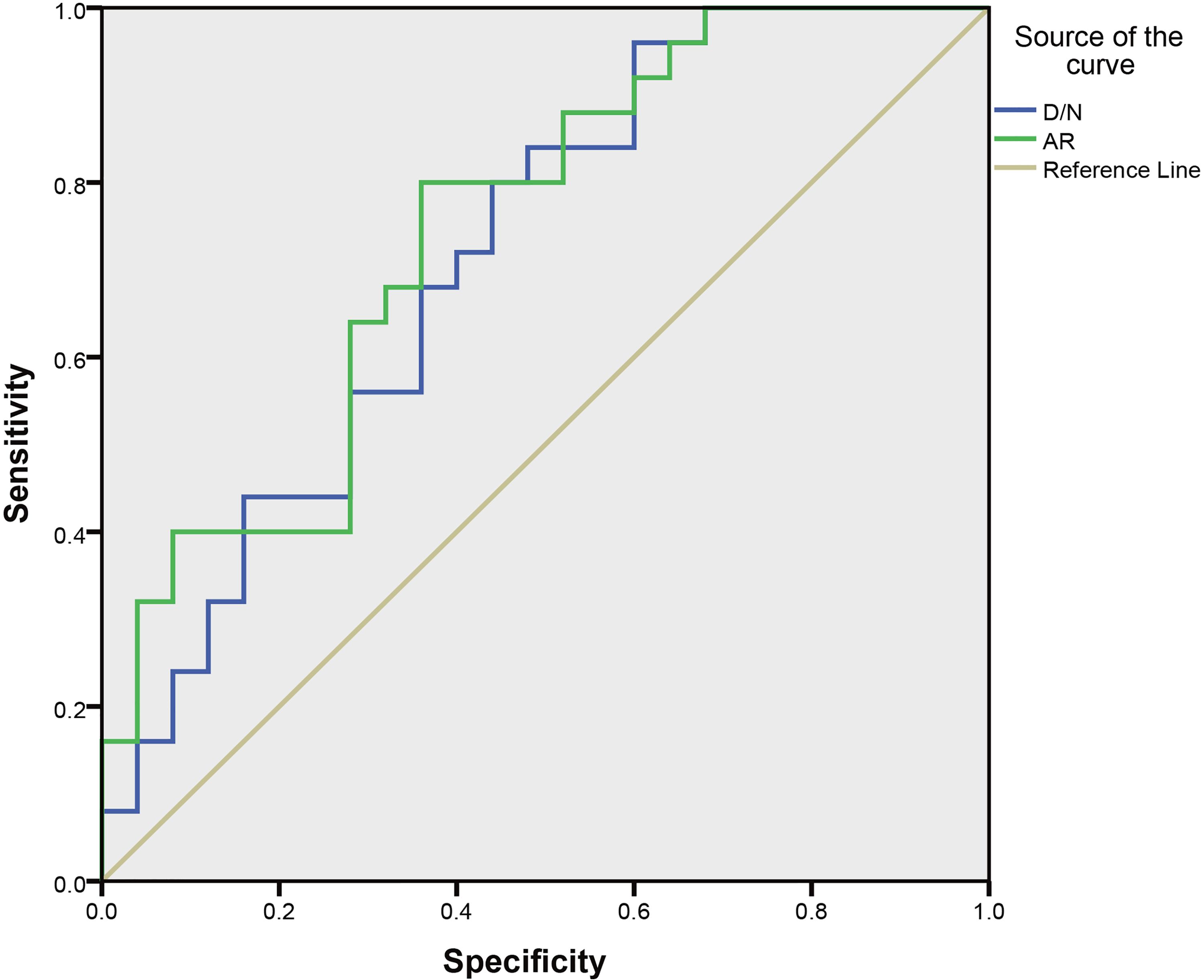
Areas under the receiver operating characteristic curves for ar and d/n. AR: Aspect ratio, D/N: Dome-to-neck ratio.
Area under the curve for AR and D/N.

AUC: the area under the curve.
Discussion
Some clinical trials have proposed that aneurysm rupture is associated with a variety of factors, such as AR, size ratio, neck size, flow angle, aneurysm location, wall shear stress (WSS), WSS gradient, smoking, and irregular shape.9–15 However, there is still no clear evidence indicating which morphological parameter is more relevant to aneurysm rupture risk. In this study, using PSM, we obtained further evidence that aneurysm rupture is related to morphological parameters.
In accordance with previous studies, we used PSM to balance the patients’ baseline characteristics and exclude known risk factors. The PHASES study, which was a pooled analysis of six prospective cohort studies, demonstrated that age and hypertension were independent risk factors for aneurysm rupture. 12 Regarding sex, one study showed that female patients were more prone to aneurysm rupture; 16 however, the study was conducted by a Japanese research team, and whether the results are applicable to other countries still needs to be confirmed in further studies. Previously, Etminan and Rinkel 17 et al. found that smoking and hypertension were associated with aneurysm rupture. In the current study, PSM was used to balance these risk factors between the ruptured and unruptured ACoA aneurysm groups.
To our knowledge, this is the first study to use PSM to analyze the morphological factors associated with anterior communicating aneurysm rupture. In previous analyses of the morphological factors associated with ACoA rupture, most parameters were measured by computed tomography angiography;18,19 in this study, DSA data were used for more accurate measurements. Aneurysm size, flow angle, and size ratio have been reported to be associated with aneurysm rupture in previous studies;18–20 however, these factors were not found to be statistically significantly associated with aneurysm rupture in the present study. Our study found that the median and mean size ratio, flow angle, and aneurysm size were higher for ruptured aneurysms than those for unruptured aneurysms, although there was no statistically significant correlation between the factors and rupture risk. This may be related to the small sample size or different measurement methods in this study.
D/N was defined as the ratio of the maximum diameter of an aneurysm dome to neck size. D/N is usually used to determine if an aneurysm has a wide neck (dome-to-neck ratio < 2 or neck ≥ 4 mm). Few studies have reported that D/N is a risk factor for aneurysm rupture. When the maximum diameter of an aneurysm remains unchanged, smaller neck size is associated with higher D/N, which may affect aneurysm rupture owing to the influence of the aneurysmal neck. In the ARETA study, which was a prospective, multicenter study, smaller neck size appeared to be associated with aneurysm rupture. 21 A wide neck is usually recognized as a risk factor for aneurysm recanalization after coil embolization, 22 and a protective effect against aneurysm rupture has not been reported.
AR was first reported by Ujiie et al. 23 and was defined as the ratio of the maximum perpendicular height to the cross-section of the aneurysm neck. Ujiie et al. 23 reported that an AR > 1.6 is associated with aneurysm rupture. Recently, several studies have also reported that aneurysm rupture is often associated with high AR.10,24–26 Multiple studies have confirmed that the risk of rupture is significantly increased when AR is greater than a certain ratio; however, there is no unified standard for the cut-off value for AR, with proposed cut-off values of 1.4 27 and 1.6. 23 Our data showed that the cut-off between ruptured and unruptured ACoA aneurysms was 1.09, which was smaller than the cut-off reported in previous studies. Previously, Qiu et al. 27 reported that narrow-necked aneurysms (AR ≥ 1.4) had lower mean aneurysm WSS, which is associated with vascular endothelial cell injury. 28 Therefore, lower neck size or greater dome size and larger D/N and AR are associated with a higher risk of aneurysm rupture. Our study provides more plausible evidence of the association between these morphological parameters and ACoA aneurysm rupture. Therefore, when encountering a patient with an unruptured ACoA aneurysm, we can first evaluate the possibility of aneurysm rupture by DSA imaging, and if the aneurysm has a high AR (AR > 1.09) and D/N (D/N > 1.29) and a small neck size, the aneurysm requires prompt surgical treatment.
There are some limitations in the present study. First, the retrospective design might have generated bias in the data collection and statistical analysis. Second, the morphological parameters in this study were measured by an experienced neurointerventionist using three-dimensional subtraction angiography images; automatic machine measurements may reduce bias. Third, our analysis of aneurysm morphology was based on the assumption that aneurysm shape does not change before and after rupture. However, aneurysm morphological changes may occur after aneurysm rupture. 29 Fourth, after PSM, the sample sizes of the patients are usually decrease compared with the original sample sizes because unmatched patients are often removed from the dataset. This may have a negative impact on the final study conclusions in this study owing to the small initial sample size that we used. Furthermore, our conclusions were derived from analysis of ACoA aneurysms, which may not apply to aneurysms in other locations. Finally, further studies with larger ACoA aneurysm cohorts are necessary to confirm our results.
In conclusion, after PSM, ruptured ACoA aneurysms showed a significantly higher AR and D/N but a smaller neck size than those of unruptured ACoA aneurysms. These morphological parameters can predict the risk of aneurysm rupture in ACoA aneurysm patients who choose conservative treatment.
Footnotes
Acknowledgements
Author contributor statement
Chencheng Ma: Data curation, Writing- Original draft preparation, Methodology; Lei Mao: Conceptualization, Methodology; Guangjian Zhang: Software, Validation; Yuqi Shen: Software, Validation; Hanxiao Chang: Visualization, Investigation; Zheng Li: Supervision; Hua Lu: Writing- Reviewing and Editing.
Ethics statement
This study was approved by Institutional Review Board of Jiangsu Province Hospital. The need to obtain written consent from the patients was waived by the Institutional Review Board.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China, Natural Science Foundation of Jiangsu Province, (grant number No. 81901258, No. H2017022).