
Abstract
Background
Transradial access (TRA) is becoming more popular in neurointerventional radiology procedures and has been associated with reduced mortality, morbidity and access site complications. Guidelines state that TRA is a feasible option for posterior circulation thrombectomy however the evidence base is limited and no systematic literature review has yet been undertaken to evaluate its safety and efficacy.
Methods
The Cochrane Library, PubMed, Web of Science, Scopus, TRIP and Embase databases were searched. Outcomes collected included TICI scores, puncture to recanalisation time, mRS scores at 90 days and access site complications.
Results
291 records were identified and 31 full text articles were assessed for eligibility. Eight studies met the inclusion criteria and were meta-analysed. The rate of TICI 2b-3 was 94.7% (89.7–99.8% at 95% CI), TICI 3 was 67.9% (42.2–93.6% at 95% CI) and mRS 0–2 at 90 days was 49.8% (31.5–68.1% at 95% CI). Median puncture to reperfusion times were extracted from three studies as 24 (IQR 18–40), 24 (IQR 17.5–56.5) and 27 (IQR 24–33.5) minutes. No access site complications were reported. TICI 2b-3, TICI 3 and mRS scores were comparable to data for transfemoral access (TFA) from a large systematic review. Puncture to recanalisation times appeared lower than the TFA data but statistical comparison of this outcome was not possible.
Conclusions
The use of TRA in posterior circulation thrombectomy is safe and effective with comparable results to TFA. Further research with a larger sample size is required to fully investigate the potential for shortened puncture to recanalisation times.
Background
The femoral artery is the current standard access site for both cerebral angiography and neurointerventional procedures. 1 Numerous interventional cardiology trials have demonstrated that transradial access (TRA) reduces mortality, morbidity, access-site complications and hospital cost compared to transfemoral access (TFA)2–6 which has led to a change in the European guidelines for cardiac procedures which now recommend TRA as the default access for percutaneous coronary interventions. 7 A review 8 of prospective trials found major access site complications in mechanical thrombectomy patients undergoing TFA was 1.7% with a total complication rate of 4.6%. A systematic review 9 of 1342 patients undergoing neurointerventions performed via TRA found a major complication rate of 0.2% and total complication rate of 2.9%. As well as reduced complication rates, vertebral artery interventions, such as posterior circulation thrombectomy, may be more straightforward with TRA than TFA 10 as this approach can often be facilitated by the natural origin of the vertebral artery from the subclavian artery. 11 If this results in shorter procedure times then it could represent a positive impact on outcomes in these patients.
Nevertheless uptake in TRA for ischaemic stroke intervention appears low with 0.3–4.5% of patients undergoing thrombectomy via TRA. 12 In their ‘Current endovascular strategies for posterior circulation large vessel occlusion stroke’ report, the Society of Neurointerventional Surgery Standards and Guidelines Committee state that transradial access may be considered as an alternative to TFA given anatomic advantages 13 however this conclusion is only based on evidence from one study of 9 patients. 11 Furthermore, while there have been systematic literature reviews and meta-analyses covering TRA in mechanical thrombectomy in general14–16 there are no such reviews published using studies and data solely from posterior circulation thrombectomy groups despite the unique challenges and advantages of TRA in these cases.
Methods
Literature search
Databases searched were Cochrane Library, PubMed, Web of Science, Scopus, TRIP and Embase. The same search terms and bracket grouping and Boolean operators were used for each database as follows:
((Radial) OR (Transradial) OR (Radial artery)) AND ((Approach) OR (Access) OR (Puncture)) AND (thrombectomy) AND ((posterior circulation) OR (vertebral) OR (basilar) OR (vertebrobasilar) OR (posterior cerebral artery))
Search terms were applied to ‘All Fields’. The search terms and strategy were intentionally broad in order to find results which included studies of TRA in mechanical thrombectomy which had posterior circulation subgroups with extractable data.
Abstracts and titles were screened and subsequent full text articles were reviewed independently by two reviewers and any discrepancies discussed and resolved. After this, all relevant data were extracted by the first reviewer using a standardised spreadsheet and checked for errors by the second reviewer.
Inclusion and exclusion criteria
Retrospective and prospective studies, case control and case series were included. Case reports, conference abstracts and non-English language studies were excluded. Studies were also excluded if they did not use TRA first-line or did not have extractable data, such as those containing data for both anterior and posterior circulation thrombectomies where the posterior circulation subgroup's data were not presented separately or could not be obtained from the authors.
Data extraction and quality assessment
Demographic data were collected including number of subjects, percentage male, mean age and thrombus location. Quality assessment of the studies was performed using the National Institutes of Health Quality Assessment Tool for Case Series. 17
Extractable data of interest to the meta-analysis were divided into three main categories; technical, clinical and safety outcomes. Outcome measures were subdivided into those which were conditional for inclusion in the meta-analysis and other measures which were of additional interest and could be analysed if sufficient studies contained them (Table 1). Only one of the conditional outcomes needed to be met for the study to be included.
Outcomes required for inclusion and additional interest.
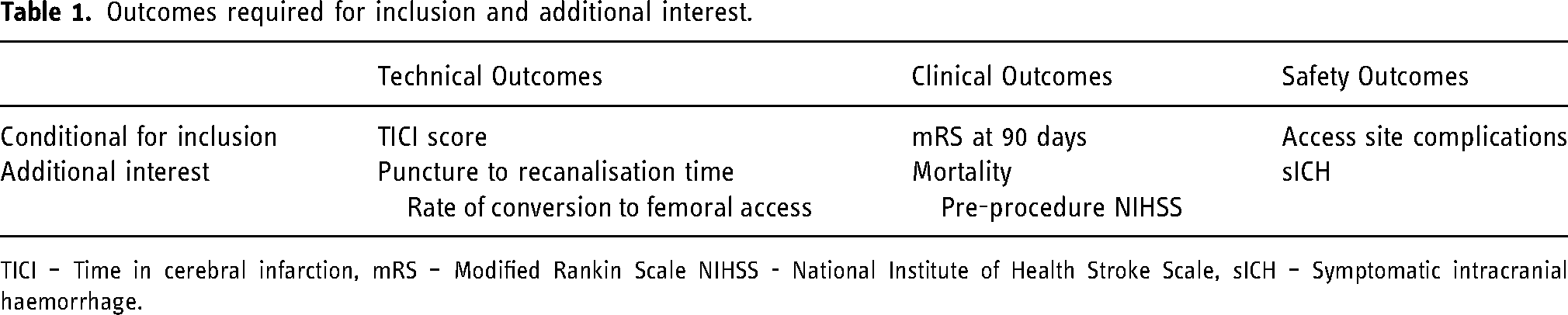
TICI – Time in cerebral infarction, mRS – Modified Rankin Scale NIHSS - National Institute of Health Stroke Scale, sICH – Symptomatic intracranial haemorrhage.
Statistical analysis
TICI scores and rates of mRS 0–2 at 90 days underwent proportional meta-analysis at 95% confidence intervals (CI). The DerSimonian-Laird random effects model was used due to expectation of high variability between the studies 18 and the analysis was carried out using Open-Meta software (Available at: http://www.cebm.brown.edu/openmeta/). Medians and interquartile ranges (IQR) were calculated for puncture to recanalization times where patient-level data were available.
A two-tailed z-test was used to compare pooled proportions of TICI 2b-3 and mRS 0–2 at 90 days to data from a recent systematic review of posterior circulation thrombectomy outcomes in 1612 patients. 19
Results
Literature search
The search was carried out on 29th November 2021 and identified 291 records. One additional article was identified through citation searching. After the removal of duplicates and initial screening, 31 full text articles were assessed for eligibility (Appendix 1). Eight articles met inclusion criteria and included extractable and relevant end-point data11,16,20–25 (Appendix 2). These studies were either entirely posterior circulation case series or included sufficient subgroup breakdown of data from case series of anterior and posterior circulation large vessel obstruction (LVO). No further unpublished subgroup data was obtained from authors who were contacted.
Quality assessment
All eight studies were case series and only one was prospective. Using the National Institutes for Health Quality Assessment Tool for Case Series, 17 three were assessed to be of good quality, the remaining five as fair quality (Appendix 3).
Baseline demographics
All eight studies were published between 2018 and 2021 containing a total of 76 patients who underwent posterior circulation thrombectomy via TRA. Five of the studies examined only posterior circulation thrombectomy with the remainder containing data from both anterior and posterior circulation thrombectomy. Four studies compared TFA with TRA and three studies reported on percentage of cases using the right versus left radial artery.
For the studies covering thrombectomy in the anterior and posterior circulation, baseline demographic data were only available from those which provided it for the posterior circulation subgroup (Table 2).
Demographic data.
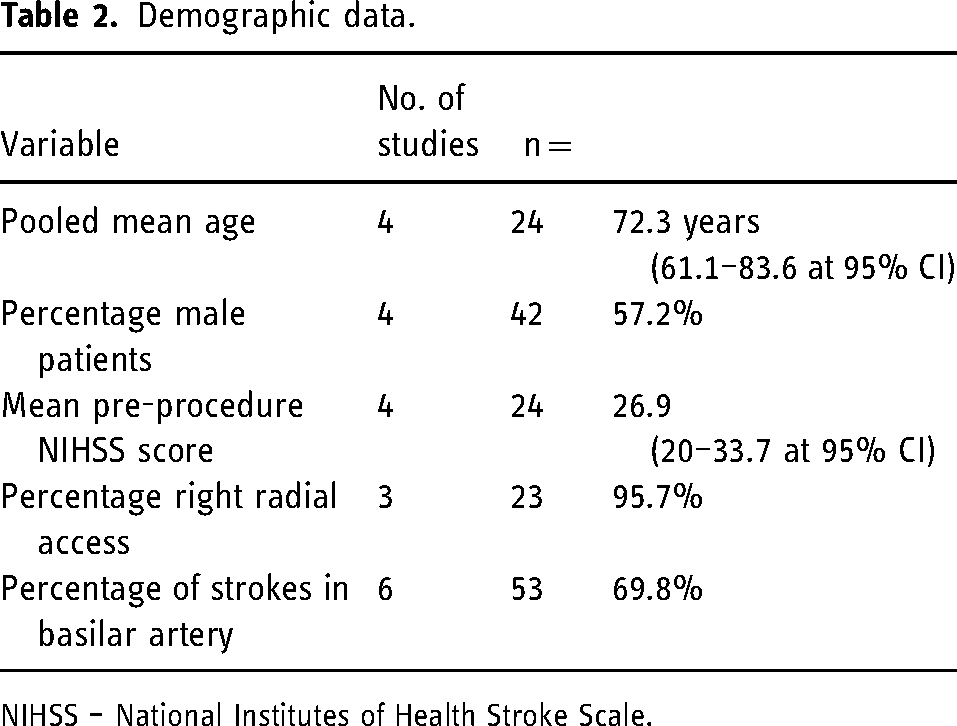
NIHSS – National Institutes of Health Stroke Scale.
Meta-analysis
Proportions of TICI 2b-3 were reported in seven studies (n = 65) as 94.7% (89.7–99.8% at 95% CI) (Figure 1) and TICI 3 proportions were reported by five studies (n = 31) as 67.9% (42.2–93.6% at 95% CI) (Figure 2). Proportions of mRS scores of 0–2 at 90 days were reported in three studies (n = 33) as 49.8% (31.5–68.1% at 95% CI) (Figure 3).
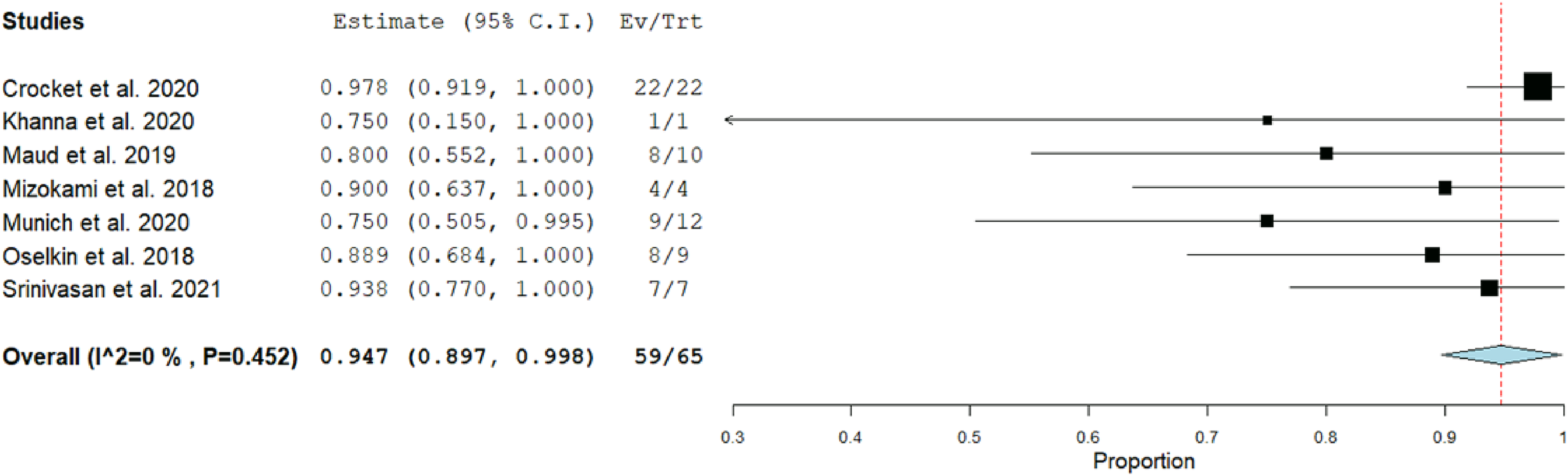
TICI 2b-3 proportional meta-analysis.
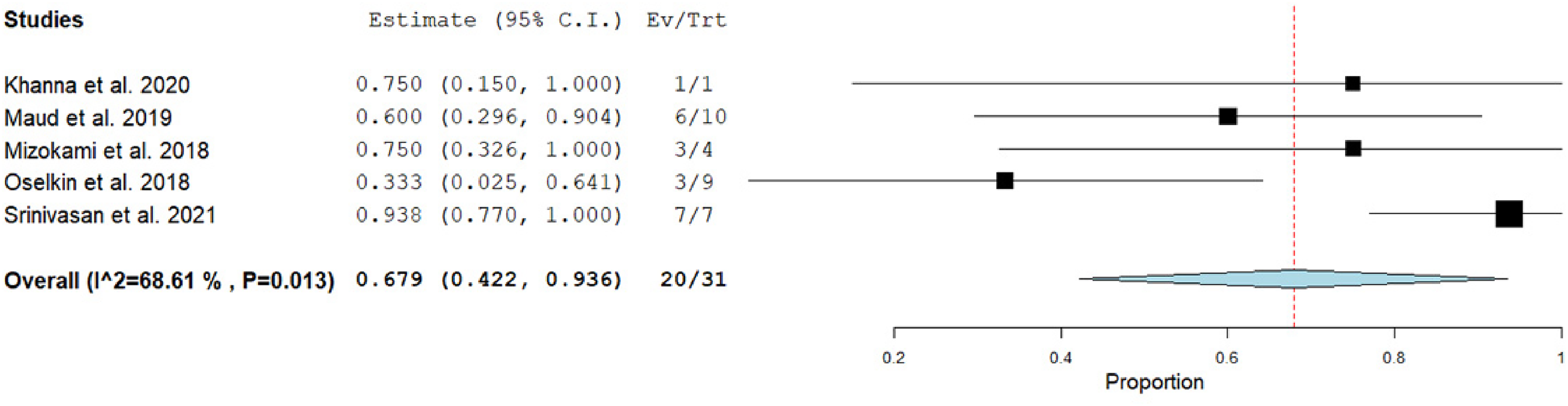
TICI 3 proportional meta-analysis.
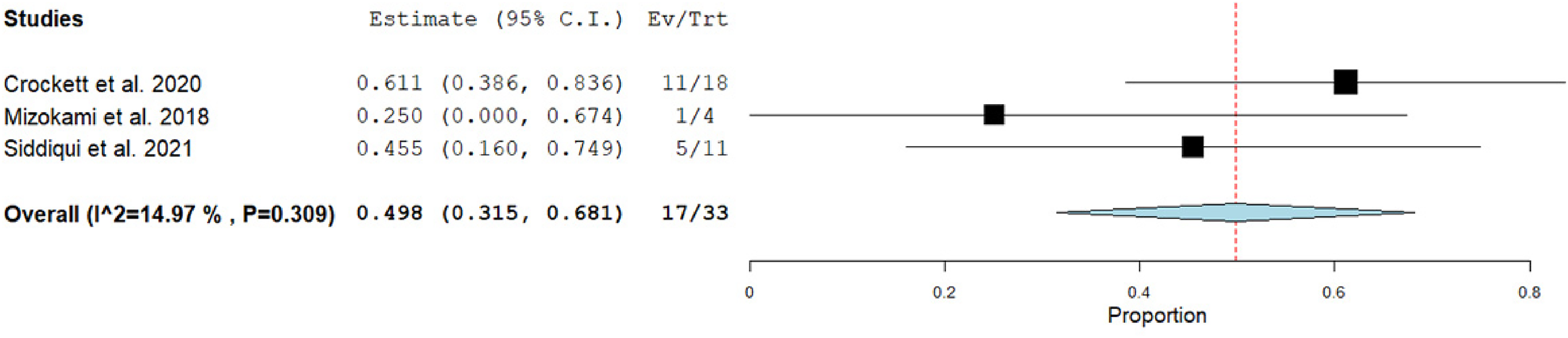
mRS 0–2 at 90 days proportional meta-analysis.
Median puncture to reperfusion times with interquartile ranges (IQR) were either provided or calculated for three studies (n = 35) (Table 3 and Figure 4).
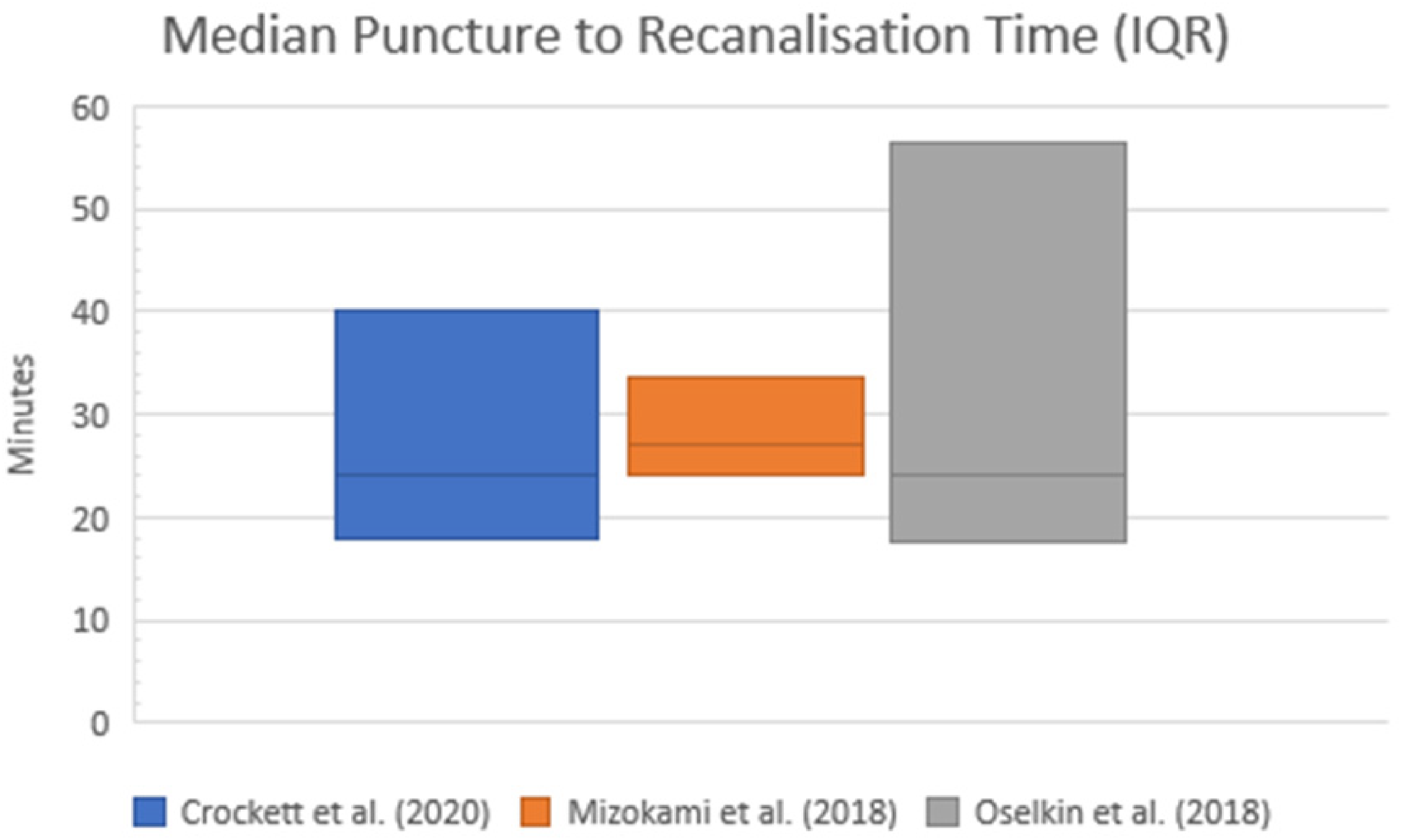
Median puncture to recanalisation times by study.
Median puncture to recanalisation times.
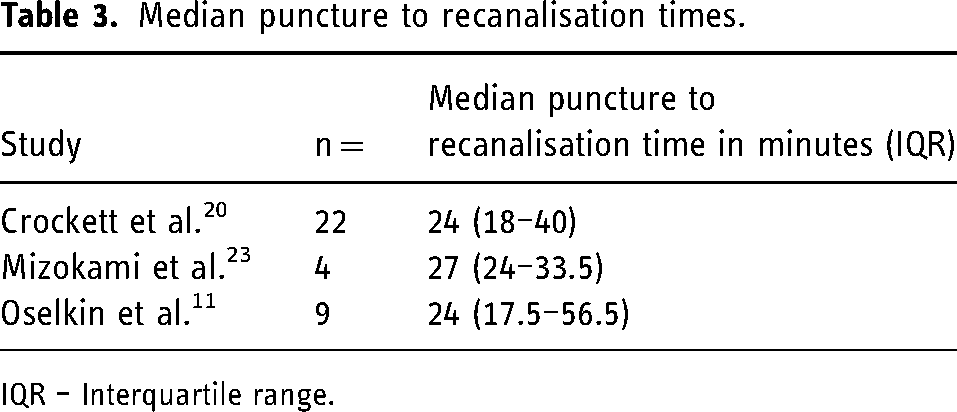
IQR – Interquartile range.
Five studies11,20,22–24 (n = 57) reported no access site complications though one instance of radial access failure was reported by one study 20 (n = 22), representing 4% of the patients in that study. Three-month mortality rate was reported by one study 16 (n = 11) at 36.3%. One study 20 (n = 22) reported sICH rate at 0%.
Comparative analysis
There was no significant difference in this study's pooled rates of TRA TICI 2b-3 (91% vs. 86% p = 0.27) and mRs 0–2 at 90 days (52% vs. 38% p = 0.10) compared to the TFA data from the comparison study. 19
Discussion
TICI, mRS and access site complication outcomes
The TICI 2b-3 and mRS 0–2 pooled outcomes were consistent with those of a large systematic review of TFA in posterior circulation stroke, 19 demonstrating that the technical and clinical efficacy of TRA is similar to TFA. Heterogeneity was low in meta-analysis of rates of TICI 2b-3 and mRS 0–2 indicating reduced chances of clinical or methodological diversity, thereby strengthening the validity of the analysis. There were no access site complications reported in 57 patients across five studies. This is consistent with the low complication rates (2.9%) found in TRA for a broad range of neurointerventional procedures 9 and underlines the superior safety profile of TRA.
Four studies16,22–24 included in this systematic literature review directly compared TRA with TFA but differed in their conclusions. Siddiqui et al. 16 reported higher successful reperfusion rates and improved functional outcomes with TFA when analysing all anterior and posterior circulation thrombectomies but did not find a difference for the posterior circulation subgroup. Munich et al. 24 concluded that TRA has superior access-site complication rates since no complications occurred in their TRA group, which included 12 posterior circulation thrombectomy patients. Maud et al. 22 found no significant difference in rates of TICI 2b-3, TICI 3 or mRS 0–2 at discharge between their TRA and TFA groups. Mizokami et al. 23 reported higher rates in their TRA group of TICI 2b-3 (100% vs. 80%), TICI 3 (75% vs. 0%) and fewer access site complications (0% vs. 20%) than the TFA group however no statistical analysis was undertaken on these results.
Puncture to recanalisation time
Time is a significant factor in the outcomes of posterior circulation thrombectomy with the chances of patients achieving a good functional outcome (mRS 0–2) decreasing by more than 50% if reperfusion is achieved more than 6 h after onset. 27 Similarly, duration of procedure time can have an impact on outcomes.
Although there was no statistical comparison made between puncture times to recanalisation, the median times reported by studies in this literature review (24, 24 and 27 min) appear substantially lower than those reported by studies from the TFA systematic review comparison data 19 where only one of 17 studies which reported this outcome had a median puncture to recanalisation time of <30mins. Achieving recanalisation within this timeframe has been associated with a much higher chance of good functional outcomes (OR 5.16, 1.68–15.84 at 95% CI). 28 The difference between the TRA and TFA groups underlines the need for further investigation as to whether TRA represents a time-saving technique that could be potentially valuable in posterior circulation thrombectomy.
Mizokami et al. 23 reported faster time to recanalisation in the TRA group than the TFA group (28.8 min ± 6.2 vs. 35.5 min ± 14.9) however statistical analysis on these results was not undertaken. One study 22 concluded that puncture to reperfusion time is faster in TRA versus TFA for posterior circulation stroke (29.2 ± 17.6 vs. 63.9 ± 56.7 min, p = 0.08) but this did not confer improved functional outcomes (40% vs. 40% mRS 0–2 at discharge). Crockett et al. 20 found similar puncture to recanalisation times when comparing their TRA cases with their centre's previous three years’ data of 86 patients who underwent posterior circulation thrombectomy via TFA (24 min IQR: 18–40 vs. 26 min IQR: 19–40). They concluded that, due to the learning curve, it is possible with further experience that procedural times could reduce further with TRA and this could supersede TFA as the preferred approach. This is supported by a learning curve study 29 which found that with increasing experience of the technique, cerebral angiography procedure and fluoroscopy times are shorter for TRA than TFA.
Access site laterality
Three studies11,22,23 (n = 23) reported radial access site laterality. Overall 95.7% of these cases used the right radial artery for access, which is much higher than expected given that 68% of patients have been shown to have left vertebral dominance 30 for which the left radial artery would provide the optimal route, given the low success rate (52%) of cannulating the left vertebral artery via right TRA. 31 This may represent selection bias due to operator preference for access site rather than the patient's overall suitability for radial access. For cerebral angiography, left transradial access has been shown to be technically feasible, safe and effective 32 so it is necessary for posterior circulation thrombectomy that left transradial access is used where the anatomy requires it. In one study 23 patients were selected for TRA only for patients suitable for access into the right vertebral artery. Crockett et al. 20 stated that left radial access was used in cases where the right vertebral artery was hypoplastic indicating that this would not affect patient suitability for TRA however they do not report their percentages of left versus right TRA.
Limitations
This study is limited by small overall sample size (n = 76) which is even further reduced depending on reporting of outcomes by individual studies and availability of posterior circulation subgroup data in those studies which examined both anterior and posterior circulation LVO.
There were no randomised controlled trials included in this systematic literature review. Only one study 20 was prospective in design and the other seven studies were retrospective. The retrospective nature of the studies allows for analysis of images taken during thrombectomy but not for intentional patient follow-up where this is not already routine practice. While seven of the eight included studies reported TICI scores, only three reported mRS at 90 days. All cases were consecutive for each study but those that were retrospective are subject to inherent biases in this type of design, namely the treatment preferences and practice patterns of the operators involved. 24
There is potential for selection bias as evidenced by the higher-than-expected rate of right radial artery puncture. Patients may have been selected based on the suitability of the anatomy given operator preference for right radial artery puncture. Ideally, consecutive patients in case series should be selected based on overall suitability for TRA as opposed to their suitability for right sided TRA alone. A novel grading scale has been developed for TRA difficulty in cerebral angiography 33 and it is possible an adapted version could be used to select patients for TRA in posterior circulation thrombectomy in future prospective studies to reduce selection bias from operator preference.
In addition, this study did not review the specific equipment and thrombectomy technique used which may be variable in cases using TRA. Future studies should consider including this to reduce the potential for a confounding variable and to provide further insight into the results.
Conclusion
This meta-analysis demonstrates that TRA is safe and effective for use in posterior circulation stroke. Though statistically insignificant, there is an indication that TRA may represent faster puncture to reperfusion times and improved functional outcomes at 90 days. Further prospective studies comparing TRA and TFA groups will be required to investigate this fully.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional ethical approval is not required for this study, given that all of the data used is publicly available.
Appendix 1
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources 26
Appendix 2
Data extraction from included studies (where applicable, n represents numbers in posterior circulation subgroup only)
Where entries are left blank (-) this is due to either the data not having been collected or not reported by the study. Demographic and outcome data were not extracted where they were not available for the posterior circulation subgroup.
Appendix 3
National Institutes for Health Quality Assessment Tool for Case Series. 17