
Abstract
Introduction
The role of endovascular treatment in cervical artery dissection (CAD) is equivocal. This study compared cerebral blood flow in CAD between medically and endovascularly treated patients using quantitative magnetic resonance angiography (QMRA).
Methods
Retrospective chart review was completed for patients with CAD. Inclusion criteria were adults (>18 years) with diagnosis of dissection of the internal carotid artery or vertebral artery who received QMRA. The cases were reviewed for clinical presentation, diagnosis, management, and imaging, and in particular, patients who underwent endovascular treatment were evaluated.
Results
Forty-one patients were included, 46.3% female and mean age 46.0+/− 11.9 years. 21 patients (51.2%) had contralateral (ICA) dissections while 19 (46.3%) had vertebral artery (VA) dissections, and 1 had both involved. Five patients underwent stenting, angioplasty, or both. Baseline characteristics between patients who underwent medical versus endovascular treatment were similar, although patients undergoing stenting/angioplasty were more likely to have diabetes (p = 0.015) and prior anticoagulation use (p = 0.007). All endovascular patients demonstrated ischemia on MRI versus 53.1% of those undergoing medical management (p = 0.047). Comparing ipsilateral vessel flow over time in these two patient groups showed those who underwent stenting or angioplasty had lower baseline flows, albeit non-significant (p = 0.629). Patients who underwent endovascular treatment had lower distal flow compared to the medical management group.
Conclusion
This study represents the first to assess vessel flow using QMRA in patients who underwent endovascular treatment of CAD. In combination with progressive symptoms, QMRA may serve as a useful adjunct in the selection of patients for endovascular intervention in arterial dissections.
Introduction
Cervical arterial dissections (CAD) in carotid or vertebral arteries cause 2–3% of all ischemic strokes and 5–22% of ischemic strokes in patients below 45 years of age, which is typically attributed to thrombus formation at the primary lesion and consequent distal emboli.1–2 However, reduced blood flow at and distal to the site of the dissection may also be an important contributing factor. Understanding quantitative differences in cerebral blood flow in CAD and its relationship to endovascular treatment could help guide management decisions such as consideration of endovascular therapy. While antiplatelet and anticoagulant medications are widely used in CAD to reduce the risk of stroke, the role of endovascular treatment remains unclear. Endovascular intervention with stenting or angioplasty is currently considered in the setting of antithrombotic contraindications or antithrombotic failure with progressive clinical symptoms or radiological stroke burden. This report describes the use of quantitative magnetic resonance angiography (QMRA) to select patients with low cerebral blood flow for endovascular therapy. Through analysis of serial QMRA and its relationship to clinical and radiological progression, we also investigated changes in cerebral blood flow over time in patients with CAD treated with medical and endovascular therapies.
Methods
Patient selection
A retrospective chart review was completed for patients with spontaneous cervical artery dissection presenting between August 31, 2009, and September 1, 2019, to a tertiary medical center in the United States. Inclusion criteria were adults (>18 years of age) diagnosed with dissection of the internal carotid artery or vertebral artery who also received QMRA neuroimaging. Patients received endovascular intervention for dissection based on a case-by-case evaluation at our institution. Institutional review board approval was obtained with a waiver of patient consent due to the nature of the retrospective study.
Data collection
Data were collected on patient characteristics, clinical presentation, diagnosis, management strategies, and radiologic imaging findings. Flow measurements of major intracranial vessels were collected using the commercially available NOVA software (Noninvasive Optimal Vessel Analysis; VasSol, Inc.; River Forest, IL USA), which utilizes time-of-flight (TOF) and phase-contrast (PC) techniques. QMRA in the use of cerebrovascular disorders has been described and validated previously.3–20 Measurements were collected from studies performed at the time of diagnosis and at all available follow-ups, noting the first and last follow-ups in particular for analysis. Data was also collected from standard magnetic resonance imaging (MRI) of the brain, as available, to evaluate for diffusion restriction as an indicator of ischemia. Imaging was reviewed by a trained neurosurgeon, and radiology reports written by attending neuroradiologists were also reviewed for the diagnosis of ischemic stroke.
Statistical analysis
Baseline characteristics of the patients were assessed, including demographic data, underlying risk factors, clinical presentation, and treatment modality. A flow index was calculated using the flow of the ipsilateral vessel of interest (artery with dissection present) determined by QMRA divided by the flow of the contralateral vessel (for example, flow in the dissected right internal carotid artery divided by the flow in the normal left internal carotid artery). Percentage of total cerebral flow was calculated as the flow of the ipsilateral vessel of interest divided by the sum of the flow in the bilateral ICAs and bilateral VAs, multiplied by 100. Univariate analyses using X2 test assessed the association with presence of ischemia on MRI. Repeated measures ANOVA were used to analyze the flow in the ipsilateral vessel and contralateral vessel over time, and box plots were used to graphically display these values. Statistical analyses were performed using SPSS Statistics software (Version 27, IBM Corporation, Armonk, NY).
Results
Baseline characteristics
A total of 41 patients met inclusion criteria with mean age 46.0+/− 11.9 years. There was a slight male predominance in the cohort with 53.7% male (N = 22) and 46.3% female (N = 19). The majority of patients presented with neurologic sequelae (75.6%, N = 31), with or without accompanying headache or neck pain. Symptoms included both transient or permanent paresis or plegia, numbness, paresthesias, change in vision, dysarthria, aphasia, dizziness or vertigo, ataxia, and Horner's syndrome, among others. More dissections occurred in the internal carotid artery (ICA) as compared to the vertebral artery (VA) (51.2% vs. 46.3%); one patient had both ICA and VA dissections at presentation. Baseline characteristics compared between patients who underwent medical management versus endovascular treatment were similar; however, patients undergoing stenting or angioplasty were more likely to have diabetes (p = 0.015) and prior anticoagulation use (p = 0.007). All patients in the endovascular group demonstrated ischemia on MRI versus 53.1% of those undergoing medical management (p = 0.047). These findings have been summarized in Table 1.
Comparison between characteristics of patients with stenting/angioplasty and those without.
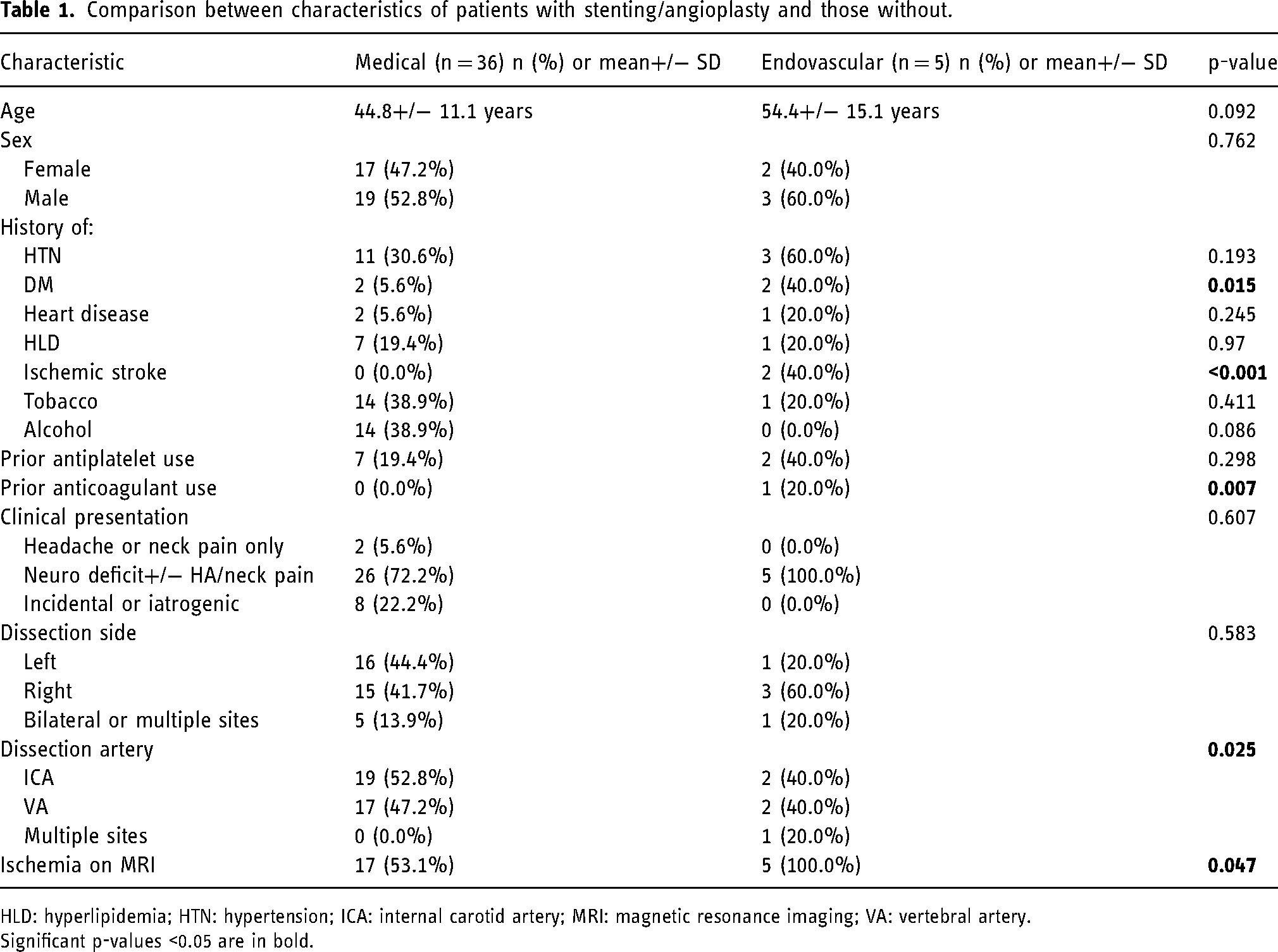
HLD: hyperlipidemia; HTN: hypertension; ICA: internal carotid artery; MRI: magnetic resonance imaging; VA: vertebral artery. Significant p-values <0.05 are in bold.
Quantitative MRA flow measurements
Patients selected for endovascular treatment had lower baseline cerebral blood flow in arteries distal to the CAD than patients treated with medical management alone (Figures 1 and 2).
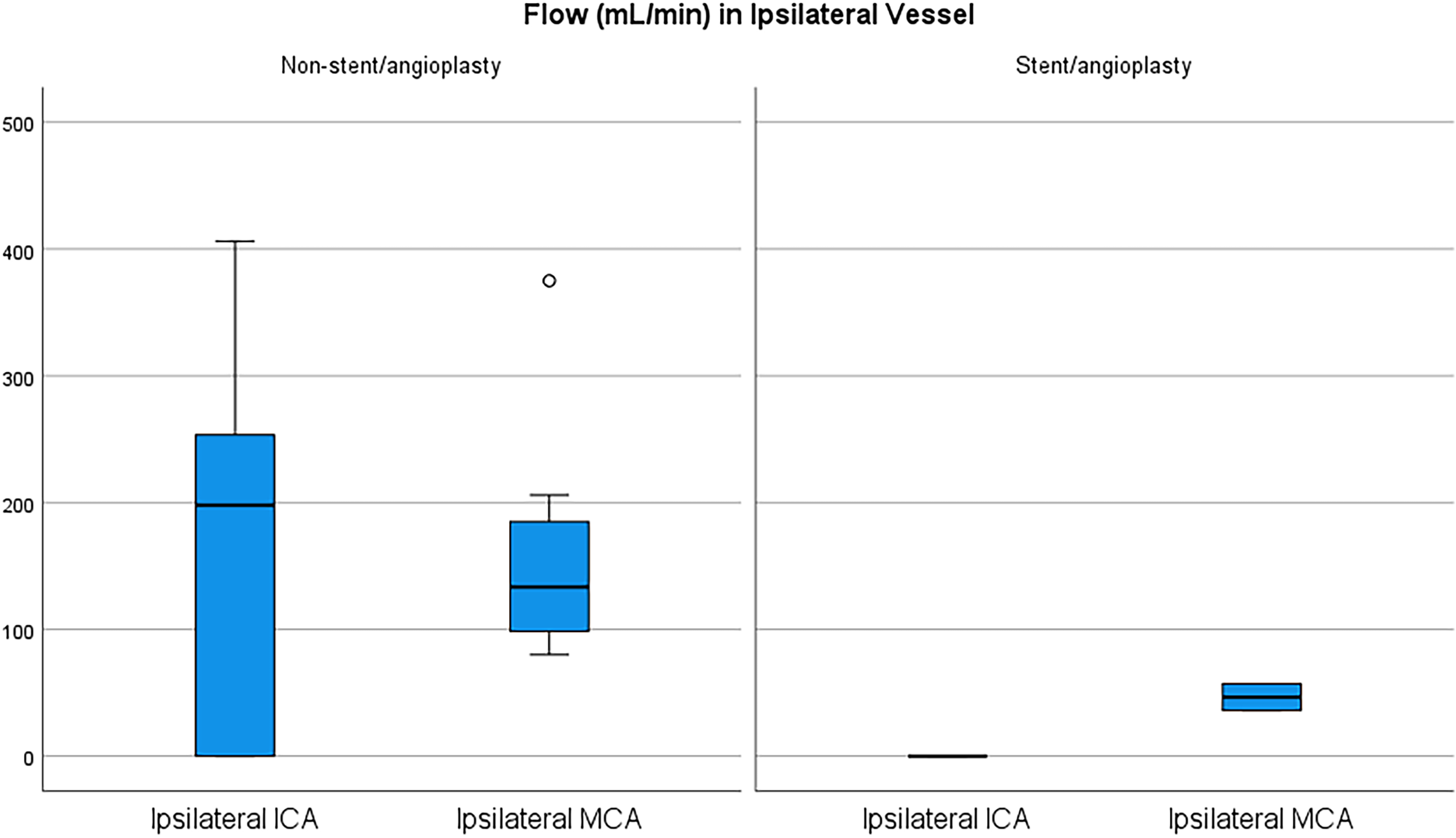
Box plot of flow measurements for patients with ICA dissections through ipsilateral vessel and ipsilateral MCA with and without endovascular treatment.
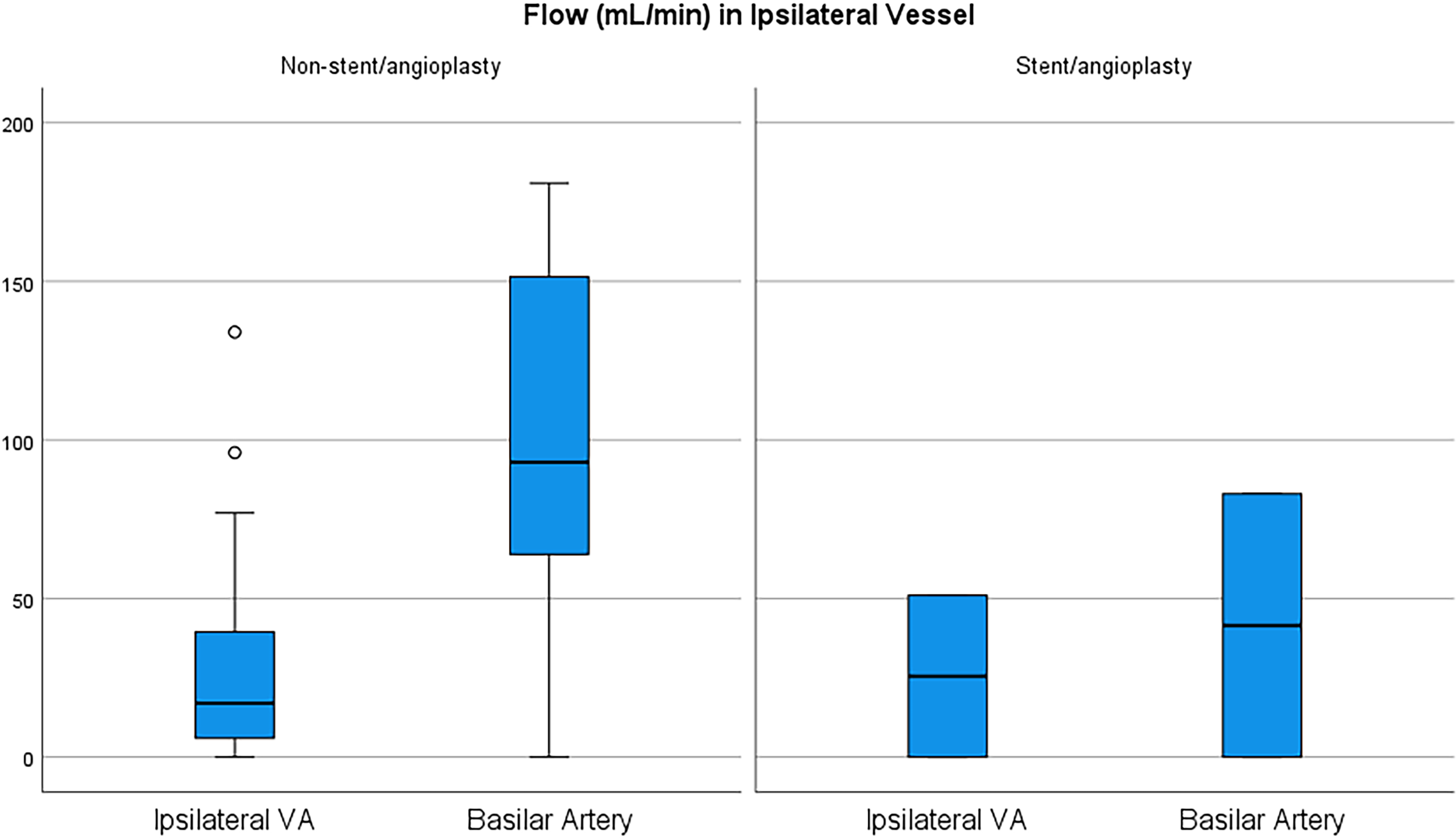
Box plot of flow measurements for patients with VA dissections through ipsilateral vessel and ipsilateral BA with and without endovascular treatment.
Ipsilateral flow over time from baseline to final follow-up improved in all five patients who underwent stenting or angioplasty (Figure 3). Comparing ipsilateral vessel flow over time in our two patient groups showed that cerebral blood flow increased similarly over time and converged (p = 0.629) (Figure 4).
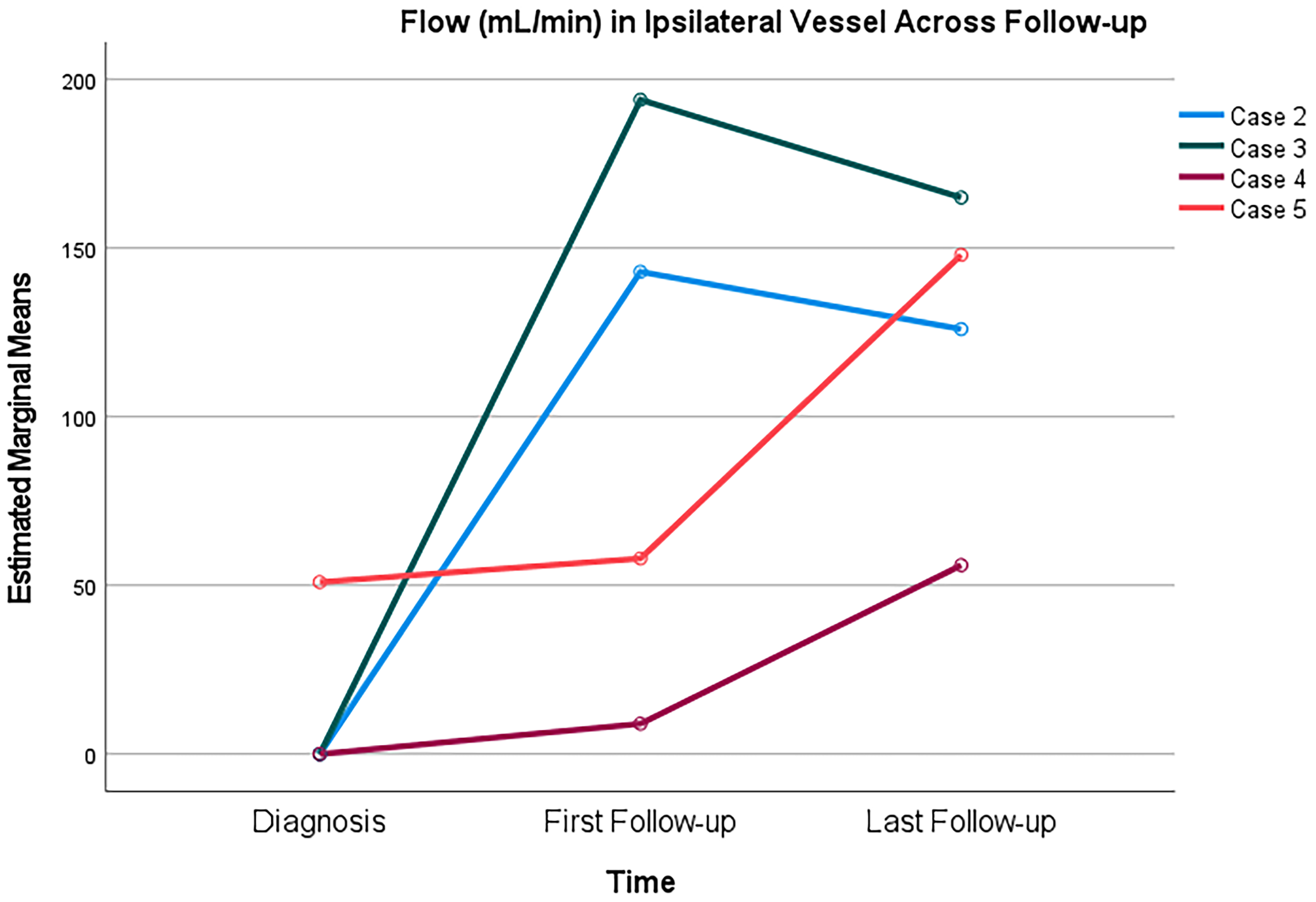
Spaghetti plot of ipsilateral vessel flow over follow-up in patients who underwent stenting/angioplasty.
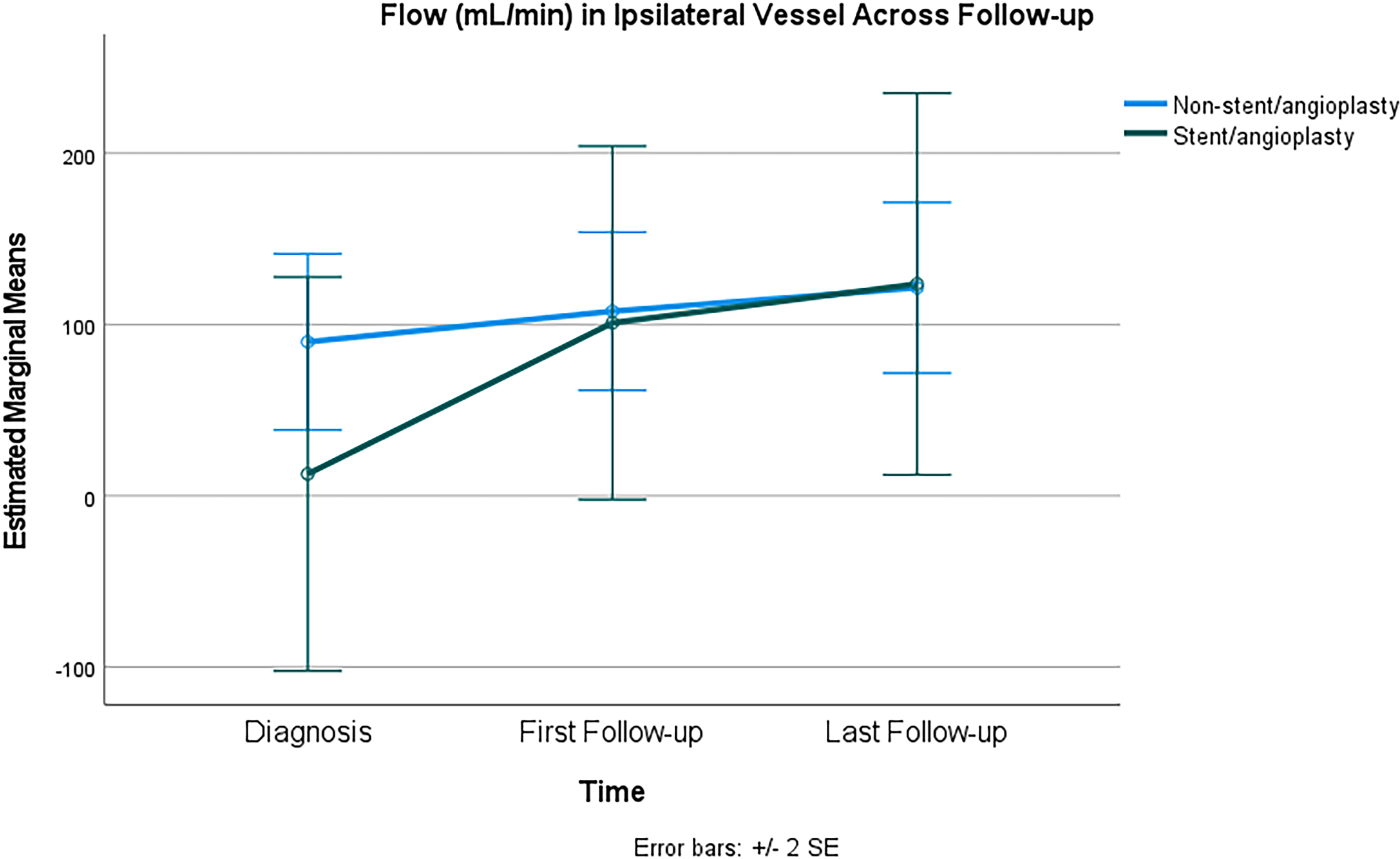
Two-way repeated measures ANOVA comparing flow in the vessel of interest in patients with stenting/angioplasty and those without (within-subject and between-subject design, with Greenhouse-Geisser correction for sphericity, p = 0.130 for within-subject effects and p = 0.629 for between-subject effects). Patients with bilateral or multiple dissection sites excluded.
Case summaries
Table 2 highlights the five patients who underwent endovascular intervention for the treatment of their dissection. Two patients had dissections in the ICA only, two in the VA only, and one with a dissection found in both the ICA and VA. Three underwent stenting only, one angioplasty only, and another with stenting, angioplasty, and thrombectomy. All patients presented with symptomatic disease and evidence of ischemia on MRI. QMRA showed impaired distal flow in all patients (Figure 3 and 4).
Patient characteristics at presentation.
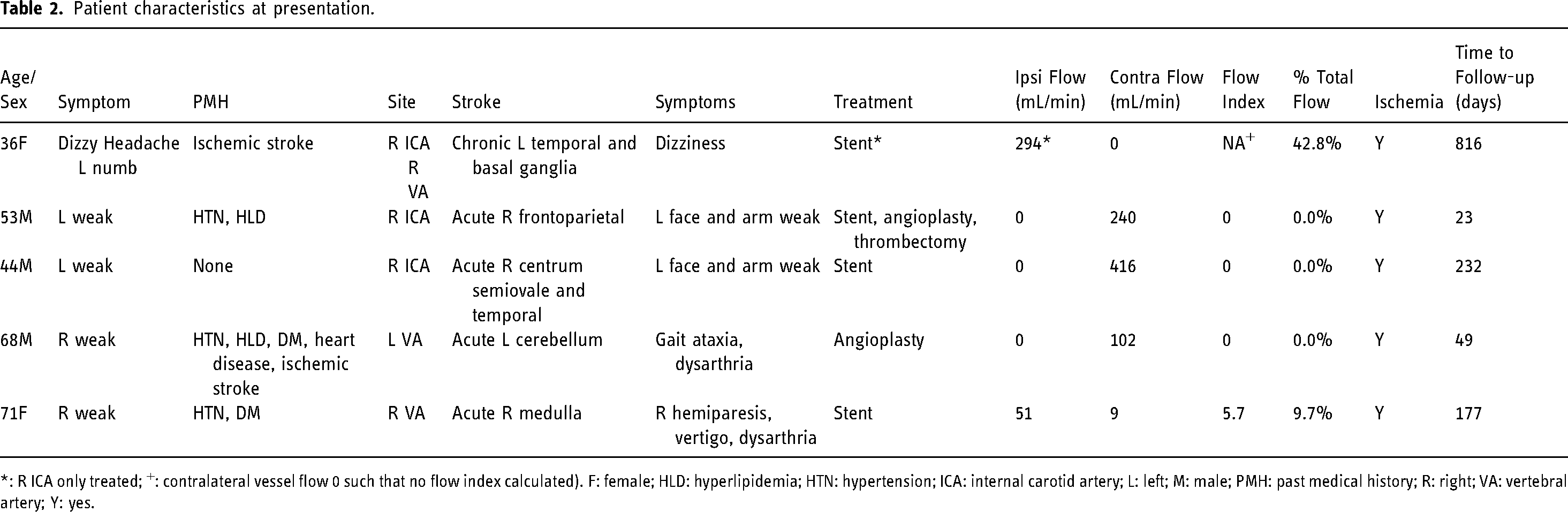
*: R ICA only treated; +: contralateral vessel flow 0 such that no flow index calculated). F: female; HLD: hyperlipidemia; HTN: hypertension; ICA: internal carotid artery; L: left; M: male; PMH: past medical history; R: right; VA: vertebral artery; Y: yes.
Example: Case 2. A 53-year-old man presented to an external hospital with acute-onset left hemiparesis and right-sided gaze preference. He was given thrombolytic therapy and transferred to our facility where emergent angiography revealed acute dissection within the right cervical internal carotid artery with severe stenosis at the petrous segment as well as chronic dissection involving the cervical left internal carotid artery. QMRA revealed indeterminate flow in the right ICA, right MCA flow of 36 mL/min, left ICA flow of 240 mL/min, and left MCA flow of 109 mL/min. The patient was started on intravenous anticoagulation with heparin and required a vasopressor to maintain systolic blood pressure >140 mmHg. On day 5, he developed worsening left hemiparesis with CT revealing progression of ischemia. Due to low flow within the right anterior circulation and progression of neurological symptoms and radiographic ischemia despite medical management, the patient was taken for repeat angiography for possible stenting. Angiography revealed acute occlusion of the right internal carotid artery for which the patient was treated with mechanical thrombectomy followed by cervical and petrous internal carotid artery stenting and angioplasty. Two-week follow-up QMRA revealed improved flow: right ICA flow of 143 mL/min, right MCA flow of 81 mL/min, left ICA flow of 232 mL/min, and indeterminate left MCA flow. Thereafter, the patient did well with stable follow-up QMRA and carotid artery ultrasound studies for two years. (Figure 5(a)–(d))
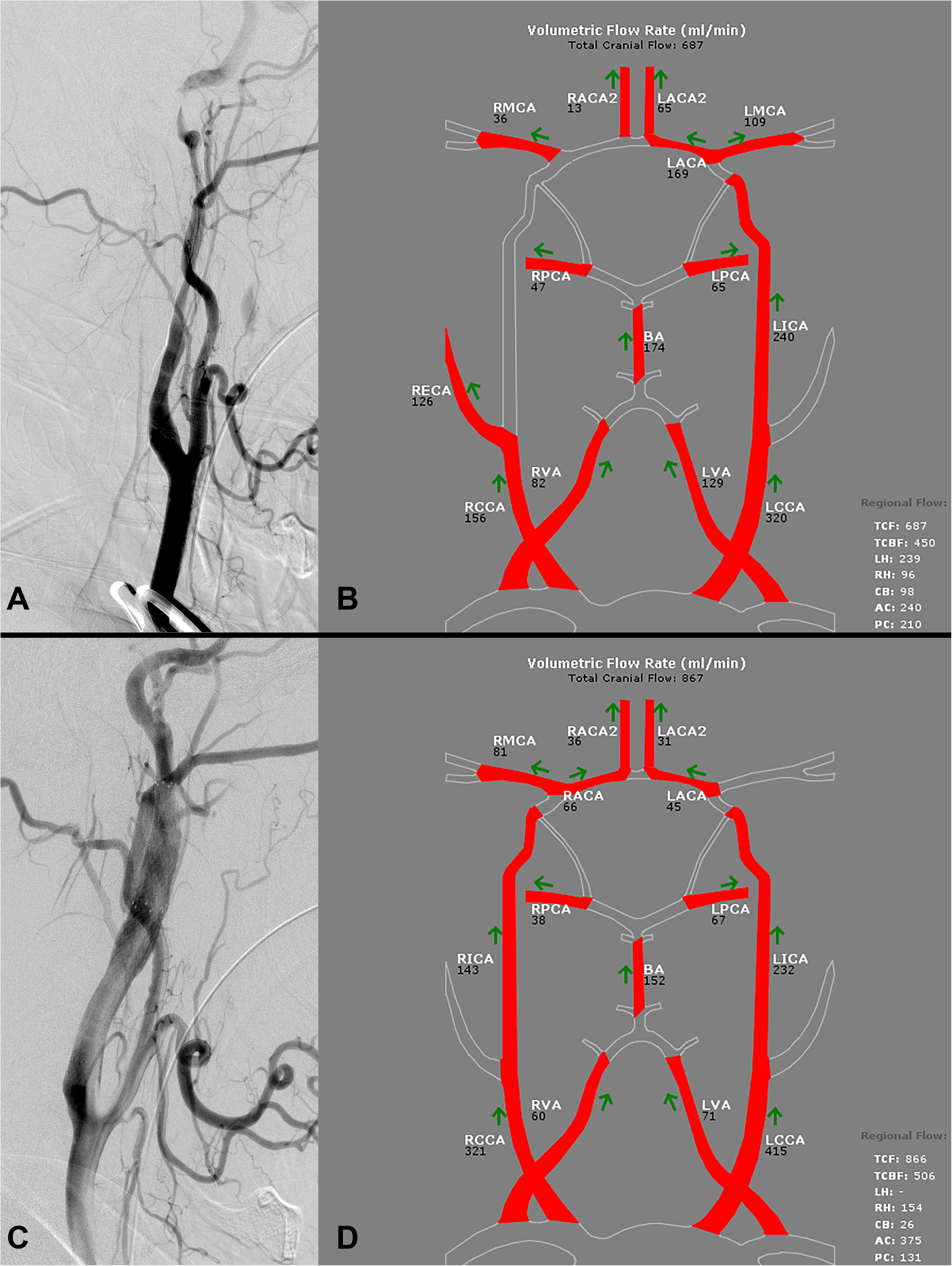
(a) Initial diagnostic cerebral angiogram showing dissection in the right ICA. (b) Initial MRA NOVA showing diminished flow in the ipsilateral ICA and MCA. (c) Post-procedural diagnostic cerebral angiogram showing patent stent within right ICA. (d) Post-procedural MRA NOVA showing improved flow in the ipsilateral ICA and MCA.
Discussion
This study represents the first to assess vessel flow using QMRA in patients who underwent endovascular treatment of cervical arterial dissections; however, QMRA has been evaluated and validated in multiple cerebrovascular conditions in the past few decades.3–14 Of particular interest to this study, this technique has been used to quantitatively study blood flow pre- and post-endovascular treatment in the cranial circulation.15–20
Understanding QMRA and its relation to CAD and endovascular treatment may help guide management decisions. In combination with progressive symptoms, QMRA may serves as a useful adjunct in the selection of patients for endovascular intervention in arterial dissections. Figures 2 and 3 showed the diminished distal flow on the initial studies in those who underwent stenting or angioplasty: patients with ICA dissections had lower flow in the ipsilateral MCA, and patients with VA dissections had lower flow in the basilar artery, when compared to patients who underwent medical management only. The case descriptions further highlight this management paradigm. Furthermore, although patients were evaluated on a case-by-case basis for intervention at our institution, four of the five patients had progressively worsening symptoms. Two patients additionally had significant atherosclerotic disease, including contralateral ICA occlusion in one patient and contralateral VA stenosis in the other, and both of these patients had a history of prior stroke.
Interestingly, although patients who underwent stenting or angioplasty had lower flow initially in comparison to the medical management group, it is important to note that ipsilateral flow increased over time across all groups, regardless of intervention type. This result highlights the natural history of patients with dissections, whereby flow improves over time in the affected vessel, regardless of endovascular intervention. Thus, it is prudent to consider the criteria for intervention: failure of medical management, as evidenced by escalating or crescendo-type symptoms or recurrent stroke. Cerebral ischemia with arterial dissection is typically attributed to thrombus formation at the primary lesion and resultant distal emboli; however, the presence of recurring or crescendo symptoms may indicate the potential for hemodynamic compromise caused by the dissection. Low flow within the vasculature distal to the dissection on QMRA could stratify patients with recurrent symptoms and aid decision-making in endovascular intervention. Therefore, although the natural history of dissections involves improvement in flow over time, selecting patients with progressive symptoms and quantitative evidence of low flow for endovascular therapy may preempt failure of medical management and prevent progression of symptoms or ischemia. While crescendo symptoms and diminished ipsilateral distal flow motivated the placement of the stent in Case 2 above, Case 1 interestingly required consideration of stent placement due to low flow in the contralateral MCA, as the patient also presented with an incidental chronic contralateral ICA occlusion.
In current literature, the use of endovascular intervention has generally been reserved for CAD patients with recurrent ischemic events despite antithrombotic therapy, contraindications to antithrombotic therapy, iatrogenic dissections, and dissections with rupture or impending rupture.21–24 No randomized control trials or controlled clinical trials have been reported that compare endovascular and antithrombotic therapy with antithrombotic therapy alone, and therefore, it is difficult to ascertain the indications, safety, and efficacy of endovascular treatment of CAD. Case reports and case series have largely reported on traumatic cervical artery dissections, which may have a different pathophysiology than spontaneous dissections, which we primarily describe in this study.
There are several limitations in this study. First, the number of patients in the endovascularly treated group is small, and thus, the results of the statistical analysis should be interpreted with caution. Also, as a retrospective review, the availability of data within the electronic medical record may be limited. Further, all causes of dissection were included: spontaneous and iatrogenic; thus, the study population generally does not include patients with dissection secondary to trauma, which would require other considerations in their management paradigms, particularly in regard to antiplatelet therapy or anticoagulation use. In addition, because the use of QMRA was part of the inclusion criteria, this presents a potential selection bias in those patients, although it is common practice at this institution to employ QMRA imaging in any condition where cerebral blood flow may be of concern.
Conclusion
This study represents the first to assess vessel flow using QMRA in patients who underwent endovascular treatment of cervical arterial dissections. In combination with progressive symptoms, QMRA may potentially serve as an adjunct in the selection of patients for endovascular intervention in arterial dissections, but larger, prospective studies would be required for validation. Although patients who underwent stenting or angioplasty had lower flow initially in comparison to the medical management group, ipsilateral flows increase across all groups over time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.