
Abstract
Background
Distal anterior cerebral artery (DACA) aneurysms are rare, and endovascular treatment of these aneurysms is challenging. Thromboembolic events, including silent ischemic events, are one of the most important complications of coil embolization for cerebral aneurysms. The treatment outcomes and predictors of silent ischemic events in coil embolization for unruptured DACA aneurysms were investigated, focusing on the morphological characteristics of aneurysms, especially the inflow angle (IA) and global outflow angle (GOA).
Methods
A total of 12 patients with 12 unruptured DACA aneurysms, treated with coil embolization at our institute, were retrospectively investigated. Predictors for silent ischemic events were evaluated by comparing diffusion-weighted imaging (DWI)-positive and DWI-negative patients.
Results
Silent ischemic events detected on DWI were observed in eight aneurysms (66.7%). Comparison of the morphological characteristics of aneurysms between the two groups showed a significantly smaller GOA in the DWI-positive group than in the DWI-negative group (172.6 ± 17.7° vs. 216.8 ± 16.8°, P < 0.01). A multivariate analysis showed that GOA <195° was a significant predictor of silent ischemic events (P = 0.04; odds ratio: 23.62; 95% confidence interval: 1.11–490.39).
Conclusion
A small GOA was a significant predictor of silent ischemic events after coil embolization for unruptured DACA aneurysms. While some patients can be treated safely with minimally invasive coil embolization, it is necessary to consider surgical clipping in patients at high risk of thromboembolic events with coil embolization.
Keywords
Introduction
The anterior cerebral artery (ACA) is divided into five segments (A1–A5); the A2–A5 segments, originating from the anterior communicating artery complex, is referred to as the distal ACA (DACA). 1 DACA aneurysms are rare and reportedly account for 2%–9% of all cerebral aneurysms.2,3 The treatment methods of clipping and coil embolization are equally challenging. Clipping for DACA aneurysms using the inter-hemispheric approach presents certain technical problems such as: adhesion at the cingulate gyri; a deep and narrow operative field; and difficulty in controlling the proximal parent artery, leading to a high intraoperative rupture rate (0%–50%).4,5 A high morbidity rate (0%–9.3%) has been reported for clipping.6,7 Conversely, the distal vascular distribution and small size of the aneurysm8,9 result in difficulty in controlling the microcatheter during coil embolization for DACA, and intraprocedural perforations (12%) occur more often in DACA aneurysms than in aneurysms at other locations. 9 Therefore, DACA aneurysms are difficult to treat using coil embolization. 10 Treatment outcomes of coil embolization for cerebral aneurysms have improved with the development and advancement of devices; however, this method remains challenging.11–14 There are several reports of coil embolization for unruptured DACA aneurysms in the literature.9,10,12,14–17
Although antiplatelet therapy is widely used for prevention of thromboembolic events, these events continue to be an important complication of coil embolization for cerebral aneurysms. Thromboembolic events can manifest as follows: 1) thrombus formation observed during the procedure; 2) clinical ischemic symptoms, recognized as ischemia on neurological evaluation, which can be a transient ischemic attack or a permanent ischemic infarction; and 3) silent ischemic events, abnormalities detected by diffusion-weighted magnetic resonance imaging (DW-MRI). 18
Arterial bifurcation morphology is reported to be an important determinant of hemodynamic patterns. 19 Therefore, we focused on the arterial bifurcation angle, and assumed that the bifurcation angle affects the treatment outcome of coil embolization. We had earlier reported that outflow angle affects the treatment outcomes of coil embolization for unruptured middle cerebral artery bifurcation aneurysms. 20 Global outflow angle (GOA) was reported as a predictor of re-treatment in coil embolization for unruptured middle cerebral artery bifurcation aneurysms. 21
In the present study, we investigated the treatment outcomes and predictors of silent ischemic events in coil embolization for unruptured DACA aneurysms, focusing on morphological characteristics, especially the angle between the aneurysms and the surrounding blood vessels, and their association with silent ischemic events.
Materials and methods
Out of a total of 18 patients with DACA aneurysms treated with coil embolization from April 2009 to March 2019 at our institute, 12 unruptured DACA aneurysms in 12 consecutively treated patients were retrospectively investigated. The inclusion criteria included an age ≥18 years and an unruptured aneurysm. Cases with follow-up period of ≤1 year were excluded.
Patient characteristics including age, sex, medical history (hypertension, diabetes, hyperlipidemia), smoking habits (including present or past smoking history), modified Rankin Scale (mRS) before the procedure, antiplatelet therapy, and radiological characteristics of the aneurysm, such as location, size, neck size, aspect ratio, and dome/neck ratio (D/N ratio), were considered. The treatment outcomes of using the balloon-assisted technique, stent-assisted technique, the number and length of coils, and procedural duration were investigated. Immediate angiographic outcomes were categorized as complete occlusion (CO), neck remnant (NR) or body filling (BF). 3 We also analysed: complications (transient or permanent, thromboembolic or hemorrhagic); diffusion-weighted imaging (DWI) positivity rate; whether re-treatment was required; time to re-treatment after the procedure; mRS score of 0 at 1 year; and angiographic CO at 1 year, and during the follow-up period. Hemorrhagic complications were evaluated immediately after the procedure using computed tomography.
All patients were administered either mono-antiplatelet therapy (aspirin 100 mg/day or clopidogrel 75 mg/day) or dual antiplatelet therapy (aspirin 100 mg/day and clopidogrel 75 mg/day), at least one week before the procedure. Patients administered dual antiplatelet therapy were wide-neck cases where stent placement might be necessary based on preoperative imaging findings. The procedure was performed under general anesthesia for all patients. After femoral sheath placement, systemic heparinization was started with a loading dose of 4000–5000 IU of heparin; activated clotting time was maintained at >250 s during the procedure. After the procedure, heparin administration was stopped and therefore, reversed naturally; only antiplatelet therapy was continued. For patients with stent-assisted technique, dual antiplatelet therapy was continued for 1 year after the procedure, and thereafter, mono-antiplatelet therapy with aspirin 100 mg/day or clopidogrel 75 mg/day was continued indefinitely. For patients without stent-assisted technique, aspirin 100 mg/day or clopidogrel 75 mg/day was continued for 6 months after the procedure.
Magnetic resonance imaging (MRI) was scheduled within 24–36 h after the procedure. Imaging was performed with the MAGNETOM Avanto 1.5 T MRI system (Siemens, Erlangen, Germany) till March 2014 and the MAGNETOM Skyra 3 T MRI system (Siemens) from April 2014 using a multi-section, single-shot spin-echo echo-planar imaging sequence.
Follow-up angiographic outcomes at 6 months and 1 year after treatment were assessed using MRI and magnetic resonance angiography (MRA). If the examination results were stable, MRI and MRA were performed annually thereafter. Additional follow-up angiography was performed in patients with a potential risk of recanalization, as determined by MRA, and re-treatment was performed based on the angiographic findings.
To investigate the predictors of silent ischemic events, the following patient characteristics in DWI-positive and DWI-negative groups were compared: sex, age, medical history (hypertension, diabetes, hyperlipidemia), smoking habits, antiplatelet therapy, radiographic characteristics of the aneurysm (size, neck size, aspect ratio, D/N ratio), stent-assisted technique, procedural duration, and immediate angiographic outcome. With reference to the preoperative three-dimensional (3D) digital subtraction angiography (DSA) images, two angles were calculated based on the surrounding blood vessel and aneurysm, resulting in an intraoperative working angle for neck identification. Each of the two angles is shown in Figure 1. The inflow angle (IA) was composed of the A2 segment and the axis of the aneurysm (Figure 1A), 22 and the GOA was composed of the A2 segment and the bilateral A3 segments (Figure 1B). 21 The A2 diameter (A2D) near the neck, and the A3 diameter (A3D) of the pericallosal artery and the callosomarginal artery, near the neck were calculated. The difference in diameter between the A2D and A3D (A2–3D), and the difference in diameter between the bilateral A3Ds (A3–3D) were also calculated. DSA, including frontal and lateral views, 3D rotational angiography, and a working view were acquired on a biplane Axiom Artis Q BA angiography system (Siemens). From the initial DSA, measurements of the morphological characteristics of the aneurysm and angles were performed on a dedicated workstation using the Syngo Workplace (Siemens).

A. Schema of the inflow angle (IA): The angle between the parent artery (A2) and aneurysm dome axis is defined as the IA. B. Schema of the outflow angle (GOA): The angle between the bilateral daughter artery (A3) is defined as the GOA., which is measured on the inflow vessel side and not the aneurysm side.
This study was approved by the hospital's review board.
Statistical analysis
Statistical analysis was performed using SPSS for Mac (version 24.0 IBM Corp., Armonk, New York, USA). Continuous variables were presented by mean with standard deviation. Chi-square (χ2) test, Fisher's exact test, and Student's t-test were used to compare the DWI-positive and DWI-negative groups. Related factors of silent ischemic events with P-value of <0.1 in univariate analysis, were evaluated using multivariate logistic regression analysis. In addition, we investigated the association between GOA and DWI using receiver operating characteristic curves, and the optimal cut-off value was determined. A P-value of <0.05 was considered statistically significant.
Results
A total of 12 unruptured DACA aneurysms in 12 patients were consecutively treated using coil embolization at our institute. Patients’ and radiological characteristics of aneurysms are summarized in Table 1. The mean age of the patients was 68.8 ± 6.58 years. There were three males and nine females. Hypertension, diabetes, and hyperlipidemia was observed in four (33.3%), one (8.3%) and one (8.3%) patient, respectively. Smoking habits were observed in four (33.3%) patients. The preoperative mRS score was 0 in all cases. All patients had A2–A3 bifurcation aneurysms. The mean aneurysm size, neck size, aspect ratio, and D/N ratio were 6.68 ± 2.23 mm, 3.74 ± 0.86 mm, 1.48 ± 0.55, and 1.33 ± 0.44, respectively. Five patients underwent mono-antiplatelet therapy, and seven underwent dual antiplatelet therapy.
Patients’ and radiological characteristics of aneurysms of coil embolization for unruptured distal anterior cerebral artery aneurysms.
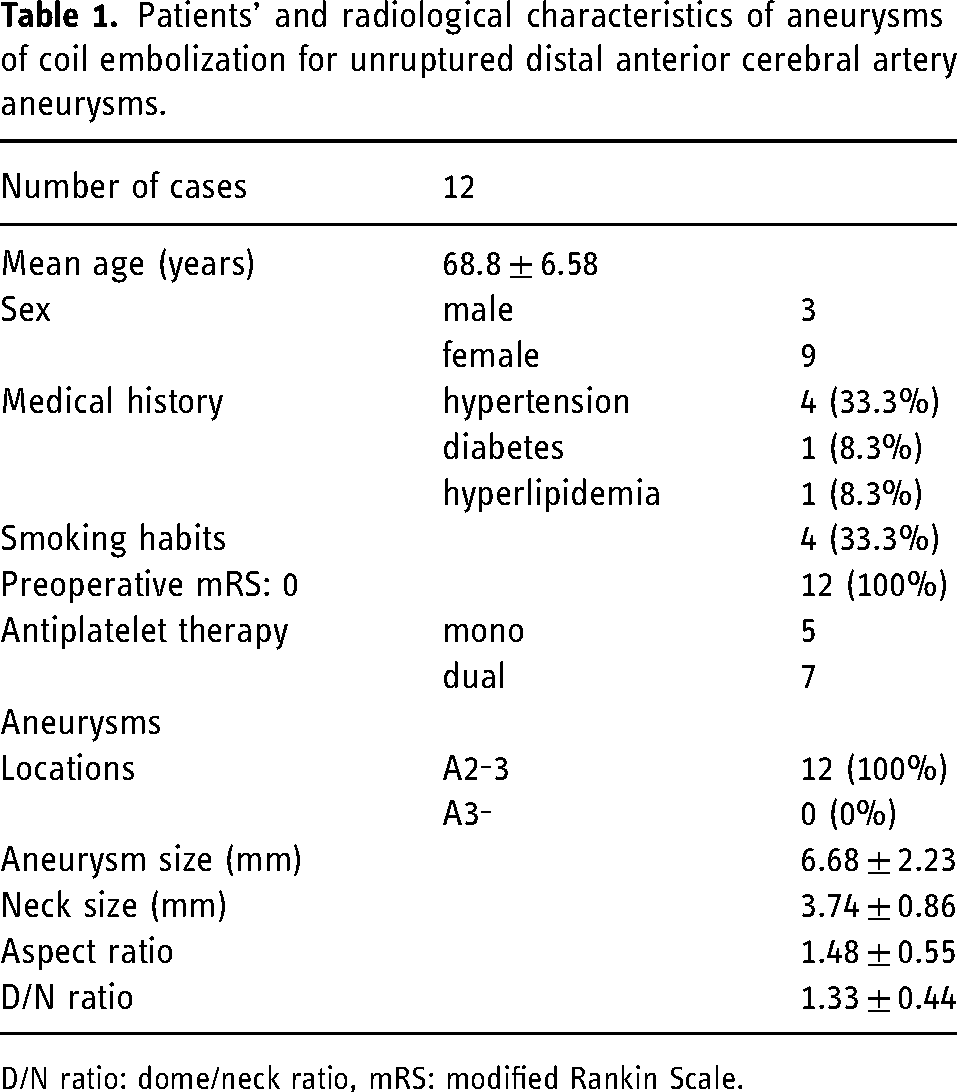
D/N ratio: dome/neck ratio, mRS: modified Rankin Scale.
Treatment outcomes are summarized in Table 2. All cases were treated using the adjunctive technique; nine aneurysms (75%) were balloon-assisted and three aneurysms (25%) were stent-assisted. The mean number of coils was 5.67 ± 2.66; the mean coil length was 44.6 ± 33.7 cm; the mean procedural duration was 136.6 ± 57.7 min, the immediate angiographic outcome was CO, NR, and BF, in one (8.3%), seven (58.4%), and four (33.3%) patients, respectively. Perioperative complications were observed in two (16.7%) patients, both of which were hemorrhagic complications. One patient had an intracerebral hemorrhage of the splenium of the corpus callosum due to perforation, and prolonged mild disturbance of consciousness. The other patient had an asymptomatic, small intracerebral hemorrhage. Eight patients (66.7%) had silent ischemic events, detected on DWI in the treated vascular territory. Re-treatment was required in two cases (16.7%), and mean time to re-treatment after the procedure was 15 ± 12 months. One year after the procedure, the mRS score was 0 in 11 cases (91.7%) and CO was observed in nine cases (75%). The mean follow-up period was 42.7 ± 37.5 months; no cases of rupture or bleeding, caused by the treated aneurysm, was observed during the follow-up period.
Treatment outcomes in coil embolization for unruptured distal anterior cerebral artery aneurysms.
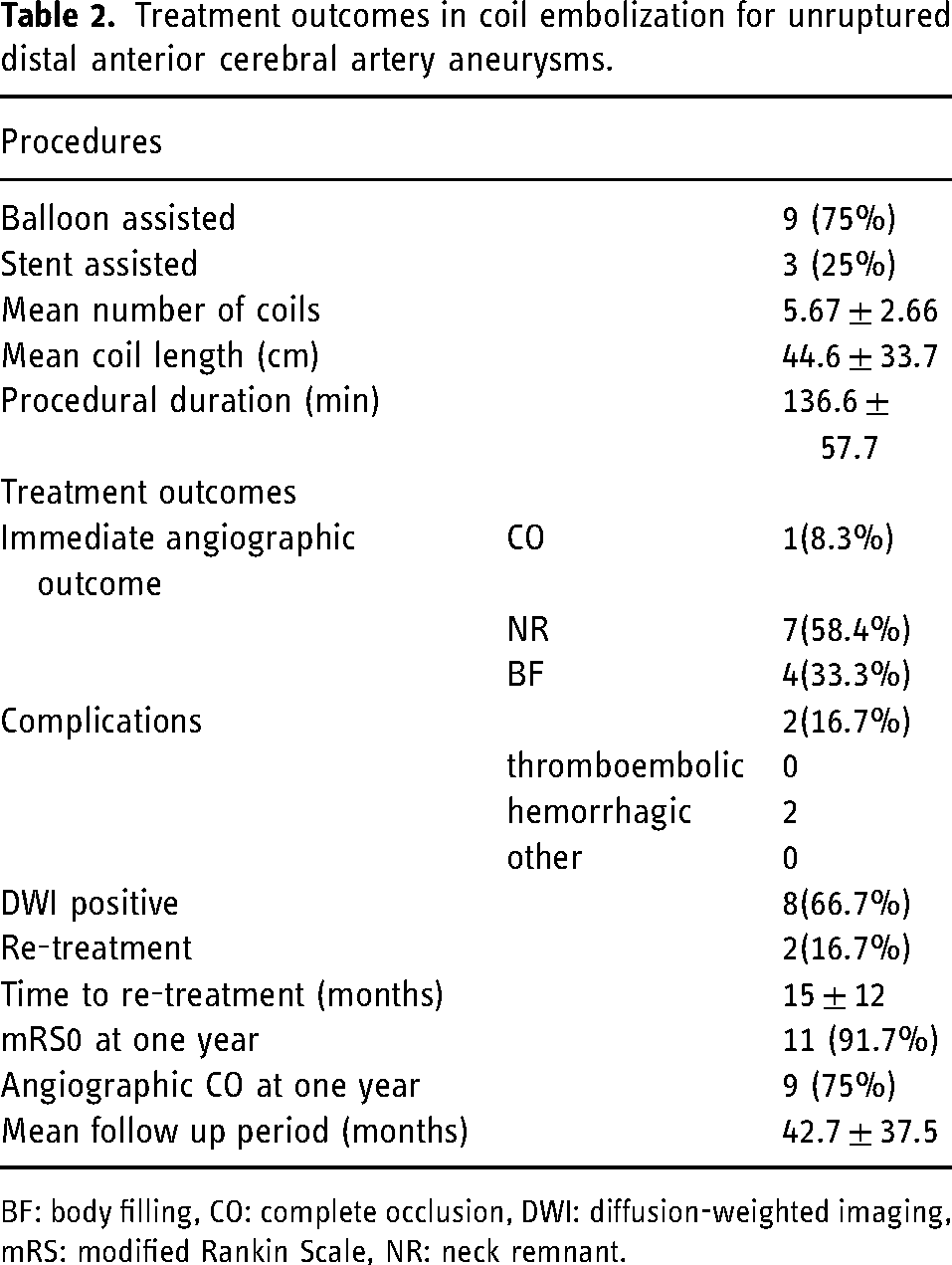
BF: body filling, CO: complete occlusion, DWI: diffusion-weighted imaging, mRS: modified Rankin Scale, NR: neck remnant.
Patient characteristics, radiological characteristics of aneurysms, and treatment outcomes in the DWI-positive and DWI-negative groups are summarized in Table 3. Age, sex, medical history, smoking habits, antiplatelet drug therapy (mono or dual), aneurysmal characteristics (size, neck size, aspect ratio, D/N ratio), stent-assisted technique, procedural duration, and immediate angiographic CO were compared between the groups. Univariate analysis showed no significant differences in any of the factors including procedural duration; however, age tended to be higher in the DWI-positive group (P = 0.07)
Patient characteristics, radiological characteristics of aneurysms, and treatment outcomes in the DWI-positive and DWI-negative groups.
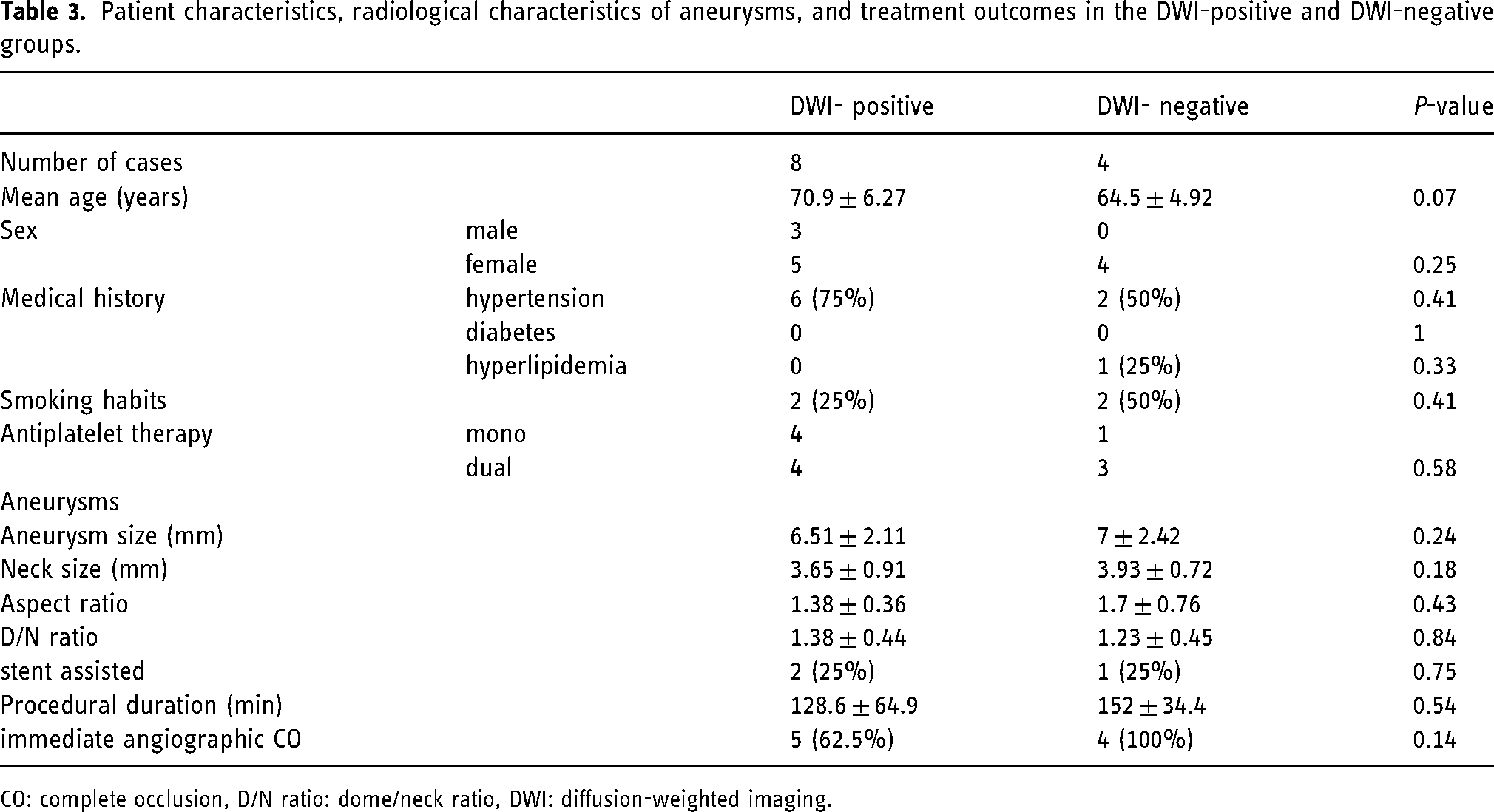
CO: complete occlusion, D/N ratio: dome/neck ratio, DWI: diffusion-weighted imaging.
The morphological characteristics of the two groups are summarized in Table 4. The comparison between the two groups showed that GOA was significantly smaller in the DWI-positive group (172.6 ± 17.7° vs. 216.8 ± 16.8°, P < 0.01), in the univariate analysis. There were no significant between-group differences in other factors; however, A2-3D tended to be smaller in the DWI-positive group (P = 0.09). The optimal cut-off value of GOA was determined using the receiver operating characteristic curve with Youden's index; the point where the value of sensitivity + specificity −1 was maximum was set as the cutoff value and was set to 195° for multivariate analysis. The predictors of silent ischemic events in the multivariate analysis are summarized in Table 5. The cut-off value of predictors was also determined using receiver operating characteristic curves with Youden's index (A2–3D: 0.5). Multivariate analysis, which included factors such as age, A2–3D, and a small GOA (GOA <195°), showed that small GOA was a significant predictor of silent ischemic events (P = 0.04; odds ratio: 23.62, 95% confidence interval: 1.11–490.39).
The morphological characteristics of the DWI-positive and DWI-negative groups.
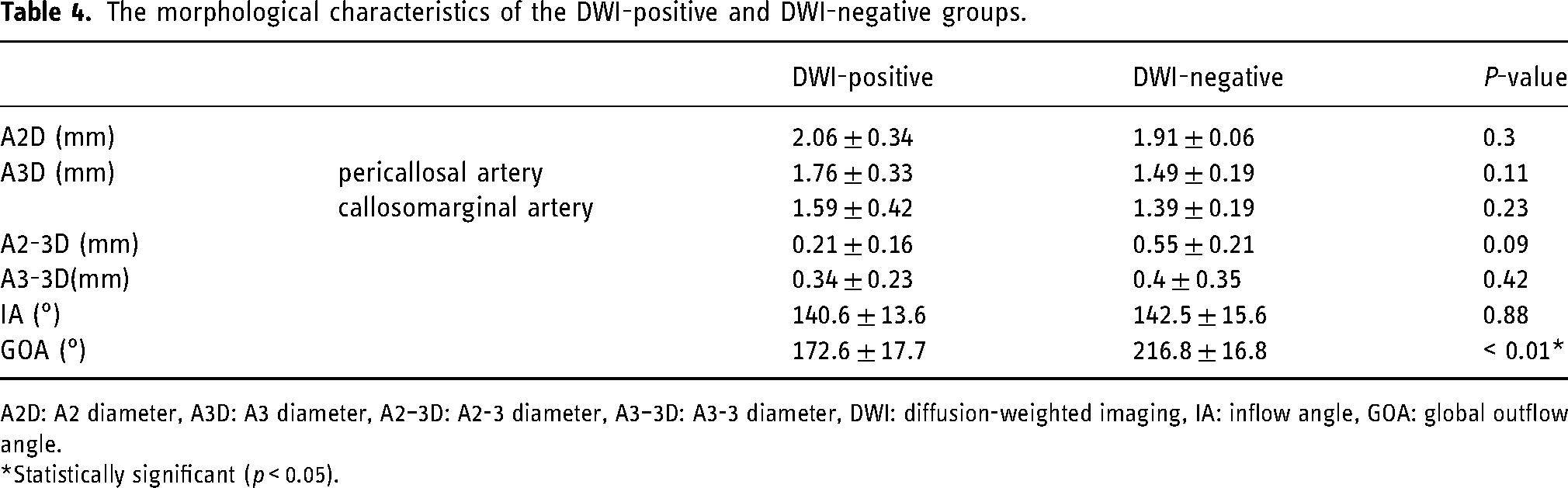
A2D: A2 diameter, A3D: A3 diameter, A2–3D: A2-3 diameter, A3–3D: A3-3 diameter, DWI: diffusion-weighted imaging, IA: inflow angle, GOA: global outflow angle.
*Statistically significant (p < 0.05).
The predictors of silent ischaemic events in the multivariate analysis.
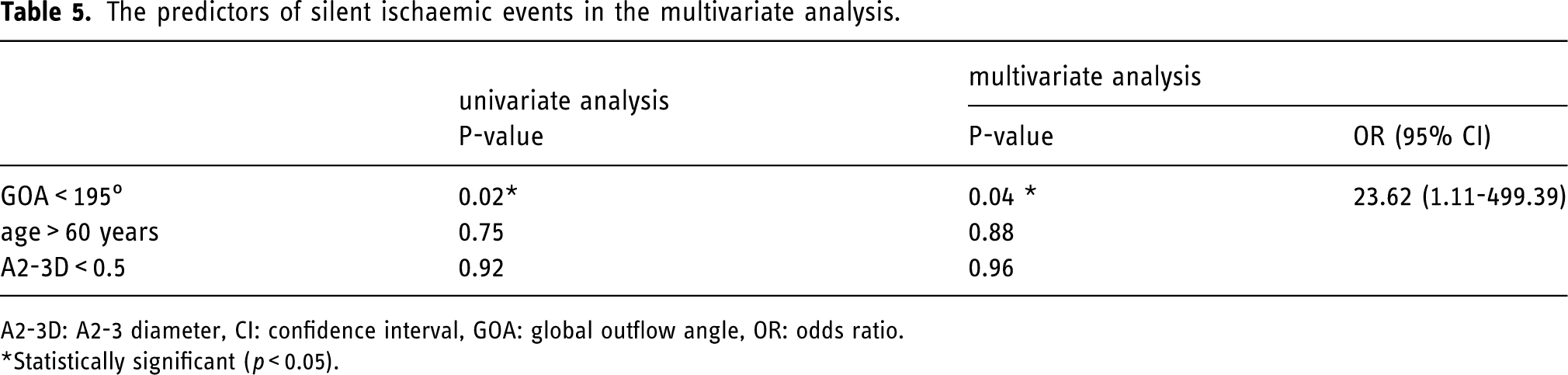
A2-3D: A2-3 diameter, CI: confidence interval, GOA: global outflow angle, OR: odds ratio.
*Statistically significant (p < 0.05).
Discussion
The frequency of treatment with coil embolization for aneurysms has increased since the commencement of International Subarachnoid Aneurysms Trial study. 23 However, coil embolization for DACA aneurysms remains challenging and therefore, controversial.
The treatment outcomes of coil embolization for DACA aneurysms from previous studies are summarized in Table 6.9,10,12,14–17 Most reports included ruptured aneurysms. In previous reports of coil embolization for DACA aneurysms, the rate of immediate angiographic CO has ranged from 23.1% to 100%.9,10,12,14–17 In the present study, the rate of immediate angiographic CO was 8.3%, and the rate of immediate angiographic CO and NR combined was 66.7%. However, the rate of angiographic CO at 1 year after the procedure was 75%, and rupture caused by treated aneurysm was not detected during the follow-up period.
The treatment outcomes od coil embolization for distal anterior cerebral artery aneurysms from previous studies.
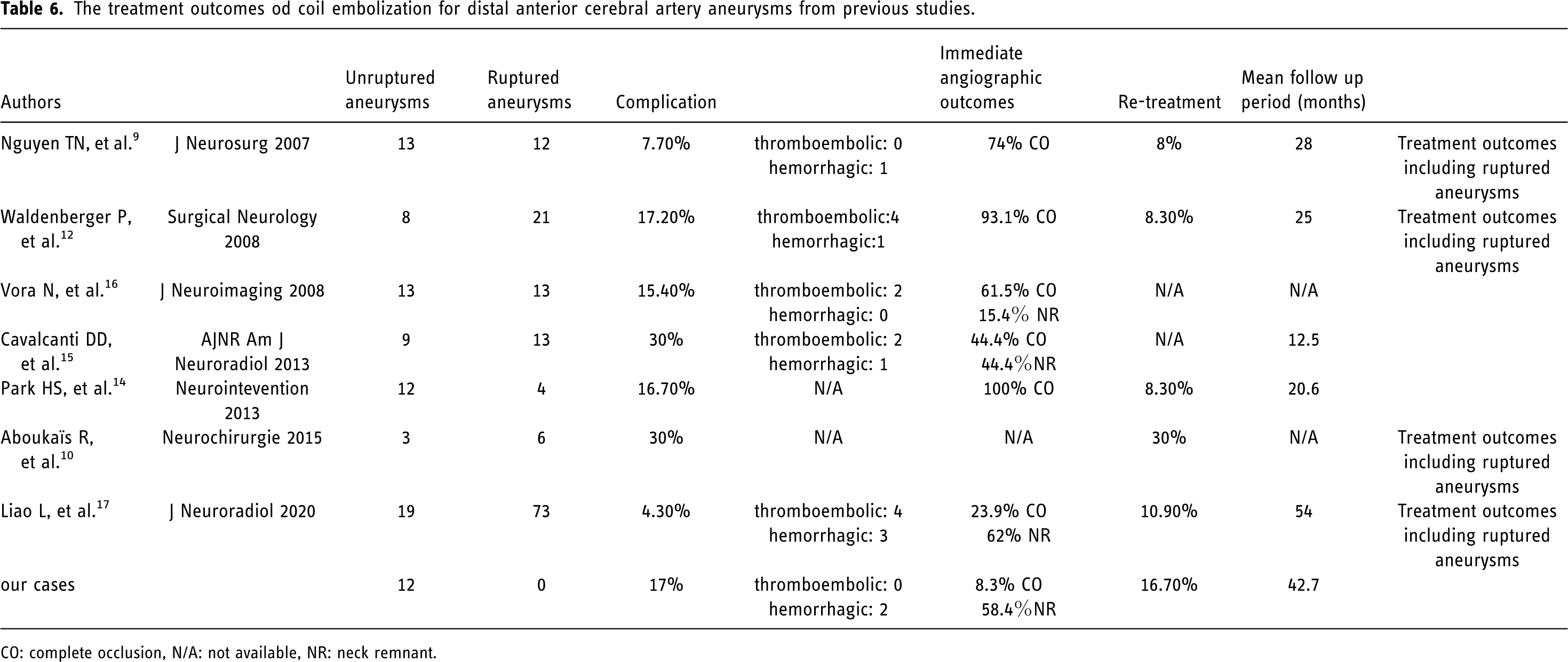
CO: complete occlusion, N/A: not available, NR: neck remnant.
The rate of re-treatment generally ranged from 8% to 30%.9,10,12,14–17 The rate of re-treatment was 16.7% in the present study.
The rate of perioperative complications has ranged from 4.2% to 17.2%.9,10,12,14–17 The rate of perioperative complications was 17% in the present study, similar to that reported in previous studies. In previous studies, the rate of procedure-related mortality was 2.9%–9%, and procedure-related morbidity was 8%.6,9,12 In the present study, the rate of procedure-related mortality was 0%, and procedure-related morbidity was 8.3%. There were more hemorrhagic complications than thromboembolic complications during coil embolization for DACA aneurysms in previous studies,9,14 while all complications were hemorrhagic in the present study. The rate of thromboembolic complications ranged from 0% to 17.2% in previous studies,9,10,12,16 however, no symptomatic thromboembolic complications were detected in the present study. Overall, the treatment outcomes of the present study are acceptable.
Generally, the predictors of thromboembolic events after coil embolization are ruptured aneurysm, bifurcation aneurysm, prolonged procedure time, 24 and the use of a balloon-assisted and stent-assisted technique. 25 It has been reported that the rate of silent ischemic events after coil embolization ranges from 10% to 77%.26–33 However, the rate of silent ischemic events after coil embolization, and predictors of thromboembolic events in coil embolization for DACA aneurysms have not been reported. The rate of silent ischemic events was 66.7% in the present study.
Predictors of silent ischemic events after coil embolization also include an increased number of devices, such as adjunctive 32 (stent-assisted, double balloon-assisted) and double-catheter 33 techniques, and ruptured aneurysm. 34 However, the long-term influence of silent ischemic events remains unclear.35,36 In the present study, all cases were treated using adjunctive techniques; most were treated using single balloon-assisted and single catheter technique, with a few being treated using stent-assisted technique.
The risk of aneurysmal rupture based on the morphological characteristics of aneurysms has been reported. 37 However, no study has investigated the association between thromboembolic events after coil embolization for DACA aneurysms and morphological characteristics. Our study focused on blood vessel diameters, such as A2D and A3D, however, no association was observed between thromboembolic events and vessel diameter. To date, no study has investigated the association between the morphological characteristics and treatment outcomes of coil embolization for DACA aneurysms. Our study also investigated the association between the two angles (IA and GOA) and silent ischemic events.
To the best of our knowledge, the present study is the first to investigate the association between GOA and silent ischemic events after coil embolization for DACA aneurysms. GOA <195° was a significant predictor of silent ischemic events in the present study. If the GOA is small, then the blood vessel shift of the A3 segment is enlarged upon device placement. Thus, when a device, such as a balloon or stent, is placed, the direction of blood flow changes, resulting in thrombus formation and, perhaps, increase in the risk of silent ischemic events. In addition, a small GOA makes it difficult to introduce the device into the A3 segment, and when the number of manipulating devices—such as the micro guide wire—is increased, the procedural duration may be prolonged; therefore, the risk of silent ischemic events may also increase; however, procedural duration was not predictor of silent ischemic events in this study. Hence, GOA is a useful predictor of silent ischemic events after coil embolization for unruptured DACA aneurysms.
Study limitations
This was a non-randomized, retrospective, single-center study with a small sample size. Therefore, the generalization of our results to wider populations may be limited.
Antiplatelet reactions were not examined because the VerifyNow system (Accumetrics, San Diego, California) is not approved in our country. Unavailable information regarding the patients’ response to clopidogrel is a major limitation for the stent-assisted coil embolization cases (n = 3). A non-responder to clopidogrel would be expected to show silent ischemic events.
As computational fluid dynamic analysis was not performed, changes in parameters during device insertion and placement could not be evaluated. Therefore, changes in the GOA during device insertion and placement have not been evaluated.
Conclusion
The predictors of silent ischemic events after coil embolization for unruptured DACA aneurysms were investigated in the present study; a small GOA was identified as a significant predictor of silent ischemic events. On the contrary, procedural duration was not predictor of silent ischemic events. It is unclear whether clipping or coil embolization is more effective for the treatment of unruptured DACA aneurysms. However, some cases can be treated safely with minimally invasive coil embolization, and it is important to identify these cases. Thus, the aneurysmal shape and neck diameter and evaluation of the GOA should be considered before the procedure. Surgical clipping should be considered as an alternative in patients at high risk of thromboembolic events after coil embolization.
Footnotes
Author contributors
Conceptualization: Suzuki R, Takigawa T; Writing original draft preparation: Suzuki R; Statistical analysis: Suzuki R; Data curation: Suzuki R, Nagaishi M; Methodology: Suzuki R, Nagaishi M; Writing-reviewing and editing: All authors; Administrative/technical/material support: Takigawa T, Hyodo A; Supervision: Hyodo A, Suzuki K.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent
This research has been approved by the Ethical Review Board at Dokkyo Medical University Saitama Medical Center (approval number: 2021). The requirement of informed consent was waived owing to the retrospective study design.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.