
Abstract
Background
Intraoperative magnetic resonance imaging system (iMRIS) surgical theatre is a highly integrated operating room with an intraoperative magnetic resonance imaging (iMRI) designed originally for brain tumour surgery. Its use in neurointerventional procedures, particularly in the setting of endovascular coiling of intracranial aneurysms, has not been discussed in the literature to date. We present our initial experience about the safety and feasibility of iMRI to assess post operative complications and provide baseline imaging post coiling of intracranial aneurysms.
Methods
Consecutive patients who underwent iMRI between 2015 and 2018 were included in the study. Demographic, clinical details, endovascular technique and surgical outcomes were collected. Details of anesthesia during the procedure were also collected.
Results
Fifteen patients underwent iMRI with MRA to assess post coiling status of their elective endovascular coiling of intracranial aneurysms. The mean age in this cohort was 61 years and 46.7% were male. No immediate complications were seen either from the endovascular procedures or from the iMRI. All iMRI scans were performed as planned with no aborted or truncated scans. The image quality of the iMRI/MRA was adequate to detect the residual aneurysm, if present. There was no residual aneurysm on the angiogram that were not detected on the iMRIs. Of the 15 patients, 10 were safely discharged the following day and other 5 were discharged 2 days after their surgery.
Conclusions
The iMRI is an advantageous tool which can be integrated into neurointerventional workflow resulting in early post peri-procedural feedback and potentially reduced post-operative hospital stay.
Background
Endovascular treatment with coils has become an established treatment technique for intracranial aneurysms with favourable outcome. 1 In the setting of elective coiling of intracranial aneurysms, patients usually undergo a baseline MRI and MR angiogram (MRA) before being discharged from hospital. They then undergo long term follow up MRI and MRA to monitor the stability of the treated aneurysm. The post coiling MRI provides an important assessment for any perioperative complications.2–4 In most centres, the baseline MRI/MRA is usually done the day after coiling the aneurysms. Getting this MRI/MRA done on the day of surgery presents significant logistical challenge in most hospitals.
Intraoperative magnetic resonance imaging system (iMRIS) is a multifunctional surgical theatre with the technology to transport an MRI scanner on a ceiling-mounted rail system between an operating room and adjacent diagnostic room,5–7 essentially bringing the MRI scan to the operating room and patient. The iMRIS magnet's initial intents were to help surgeons plan and obtain real time images without moving the anaesthetized patient.8–10 A new VISIUS Surgical Theatre features an MR scanner, a bi-plane angiography system and a neurosurgical operative room, where the MR scanner can be deployed into any of three rooms permitting rapid transitions between MR imaging, conventional surgery or endovascular intervention. 11 This also allows the MRI to be used for diagnostic purposes when not in use intraoperatively.
Use of intraoperative MRI (iMRI) has not been reported for use in the endovascular coiling of intracranial aneurysms. The purpose of this study is to report the safety and feasibility of iMRI for patients undergoing endovascular coiling of intracranial aneurysms.
Methods
The study was approved by our institutional research ethics board (REB number- H2019:019) with waiver of consent. The study was done at a tertiary neurosciences centre which is the fifth centre in North America equipped with a VISIUS Surgical Theatre. This includes a biplane angiography suite (Axium Artis, Siemens Medical Solutions USA, Inc) and 3 tesla MRI scanner (MAGNETOM Verio, Siemens Medical Solutions USA, Inc).
The interventional neuroradiology database was searched to identify patients who have undergone iMRI. We included consecutive patients who underwent iMRI between 2015 and 2018. The other patients with endovascular coiling for elective intracranial aneurysms were followed up with conventional method i.e., post-surgical MRI in 1–3 days. Demographic, clinical details, endovascular technique and surgical outcomes were collected. Details of anesthesia during the procedure were also collected.
All patients were preplanned to undergo iMRI immediately after the endovascular coiling of their aneurysms. Standard patient positioning, draping and devices were used for the endovascular procedure. The patient was informed and consented for the addition of iMRI planned to immediately follow the endovascular procedure. As is the standard in the surgical theatre, a complete count of devices, particularly metallic needles, wires and instruments was performed before, during and after in accordance with standard MRI room safety protocols. The room itself was marked with standard gauss lines with monitoring and anesthetic equipment all meeting MRI room standards. At the end of the procedure, all catheters, wires and procedural equipment were removed from the room. Hemostasis at the groin site was confirmed in standard fashion. The patient was kept draped and under general anesthesia during the iMRI with a clinical nurse and anesthesiologist remaining, with all other personnel moved to the control room. The iMRI was followed the same imaging protocol as our regular MRI protocol for baseline imaging after endovascular coiling of intracranial aneurysms. The sequences acquired included Sagital T1, axial FLAIR, DWI/ADC and post-gadolinium T1 weighted images of the brain. A 3D time-of–flight MR angiogram and contrast enhanced MR angiogram of the circle of Willis were performed at the same time. These MRI studies were tagged as ‘STAT’ and were reported by fellowship trained neuroradiologists within 1-2 h from the image acquisition. In addition, the interventional neuroradiologists participating in the coiling were present at the time of iMRI and were available for real time interpretation of the images and consultation.
Anesthesia considerations- All patients were assessed in the pre-anesthesia clinic by the attending anesthesiologist two to three weeks prior to the surgery. In addition to standard assessment, all patients were evaluated for the MRI compatibility. On the day of surgery, all patients were screened by nursing, anesthesia and radiological team. The anesthesia check list (needle, equipment etc. counts) was performed by the anesthesiologist at three points: preoperative, before iMRI, and after iMRI. The standard anesthesia technique was utilized for all patients planned for iMRI after the coiling procedure. Detailed anesthesia protocol from our institution has been published. 12 At the conclusion of the surgery, all patients were reversed and extubated smoothly.
Statistics- Simple observational summary statistics were done to report the mean and percentages.
Results
A total of 15 patients underwent iMRI immediately after elective endovascular coiling of intracranial aneurysms between 2015 and 2018. Patient demographics and preoperative characteristics as in Table 1.
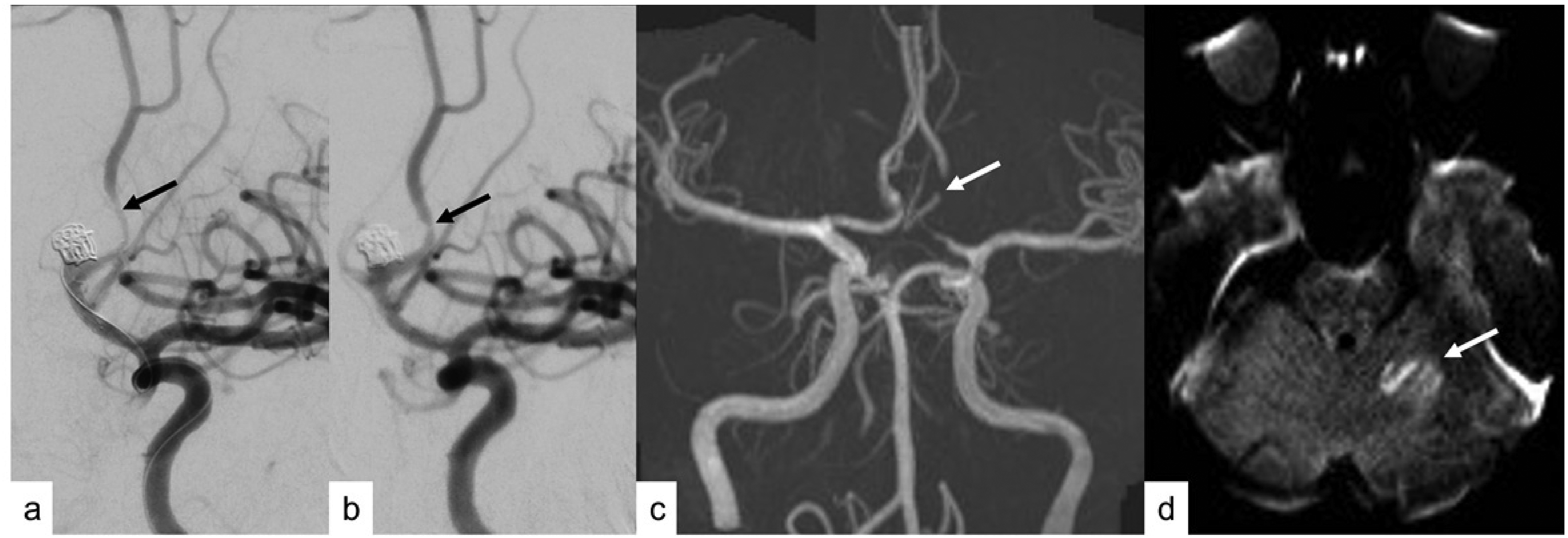
Demographic, clinical and technical details of all patients treated with endovascular coiling of intracranial aneurysms that underwent intra-operative MRI (iMRI).
ACom- Anterior Communicating artery; MCA- Middle Cerebral artery; PCom- Posterior Communicating Artery; CTA- Computed Tomographic Angiography; MRA- Magnetic Resonance Angiography, iMRI- intraoperative MRI; DWI- diffusion weighted imaging.
The mean age in this cohort was 61 years and 46.7% were male. All patients underwent elective treatment of their unruptured aneurysms except one patient who had a remote history of subarachnoid hemorrhage. Three patients (20.0%) had undergone prior endovascular coiling of the same cerebral aneurysm. Twelve (80%) aneurysms were located in the anterior circulation and three (20%) in the posterior circulation. The average size of treated aneurysm was 6.6 mm (range from 3–11 mm). Seven patients (46.7%) had small residual/recurrent neck post procedure either on immediate or on long term follow up imaging. No immediate complications were seen either from the endovascular procedures or from the iMRI. All iMRI scans were performed as planned with no aborted or truncated scans. In one patient, small residual sac was demonstrated intra-operatively by angiogram and baseline iMRI, that remained stable on follow up (1/15) (Figure 1). The image quality of the iMRI/MRA was adequate to detect the residual aneurysm, if present. There was no residual aneurysm on the angiogram that were not detected on the iMRIs. Of the 15 patients, 10 were safely discharged the following day and other 5 were discharged 2 days after their surgeries. In one patient, left ACA had spasm post stent placement that improved with intra-arterial verapamil (Figure 2). The residual vasospasm was re-demonstrated on the time-of-flight images on iMRI (Figure 2). This helped guide aggressiveness of post operative care, blood pressure goals, fluid balance. This patient also had an asymptomatic small embolic infarct in the left cerebellum (Figure 2).
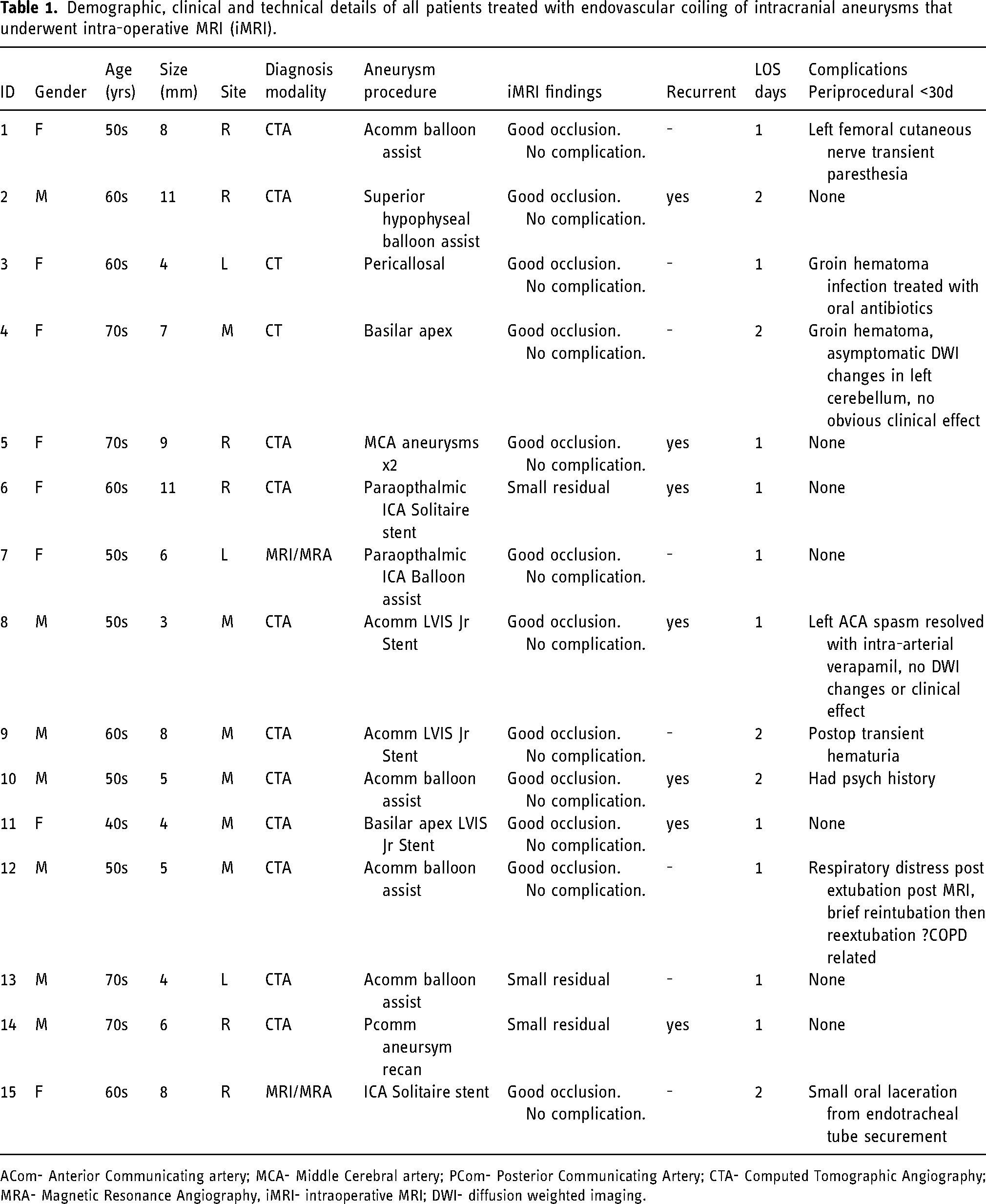
Recurrence of previously coiled (a) right posterior communicating artery aneurysm (arrow). Immediate post-treatment angiogram (b) showed no or minimal residual filling of the aneurysm neck (arrow). The iMRI showed small residual filling (arrow) at the neck on (c) time-of-flight MR angiogram and (d) contrast enhanced MR angiogram.
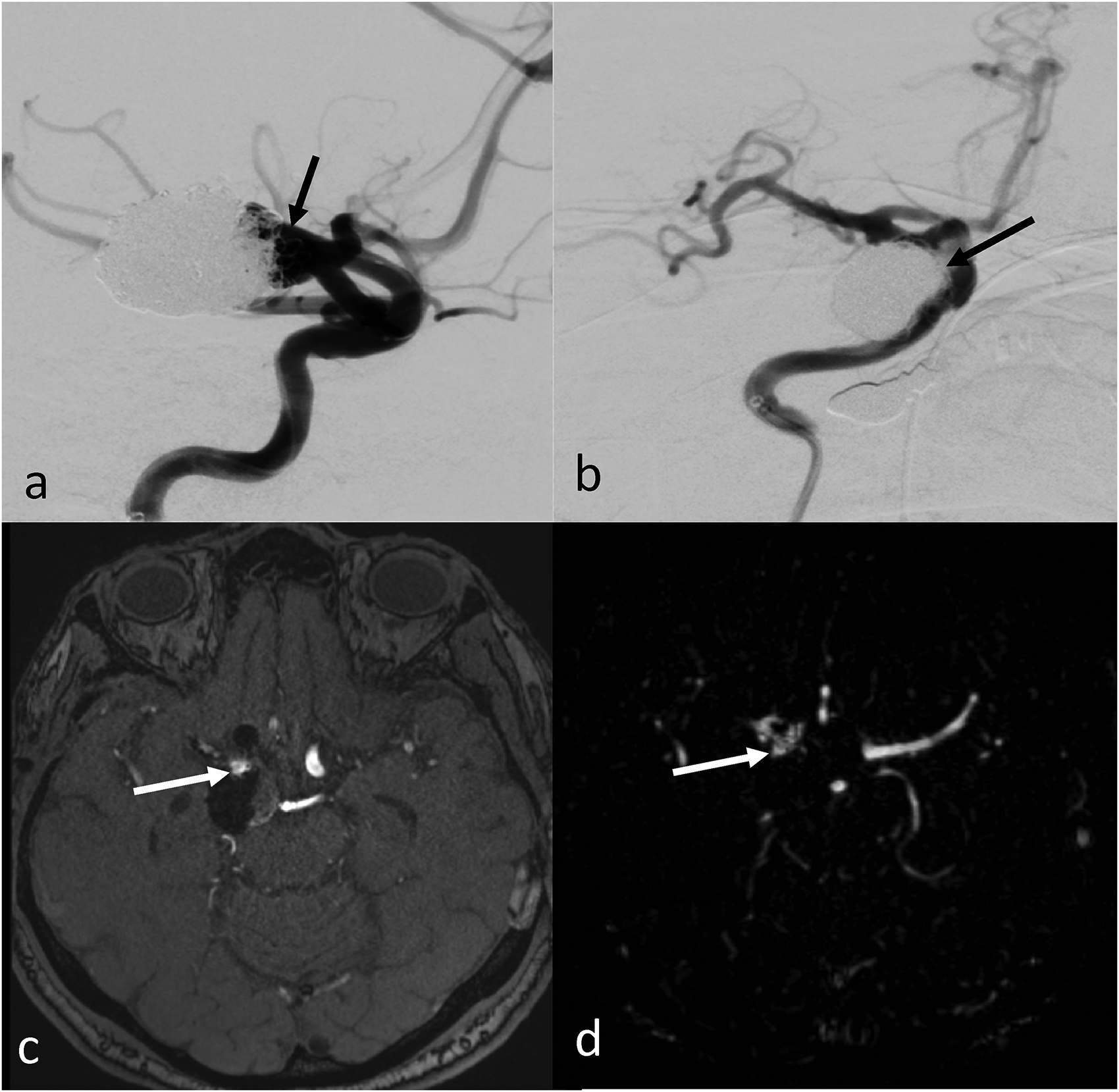
Patient with coiling of (a) an anterior communicating artery aneurysm developed spasm secondary to stent placement (arrow). (b)The spasm improved with intra-arterial verapamil with focal residual spasm (arrow). (c)The residual vasospasm (arrow) was also seen on the time-of-flight MR angiogram done as part of intra-op MRI (iMRI). (d) The iMRI also showed a clinically silent left cerebellar small embolic infarct (arrow) on diffusion weighted images.
Discussion
We report a series of patients with intracranial aneurysms where iMRI was used intraprocedurally immediately after coiling. To our knowledge, this is the first description of the usage of iMRI for an elective endovascular coiling of intracranial aneurysms. Although iMRI is still growing in its availability, our study confirms the feasibility and safety of iMRI for such procedures.
Performing iMRI is logistically complex if the patient needs to be moved to an MRI under anesthesia. With the IMRIS facility, the patient remains on the table and the MRI machine moves to the patient's table. This has been proven to be a game changer in iMRI for tumour surgery. In centres, where iMRI facility is available, it can be used to assess the intracranial aneurysms immediately after the endovascular coiling. The current iMRI could perform the same imaging sequences as our clinical MRI. This obviates the need for baseline MRI in these patients on the immediate postoperative day and also helps ease the case load on the clinical MRI scanner. By performing the baseline MRI in the operative room, this could potentially reduce the hospital stay of these patients by at least one day. Although the length of stay did not change in our study, it could potentially happen in the future. This could save significant health care resources. The strategic and financial benefits of day surgery in the endovascular setting are desirable. However, this is limited due to few availability of iMRI. It remains to be seen if such saving in health care resources could offset the upfront implementation cost of iMRI.
Presurgical planning- In addition to various considerations related to intracranial aneurysm, subarachnoid hemorrhage and coiling procedure, there are multiple key issues related to this combined coiling and iMRI technique.12–14 Firstly, all implication related to iMRI suite including long extensions for IV lines, and breathing circuits, MRI compatibility, interference with monitoring, effect of monitoring system on MRI images, limited access to airway and noise interference should be carefully planned and assessed. Secondly, anesthesia check list should be screened properly. Thirdly, the duration of anesthesia usually gets prolonged by an hour or so and this is attributed to preparatory time, performing check list from multiple stakeholders, imaging time etc. This increase in anesthesia time could potentially have complications, although very rare. Hemostasis at the groin site was secured using standard process. In case of any complications, these can be dealt with while the patient is still on the table in the suite with surgical team around. Due to the missile effects of small metallic objects under MRI, the safety of patient as well as all team members remains crucial and should be ensured with continuous vigilance and effective communication.
Detecting early changes on MRI could potentially change patient management. In our series, one patient showed vasospasm in anterior cerebral artery on iMRI. This patient was managed aggressively with fluid and vasopressors in the post-operative period. Although these complications are rare, early detection results in optimum patient management.
Limitation- Our study had all the limitations of a small retrospective study. Our study did not assess the financial implication of iMRI in patients undergoing endovascular treatment of intracranial aneurysms. All patient in our study underwent an elective endovascular coiling of their aneurysms. We could not assess safety and feasibility of iMRI in patients with endovascular treatment of ruptured intracranial aneurysms. The iMRI could block the angio room for the duration of iMRI and a back-up room should be available for urgent cases. In the absence of back-up room, the iMRI needs to be aborted to facilitate any emergency cases.
Conclusion- An iMRI is feasible and can be safely used for immediate assessment of post endovascular aneurysm coiling patients and provide a baseline post-op MRI to assess any residual neck. They could potentially reduce the length of postoperative hospital stay for these patients.
Footnotes
Statement of authorship
YY, TC and ZK- data collection and Manuscript writing; JS- Conceptualization, manuscript writing and review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
“All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards”.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.