
Abstract
A 54-year-old man noticed right-sided pulsatile tinnitus for the past six months and recently started experiencing transient visual obscurations when standing up. MRI demonstrated two separate brain dural arteriovenous fistulas (bdAVF) in sagittal and right sigmoid dural sinuses. Neuro-ophthalmological exam demonstrated severe bilateral optic disc edema with preserved visual acuity but early nerve fiber bundle defects on visual field testing. Hypercoagulable profile testing revealed very elevated D-dimer, significantly decreased protein S level and elevated homocysteine levels. This case highlights importance of referring all patients with bdAVFs for neuro-ophthalmological consultation as venous hypertension can cause increased intracranial pressure and resultant papilledema. Papilledema does not affect central vision until late stages when visual loss is irreversible thus screening for its presence and pre-treatment extent of peripheral visual loss is paramount. It also demonstrates that hypercoagulable workup should be initiated in all patients with bdAVF in order to prevent future thromboembolic events.
Case
A 54-year-old man noticed right-sided pulsatile tinnitus for the past 6 months. He had a history of obstructive sleep apnea treated with continuous positive airway pressure device and psoriasis treated with topical betamethasone cream. He also had a longstanding history of migraines with auras, however, for the past 3 months he has been waking up with mild headache and noticed transient visual obscurations on awakening. Magnetic resonance imaging (MRI) of the brain with magnetic resonance angiography/venography (MRA, MRV) demonstrated trans-osseus vascular channels in the occipital region, with hyperintensity in the distal aspect of the superior sagittal sinus, torculum herophili, and right sigmoid sinus, suggestive of brain dural arteriovenous fistulas (bdAVF). There was also lack of flow void in the right transverse and sigmoid sinus and mild chronic ischemic microangiopathic disease with hemosiderin deposition in the right superior frontal and left middle frontal gyrus (Figure 1).
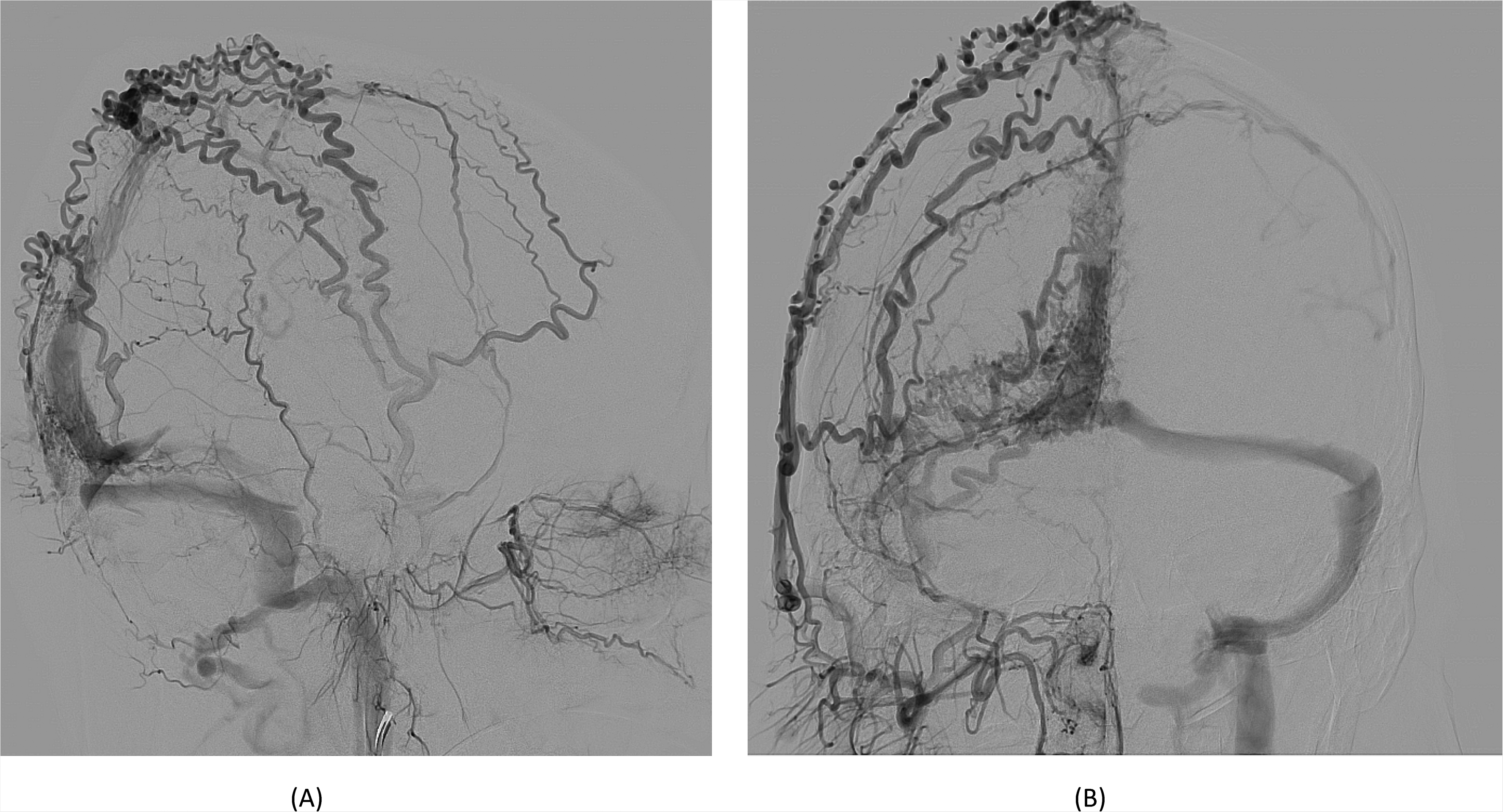
A – lateral image and B – anterior-posterior image, both from a right external carotid artery angiogram showing brain dural arteriovenous fistula (bDAVD)with two discrete fistulous points. One fistulous point is close to the torcula and the other in the middle third of the superior saggital sinus. The torcula bDAVF has arterial supply via right and left occipital artery branches (not shown), draining into torcula, with retrograde flow into straight sinus. The sagittal sinus bDAVF has arterial supply from branches of the right and left MMA, right and left STA, left occipital and falcine artery arising from the left opthalmic artery (not shown). Venous drainage is into left parietal cortical veins and sagittal sinus.
He was referred for neuro-ophthalmic evaluation which revealed central vision of 20/25 in each eye and no relative afferent pupillary defect. Ocular motility was full and eyes were orthophoric on alignment testing. Ophthalmoscopy though demonstrated severe disc edema bilaterally (Figure 2). Formal visual fields demonstrated enlarged blind spots in both eyes with mean deviation of −3 dB and −3.9 dB (Figure 3). Peripapillary optical coherence tomography demonstrated severe elevation of retinal nerve fiber layer with average thickness of 300 and 279 microns (Figure 4). Diagnosis of two separate bdAVFs that resulted in increased intracranial venous pressure and thus severe papilledema was made. Extensive hypercoagulable workup revealed presence of very elevated D-dimer 1.11 mg/L, normal 0-0.49), elevated homocysteine (20 mcmol/L, normal <15) and significantly decreased protein S level (0.2 uml, normal 0.59-1.26). Urgent endovascular embolization of the bdAVFs was performed resulting in resolution of papilledema 1 month later.
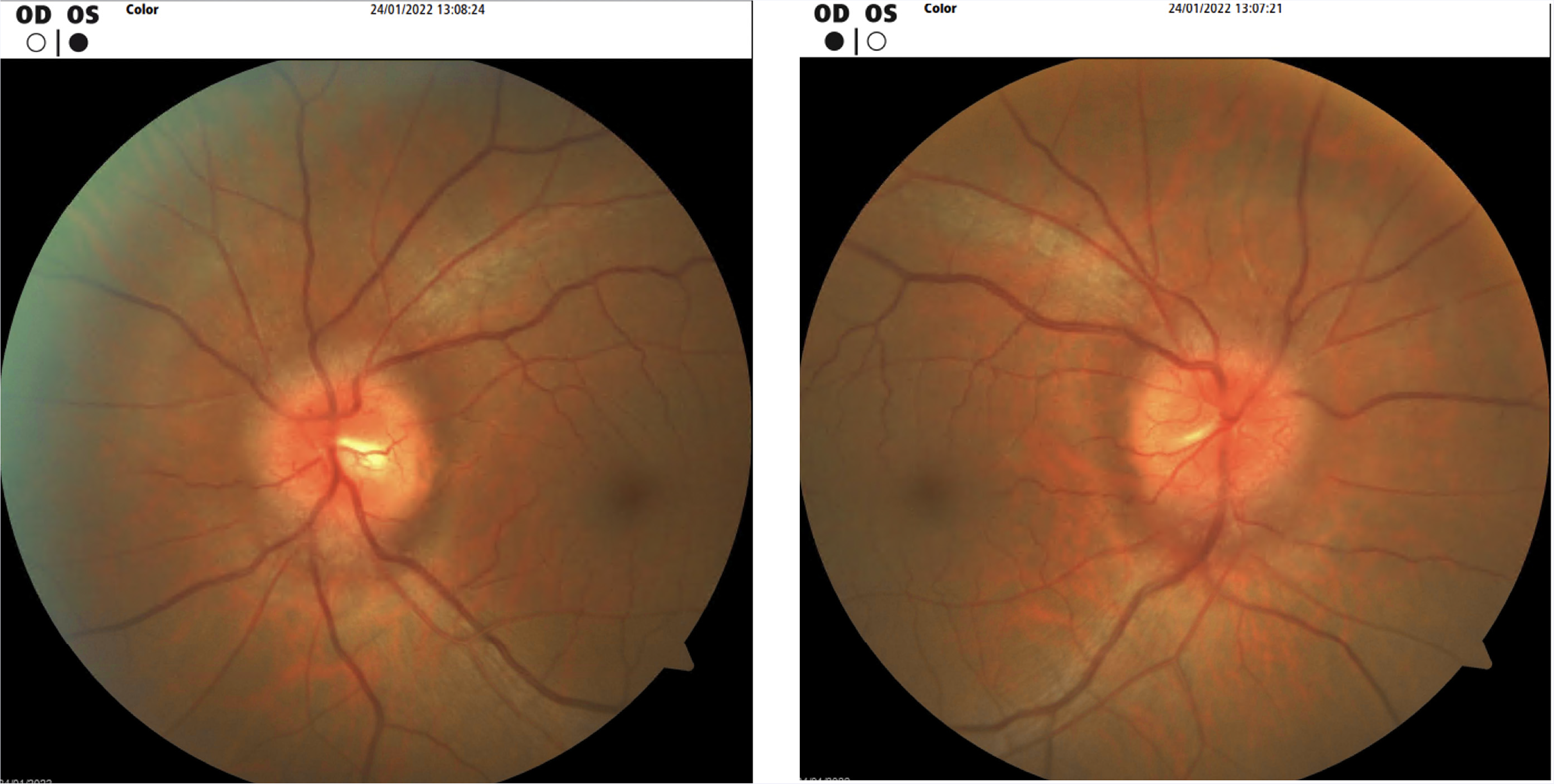
Fundus photograph demonstrating bilateral severe optic nerve head edema.
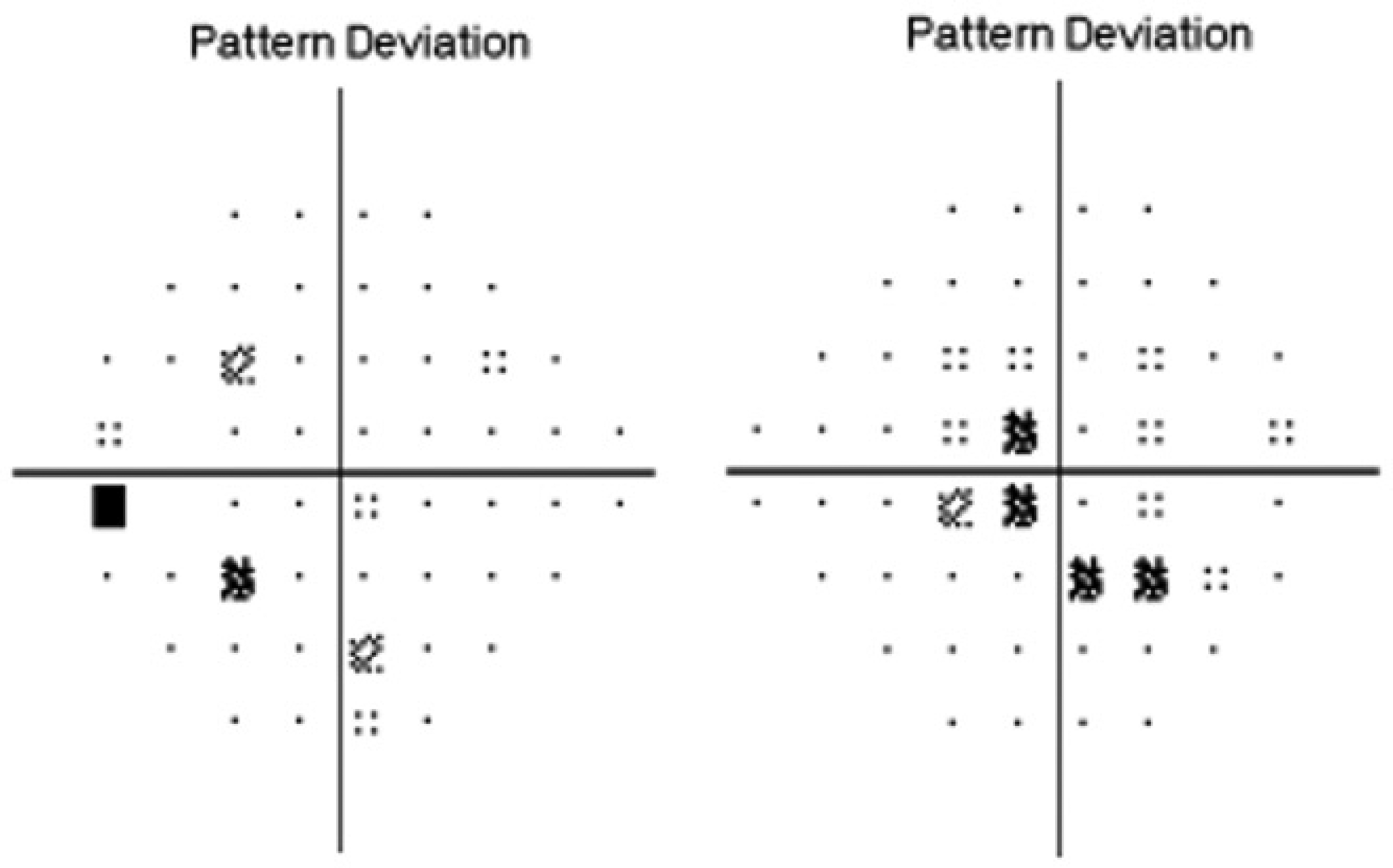
Humphrey visual fields (24 algorithm, pattern deviation printout) of the right (on the right) and left (on the left) eye demonstrating early nerve fiber bundle defects, greater in the right eye.
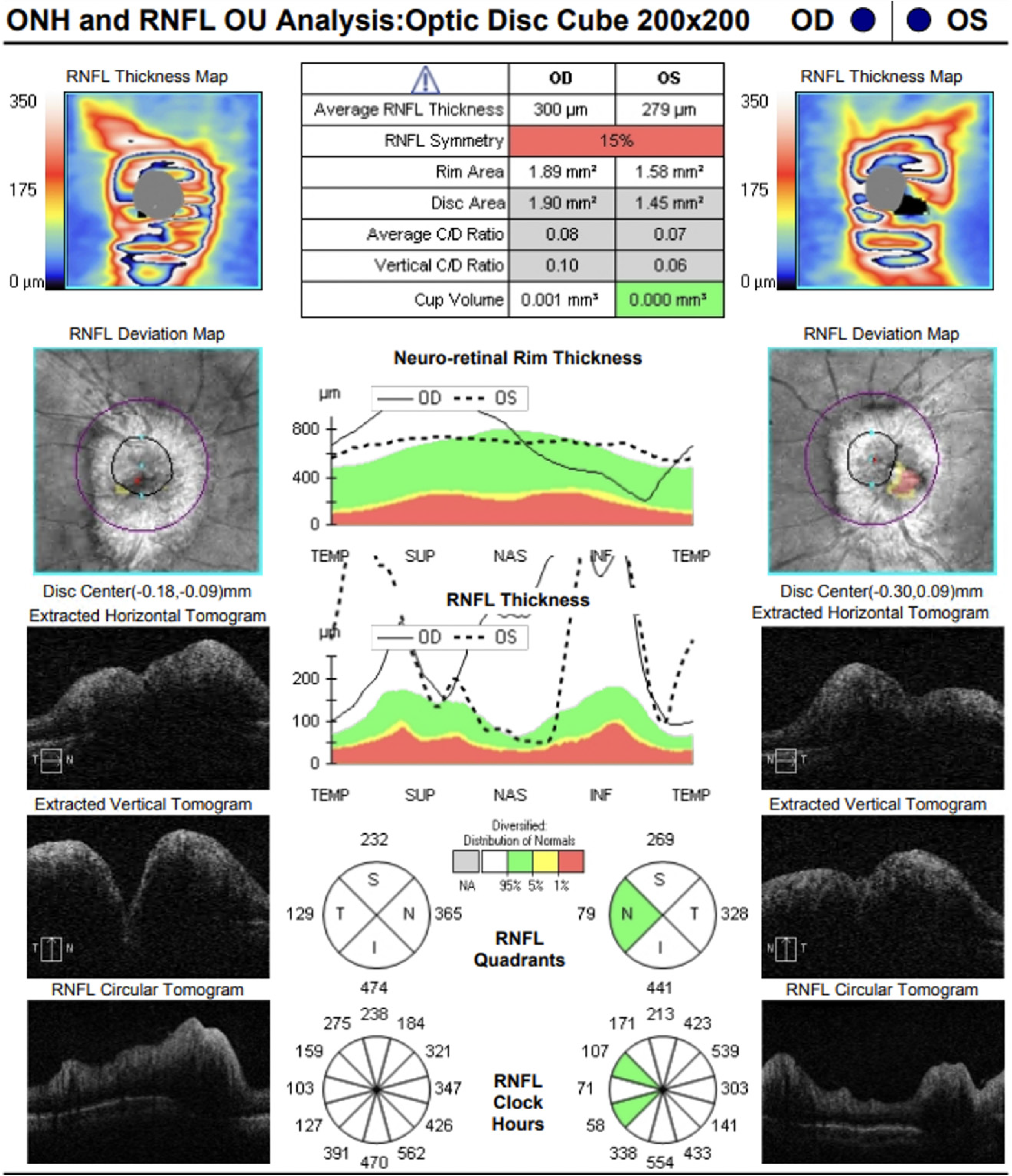
Peripapillary ocular coherence tomography demonstrating severe elevation of peripapillary retinal nerve fiber layer in each eye.
Discussion
As bdAVFs are typically caused by abnormal communication between one of the meningeal arteries and one or several dural venous sinuses, they can lead to the so-called “arterialization” of dural sinuses and thus decreased venous outflow from the brain. This in turn can lead to papilledema as intracranial pressure rises.1,2 One study looked at 12 patients who were diagnosed with bdAVF and had symptoms of increased intracranial pressure and found that 8/12 had papilledema and 4/12 already developed optic atrophy as a consequence of long standing papilledema. 3 Thus, as patients with papilledema will most often have no visual complaints because it spares central vision initially and causes slow peripheral vision loss until optic atrophy develops, it is paramount that all patients with presumed bdAVFs be referred for neuro-ophthalmic evaluation to document the extent of their visual field loss prior to interventional procedure being performed.4,5 If left untreated, papilledema will progress to irreversible peripheral vision loss in almost all cases.
Patients with bdAVFs should also undergo a detailed hypercoagulable work-up. Previous studies have demonstrated a strong association between bdAVFs and underlying hypercoagulable state, the main hypothesis being that venous thrombosis is the first inciting event in patients with bdAVF which then causes venous hypertension and eventual angiogenesis thus creating vascular shunts. 6 However, some have proposed that the arteriovenous malformation may precede venous thrombosis, which then occurs as a result of prolonged hypertension and hypertrophy of the venous sinus 7 Suggested hypercoagulable work up should address situational, inheritable, and acquired risk factors. Situational factors include long periods of immobility, oral contraceptive use, chemotherapy, and heparin-induced thrombocytopenia. Inheritable risk factors have been well documented and include defects in clotting factors such as Factor V Leiden, Protein C/S deficiency, prothrombin gene mutation, antithrombin deficiency. The list of acquired hypercoagulable states includes but is not limited to cancer, recent surgery, pregnancy, membranous glomerulopathy, inflammatory bowel disease, antiphospholipid syndrome, and more.6,8–10
Previous studies have investigated the co-occurrence of an underlying hypercoagulable state with bdAVFs. In recent studies that measure the prevalence of hereditable risk factors with bdAVFs, Factor V Leiden and prothrombin gene mutations were the most common thrombophilic mutations identified, being present in 33% and 48% of a two separate study populations with bdAVFs.8,9,11 However, other studies have described the prevalence of bdAVFs with other heritable thrombophilias such as protein C/S deficiency and hyperhomocysteinemia, though rates tend to vary from 25–45% across these studies due to small sample sizes.12,13 To our knowledge, there are no studies investigating the prevalence of acquired hypercoagulable risk factors in patients with bdAVFs and this remains an area for further research. Presence of hypercoagulable state associated with bdAVFs can significantly impact the clinical care as these patients can develop deep vein thromboses, pulmonary embolism, dural sinus thrombosis, and cancer.
In summary, we described a patient with bdAVF who had severe papilledema due to resultant intracranial venous hypertension. As central vision in patients with papilledema is preserved until optic atrophy develops at which point the visual loss is irreversible, all patients with newly diagnosed bdAVF should be screened for its presence. This will also document the baseline extent of the peripheral vision loss prior to bdAVF treatment and preclude further association of visual loss with endovascular embolization procedure. Finally, we highlight importance of screening all patients with bdAVF for the presence of underlying hypercoagulable state as its prevalence in these patients is high presumably due to dural sinus thrombosis developing first and then its recanalization leading to formation of bdAVF.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.