
Abstract
Background
Spinal catheter angiography is commonly performed in the evaluation and treatment of spinal vascular lesions. The typical approach to spinal angiography consists of access through the femoral artery with the use of suitably shaped catheters for selective catheterization of the spinal segmental vasculature. The purpose of our study was to evaluate the safety and feasibility of distal transradial access through the “anatomical snuffbox” for targeted spinal angiography, for the investigation and treatment of selected spinal lesions
Methods
A retrospective review of patients who underwent transradial spinal angiography and embolization was performed from August 2019 to January 2022. A total of eight patients were identified, who underwent targeted spinal angiography through distal transradial access. Outcome measures were documented in a tabular manner.
Results
Radial access was successful in all patients. Seven patients had vascular tumors of the spinal column and underwent tumor embolization followed by segmental artery occlusion prior to surgery. One patient had a spinal dural AV fistula that could not be embolized due to feeding vessel tortuosity and eventually went on to have a laminectomy. Mean fluoroscopy time was 31.4 min. There were no access site hemorrhagic complications. One patient experienced transient mild hand numbness during the period of hemostasis with the vascular compression device that resolved completely within 24 h.
Conclusions
Distal transradial access is a feasible and safe option for targeted spinal angiography and treatment in selected patients.
Introduction
Spinal angiography is performed for various indications to evaluate and treat vascular diseases of the spine and spinal cord. Common indications include localization of sites of arteriovenous (AV) shunting in cases of spinal dural AVFs prior to definitive management, evaluation, and treatment of spinal cord AVMs and pial AVFs as well as the pre-operative evaluation of hyper-vascular secondary neoplastic lesions of the spine prior to surgical resection. Therapeutic embolization may also be performed to limit intra-operative bleeding during extra-periosteal approaches for en-bloc resection in primary bone tumors.
Angiography of the spinal neuraxis can be an onerous exercise given the need to evaluate multiple spinal segmental arteries. With advancements in cross-sectional vascular imaging, pre-procedure radiological localization helps target potential sites for selective angiography and targeted therapy, with reduced overall angiography time, radiation dose and contrast load. But in cases of ambiguity, complete spinal angiography is mandatory for lesions that have a high degree of suspicion based on known MRI features of the same.
Most cases are performed with specifically shaped catheters through a percutaneous transfemoral approach. There is growing interest amongst neurointerventionalists to approach vascular access through a transradial approach.1–4 This has been primarily driven by the cardiology community where there is an increasing push to adopt a radial-first approach for coronary interventions.5,6
More recently, accessing the radial artery distally through the anatomical snuffbox has been gaining traction due to its many advantages over traditional proximal radial access. Although solid randomized data are still lacking, published data so far report faster access site hemostasis and lower radial artery occlusion rates. Because of the well collateralized blood supply to the fingers, hand ischemia due to radial artery occlusion is rare. Added advantages of this technique are preservation of the proximal vessel for future arterial access, graft harvesting for surgical conduits and AV fistula creation in hemodialysis patients.
We report our experience in eight cases where the radial artery was used for targeted spinal angiography and embolization. Seven of the patients were referred prior to spinal surgery for targeted evaluation and pre-operative embolization before en-bloc or intralesional resection and instrumented stabilization for bone tumors. All these patients additionally underwent segmental arterial embolization. One patient was scheduled for selective spinal angiography and embolization of a spinal dural AV fistula. Embolization was not successful due to vascular tortuosity precluding stable microcatheter positioning and surgical disconnection of the fistula was performed.
Methods
A retrospective review of patients who underwent transradial spinal angiography and embolization was performed from August 2019 to January 2022. Institutional Review Board approval was obtained for retrospective review of data from our prospectively maintained database. Eight patients were identified in total who had successful distal transradial access for targeted spinal angiography. Patient demographics, imaging data and procedural metrics were reviewed. All procedures were performed in a biplane neuroangiography unit (Siemens Axiom, Erlangen, Germany).
Technique
Informed consent was obtained from all patients and the procedures were performed under general anesthesia. Muscular paralysis was utilized to obtain motion-free DSA runs with controlled breath hold for precise evaluation of anterior spinal artery at each segmental level.
Distal transradial access was successfully obtained in all eight patients, with no access site crossovers. The technique for distal radial access has been previously well described. 7 In cases where left-sided access was obtained, the arm was adducted and brought to the midline in a sterile manner while in a pronated position to facilitate access from the right side of the patient. Once left-sided access was obtained and the catheter was introduced into the sheath, the left hand was positioned away from the radiation field. A Glidesheath slender sheath was used in all cases (Terumo Medical Corporation, Somerset, NJ). Angiography was performed at pre-determined levels based on prior imaging with special attention to spinal artery supply from the segmental branches as well as adjacent levels prior to any particle or liquid agent embolization.
Choosing appropriately shaped catheters for segmental artery catheterization from the radial approach can be challenging. In our experience the Bentson-Hanafee-Wilson 2 shaped catheter (Terumo Medical Corporation, Somerset, NJ) works best from a transradial approach, especially in younger individuals. The tip configuration is relatively neutral for a variety of segmental artery take-off angles and gives reasonable support against the opposite aortic wall. Reverse curve catheters may be necessary (Simmons, Mikaelson and Mani shaped catheters) in cases with patulous aortas, and for higher thoracic levels. Pre-procedure cross sectional imaging showing the calibre of the aorta, segmental artery take-off, and concomitant atherosclerotic disease, when available, was useful in determining choice of catheter configuration. Segmental levels down to the lower thoracic levels were catheterized with 100 cm long catheters. The limiting factors for devices are the currently available lengths for catheters needed for lumbar and sacral segments as well as for taller individuals. An exchange length wire is handy for quick change-out of catheters. Angiography was successfully performed in all our patients.

Sagittal T1-weighted MR imaging through the thoracic spine in a patient with known renal cell carcinoma demonstrates marrow replacement of the T3 vertebral body and posterior elements with epidural tumor component dorsal to the spinal cord (white arrowheads) (A). 5 French Mani shaped catheter with tip positioned within the left supreme intercostal artery with microcatheter injection demonstrating vascular tumor blush (B). Roadmap fluoroscopy at completion of embolization demonstrating Liquid embolic cast within the tumor bed and left sided segmental artery (C).
After the procedure, hemostasis was obtained using a distal radial hemostatic band (Merit Medical Systems, South Jordan, UT) and a patent hemostasis technique. Ultrasound was immediately employed to evaluate the proximal radial artery after band placement.
Results
Seven patients had vascular tumors of the spinal column and underwent successful tumor embolization followed by segmental artery occlusion prior to surgical resection. One patient had a spinal dural AV fistula supplied from the right T10 segmental artery. In this patient, an attempt was made to perform superselective catheterization for embolization. However, this could not be performed due to severe tortuosity of the feeding artery, and lack of support from the guiding catheter. After a discussion with the surgical team, the patient subsequently underwent laminectomy for surgical disconnection of the fistula.
Two of the patients had right-sided dTRA access and the remainder of patients had left-sided dTRA access. Individual details are provided in Table 1 with selected illustrative cases described below. Although a targeted approach was taken, we were able to catheterize multiple segmental vessels per case (Range 3–8), mostly to evaluate for the presence of anterior and posterior spinal artery contributions and tumor vascularity from adjacent segments.
Details of targeted spinal angiography cases performed using radial access.
Abbreviations: dTRA: Distal Transradial Access; BHW2: Bentson-Hanafee-Wilson 2; RCC: Renal Cell Carcinoma; dAVF: dural Arteriovenous Fistula.
There were no access site hemorrhagic complications. One patient experienced transient mild numbness in the region of the thumb and dorsal hand during the period that the hemostatic compression device was applied. These sensory symptoms resolved completely within 24 h of the procedure. There were no instances of radial artery occlusion by palpation at 24 h.
Illustrative cases
Case 1
An atypical hemangioma involving the T10 vertebral body was diagnosed on MRI. There was a sizeable epidural component resulting in progressive cord compression and early myelopathic symptoms (Case 1 Table 1). The surgical procedure proposed was a T7 to L2 posterior instrumented fusion and en-bloc T10-T11 vertebrectomy with an interbody cage prosthesis supplemented with local and allograft bone. A distal right radial artery access was obtained (Figure 1A) and a 5 Fr Glidesheath slender introduced. There was an eccentric component towards the left on MRI (Figure 1B) and the left T10 segmental artery was targeted for our first injection (Figure 1C). Due to the relatively horizontal origin of the segmental arteries at this level, a Bentson-Hanafee-Wilson 2 catheter was used for the angiography, including adjacent segmental levels above and below the lesion. A DMSO compatible microcatheter was advanced into the T10 and T11 segmental arteries bilaterally. Tumor embolization and segmental artery occlusion at each of these levels was performed using Onyx 18 liquid embolic agent. Post embolization runs demonstrated satisfactory devascularization of the lesion, with only minimal residual supply from the left T9 (Figure 1D,E).
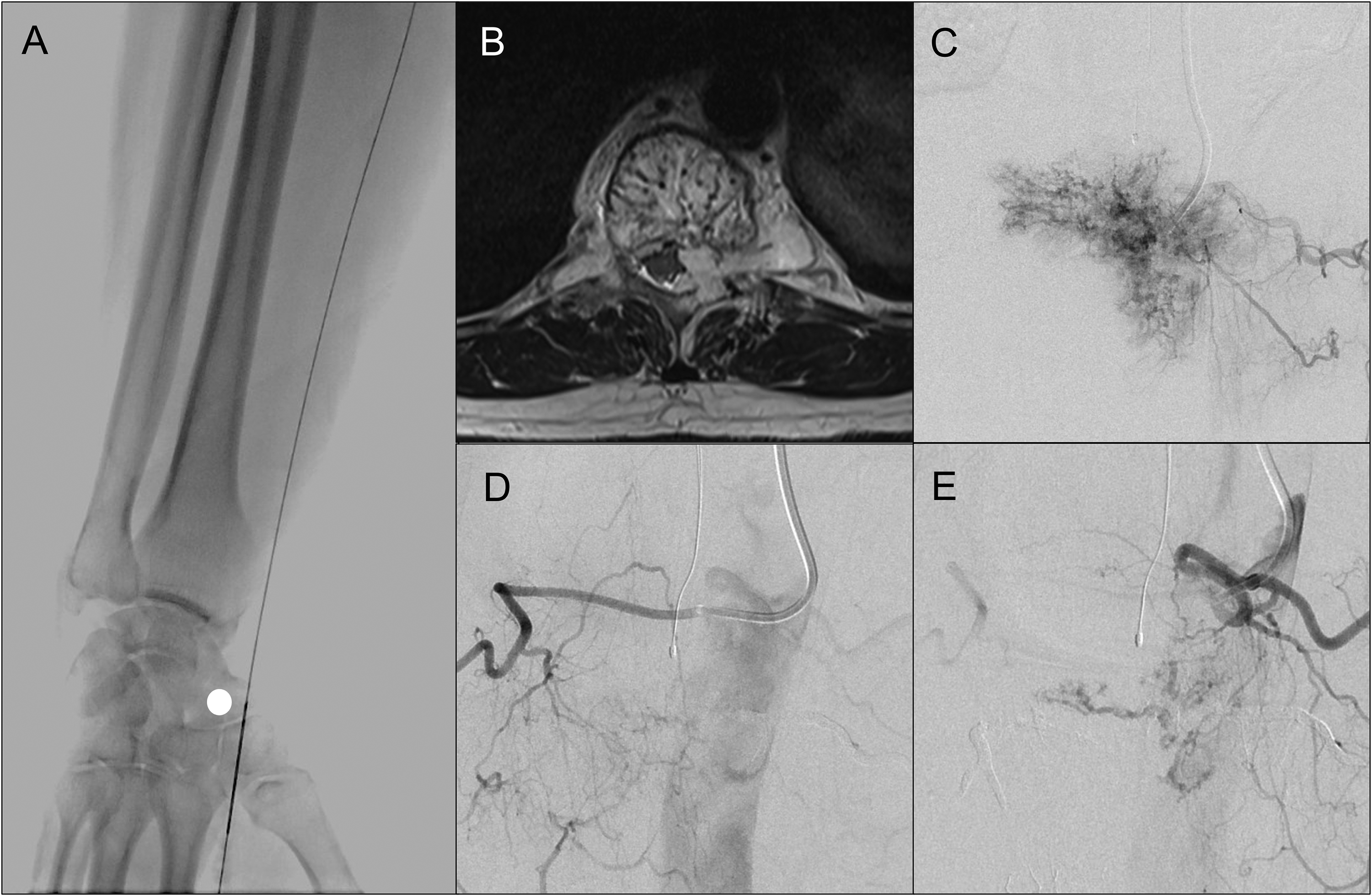
Fluoroscopic image demonstrating puncture site of the right distal radial artery against the scaphoid (white circle) (A). Axial T2-weighted MR Imaging demonstrates a hemangioma of the T10 vertebral level with an epidural component resulting in cord compression (B). Left T10 injection through a Bentson-Hanafee-Wilson 2 catheter shows significant vascular blush associated with the lesion (C). Post embolization runs from bilateral T9 segmental arteries showed near complete devascularization of the lesion with very minimal adjacent level supply from the left (D, E).
Case 2
A patient presented with myelopathic symptoms from metastatic renal cell carcinoma to the T3 level (Case 4 Table 1) identified on MRI (Figure 2 A). There was an extra-osseous soft tissue component dorsal to the cord and eccentric to the left. A T3 en-bloc vertebrectomy was planned for resection with pre-operative embolization. For the embolization procedure, a right distal transradial access was obtained. The right side was chosen in this case to utilize the inner curvature of the aortic arch for support during embolization. Multiple catheter shapes were attempted, with an eventual stable position obtained using a Mani shaped catheter (Figure 2B). A DMSO compatible microcatheter was advanced closer to the tumor, with tumor vascularity identified from the left supreme intercostal artery (Figure 2B). The lesion was embolized using Onyx 18 liquid embolic agent. The injectate was seen to penetrate the tumor vascular bed and was extended to include the segmental artery (Fig2C). The patient underwent successful tumor resection with posterior instrumented fusion.
Case 3
A spinal dural AVF was diagnosed on MRI, with a typical clinical presentation of slowly progressive paraparesis (Case 6 Table 1). A screening MRI of the thoracic and lumbar spine revealed multiple enlarged vascular flow voids within the thoracic spinal canal (Figure 3A). A dedicated MR angiogram demonstrated spinal arterial supply to the fistula from the right T10 segmental artery. A plan was made to perform selective angiography and embolization of the lesion. A left distal trans-radial access was obtained, and a 6 Fr Glidesheath (Terumo) was inserted. Selective spinal angiography (Figure 3B) and 3-dimensional rotational cone-beam CT imaging (Fig 3C) from the right T10 segmental artery confirmed the presence of the spinal dural AV fistula and the angioarchitecture. Regional exploration of the segmental arterial vasculature did not demonstrate adjacent level origin of anterior or posterior spinal artery contributors. Multiple attempts were made to selectively catheterize the feeding artery. There was an acute take-off of the radicular artery from the dorsal spinal artery noted (Fig 3C). This combined with an inability to engage the small sized segmental artery with the guiding catheter precluded satisfactory microcatheter positioning for safe embolization. After discussion with the surgical team, laminectomy and surgical disconnection was undertaken for definitive cure.
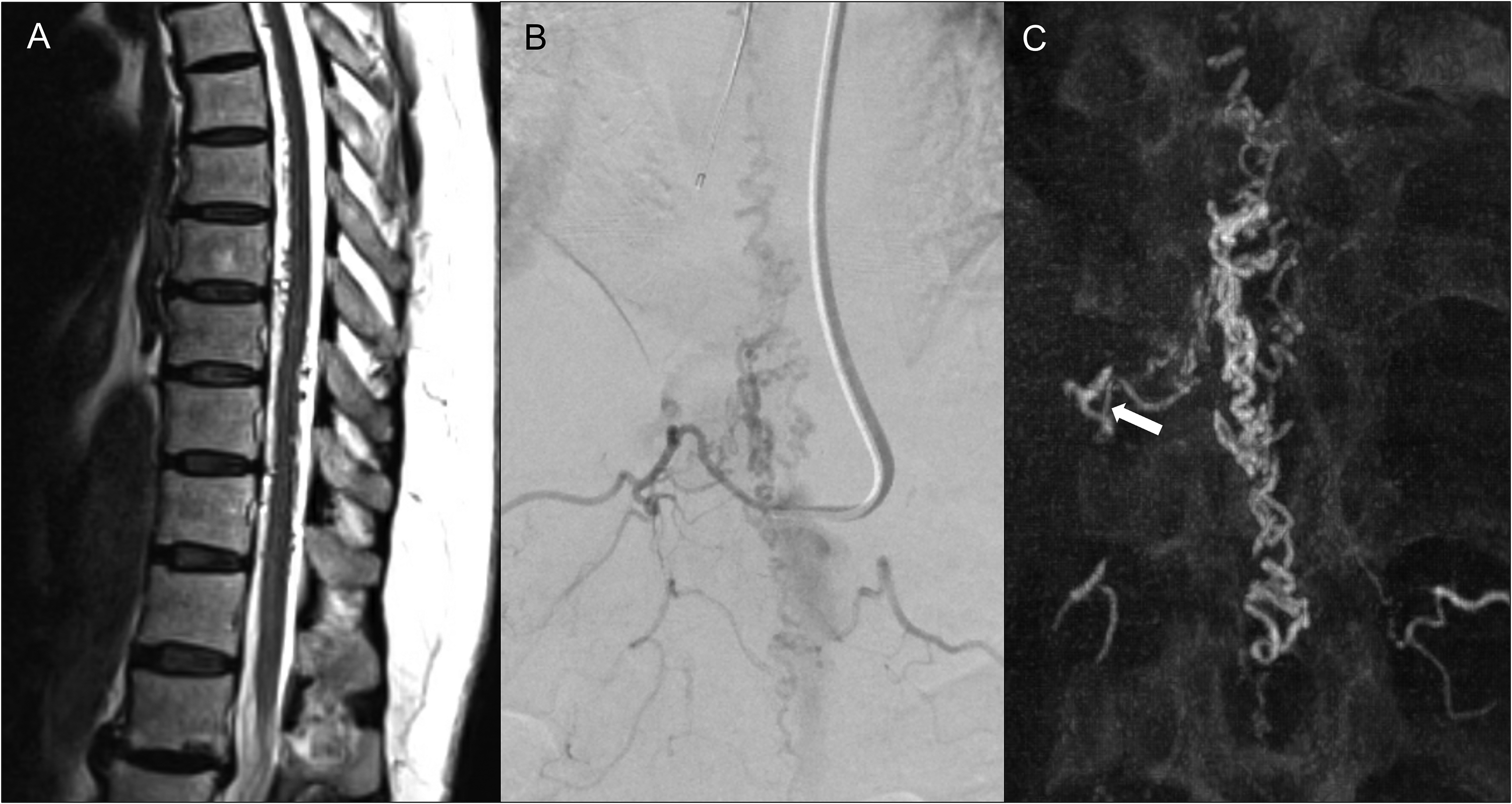
Sagittal T2-weighted MRI of the thoracic spine demonstrating multiple enlarged flow voids within the thoracic spinal canal in relation to the spinal cord (A). Frontal projection of DSA showing the Bentson-Hanafee-Wilson 2 catheter within the right T10 segmental artery with demonstration of the site of AV shunt within the right T10 nerve root sleeve (B). Note the small caliber of the segmental artery with respect to the catheter contributing to lack of stability. Coronal reconstructed images from the intra-procedural Cone-beam CT acquisition demonstrate an acute take off and tortuous cranial looping of the feeding radicular artery (arrow).
Discussion
Spinal angiography can be a cumbersome procedure especially in the setting of localizing spinal vascular lesions where the feeding segmental artery has not been identified by pre-procedural non-invasive imaging. It can be time consuming, and in certain situations the procedure may be aborted when contrast load limits have been reached. Advancements in cross sectional imaging have made the identification of feeding vessels to spinal vascular lesions easier. Moreover, targeted spinal angiography and embolization prior to surgical resection of neoplastic lesions have been shown to limit intraoperative blood loss. At our centre, the pre-operative endovascular approach to vascular spinal tumors includes a combination of tumor embolization when feasible and selective spinal segmental artery embolization to increase operative confidence for extensive spinal surgical procedures such as en bloc vertebrectomies. Segmental artery embolization is also critical for the extra-periosteal approach in these difficult operations where arterial injury or avulsion can occur intra-operatively.
Traditional access for spinal angiography is typically obtained through the femoral arterial route usually with a 5 or 6 French short sheath and a suitably shaped catheter is used for segmental artery catheterization. Trans-radial access for cardiology procedures is now mainstream and included in guidelines for coronary angiography and interventions. 5 There is also increasing adoption of a distal radial approach for both angiography and interventions, for a hypothetical increase in overall safety profile. 8 This is currently under investigation in ongoing clinical trials.
Numerous recent reports have shown the benefit of trans-radial access for neurointerventional procedures for supra-aortic lesions.3,4 Many body and peripheral interventionalists are also switching to trans-radial access. 9 With appropriate precautions, many of the risks such as cerebral ischemic complications and radial artery spasm have been mitigated along with refinement of technique. There is more recent published literature on the use of the distal radial artery for Neuroangiography and interventions for a wide variety of cases.10–12
The use of radial access for spinal angiography has not been widely reported. There is possibly a significant advantage in spinal angiography patients where post-procedural lower extremity neurological evaluation is not limited by strict immobility protocols. Also, many patients with spine pathology find it uncomfortable to lay flat for long periods after the procedure, due to the restrictions required when accessing the femoral artery for embolization. With a radial approach, patients are not restricted from sitting upright and may be positioned appropriately for post anaesthetic care in the recovery unit. The added benefits of using a left sided approach are the use of the non-dominant hand, as most individuals are right hand dominant, and a more straight-forward access to the descending aorta. There is also a lower theoretical risk of cerebral thromboembolism from left sided access as the catheters do not traverse the aortic arch.
Kühn et al. in their large series of distal radial cases, describe one patient who underwent spinal angiography and pre-operative embolization. 10 In their case, they used a right radial approach for pre-operative embolization of a T8 lesion through the left T8 segmental artery (personal communication). Orru et al. described a radial approach in the treatment of a sacral dural AVF. 13 Their patient had a symptomatic sacral dural AVF fed by the lateral sacral artery. Spinal diagnostic angiography from a femoral approach was made difficult due to an aorto-bi-iliac endograft. Endovascular embolization was successful in treating the fistula through a transradial approach. Caton et al. have recently described a series where embolization was performed for a T3 metastatic lesion and an L4 aneurysmal bone cyst. 14 These reports also highlight the feasibility of segmental arterial catheterization and embolization along the entire spinal neuraxis.
Radial access for intra-operative angiograms in the prone or three-quarter prone position for patients undergoing surgical treatment for spinal vascular lesions have been previously published (3 patients in the series by Lang et al. and 4 patients by Haynes et al.).15,16 The use of the distal radial access site for the pre-operative spinal angiogram and embolization helps preserve the vessel more proximally for standard radial artery monitoring during the surgical procedure and if this access is considered for intra-operative angiography.
There are certain limitations to a radial approach for spinal angiography. Although in our series targeted angiography was feasible, diagnostic spinal angiography of the entire neuraxis might be challenging given the limitations of current catheter configurations. Another limiting factor, as mentioned previously, is the length of currently available catheters that preclude treatment of lower lumbar and sacral levels. In our series, one patient experienced sensory changes in the hand during the period of patent hemostasis with a dedicated compression device. This was transient and symptoms were completely resolved at 24 h. We hypothesize that this likely resulted from concomitant pressure to the superficial branch of the radial nerve within the anatomical snuffbox, compounded by local anesthetic infiltration. There is also a risk of higher procedural and fluoroscopy times with a non-conventional approach, however in our series mean fluoroscopy times compared favorably with control patients undergoing similar procedures through femoral arterial access (31.4 min vs. 35.9 min).
Conclusion
Our case series highlights the feasibility of transradial access for spinal angiography, supplementing the existing literature on the topic published previously.13–16 The procedure is especially useful for targeted angiography and embolization prior to major surgical resections for vascular spinal tumors. There was a very low rate of minor complications with no incidences of major access site bleeding events, critical hand ischemia or permanent neurological deficits. Although routine use of transradial access may not be practical in all patients requiring spinal angiography, this technique may be considered in selected situations where femoral access is challenging, as an alternative when considering angiographic evaluation and targeted therapy of the spinal neuraxis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.