
Abstract
Introduction
Mechanical thrombectomy (MT) with combined treatment including both a stent retriever and distal aspiration catheter may improve recanalization rates in patients with acute ischemic stroke (AIS) due to large vessel occlusion (LVO). Here, we evaluated the effectiveness and safety of the REACT aspiration catheter used with a stent retriever.
Methods
This prospective study included consecutive adult patients who underwent MT with a combined technique using REACT 68 and/or 71 between June 2020 and July 2021. The primary endpoints were final and first pass mTICI 2b-3 and mTICI 2c-3 recanalization. Analysis was performed after first pass and after each attempt. Secondary safety outcomes included procedural complications, symptomatic intracranial hemorrhage (sICH) at 24 h, in-hospital mortality, and 90-day functional independence (modified Rankin Scale [mRS] 0–2).
Results
A total of 102 patients were included (median age 78; IQR: 73–87; 50.0% female). At baseline, median NIHSS score was 19 (IQR: 11–21), and ASPECTS was 9 (IQR: 8–10). Final mTICI 2b-3 recanalization was achieved in 91 (89.2%) patients and mTICI 2c-3 was achieved in 66 (64.7%). At first pass, mTICI 2b-3 was achieved in 55 (53.9%) patients, and mTICI 2c-3 in 37 (36.3%). The rate of procedural complications was 3.9% (4/102), sICH was 6.8% (7/102), in-hospital mortality was 12.7% (13/102), and 90-day functional independence was 35.6% (36/102).
Conclusion
A combined MT technique using a stent retriever and REACT catheter resulted in a high rate of successful recanalization and first pass recanalization in a sample of consecutive patients with AIS due to LVO in clinical use.
Introduction
Endovascular treatment has been established as the standard of care for acute ischemic stroke (AIS) due to large vessel occlusion (LVO) based on the results of pivotal trials.1–4 However, most of the thrombectomies in these trials were performed using stent retriever (SR) devices, and technical debate about the safest and most effective approach to achieve mechanical recanalization remains frequent.5–7
The degree of recanalization is commonly evaluated using the modified treatment in cerebral ischemia (mTICI) score, 8 with successful recanalization defined as higher than 50% reperfusion of the target vessel (mTICI 2b-3). In a pooled meta-analysis of major trials, successful recanalization was achieved in 71% of patients. Nevertheless, the ultimate objective of mechanical thrombectomy (MT) is achievement of complete recanalization with a single attempt (first-pass effect [FPE]) 9 which was been reported to have occurred at a rate of 25–40% in a larger series of consecutive patients.
The combined MT technique utilizes both a SR and a distal aspiration catheter (DAC). This technique relies on synergy between the direct retrieval capability of the SR and the aspiration force and probable local flow arrest of the DAC. 10 As both SRs and DACs have technologically evolved over recent years, this combined technique has become one of the most frequently used.4,7,11
In vitro studies have shown that REACT 68 and REACT 71 aspiration catheters (Medtronic, Minneapolis, MN, USA) present two of the highest aspiration forces and largest effective inner diameters among DACs. 12 In addition, these catheters have been shown to be safe and effective devices for use in direct aspiration or the combined technique. 13 We aim to explore the clinical and procedural outcomes among consecutive patients treated with the combined MT technique using REACT catheters in daily practice.
Methods
The data supporting the findings of this study are available from the corresponding author upon reasonable request
Study design and population
Between June 2020 and July 2021, patients who received treatment using the combined MT technique with REACT catheters in our center were recorded. All patients aged 18 years or older with AIS due to an anterior or vertebrobasilar LVO who fulfilled MT criteria according to current guidelines and clinical practice were included. Patients were consecutively included regardless of National Institute of Health Stroke Scale (NIHSS) score, Alberta Stroke Program Early CT Score (ASPECTS), or time from onset to treatment. Procedures were performed by one of five different interventionalists possessing at least two years of experience. The use of standard-dose thrombolysis was at the treating physician's discretion, following current guidelines.
Clinical and radiological variables
Upon admission, all patients underwent clinical assessment, including demographic information and medical history, physical exam, NIHSS scoring, and modified Rankin Scale (mRS) scoring by stroke neurologists. NIHSS scoring was also performed after 24 h and again at 5 days or before discharge. Relevant workflow times (symptoms onset, hospital admission, imaging acquisition, intravenous tissue plasminogen activator bolus, arterial puncture, and recanalization) were also recorded by stroke neurologists. Functional outcome at 90 days was evaluated using an mRS score obtained through a structured telephone-based interview performed by certified neurologists, with functional independence defined as a mRS score ≤ 2.
Diagnostic neuroimaging (CT or MRI) was performed on admission and after 24 h. Radiologic variables such as ASPECTS, the presence and location of LVO (assessed by CT angiography or digital subtraction angiography), and intracranial hemorrhage detection at 24-h follow-up were assessed by local neuroradiologists. Local interventionalists assessed all neuroimaging and determined the extent of recanalization according to the modified treatment in cerebral ischemia (mTICI) scale, as well as incidences of first-pass complete recanalization (mTICI 2c-3; i.e. FPE) and sudden recanalization (progression from mTICI 0–1 to 2b-3 in a single pass). 14 The rates of successful recanalization (mTICI 2b-3) were measured after each pass and at the end of the procedure. All angiograms were reviewed by a senior interventional neuroradiologist with more than 10 years of experience.
The primary outcomes of interest were the rates of successful recanalization (mTICI 2b-3) and FPE. Secondary outcomes were procedural time, neurological status at 24 h and 5 days, rate of sudden recanalization, and mRS score at 90 days. Secondary outcomes related to safety included the incidence of any serious adverse event (SAE) including symptomatic intracranial hemorrhage (sICH), neurological worsening defined as an increase of ≥ 4 points in NIHSS score (performed at 24 h, and 5 days or discharge), procedural complications (e.g. arterial perforation, dissection, vasospasm in target vessel, distal emboli), and in-hospital mortality.
We also performed a sub-analysis on only those patients who fulfilled class I-A indication for MT based on current guidelines. 15 Class I-A designation is assigned to patients receiving treatment within 16 h of symptom onset or time last known well with MCA M1 segment or ICA occlusion, mRS 0–1, ASPECTS ≥ 6, and NIHSS score ≥ 6.
Procedural technique
All procedures were performed under local anesthesia and conscious sedation. Through a percutaneous transfemoral or transradial approach, a long 6F sheath was placed in the ICA or vertebral artery. The triaxial system was completed with the introduction of a REACT catheter (REACT 71 or 68 was selected at the discretion of the interventionalist) and a 0.021-inch microcatheter with a 0.014-inch microwire. The microcatheter was then advanced through the occlusion site, and the SR (selected by the interventionalist) was deployed.
Once the SR was deployed, and the system was anchored, the REACT catheter was advanced to the clot position under distal aspiration with a manual or pump aspiration system initiated at the moment of catheter-clot contact. In most cases, the SR and the REACT catheter were completely removed from both guide catheter and long sheath under continuous aspiration (SAVE technique). 10 However, the Solumbra technique (removing the SR without removing the aspiration catheter if it is not occluded) was preferred by one of the interventionalist and when distal access was laborious.
Statistical analysis
Descriptive and frequency statistical analyses were performed using SPSS V.23.0 software. Shapiro-Wilk test was used to ensure normality of continuous variables. Categorical variables are presented as absolute values and percentages, and continuous variables are given as medians (interquartile range [IQR]) or means (±standard deviation [SD]) as indicated.
Results
During the inclusion period, 102 patients underwent MT with the combined technique using REACT catheters. The mean patient age was 78 (IQR: 73–87) years, 50.0% (51/102) patients were female. The median premorbid mRS score was 1 (IQR: 1–2), with 15.7% (16/102) having an mRS ≥ 3. At admission, the median NIHSS score was 19 (IQR: 11–21), the median time from stroke onset/last time seen well to hospital admission was 230 (IQR: 122–570) minutes and the median baseline ASPECTS was 9 (IQR: 8–10). Demographic and baselines characteristics are presented in Table 1.
Demographics and clinical data.
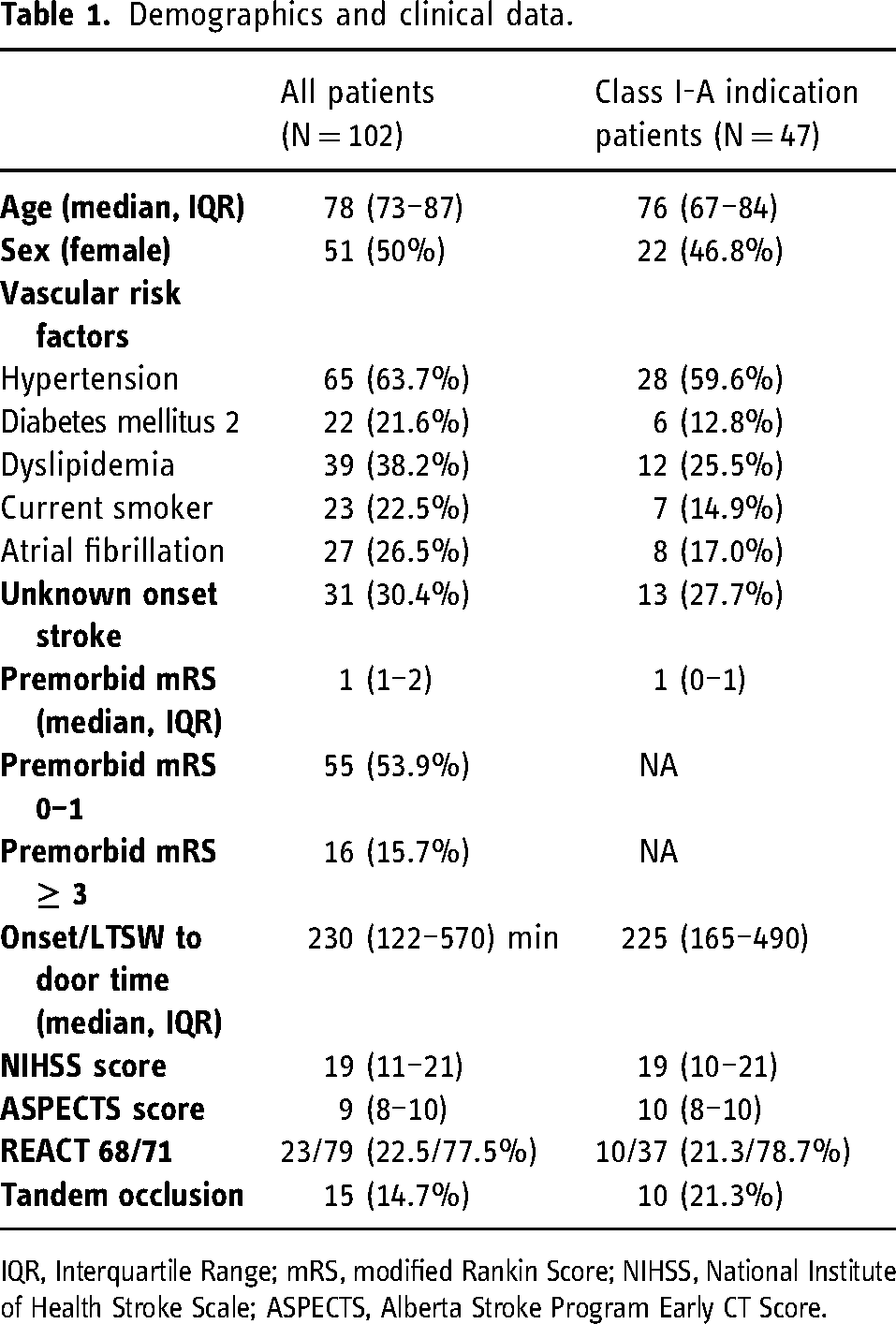
IQR, Interquartile Range; mRS, modified Rankin Score; NIHSS, National Institute of Health Stroke Scale; ASPECTS, Alberta Stroke Program Early CT Score.
Procedural data and outcomes.
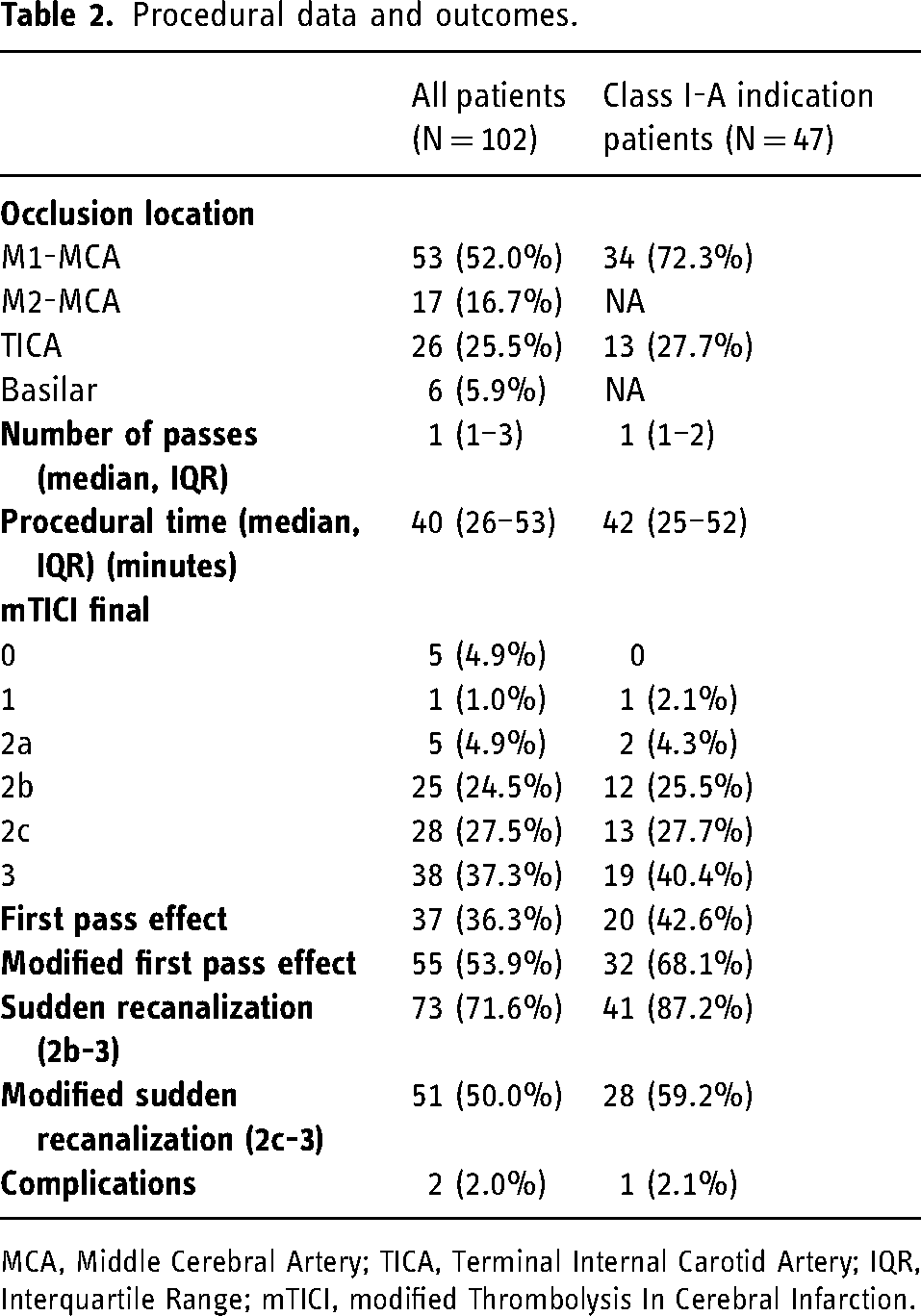
MCA, Middle Cerebral Artery; TICA, Terminal Internal Carotid Artery; IQR, Interquartile Range; mTICI, modified Thrombolysis In Cerebral Infarction.
The site of occlusion was the internal carotid artery (ICA) in 25.5% (26/102) of patients, the M1 segment of the middle cerebral artery (MCA) in 52.0% (53/102) of patients, the M2 segment of the MCA in 16.7% (17/102) of patients, and the basilar artery in 5.9% (6/102) of patients. Tandem occlusion, defined as the presence of extracranial ICA occlusion or high-grade stenosis combined with intracranial LVO, was present in 14.7% (15/102) of patients. Of the included patients, 47 fulfilled class I-A indication based on current guidelines. REACT 71 was used in 77.5% (79/102) of patients and REACT 68 in the remaining 22.5% (23/102).
Different stent retrievers were used, including Solitaire-X® in 72 (70.6%) patients, Catchview® in 19 (18.6%), Aperio® in 4 (3.9%), Neva® in 3 (3.0%), Trevo® in 2 (2.0%), pRESET® in 1 (1.0%) and Embotrap® in 1 (1.0%).
Study outcomes (Table 2)
Median procedural time from arterial puncture to recanalization was 40 (IQR 26–53) minutes, and the median number of passes was 2 (IQR 1–3). With the anchoring effect of the stent retriever and the support of guide catheters, REACT could be tracked into the desired position in all patients in our series.
Successful recanalization (mTICI 2b-3) was achieved in 89.2% (91/102) of patients with a rate of complete recanalization (mTICI 2c-3) of 64.7% (66/102). Successful recanalization was achieved in a single attempt in 55 (53.9%) patients and complete recanalization in 36.3% (37/102). The rate of sudden recanalization was 71.6% (73/102); in 50.0% (51/102) of patients, mTICI scores progressed from 0–1 to 2c-3 in a single pass.
Procedural complications occurred in 3.9% (4/102) of patients. All four patients showed extravasation of contrast due to arterial perforation related to microcatheterization; two were asymptomatic and two had a worsening of the 24 h NIHSS score ≥4. The rate of sICH was 6.8% (7/102), and 13 (12.7%) patients died during hospital admission. No patients experienced dissection or symptomatic vasospasm related to the REACT catheter. The rate of functional independence (mRS 0–2) at 90 days was 35.6% (Figure 1).
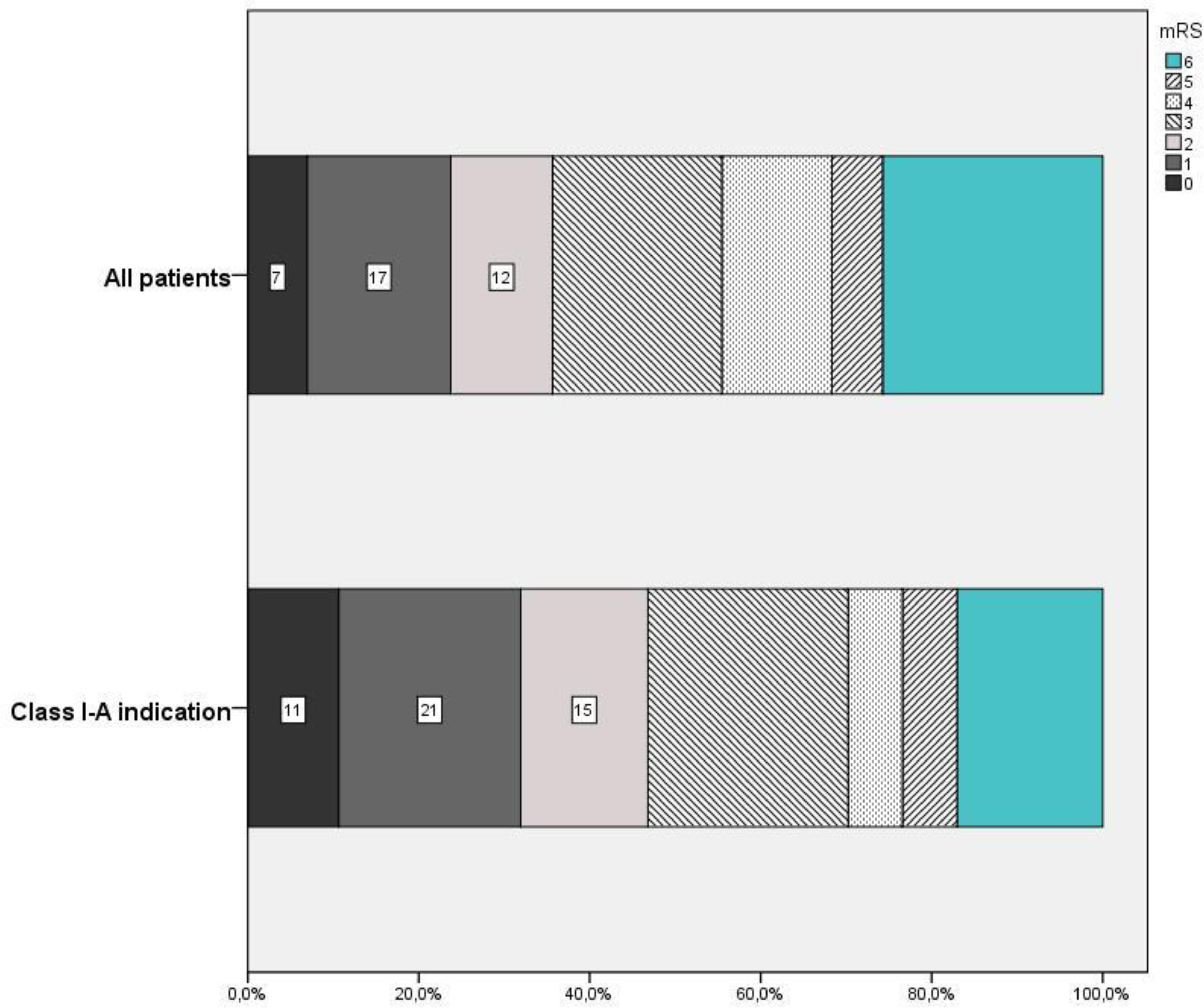
Functional outcome of all patients and those who fulfilled class I-A mechanical thrombectomy indication of current guidelines.
Analysis of class I-A patients
Of the total patient sample, 46.1% (47/102) fulfilled the criteria for class I-A indication for MT. Among patients with premorbid mRS score 0–1 and occlusion of the MCA-M1 segment or ICA, the rate of successful recanalization was 93.6% (44/47), and complete recanalization was achieved in 68.1% (32/47) of patients. The median number of attempts was 1 (IQR 1–2) in these patients. The first pass successful recanalization rate was 68.1% (32/47), with complete recanalization occurring in 42.6% (20/47). The rate of sudden recanalization was 87.2% (41/47) and the rate of mTICI progression from 0–1 to 2c-3 in a single pass was 59.2% (28/47).
The procedural complication rate (2.1% [1/47]) and median procedural time (42 min, IQR 25–52) were similar to the whole sample. The incidence of sICH in these patients was 4.3% (2/47), and 4 (8.5%) patients died during hospital admission. The rate of functional independence (mRS 0–2) at 90 days was 46.8% (Figure 1).
Discussion
In this study, the combined MT technique with SR and REACT aspiration catheter demonstrates high rates of successful recanalization in a consecutive sample of patients with AIS due to LVO. The rates of successful (mTICI 2b-3) and complete (mTICI 2c-3) recanalization, FPE, and sudden recanalization in our patients, along with the low incidence of complications, suggest the safe and effective use of REACT catheters in the combined MT technique. A sub-analysis of patients meeting class I-A MT criteria demonstrates particularly positive outcomes in this subgroup, with high rates of recanalization and a decreased incidence of complications compared to the entire cohort studied.
Although the benefit of successful recanalization has been consistently shown even in patients with established large infarct lessions, 16 the ultimate objective of endovascular treatment is to achieve complete recanalization while avoiding clot fragmentation and vessel wall damage that may be introduced with multiple attempts. 17 Distal embolization 18 and clot fragmentation may contribute to incomplete recanalization during MT. In addition, clot characteristics related to composition,19,20 time from onset to treatment initiation, 21 and mechanical behavior (stiffness or stickiness) may affect the success of each attempt. The primary strategy of the combined method is to incorporate both thrombectomy approaches (aspiration and clot trapping) in an effort to increase the success rate of the first pass. REACT catheters have been shown to have a high suction force and sufficient tip distensibility to trap the clot, 12 making them ideal for use in this dual technique. Indeed, the combined technique showed a high rate of FPE (36.3%) and sudden recanalization (71.6%) in our patient sample. Furthermore, compared with previously published series, the rate of successful and complete recanalization after the first pass were similar or higher.3,22
While larger DAC diameter has been associated with better recanalization results,13,23 other characteristics such as suction force 24 and catheter tip distensibility 12 may influence aspiration efficacy and final recanalization results. Navigation of the REACT catheter over the SR wire may reduce the impact effect of the catheter against the vessel wall and thus reduce the risk of dissection. Using an SR as an anchor improves the navigability 10 of REACT catheters allowing face-to-face clot contact 25 and avoiding sudden progression of the catheter which can occur near the ostia of the ophthalmic and choroid arteries, minimizing a potential source of dissection.
The benefit of larger DAC diameter and its balance with navigability continues to be explored in prospective studies focused on new larger-diameter catheters such as Zoom 88 26 or ANA. 27 In the same way, the effect of new delivery or navigability systems such as Tenzing 28 or MIVIQ 29 will be evaluated in prospective studies. Moreover, the use of balloon guide catheters has been shown to improve the rate of FPE11,30,31 and reduce distal emboli. 31 The inner diameters of balloon guide catheters are usually incompatible with larger bore DACs. 32 However, the use of superbore aspiration catheters has been shown to achieve better revascularization outcomes and reduced rates of distal emboli compared with 6Fr devices when paired with a balloon guide catheter. 33 Prospective randomized clinical trials are necessary to determine which technique is superior in achieving complete recanalization with the fewest attempts and complications.
Our study included an older patient sample (median age 78 [IQR 73–87] years) with a higher range of premorbid disability (mRS ≥ 3, 15.7%) than most technical registries or trials. The rate of functional independence at 90 days was lower than previously reported in MT studies, likely due to our sample's previously described demographic characteristics. However, this rate was similar to pivotal thrombectomy trials2–4 when selecting for class I-A patients with premorbid mRS scores of 0–1 who underwent MT due to MCA M1 segment or terminal ICA occlusion. The rate of procedural success was also higher in class I-A patients, who were similar to the majority of patients included in previous trials and other series.34,35 Use of the combined technique in this group of patients showed a clear improvement in terms of the rate of successful (mTICI 2b-3, 93.6%) and complete (mTICI 2c-3, 68.1%) recanalization compared with previously published series. Additionally, the FPE (42.6%) and sudden recanalization rates (87.2%) support the potential of this approach to improve clinical outcomes.
Our study has some limitations. First, local interventionalists reported procedural outcomes without an independent core lab, which introduces a potential bias; however, our results are similar to a previously published study of the same technique evaluated by an independent core lab. 10 Also, previously published data has been used for comparison due to the single-arm design of our study.
Conclusion
The combined MT technique using a stent retriever and REACT aspiration catheter has shown a high rate of successful recanalization and FPE in a sample of consecutive patients in a real-world setting. The recanalization rates, low number of attempts, and fast procedure time support the use of the combined technique.
Footnotes
Acknowledgements
The authors acknowledge Medtronic, Inc. for editorial assistance.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MRi has modest ownership and serves on the advisory board of Methinks Software; he has a consulting agreement with Medtronic, Stryker, Johnson and Johnson, Perflow Medical, Anaconda Biomed, Apta Targets, Ceronovus, Philips, Sanofi, and Rapid AI. AT has received personal fees from Anaconda Biomed, Balt, Medtronic, Perflow, and Stryker.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author's note
Alejandro Tomasello is affiliated at Grup de Neurorradiologia, Vall d'Hebron Institut de Recerca, Barcelona, Spain.