
Abstract
Introduction
Management of intracranial artery dissection (IAD) remains elusive in medical practice. Intracranially, vertebral artery dissection (VAD) is more commonly encountered than internal carotid artery dissection (ICAD). Deconstructive (EVT-d) and reconstructive (EVT-r) endovascular techniques have been utilized to treat VAD and ICAD. This meta-analysis investigates the safety and efficacy of EVT-r and EVT-d in the management of VAD and ICAD.
Methods
The literature was searched for all studies with consecutive patient series evaluating EVT-d or EVT-r for VAD or ICAD management. Baseline characteristics and outcomes were compared between EVT-r and EVT-d groups using the random-effect model and meta-regression approaches.
Results
Overall, 1095 cases pooled from 56 studies were included. There was no statistically significant difference in baseline characteristics between VAD and ICAD. EVT-r was applied in 647 cases (59.1%) and EVT-d in the rest There was no statistical difference in the rate of procedural complications between EVT-r and EVT-d. Although EVT-d was significantly associated with higher rates of complete aneurysm occlusion (86.4%), lower rates of good clinical outcomes (72.1%) and higher mortality (15.1%) were achieved compared to EVT-r (70.2%, 83.3%, and 9.5%; respectively). The mortality rate was higher, and good clinical outcomes were less common in ruptured aneurysms. Ischemic presentation was statistically associated with poor outcomes (mRS 3-5) but low mortality. ICAD often tended to grow following treatment and resulted in poor neurological outcomes.
Conclusions
IAD has favorable outcomes when treated appropriately. Novel reconstructive endovascular techniques are promising and should be integrated well in endovascular practice. Further studies are warranted.
Keywords
Introduction
Intracranial artery dissection (IAD), especially symptomatic ones leading to subarachnoid hemorrhage (SAH), acute ischemic stroke, or compression, are associated with high morbidity and mortality rates when left untreated.1–3 IAD more commonly affects the posterior circulation and the vertebral arteries, much less frequently, the internal carotid artery and anterior circulation. 4 Endovascular treatments (EVT) have emerged as a successful option to manage symptomatic IAD. Various deconstructive endovascular (EVT-d) approaches, such as trapping or sacrifice of the parent vessel harboring ruptured dissecting aneurysms, have been heavily used to treat IAD in the past In the last twenty years, an accelerating evolution in selective endovascular techniques led to a replacement of most of the deconstructive techniques with reconstructive approaches like stenting, stent-assisted coiling, and flow diverters to preserve the parent artery, thus avoiding the harmful sequences of deconstructive techniques.
Many retrospective cohort studies evaluated the newly introduced techniques for IAD management.5–8 Nevertheless, most case series have a relatively small sample size, and adequately powered randomized double-blinded clinical trials are lacking. A large meta-analysis comparing the reconstructive endovascular technique (EVT-r) and EVT-d for management of 478 patients with vertebrobasilar artery dissection was published in 2015. 9 Considerable number of studies about EVT-r was published recently, which calls for an updated meta-analysis. Furthermore, investigation of the safety and efficacy of these techniques in both anterior and posterior circulation is beneficial. In this study, we investigate the safety and efficacy of EVT-r and EVT-d techniques in the management of intracranial vertebral (VAD) and internal carotid artery (ICAD) dissections.
Methods
Search strategy
The literature was searched on Pubmed, PMC, and Embase via API through the Nested Knowledge AutoLit software (AutoLit, Nested Knowledge, St Paul, MN) in December 2021 for reconstructive and deconstructive endovascular treatments of intracranial vertebral and internal carotid artery dissections. The search was performed in accordance with PRISMA guidelines. Search strategies were created using a combination of keywords, and standardized index terms included “Intracranial dissections,” “Occlusion,” “Stent,” “Parent artery sacrifice,” “Stroke,” “Subarachnoid hemorrhage” Rupture” (Appendix). Results were limited to the English language from inception until now.
Eligibility criteria
Inclusion criteria included: 1) Studies reporting a consecutive series of patients with anterior circulation (ICA) or posterior circulation (VA) dissections managed with either reconstructive (EVT-r; flow diverters, stenting, stent-assisted coiling, etc.) or deconstructive (EVT-d; parent artery sacrifice) endovascular techniques with clear reporting of the primary outcomes, 2) Series of at least five patients reporting the angiographic and clinical outcomes besides procedural complications. Exclusion criteria included: 1) Editorial or opinion article, 2) Review articles, 3) Case report or <5 patients, 4) in vitro or animal study, and 5) Secondary study of previously reported data.
Study selection process
One author screened the titles and abstracts for inclusion using Nested Knowledge's screening software. The same author retrieved full-text articles of the included abstracts and screened them, and the senior author approved all inclusion decisions.
Data extraction and outcome measures
Baseline characteristics of each study population were collected, including age, gender, lesion location, and clinical presentation (ischemic, hemorrhagic).
The included studies were subdivided into two groups. The first group comprised patients managed with EVT-r, and the second group included those who received EVT-d. To evaluate the efficacy and safety of both techniques, the clinical and angiographic outcomes and procedural complications of the treatment population for both techniques at the last follow-up were analyzed. The angiographic outcomes were represented by the intervention success rate, the complete occlusion, recurrence, and growth rates (for initially incompletely occluded or stented lesions) of treated dissecting aneurysms, and the patency rates of parent artery at last follow-up. Clinical outcomes were analyzed under three groups; good (mRS 0–2) and poor clinical outcomes (mRS 3–5) and mortality rates (mRS 6). Procedural complications were assessed as hemorrhagic and ischemic complications with attention to recurrent/de novo hemorrhage/ischemia.
Statistical analysis
The cumulative incidence (event rate per patient at the end of the study) for each study was estimated and 95% CI. We used a random-effects model to pool incidence rates across studies because of the marked heterogeneity expected in the populations and interventions across various studies. The I2 statistic was used to express the proportion of inconsistency not attributable to chance. Meta-analysis for all outcomes using Freeman-Tukey double arcsine transformation and meta-regression for outcomes of interest were performed using the MAJOR tool (METAFOR package) through JAMOVI statistical Software and OpenMeta[Analyst] open source Statistical Software.
Results
Search results & baseline characteristics
After title-abstract and full-text screenings (Figure 1: PRISMA flow diagram), 1095 patients from 56 studies2–8,10–58 underwent EVT for intracranial artery dissections were included in this analysis (Table 1). The publication timeline of included studies 1999 to 2021. Intracranial VAD was reported in 1000 (86.8%) patients, and the rest (13.2%) located in the internal carotid artery (ICAD) (Table 2). Both VAD and ICAD patients presented at similar mean ages (50 years) with slight male predominance in the VAD population (57.8%, ICAD: 50.5%). Overall, nine (28.2%) of 37 unruptured ICAD patients presented with ischemic symptoms and 71 (79.4%) with subarachnoid hemorrhage. The ischemic presentation was reported in 12.7% of patients with VAD, and 67% were admitted with SAH. EVT-d was applied in 483 (46.2%) VAD and 5 (5.3%) ICAD patients. The vast majority of dissecting lesions receiving EVT-d were ruptured (86.6%, p < 0.05) and located in vertebral arteries 438/443 (98.8%, p = 0.074). EVT-r procedures included stent-assisted coiling (SAC) in 293 (45.3%), stenting in 280 (43.3%), flow diverters in 61 (9.4%), and sole coiling in only 9 (1.4%) patients. In patients receiving stenting, single stent was used for 135 (48.2%) and overlapping or multiple stents in 145 (51.8%).
PRISMA flow diagram of the study selection process.
Details of included studies.
Baseline characteristics.
*T test for continuous and Chi square test was performed for categorical variables.
Reconstructive techniques
Six-hundred-forty-seven (59.1%) dissecting lesions received EVT-r; 49.8% were ruptured on initial presentation (Table 3). The intervention was successful in 92.6% of cases (586 out of 594). Procedural complications were experienced by 55 out of 607 patients [12.6% (95% CI (9.2%, 16.9%)] receiving EVT-r; 10.2% (95% CI 7.6%, 13.5%) had recurrent or de novo ischemic complaints and 7% (95% CI 5%, 9.7%) had recurrent or de novo bleeding. Delayed vasospasm was noted in 7 out of 90 patients [9.9% (95% CI 3.5%, 25%)]. Complete occlusion of EVT-r treated aneurysms was reported in 387 out of 596 aneurysms [70.9% (95% CI 61.2%, 79.1%)] at a 15.5-month-mean-follow-up. Twenty-three [9.3% (95% CI 6.4%, 13.2%)] aneurysms grew in size and 40 aneurysms [10.2% (95% CI (7.7%, 13.4%)] recurred on follow-up. Twenty-two (3.7%) out of 598 lesions demonstrated either partial or total occlusion of the parent artery. Good clinical outcomes were reported in 83.4% (95% CI 78.8, 87.2) patients and 91 out of 636 patients [14.7% (95% CI 10.3%, 20.5%)] had poor clinical outcomes. Overall mortality rate was 9.4% (95% CI 7.1%, 12.3%)].
Clinical and angiographic outcomes .
CI: confidence interval; n/t: number of events out of the total sample.
EVT-r was associated with worse angiographic outcomes; lower rates of complete aneurysm occlusion but higher rates of parent artery patency in comparison with EVT-d (p < .05). More favorable clinical outcomes and lower mortality rates were observed in the EVT-r population (p < .05). We did not observe any statistical difference by applied EVT-r technique except for higher rate of recurrent/de novo hemorrhage with flow diverters (P = 0.02). Distribution of EVT-r techniques utilized for IAD management over the last two decades are illustrated in Figure 2.
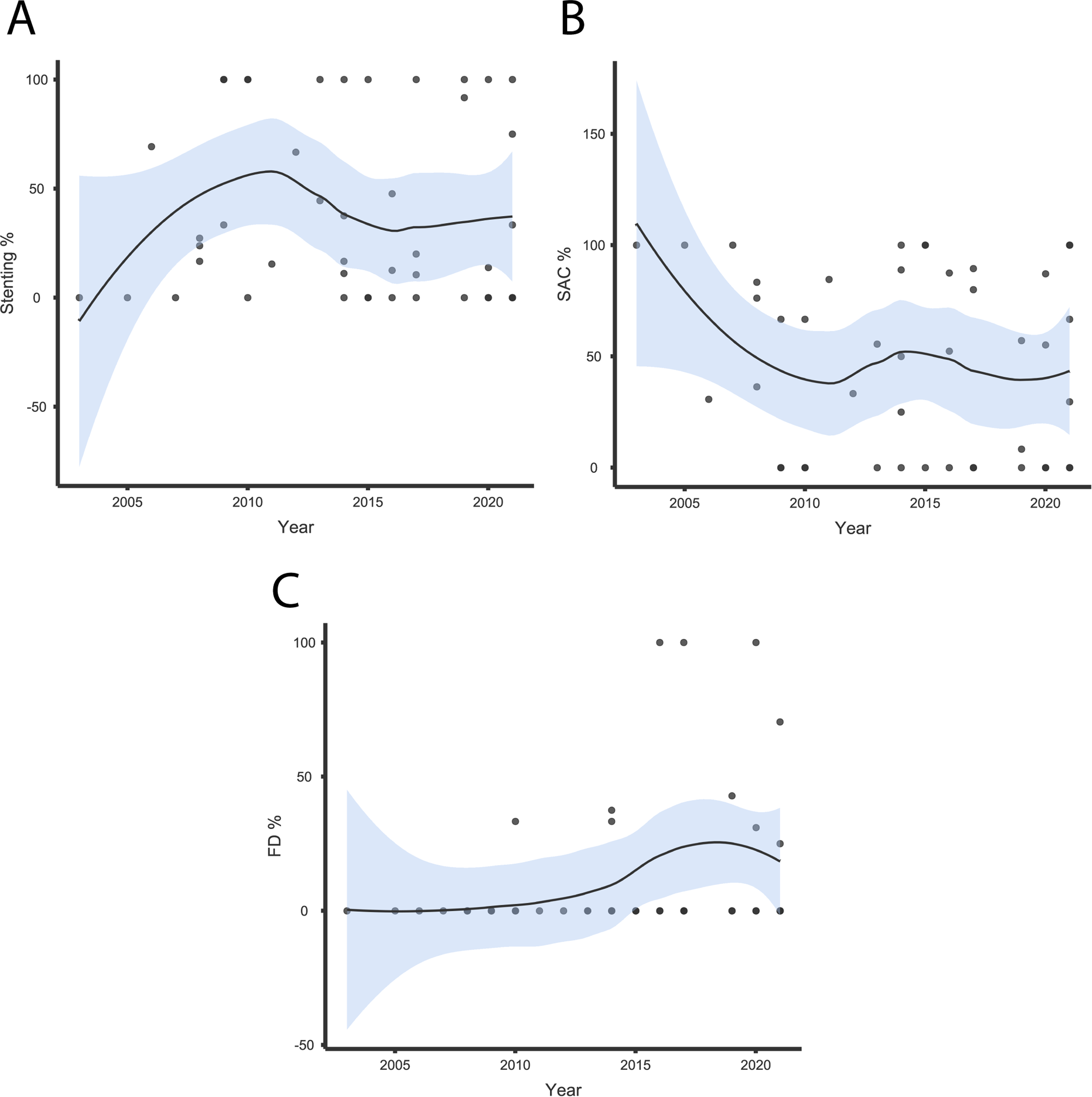
Scatterplots illustrate the distribution of EVT-r techniques;
Deconstructive techniques
Four-hundred-forty-eight (40.9%) dissecting lesions received EVT-d; 86.6% were ruptured on initial presentation. The intervention was successfully applied in 401 (93.6%) out of 411 patients. Procedural complications were experienced by 53 out of 367 patients [16.9% (95% CI (11.5%, 23.7%)] receiving EVT-d; 12.8% (95% CI 8.9%, 23.7%) had recurrent or de novo ischemic complaints and 9.4% (95% CI 5.8%, 14.8%) had recurrent or de novo bleeding. Delayed vasospasm was noted in 2 out of 95 patients [3.7% (95% CI 1.3%, 10.2%)]. Complete occlusion of EVT-d treated aneurysms was reported in 333 out of 370 aneurysms [87% (95% CI 82.7%, 90.3%)] at a 24.7-month-mean-follow-up. Two [5.9% (95% CI 2.7%, 12.6%)] aneurysms showed growth in size and 13 [7.6% (95% CI (4.9%, 11.6%)] recurred. Four (1.3%) out of 303 occluded parent arteries reopened to blood circulation. Good clinical outcomes were reported in 74.8% (95% CI 69.3, 79.6) patients and 47 out of 430 patients [14.4% (95% CI 11.1%, 18%)] had poor clinical outcomes. Overall mortality rate was 14.3% (95% CI 11.3%, 18.1%)].
Ruptured dissecting aneurysms showed worse clinical outcomes and higher mortality rates compared to unruptured aneurysms. However, they demonstrated higher complete occlusion rates regardless of the applied EVT technique (p < .05). Most patients with ischemic unruptured dissections had poor clinical outcomes on the follow-up but with lower mortality rates (p < .05). The ischemic presentation was also significantly correlated with higher aneurysm growth rates. ICAD tended to grow in size and led to overall poor clinical outcomes (p < .05). Meta-regression results are available in table 4.
Meta-regression results.
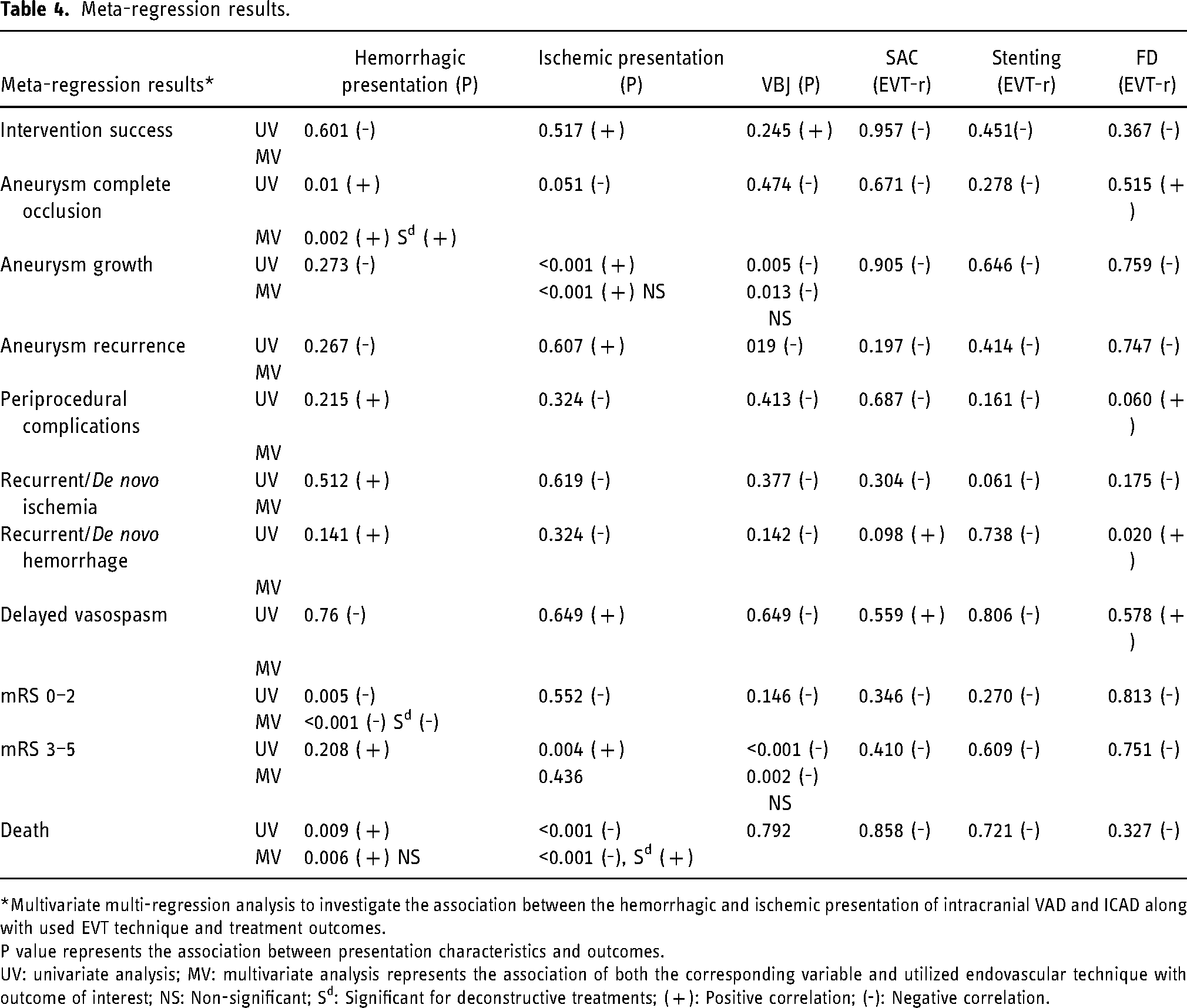
*Multivariate multi-regression analysis to investigate the association between the hemorrhagic and ischemic presentation of intracranial VAD and ICAD along with used EVT technique and treatment outcomes.
P value represents the association between presentation characteristics and outcomes.
UV: univariate analysis; MV: multivariate analysis represents the association of both the corresponding variable and utilized endovascular technique with outcome of interest; NS: Non-significant; Sd: Significant for deconstructive treatments; ( + ): Positive correlation; (-): Negative correlation.
Discussion
Our meta-analysis of close to 1100 patients with IAD analyzed the efficacy and safety of emerging reconstructive and traditional deconstructive endovascular techniques based on the most recent literature. We found that EVT-d has been utilized primarily for VAD while ICAD has been predominantly managed with EVT-r. In comparison with EVT-d, EVT-r was associated with better clinical outcomes but worse angiographic outcomes with no difference in periprocedural complications. Ruptured dissections were a major cause of unfavorable clinical outcomes and mortality. Patients with ischemic presentation experienced more disability and poorer clinical outcomes (mRS 3–5) but less mortality.
Conservative management of asymptomatic dissections is preferred. 1 Symptomatic IAD represents a clinical entity of significant challenge for treating clinicians due to its poor clinical outcomes and limited medical and interventional treatments. Previous studies reported surgical sacrifice of the dissected vessels. In selective cases, revascularization via bypass was performed to treat symptomatic IAD. 59 Endovascular treatments of IAD have been introduced in the last two decades, which have evolved from simple coiling or balloon occlusion for parent artery sacrifice to more selective and sophisticated reconstructive modalities including overlapping stenting, stent-assisted coiling, and flow diverters.3,5,11,13,17,20,43 IAD mostly affects the vertebral arteries and rarely the internal carotid arteries. Deconstructive treatments were utilized commonly for vertebrobasilar dissections with good angiographic outcomes, as reported in a previous meta-analysis. 9 Although the authors reported no statistical difference in clinical outcomes between both techniques, our updated study showed worse clinical outcomes and higher mortality rates with EVT-d. The vast majority of dissecting aneurysms managed with EVT-d were ruptured on presentation, potentially explaining more unfavorable clinical outcomes with this approach.
Similar to the previous study, we demonstrated better angiographic outcomes (dissecting aneurysm occlusion) with EVT-d. However, complete occlusion of the parent vessel does not necessarily correlate with better clinical outcomes or lower rebleeding rates. De novo/recurrent hemorrhage and stroke rates were low in EVT-d and EVT-r. Furthermore, aneurysm recurrence rates showed no significant discrepancy between both techniques. New endovascular techniques such as overlapping stents, stent-assisted coiling and flow diverters, have been introduced in the last 2 decades and often applied in IAD management. Such techniques have demonstrated excellent angiographic outcomes with preservation of blood flow within the dissected vessel, eliminating potential ischemic events. Hyun Suh et al. reported excellent clinical outcomes in 91% and complete occlusion in 90% of dissecting aneurysms receiving stent-assisted coil embolization. 43 Natarjan et al. published a series of 12 patients with VAD who underwent flow diverter embolization and demonstrated promising clinical outcomes in 91.7% and complete occlusion in all patients. 60 However, other studies reported modest clinical and angiographic outcomes following those techniques.5,47 We did not observe a noteworthy difference among these techniques in our meta-analysis. High-quality, uniform, and adequately powered studies with these novel EVT-r techniques are needed as 1) they have been very recently implemented in the treatment of IAD, 2) experience from various institutions are heterogeneous, and 3) published cohorts are small in size. These factors are significant limitations to generalizing these findings.
Anterior circulation dissections are rare and affect mainly the ICA. 61 Expectedly, the natural history of ICAD is significantly different from VAD; however, the different pathogenesis underlying ICAD and VAD is not quietly understood. 62 No statistically significant difference was found in baseline characteristics between ICAD and VAD in our study. However, in terms of management and outcomes, ICAD received primarily reconstructive treatments and often recurred/grew at follow-up. Patients with ICAD had overall poorer clinical outcomes than VAD, which had better clinical outcomes. Nevertheless, no difference in rates of procedural complications or mortality was observed. Despite the small sample size of ICAD limiting the validity of our findings, the existing data suggest that ICAD can be managed with EVT-r. Finally, EVT-d of ICAD can be detrimental and lead to major ischemic infarcts due to a much larger territory supplied by ICA (∼80% of the ipsilateral hemisphere), thus increasing mortality (malignant ischemic infarcts and herniation). Therefore, EVT-d should be only reserved for patients with ruptured ICAD and major SAH who tolerate balloon occlusion test Furthermore, integrating novel reconstructive techniques in endovascular neurosurgery training and practice is required.
Limitations
The main limitation of this meta-analysis is most studies included in our analysis are retrospective case series with a small sample size. Our meta-analysis suffers considerable heterogeneity due to the variety in evaluation and treatment protocols among institutions and dissection characteristics. We could not perform regression analyses for the clinical and angiographic outcomes based on baseline dissection characteristics (ruptured vs. unruptured, etc.) as most studies lacked this information at an individual level.
Conclusion
IAD is a unique entity affecting mostly the vertebral artery and rarely the internal carotid arteries. EVT-d has been utilized previously to obliterate VAD, while ICAD is managed mainly with reconstructive techniques. VAD typically has often good clinical outcomes after endovascular treatments. The most recent literature evidence, represented by our study, demonstrates the less favorable clinical outcomes of EVT-d. Our findings suggest that EVT-d should be reserved for selected cases, and novel EVT-r modalities should be more readily implemented and integrated into endovascular training and practice. Finally, an adequately powered, multi-center, randomized clinical trial with comparative analysis of deconstructive and reconstructive endovascular techniques for IAD management is warranted to validate our results.
Footnotes
Acknowledgements
The authors acknowledge Karl Holub, Stephen Mead, Jeffrey Johnson, and Darian Lehmann-Plantenberg for their design, development, and support of the Nested Knowledge meta-analytical software.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.