
Abstract
Wide neck intracranial aneurysms are often difficult to treat with coiling alone, and sophisticated techniques such as balloon-assisted coiling, stent-assisted coiling, flow-diversion, or intrasaccular flow-disruption are sometimes required.
This technical note reports the endovascular treatment of a recurrent middle cerebral bifurcation aneurysm by remodeling technique followed by flow-diverter (Silk Vista Baby) deployment through a remodeling balloon (double lumen balloon Eclipse 2L).
Keywords
Introduction
Since the first description of the remodeling technique (RT) known as balloon-assisted coiling (BAC) by Moret et al., new balloons have been developed to improve compliance – a mechanical property defined by the propensity of the balloon to change its cylindrical shape to the anatomy of the vessel in which it is inflated – and to change the number of lumen from one to two.1,2
The single lumen balloon catheter (SLBC) was the first type of remodeling balloon (RB) available for treating wide neck aneurysms (sidewall and bifurcation). SLBC has some disadvantages: 1) it can only be inflated if a microwire is in the lumen to block the hole that permits balloon preparation and balloon deflation; and 2) when the balloon is in a vessel, microwire removal can lead to blood reflux in the balloon that can potentially block the hole that permits balloon deflation, making deflation slow or impossible. These difficulties led to the development of the double lumen balloon catheter (DLBC).
Unlike the SLBC, the DLBC allows the clinician to navigate coils, stent, or potential flow-diverter (FD) through the balloon (whether inflated or not). Placement of coils in the aneurysm sac through DLBC has been reported as the deployment of stent (remo-stent technique).3–9
Limited information exists with regard to using DLBC to deliver FDs (remo-diversion technique) and all refer to sidewall aneurysm treatment.3,10
We report the treatment of a recurrent MCA bifurcation aneurysm combining BAC performed with a DLBC Eclipse 2L (Balt Extrusion, Montmorency, France) and a FD (Silk Vista Baby; Balt Extrusion, Montmorency, France) that was navigated and deployed through the balloon.
Technique
A man older than 60 years was treated for two intracranial aneurysms (IA). In 1982, he was treated for a ruptured left pericallosal aneurysm by clipping, and retreated by coiling in 2015 for aneurysm recanalization. In 2004, a ruptured right MCA aneurysm (undetected in 1982) was treated with coils. In January 2021, MRA followed by DSA showed MCA aneurysm recanalization. Aneurysm remnant was 5.5 mm in width, 8.4 mm in height, and 3.8 mm in neck (dome to neck ratio = 1.4) (Figure 1).
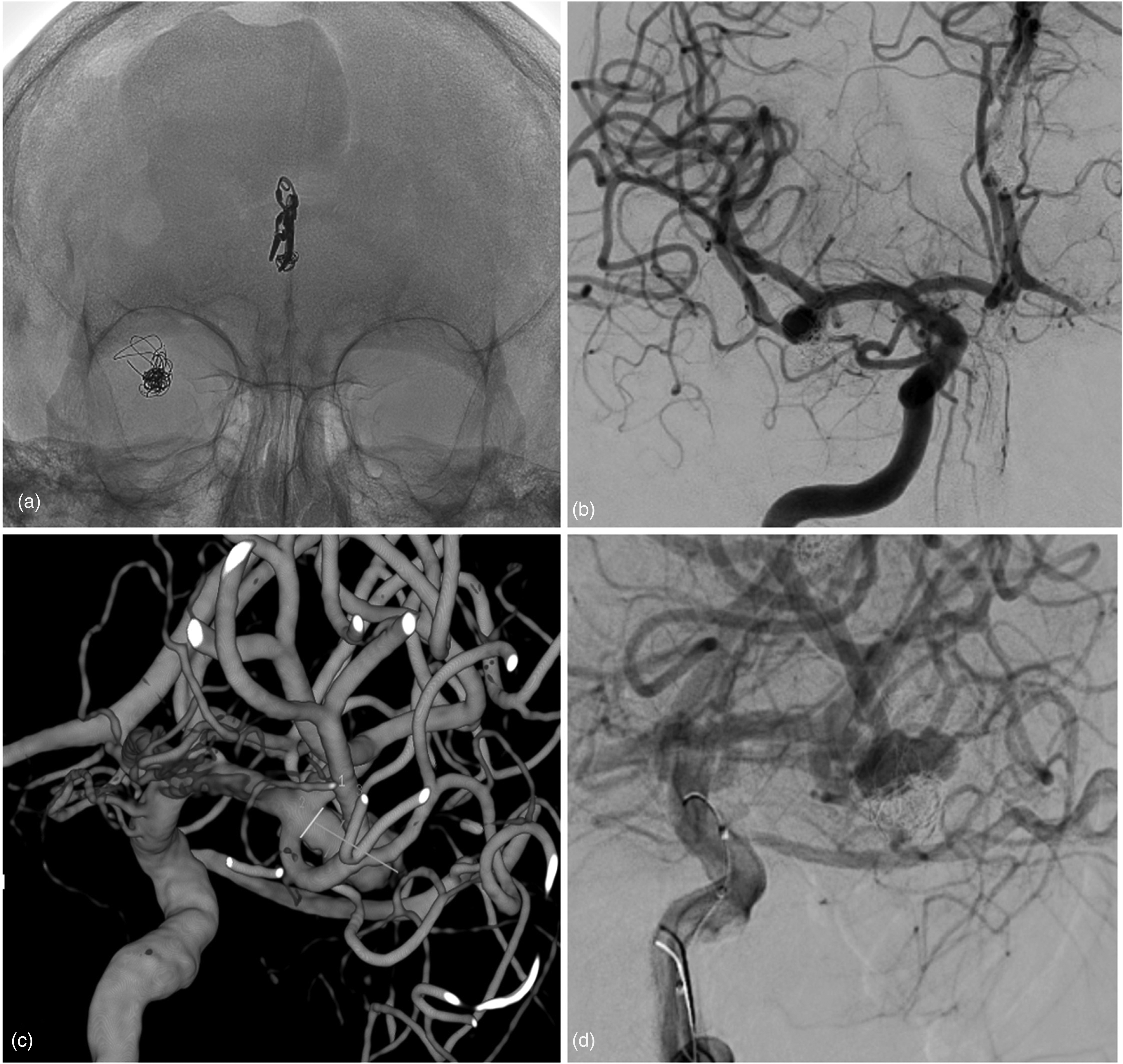
(a) Anteroposterior unsubstracted image showing the coils at projection of middle cerebral artery bifurcation and surgical clip at projection of left pericallosal artery. (b) Anteroposterior digital substaction angiography showing the middle cerebral artery aneurysm remnant. (c) 3D rotational angiography showing very irregular aneurysm (dome height: 8.4 mm; neck width: 3.1 mm; maximum dome width: 7.2 mm; dome-to-neck-ratio: 2.3). (d) Working projection.
The multidisciplinary (neurosurgeon and neuroradiologist) decision was to retreat the aneurysm by placing coils in the aneurysm sac using BAC then a FD in front of the neck.
Under dual antiplatelet therapy (250 mg Acetylsalicylic acid and 180 mg Ticagrelor) and heparin, an 8 F introducer was placed in the right femoral artery and a NeuronMax 088 (Penumbra Inc, Alameda, California, USA) was placed in the distal portion of the cervical ICA. A DAC 0.038” (Concentric Medical, Mountain View, California, USA) was placed at the ICA terminus.
As the aneurysm remnant had a wide neck, a DLBC, Eclipse 6 × 15 mm over a Transend 0.014” microwire (Stryker Neurovascular, Fremont, California, USA) was placed in the superior branch of the MCA.
Through an Echelon-10 microcatheter (eV3 Neurovascular, Irvine, California, USA), and under the cover of the Eclipse DLBC, 10 Optima coils (Balt, Irvine, California, USA) were delivered in the aneurysm sac. After coil placement, the Echelon-10 was removed.
A Silk Vista Baby 2.5 × 15 mm FD was deployed in front of the aneurysm neck between the M2 superior branch and the distal M1 segment to stabilize the coils’ mesh and prevent further recanalization. VasoCT confirmed the FD's patency and adequate expansion, and final DSA control showed a satisfactory aneurysm occlusion (Figure 2).
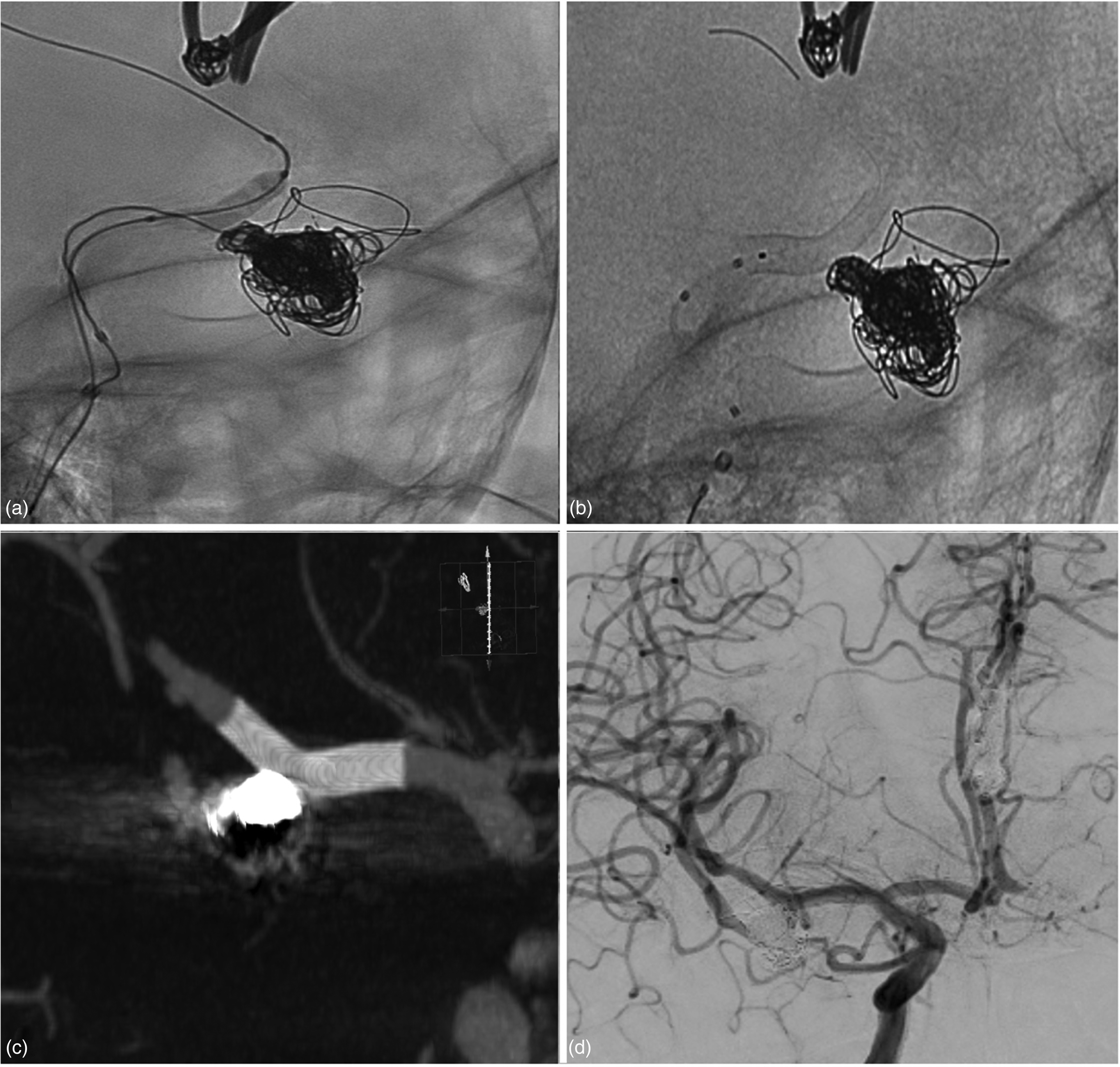
(a) Unsubtracted image shows the echelon 10 placed in the aneurysm sac; M2 superior branch were catheterized by the eclipse 2L 6 × 15 mm over a transend 0.014-inch microwire; the image demonstrates a moment in which the balloon was inflated in face of the neck of the aneurysm during the coiling of the aneurysm. (b) When the first part of treatment has terminated (coiling with remodeling technique) and the Transend and the Echelon 10 were removed, the flow-diverter Silk Vista Baby 2.5 × 15 mm was navigated and deployed through the Eclipse 2L. (c) vaso-CT shows the adequate expansion of flow-diverter. (d) Final digital subtraction angiography control.
No peri-procedural complications were observed and the patient did not experience any deficits; additionally, next day MRI imaging (including DWI) did not show any abnormalities.
The patient was discharged home on postoperative day 2 and placed on 180 mg of Ticagrelor for 3 months and 250 mg of Acetylsalicylic acid for at least 12 months.
Discussion
Treatment of IAs sometimes requires treatment which combines BAC and stent or FD placement. Deployment of an intracranial stent through a DLBC (remostent technique) has been evaluated in many reports. Several stent/balloon combinations have been reported in the literature including the LVIS junior stent (MicroVention, Aliso Viejo, California, USA) / Scepter balloon (MicroVention, Tustin, California, USA), LVIS junior / Ascent balloon (Codman Neurovascular, Miami Lakes, Florida, USA), and the LEO stent (Balt Extrusion) / Copernic 2L (Balt Extrusion). In the papers reporting these treatments, no complications were described and angiographic results were complete aneurysm occlusion or neck remnant.3–5
Galdamez et al. described deployment of 93 stents (63 LVIS junior, 15 LEO Baby [Balt Extrusion, Montmorency, France], 14 ACCLINO Flex [Acandis GmbH & Co. KG, Pforzheim, Germany] and 1 Neuroform Atlas [Stryker Neurovascular, Fremont, California, USA]) through Scepter C or XC and Eclipse 2L in 84 patients/86 aneurysms. 6 In this large series, stent deployment was always feasible. The total intraprocedural complication rate was reported for 10/86 aneurysm treatment (11.6%), including 3 in-stent thrombosis, 4 branch thrombosis, and 3 focal SAHs. Morbidity and mortality at 7 days were 2.4% and 1.2%, respectively. DSA follow-up (3–14 months; average 7 months) was available for 71/84 patients, and complete and near complete occlusion was 90.1% with residual aneurysms seen in 9.9%. 6
Deployment of a FD through DLBC (remo-diversion technique) has been reported in a very limited number of publications, all dedicated to sidewall aneurysms.3,10 Guenego et al. described 8 ICA aneurysms (5 paraophtalmic artery, 2 posterior communicating artery [pCom]), 1 anterior choroidal artery [AChA]) treated with the couple Copernic 2L / Silk. In this series, the remo-diversion technique was feasible for all treatments, and intra-stent angioplasty was performed in 5/8 procedures (62.5%). Three technical complications (37.5%) were reported (coil migration, aneurysm sac perforation, and intra-FD stent thrombosis) with no morbidity or mortality. At DSA follow-up (3–36 months; mean 8.2), the angiographical result was complete occlusion for all aneurysms. 3
To our knowledge, we describe the first case in which the remo-diversion technique was used to treat a bifurcation aneurysm. The aneurysm was potentially treatable with the jailing technique by placing a microcatheter in the aneurysm sac for coil deployment and a microcatheter in the distal M2 territory for FD deployment. However, this technique risks the coil microcatheter impeding FD deployment. According to the neck location in the middle of the bifurcation, and the fact that it was a retreatment with the risk of additional coils protruding in the bifurcation, we decided to first place some coils in the aneurysm using the remodeling technique followed by FD deployment. In current practice, this entails placing a microcatheter in the aneurysm sac for coil delivery and a balloon in front of the aneurysm neck to avoid coil protrusion. After coil placement, we withdrew the remodeling balloon and coil microcatheter and placed a microcatheter to deploy the FD. This technique required a number of microcatheter maneuvers which potentially risked losing access to the distal MCA territory as well as complications.
As the working lumen of the Eclipse 2L is 0.017-inch, we decided to use this balloon to protect coil deployment and to deploy the FD Silk Vista Baby, which is compatible with a 0.017-inch microcatheter. The Eclipse 2L is a new DBLC and its main design feature is a recently patented Flat Catheter Concept. The inflation tube and the working channel are placed side by side into the catheter, which gives it an oval shape without increasing the outer diameter. 7
This technique has three significant advantages: 1) the inflation channel is wider, increasing the inflation/deflation speed; 2) the wider inflation channel permits use of pure contrast for balloon inflation thus increasing balloon visibility and improving its safety profile; and 3) its oval shape offers greater flexibility and improves tortuous anatomy navigation. 7
Finally, in our experience, navigating the Silk Vista Baby through the Eclipse 2L was feasible, evaluated as satisfactory by the operator, and did not include deployment problems.
Conclusion
Deployment of the Silk Vista Baby FD through a double lumen balloon Eclipse 2L (remo-diversion technique) is a technically feasible and safe treatment for wide neck bifurcation IA. Additionally, the introduction of both low-profile FDs and low-profile double lumen balloons catheters may improve the ability to treat more distally located aneurysms with smaller parent vessels when RT alone is not sufficient to obtain satisfactory aneurysm occlusion.
The remo-diversion technique has three advantages: 1) it allows clinicians to combine RT and flow-diversion with limited manipulation – there is no need to replace the RB with a microcatheter to deploy the FD); 2) there is little or no risk of losing branch access where the FD will be deployed; and 3) at the end of FD deployment, the clinician can perform ballooning if required.
Footnotes
Ethical approvals
This Study involves human participants but an Ethics Committee(s) or Institutional Board(s) exempted this study.
Contributorship statement
All authors have:
Provided a substantial contribution to the conception and design of the studies and/or the acquisition and/or the analysis of the data and/or the interpretation of the data; Drafted the work or revised it for significant intellectual content; Approved the final version of the manuscript; and Agreed to be accountable for all aspects of the work, including its accuracy and integrity.
Data sharing
All data relevant to the study are included in the article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LP consults for Balt, MicroVention, Perflow, Phenox, and Vesalio.The other authors have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.