
Abstract
The advent of endovascular therapy for acute large vessel occlusion has revolutionized stroke treatment. Timely access to endovascular therapy, and the ability to restore intracranial flow in a safe, efficient, and efficacious manner has been critical to the success of the thrombectomy procedure. The stentriever has been a mainstay of endovascular stroke therapy, and current guidelines recommend the usage of stentrievers in the treatment of large vessel occlusion stroke. Despite the success of existing stentrievers, there continues to be significant development in the field, with newer stentrievers attempting to improve on each of the three key aspects of the thrombectomy procedure. Here, we elucidate the technical requirements that a stentriever must fulfill. We then review the basic variables of stent design, including the raw material and its form, fabrication method, geometric configuration, and further additions. Lastly, a selection of stentrievers from successive generations are reviewed using these engineering parameters, and clinical data is presented. Further avenues of stentriever development and testing are also presented.
Introduction
Stroke remains a major cause of global morbidity and mortality. The advent of endovascular therapy has revolutionized treatment and outcomes for acute stroke therapy. Multiple randomized trials have confirmed the beneficial impact of endovascular thrombectomy for large vessel occlusion strokes and made it the mainstay of treatment.1–5
Devices for endovascular thrombectomy have evolved significantly in the short time that mechanical thrombectomy has been provided for stroke treatment. Stentrievers (stent retrievers) have become the mainstay of the stroke therapy armamentarium of neurointerventionalists globally. Indeed, current guidelines for acute ischemic stroke with a large vessel occlusion recommend that thrombectomy with a stentriever be performed for all eligible patients, 6 although recent studies comparing stent retrieval to direct aspiration techniques have shown non-inferiority of these techniques.
Stentrievers are metallic constructs that can be delivered to the site of arterial occlusion and be used to remove the clot. Starting with the MERCI device, to now third generation stentrievers, these devices have grown more complex in design, and more successful in function.
This review considers the design and engineering aspects of stentrievers, as well as the available clinical evidence for various stentrievers.
Stentriever functional requirements and characterization
Function requirements
Neurological stentrievers are self-expanding stents that are deliverable via a microcatheter into the intracranial great vessels in the setting of an acute occlusion. The devices are designed to integrate the clots causing a large vessel occlusion (LVO) and remove these from the circulation, thus restoring intracranial flow.
Given these general principles of stentriever function, design of stentrievers must achieve the following functional requirements:
Be deployable and self-expanding with appropriate radial force, in order to achieve good vessel wall apposition. Ability to engage and integrate the clot material, given varying clot composition and density. Ability to be re-sheathed and removed while minimizing clot breakage and distal embolization of clot material.
7
High rates of first-pass recanalization (ability to remove clot and restore flow on the first deployment).
8
Minimization of endoluminal damage to the vessel wall during deployment and retrieval. Ability for multiple re-deployments in the target vessel or more distally in the case of incomplete or failed clot removal.
Stent characterization
Construction of stentrievers may leverage multiple variables in stent design to achieve optimal performance and fulfill the aforementioned design requirements. These variables have previously been used to assess available medical stents, including those for endovascular use. Stoeckel et al. have previously used five characteristics of stents to classify all available medical stents. These characteristics are material used, raw material form, fabrication method, geometrical configuration, and stent additions. 9
Material
Materials used for stents depend on whether the stent is self-expanding, or if it requires balloon-expansion. Self-expanding stents are ideal as stentrievers as they do not require the placement of a balloon, which may be less timely in acute stroke cases. Self-expanding stents also provide ease of navigability over balloon-expanding stents. These require low elastic modulus, and high yield stress, or, in the case of nitinol, high shape-memory properties. Nitinol is a nickel-titanium alloy that can recover elastic deformations of up to 10%. These allow for high elastic strain of these stents. Most stentrievers are nitinol-based self-expanding stents.
Raw material form
The stent raw material can be in several different forms. These include sheet, tubing, wire, and ribbon (flat wire) forms. 9 Sheet-based stents must then be rolled into a tubular configuration after the pattern has been formed. Variation in raw material form exists in the available stentrievers.
Fabrication method
Fabrication method refers to the mechanical process of forming the stent and depends primarily on the raw material form used. Wires can be formed into stents using coiling, braiding, or knitting techniques. Laser cutting is the most commonly used mechanism, and tubular metal is more commonly used for stents. Self-expanding stents can be cut in the small or expanded condition and must be deburred and surface-treated after. Another possible technique is water jet cutting, which has the benefit over laser cutting of not producing a heat affected zone along the cut surface. Most available stentrievers utilize the laser cutting fabrication method.
Geometrical configuration
Geometrical configuration of stents is of significant importance to the underlying functional requirements. There is a high degree of variation in the geometric configuration of stents, with advantages and disadvantages of each kind of design. Stoeckel et al. have divided stent geometry into 5 different categories: coil, helical spiral, woven, individual rings, and sequential rings configurations. 9
Coil designs are very flexible but have limited radial strength. They also have a low expansion ratio, which means that this geometrical configuration leads to higher-profile devices.
Helical spiral stents are similar to coil designs, and therefore share the high flexibility and low radial strength of coil stents. Longitudinal connections can be added to increase radial strength, at the expense of some of the flexibility.
Woven designs consist of one or more wire strands, which can be braided or knitted together. Some self-expanding stents utilize this geometric configuration. However, foreshortening is a significant concern for these types of stents.
Individual ring designs are Z-shaped rings that are typically used to support other grafts. They do not make good stand-alone vascular stents.
Sequential ring stents are comprised of a series of Z-shaped struts with connections called bridges or hinges. These connections can be regular, meaning that they occur at every inflection-point around the circumference, or periodic, meaning they occur at a pre-defined subset of these inflection-points. Peak-peak, peak-valley, or valley-valley connections exist 9
Sequential ring construction can be of a closed or open cell geometry. In closed cell designs, all internal inflection points of the structure are connected by bridging elements. Closed cell designs provide good scaffolding and a uniform surface, regardless of the degree of bending, but are less flexible than an open cell design. Open cell designs have some or all of the internal inflection points not connected to each other. The unconnected elements lead to a higher degree of structural flexibility, but comes at a cost of reduced radial strength. 9
Additions
Additional elements to the stent construction provide benefits in fluoroscopic visualization, such as radiopaque markers or coating, or in function, such as drug-eluting coating, biocompatibility coating, or hydrophilic coating. 9 Due to the poor fluoroscopic visibility of nitinol, which is the primary material for a vast majority of stentrievers, radiopaque additions are frequently utilized in the manufacture of these stents.
Brief review of existing stentrievers
This review aims to study the available (and historical) stentrievers, classify them according to the aforementioned system, and review the available evidence regarding their clinical applications. Select stentrievers from each generation are described below and summarized in Table 1.
A survey of current and historical stentrievers.
A survey of current and historical stentrievers.
MERCI retriever
The MERCI (Mechanical Embolus Removal in Cerebral Ischemia) Retriever (Concentric Medical, Mountain View, CA) was the first device approved for recanalization treatment in acute ischemic stroke, obtaining US FDA clearance in August 2004. The device was not a true stentriever and is commonly classified as a coil retriever. There are two versions of the device, the X and the L, of which the X is approved for mechanical embolectomy, while the L is only approved for foreign body removal. Both devices come in two sizes. The X device consists of a memory-shaped nitinol wire, with five helical loops of tapering diameter at the distal tip. The device sits in a straight configuration within the delivery catheter, but due to the nitinol construction, is able to conform to its memory shape once unsheathed within the target vessel. 10 The coil design suggests low radial strength of the device, which is the likely cause of low reperfusion rates.
The MERCI retriever underwent phase I and II prospective, nonrandomized studies, which enrolled 151 patients at 25 centers. An average of 2.9 retrieval attempts were performed per patient. These studies showed recanalization rates of 48%, which was improved to 58% if embolectomy was combined with intraarterial thrombolysis with tPA.11,12 Adverse events occurred in 7.1% of patients, and symptomatic intracranial hemorrhage in 7.8% of patients, of which 45% were due to vessel rupture.
Three randomized trials utilizing first-generation stroke devices were carried out between 2004 and 2012, with results published in 2013.13–15 Along with the MERCI retriever, these trials utilized the Penumbra aspiration system, which utilized an aspiration catheter with a separator wire, and a thrombus removal ring that could be deployed if aspiration alone failed.16,17 These trials were negative, showing no difference in functional outcomes between the patients treated with endovascular thrombectomy, or with intravenous tPA alone. Recanalization, as defined as TICI score 2b-3, was achieved in 67% of patients in the MR RESCUE trial, 15 while the IMS III study reported reperfusion rates between 65–81%, depending on the site of arterial occlusion. 13
The most significant reason for these trials being negative was felt to be that the first-generation embolectomy devices had low reperfusion rates. This meant that the angiographic outcomes between the intervention and control groups were not different enough to show clinical benefit. This point was also highlighted by improving clinical outcomes with an improved angiographic outcome in the MR RESCUE trial. 15 Furthermore, CT angiography was not uniformly available, and confirmation of a large vessel occlusion using vascular imaging was not an inclusion criterion uniformly.18,19 These trials laid bare the imperative of improved recanalization rates in the treatment of large vessel occlusions.
Other first-generation devices also reached various stages of development and testing but did not become as uniformly available as the MERCI device. These included the Phenox (Phenox, Germany), Catch (Balt, Montmorency, France), and Distal Access Catheter (Concentric Medical, Mountain View, CA). 19 The advent of stentrievers and their superior surgical performance, have largely shifted the market away from these devices.
Second-Generation devices: true stentrievers
Intracranial self-expanding stents were initially designed for use in aneurysm treatment, as an adjunct to coil embolization. Several authors initially reported off-label use of such stents, primarily for permanent deployment at the site of arterial occlusion.20–22 These early results showed encouraging high recanalization rates compared to first generation devices. The mechanism by which self-expanding stents caused recanalization is the entrapment and subsequent mechanical disruption of the clot by the expanding stent struts against the arterial wall. This is followed by chemical or endogenous thrombolysis, likely due to immediate anterograde blood flow obtained after stent deployment. 22
Kelly et al. reported the first case of temporary endovascular bypass using an Enterprise stent (Codman, Raynham, MA), which provided immediate flow restitution, without the need for permanent implantation of the stent itself. Another advantage of this technique was the ability to reposition the stent in case of re-thrombosis. 23
While this initial technique did not attempt embolectomy directly, the temporary stenting of the occluded vessel to reconstitute flow became the new paradigm in endovascular stroke treatment. Further use of this technique was reported also utilizing self-expanding stents designed for aneurysm treatment, including attempts at thrombectomy using the stent itself. 24 This led to the push for dedicated stent devices for thrombectomy procedures. The use of detachable stents for permanent implantation as a bailout procedure when other embolectomy techniques have failed is still a viable option. 25
Solitaire
The Solitaire FR (flow restoration) stentriever (Covidien/ Medtronic, Dublin, Ireland) was the first dedicated stentriever for endovascular thrombectomy. There was previously a Solitaire AB (aneurysm bridging) device, which had been utilized for temporary bypass and embolectomy. 24
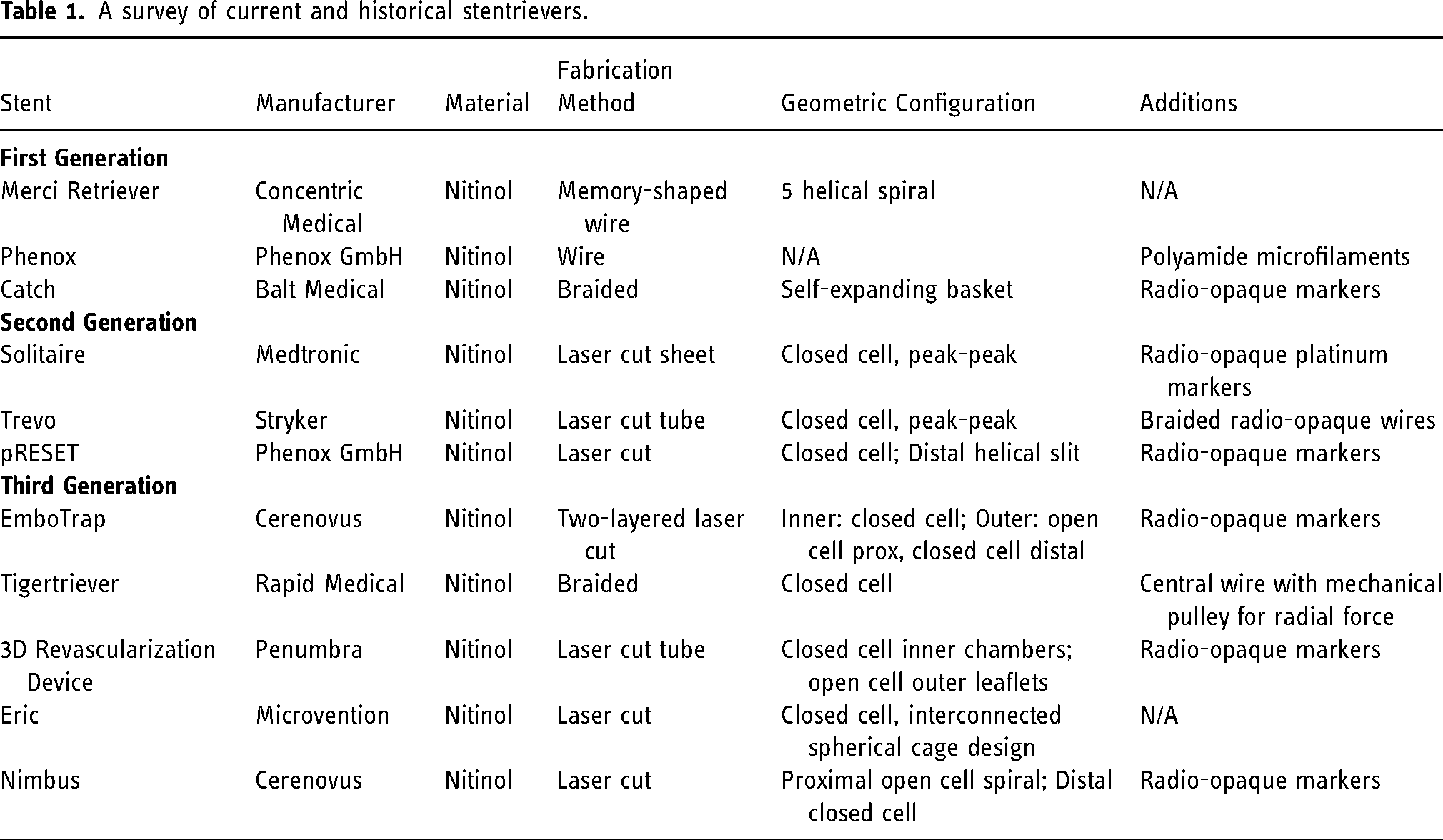
The current device is the fourth iteration Solitaire X. It is a nitinol stent, constructed from a sheet of nitinol which is laser-cut and shaped into an overlapping parametric design. The geometric configuration is that of a closed cell design, with peak-peak connections (Figure 1). The stents are available in 3, 4, and 6mm diameters, with 20mm length available in the 3mm diameter, 20 and 40mm lengths available in the 4mm diameter, and 20, 24, and 40mm lengths available in the 6mm stent. The stents have additional platinum markers at the proximal and distal ends, as well as evenly-spaced markers spaced 5–10mm apart along the stent, for visualization of stent opening and clot integration along the length of the stent. 26
A. Solitaire X device; B and C. Device overlap profile with varying vessel diameter for Solitaire X 6mm (B) and Solitaire X 4mm (C). 26 .
The parametric design leads to overlapping stent coverage leading to an increase in clot integration. Radial force applied by the stent also varies based on the vessel diameter. 26
Animal studies of the Solitaire FR device showed high degree of success in clot removal. TICI 3 flow was observed in 100% 27 and 86.7% 28 of cases, and immediate flow restoration was achieved in most cases.27,28
A single center experience with the device showed a 72.8% rate of first-pass reperfusion (TICI 2b/3), and overall successful reperfusion in 79% of anterior circulation cases. 29 Another study showed an 89% reperfusion rate using the Solitaire device. 30 Complication rates in these initial studies were low, with a 2% rate of intracerebral hemorrhage, and 4–6% rate of subarachnoid hemorrhage.29,30
Trevo
The Trevo device (Stryker, Kalamazoo, MI) is a nitinol stentriever laser-cut from a tubular nitinol sheet. The stent has a closed cell design, with peak-peak connections (Figure 2). Three platinum/tungsten wire is braided through the stent for improved fluoroscopic visualization. The device is then coated with a sodium hyaluronate hydrophilic mixture. This addition is meant to reduce friction during device deployment. The currently available version of the device, the Trevo XP ProVue Retriever, has three available sizes: 3 × 20mm, 4 × 20mm, 4 × 30mm, and 6 × 25mm. Broad portions of the device struts have an endoluminal orientation, which is designed to increase clot incorporation, as opposed to a vessel wall orientation in aneurysm bridging stents.31,32

In an animal study, the Trevo device showed successful revascularization in all cases, with first-pass recanalization in 15/16 cases. There was intimal disruption, but no evidence of damage to the media or adventitia. 31 Early human experience with the Trevo device showed similarly high levels of recanalization (TICI 2b/3) in 78.3% of patients. The rate of symptomatic ICH was 5%. 33
Evidence for thrombectomy using second-generation devices
Both Solitaire FR and Trevo underwent randomized trials comparing them to the MERCI retriever. These studies showed significantly better angiographic as well as clinical outcomes with Solitaire and the Trevo device, compared to the MERCI retriever.34–36 Collectively, these studies demonstrated a significant improvement in the state of embolectomy technology over first-generation retrievers. In the combined trial comparing either Solitaire FR or Trevo to the MERCI device, revascularization rates were 82% and 62%, respectively. Furthermore, ICH rates were 10% compared to 28%, demonstrating an improved safety profile over first-generation devices as well. 34
The second-generation stentrievers were involved in pivotal randomized trials of thrombectomy versus medical management for large vessel occlusion strokes. A total of five randomized controlled trials were performed: MR CLEAN, EXTEND-IA, ESCAPE, REVASCAT, and SWIFT-PRIME, showing significantly higher rates of good neurological outcome compared to medical management, with absolute increase in rates of good clinical outcome (modified Rankin score 0–2) ranging between 13.5–31.4%.1–5 One further study showed a 12.1% improvement in rates of good clinical outcome. 37 Stentrievers feature prominently in all these trials. Four of these six trials exclusively utilized stentrievers for the interventional arm,2,4,5,37 while the other two studies had 81.5% 1 and 86.1% 3 stentriever use in the interventional arm. Complete recanalization rates were 58.7% and 72.4% in these two trials respectively, as compared to 65.7–88.0% for the trials utilizing stentrievers exclusively.
The safety profile of stentrievers in these trials was well documented. Symptomatic ICH rates varied between 0–7.7% in the interventional groups, with no trials showing a difference compared to the non-surgical group.19,38
The DAWN trial utilized the Trevo stentriever for the interventional arm up to 24 h, and showed recanalization rates of 84% in treated patients. The trial also showed a 36% absolute difference in rates of good clinical outcome (mRS 0–2). The risk of symptomatic ICH was 6% in the interventional group. 39
While second-generation stentrievers have become the mainstay in acute stroke therapy, newer devices have been developed. These devices aim to build on the success of existing stentrievers, by improving the first-pass recanalization rates, reducing distal embolization of clot fragments, and improving the safety profile of the device by reducing complication rates. Complete revascularization (TICI 3) at the first attempt at thrombectomy is known as the first pass effect (FPE), and has been shown to be an important predictor of outcomes after mechanical thrombectomy utilizing second-generation devices.40–42 This provides the main rationale for continued development of the stentriever leveraging several facets of stent design. However, currently available data on the use of these devices does not show significant improvement in FPE or clinical outcomes over second-generation devices, and the stated goals of device development remain elusive.
Embotrap revascularization device
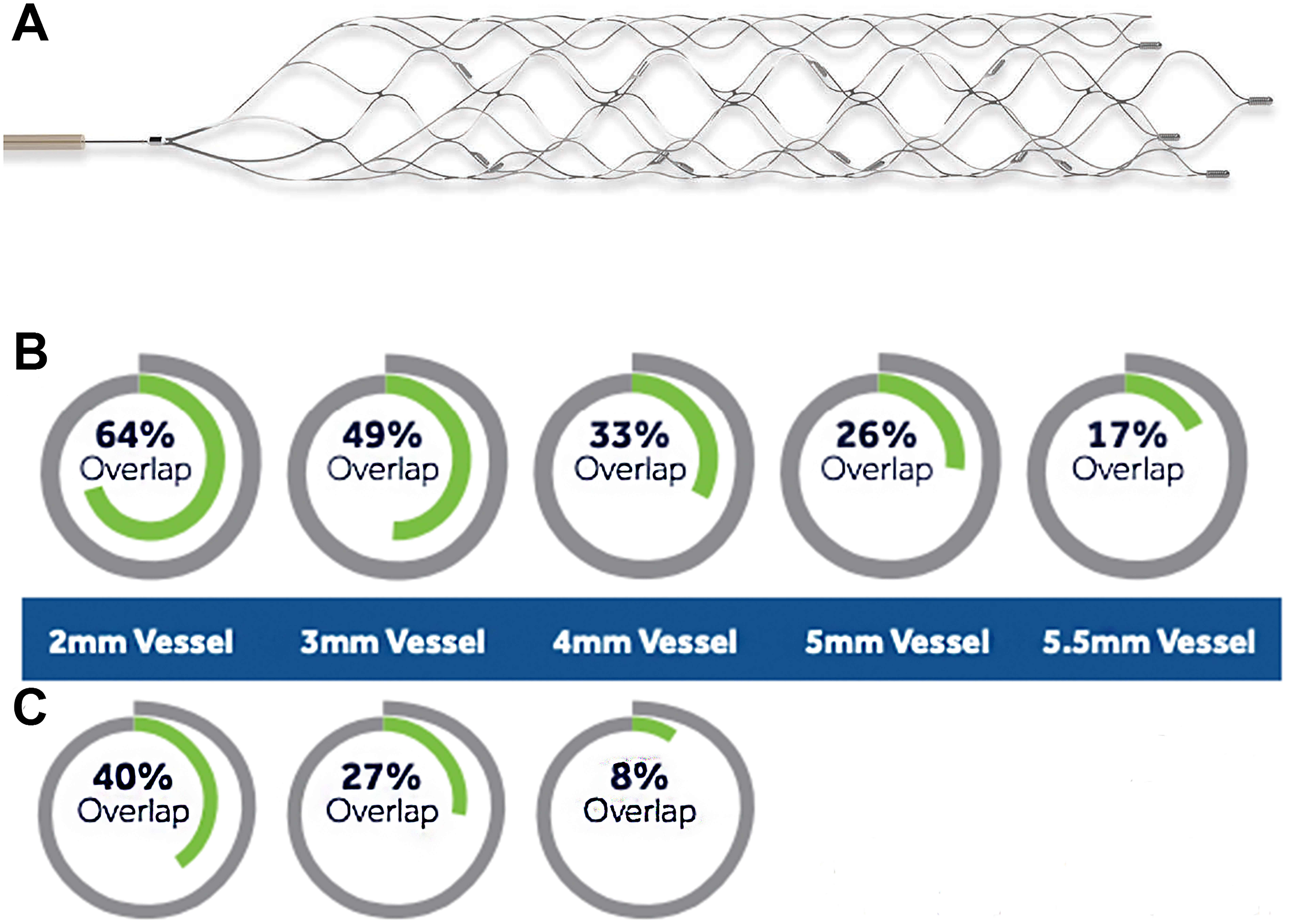
The EmboTrap Revascularization Device (Cerenovus, Irvine, CA) is a two-layered, laser-cut nitinol device, with an inner 1.25 mm closed cell stent with a high radial force that is surrounded by an outer 5/6.5 mm open cell structure with a lower radial force profile (Figure 3). The outer structure switches to a closed cell design at the tip, to act as a distal protection zone to catch clot fragments generated during mechanical thrombectomy. 43 Radiopaque markers are added proximally as well as distally for visualization. The newest version of the device, the EmboTrap III Revascularization Device, comes in three sizes: 5 × 22mm, 5 × 37mm, and 6.5 × 45mm. The large openings of the outer structure are designed to accept clot into the space between the two layers, while the high radial force inner stent creates a flow channel through the occlusion for instant recanalization. The outer leaflets are intended to maintain apposition with the vessel wall to retain the captured clot during device removal, and the closed design of the tip is designed to catch embolic fragments that have broken off from the clot.43,44 An in vitro study of the device focusing on quantifying distal emboli during model MCA mechanical thrombectomy showed that the EmboTrap produced significantly fewer emboli larger than 1mm than the Solitaire FR stentriever. Furthermore, there was a doubling in the number of emboli into the ACA territory in the Solitaire group, pointing to a protective effect of the EmboTrap during retrieval of the device in to the ICA. 43
The Embotrap III revascularization device in 5 × 22mm, 5 × 37mm, and 6.5 × 45mm sizes. .
In a series of 201 consecutive patients treated with the EmboTrap device, there was an 84.6% rate of successful recanalization (TICI 2b/3). This was superior to the RCT data that showed a 71.1% overall recanalization rate with stentrievers in the five large RCTs. The average number of passes with the EmboTrap device were 2.6. In 31 cases, another rescue device was required after the EmboTrap was unsuccessful. 45
Tigertriever
The Tigertriever (Rapid Medical, Yoqneam, Israel) is a third-generation stentriever. It is a braided, open cell device that has an additional central wire that attaches to the distal wire, which is connected to a slider mechanism in a handle. After deployment of the stent in the target vessel, the central wire can be pulled using the slider, which provides radial force and expands the stent braids to oppose the vessel wall. This action will potentially lead to improved clot integration and increase chances of first-pass recanalization. The standard version (Tigertriever) has a net length of 32 mm (unexpanded form) and can expand up to a diameter of 6mm. Two shorter versions are available, with net lengths of 23 and 20.5 mm. 46
Limited clinical data exists for the Tigertriever device. One study of 61 patients showed successful recanalization in 75.4% of patients, which first pass recanalization in 37.7%. The authors used a repeat inflation-deflation technique in a subset of these patients. This cohort showed successful recanalization in 82.6% of patients, with first pass recanalization in 47.8%. 46
3D Revascularization device
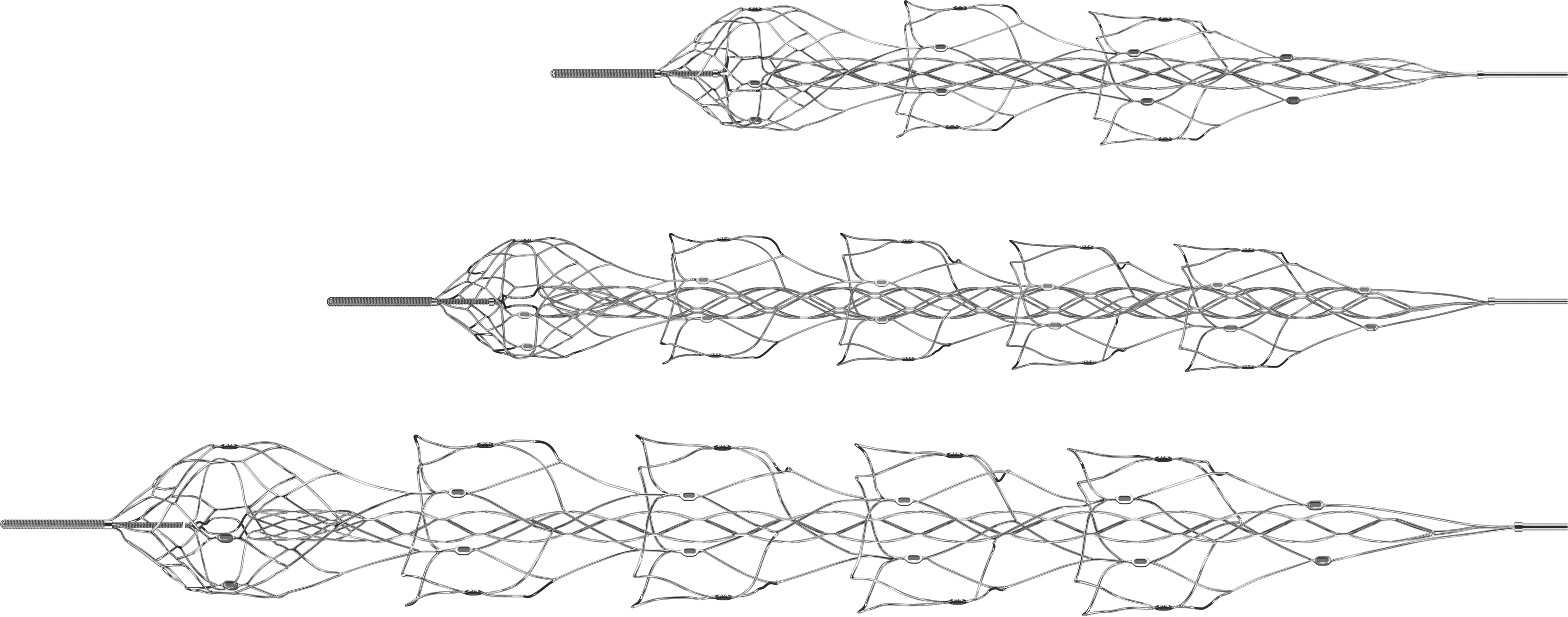
The 3D Revascularization Device (Penumbra, Inc., Alamedia, CA) is a unique, binary nitinol-based device. The device is laser cut from tubular nitinol. It is an open cell stent with outer leaflets designed to oppose the vessel wall, and 4 inner chambers that are designed for intraluminal clot interface (Figure 4). This stentriever is best classified as a combined open/ closed cell design, with some elements of both designs. Addition of radiopaque markers at the ends of the inner chambers helps with visualization. The outer leaflets are designed to exert radial force and separate the clot from the vessel wall, while the inner chambers are designed to increase clot integration, as well as reduce clot breakage and distal emboli during removal.47,48
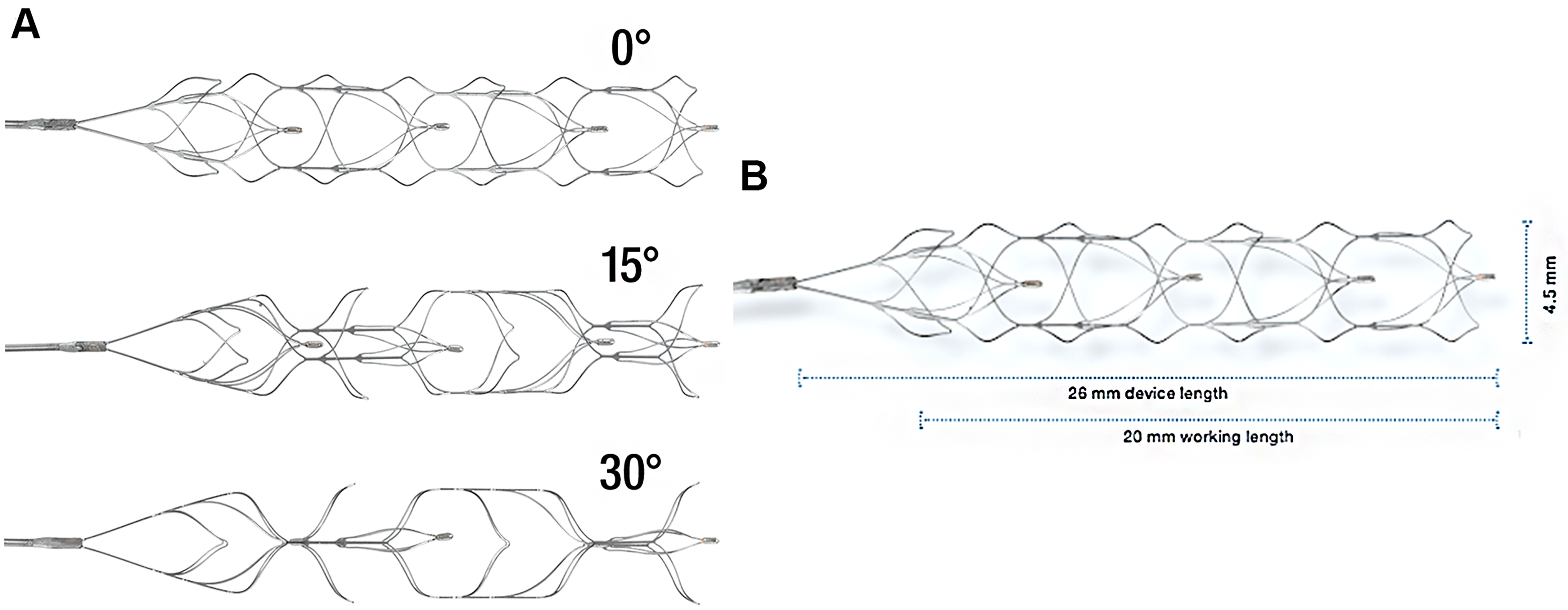
A And B. The Penumbra 3D Revascularization Device. 47 .
Clinical data for this device shows promise. Initial multi-center experience with the device showed a successful recanalization rate of 74%, and a first pass recanalization rate of 36%. There was a 4% incidence of symptomatic ICH associated with the device. The device is designed for used in conjunction with an aspiration catheter, and this trial therefore include aspiration provision. 49 A randomized trial of 3D Revascularization Device usage with suction aspiration versus aspiration alone showed 87.2% revascularization rates (TICI 2b/3) in the 3D Revascularization Device group, versus 82.3% in the aspiration-alone group. Symptomatic ICH associated with the device usage was 3.1%. 50
Over multiple iterations, the safety and efficacy of stentrievers has continued to improve. A rival technique to stent retrieval has since been developed: direct aspiration. Called ADAPT (A Direct Aspiration first Pass Technique), this technique relies on reinforced, wide-bore catheters that can be delivered to the clot itself, which can then be directly aspirated. 51 An early study reported recanalization rates of 78% using ADAPT alone. 52 The COMPASS trial randomized ADAPT and stent retrieval as a first-use technique in large vessel occlusion strokes, and showed equal likelihood of good outcomes using either technique. First pass revascularization was achieved in 57% of patients in the ADAPT group versus 51% of those in the stent retrieval group. Additionally, 85% of patients in the stent retrieval group utilized suction aspiration in conjunction with the stentriever. 53
Newer stentriever devices may therefore be adaptable to working in conjunction with direct aspiration, utilizing what has been termed the Solumbra technique. As the randomized study of the 3D Revascularization Device has shown, addition of a third-generation stentriever did improve angiographic outcomes. 50 The success of existing devices has set a high bar for newer stentriever development. Design of new devices must prioritize ease and timeliness of delivery to the target vessel, and improved rates of first pass recanalization.
Direct in vitro and in vivo animal model comparisons between various second and third generation stentrievers may help delineate the aspects of stent design that contribute to improved clinical performance and provide direction for further development. One such study compared commonly used stents, including Solitaire FR, Trevo, EmboTrap, and 3D Separator (older version) devices. Devices were compared using two mechanical and two functional tests. The mechanical tests utilized were ‘flat plate compression’ and ‘pull up traction’ tests. These tests revealed that complete section devices like Trevo (tubular stents) could not be directly compared to incomplete section devices like Solitaire (sheet stent). Most of the tested devices showed significant reduction in radial pressure when moved from 1.5 mm to 3.5 mm tubes. Functional testing of the devices consisted of retrieving tests, which tested consistent wall apposition while retrieval of the device around tortuous simulated vessels. While the Solitaire device showed consistent wall apposition, the EmboTrap and 3D Separator showed elongation around acute angled curves, and one tested Trevo device (3 × 20 mm) lost contact with the vessel wall completely. Thrombectomy trials with simulated red (clumped red blood cells) and white (fibrin based) clots of different sizes. All the tested devices showed an inability to engage and displace large white clots, while medium and small white clots were engaged and displaced to some degree. Red clots had complete engagement, but did undergo significant fragmentation, with potential for distal embolization. 54
Future trends in thrombectomy device development will continue to aim towards improving FPE rates, and to follow the evolving trends and new frontiers in thrombectomy indications. The primary amongst these is distal, or medium vessel thrombectomy. This will require smaller diameter, likely open-cell stent design stents that can provide mechanical traction and radial force around the MCA genu and in the more tortuous and smaller diameter M2 and M3 segments.
Future directions in this type of research must compare similar sized and classed stentrievers against each other and may also investigate the use of direct aspiration as an adjunct to stent use, to better quantify the additive effect of the Solumbra technique. Most of the studies stents have been updated by the vendors, therefore updating the literature with newer evidence is also of value. Comparative animal studies of stents may also be of value to the clinician. Advanced vessel wall imaging techniques, including synchrotron-based phase-contrast CT, could be employed after stent use to study endothelial damage in a non-invasive manner.
Conclusions
This review of stentrievers attempts to classify them using construction and design elements. Representative stentrievers from each generation of devices are presented along with clinical evidence supporting their use. There is a paucity of literature comparing stentrievers directly against each other with regards to mechanical and functional properties. Further testing of stents can be undertaken to inform future stentriever design and to guide clinical device selection. While device design continues to evolve at a significant pace, the aim of this review is to provide a framework for understanding the historical evolution of these devices from an engineering perspective, and criteria to evaluate newer devices with regards to their functional capabilities.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael E. Kelly, consultant for Imperative Care and Cerenovus. All other authors confirm no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.