
Abstract
Background
The WEB device offers another option for treating wide neck bifurcation aneurysms (WNBA). The objective was to compare procedure variables, radiation and implant cost between WEB and stent assisted coiling (SAC) for WNBA.
Methods
A retrospective comparison of similarly sized WNBA treated with SAC or WEB over 5-years was performed. The operating room (arrival-departure), anesthesia (intubation-extubation), procedure duration (puncture-closure), fluoroscopy time and radiation dose(m-Gy) were recorded from the patients’ charts. Implant cost per case of all implants (stents, coils, WEB) that were opened whether deployed or not was captured including any coils used in the WEB cases. The implant cost represented the true cost incurred by the institution.
Results
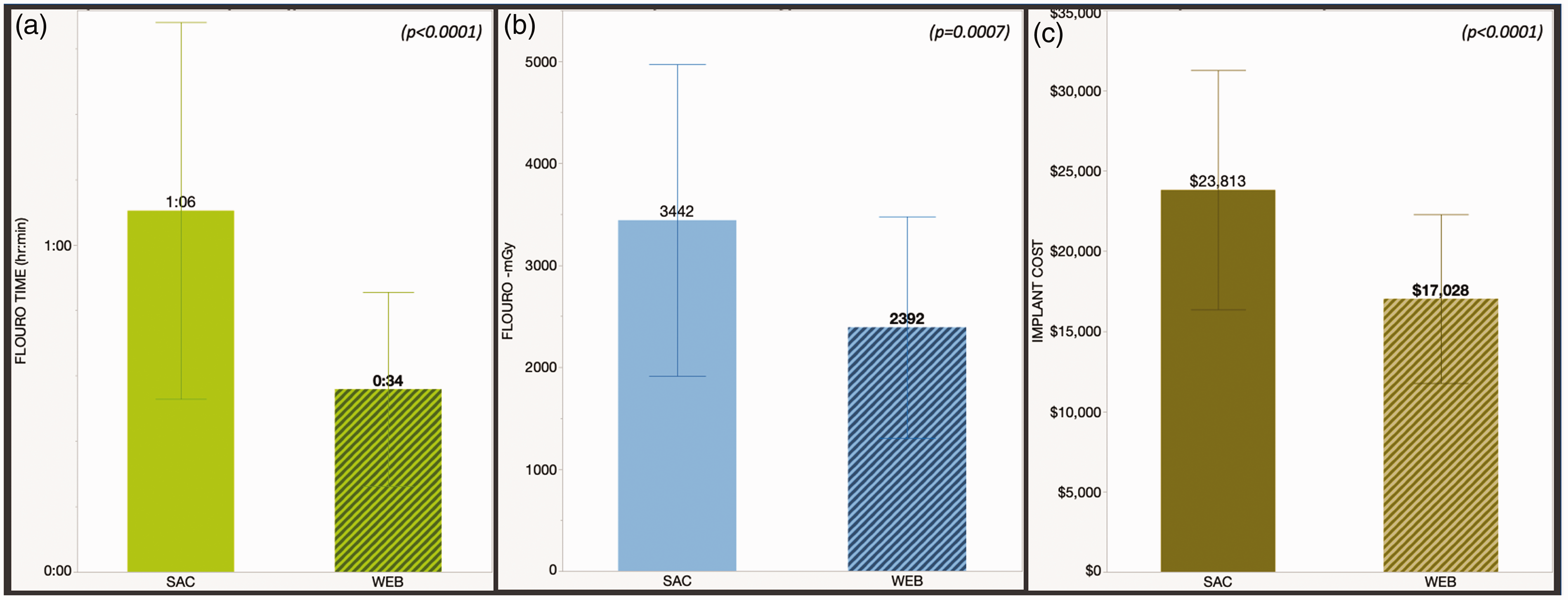
There were 46 WEB and 41 SAC cases with no significant difference in aneurysm size. There were more MCA and ACOMM (p = 0.005) and more ruptured aneurysms (p = 0.02) in the WEB group. Regarding procedure variables (hours:minutes): Operating room time WEB 2:31 (±0:37) versus SAC 3:41 (±0:50) (p < 0.0001); anesthesia duration WEB 2:05 (±0:31) versus SAC 3:13 (±0:51) (p < 0.0001) and procedure duration WEB 1:16 (±0:29) versus SAC 2:09 (±0:46) (p < 0.0001). Regarding radiation: Fluoroscopy time WEB 0:34 (±0:18) versus SAC 1:06 (±0:35) (p < 0.0001) and radiation dose WEB 2392(±1086)m-Gy versus SAC 3442 (±1528)m-Gy (p = 0.0007). The implant cost was $17,028(±$5,527) for the WEB versus $23,813 (±$7,456) for the SAC group (p < 0.0001).
Conclusion
The WEB group had significantly shorter operating room, procedure and anesthesia duration compared to the SAC group. The radiation dose and fluoroscopy time was lower for the WEB group. The total implant cost per case was significantly lower for the WEB versus the SAC group.
Keywords
Introduction
The WEB intrasaccular device (Microvention® Inc. Terumo, Aliso Viejo, CA) offers an alternative to stent assisted coiling (SAC) for wide neck bifurcation aneurysms. It is an additional tool, not necessarily suitable for all such aneurysms but with enough overlap of aneurysms that could be treated with either strategy, it is reasonable to compare the two treatments. A recent meta-analysis reported 12-month complete (Raymond-Roy 1) and adequate (Raymond-Roy 2) occlusion rates for wide neck bifurcation aneurysms (dome to neck ratio ≤2 or neck ≥4 mm) with endovascular therapy at 40% and 44% respectively. 1 When limited to level-1 studies the endovascular therapy complete occlusion rate was 29% and surgical clipping was at 44%. 1 The complete occlusion rate with coiling alone versus SAC for wide neck aneurysms was reported at 27% and 46% in the MAPS trial. 2 Another recent core lab adjudicated study focused on endovascular treatment of wide neck basial apex and middle cerebral artery bifurcation aneurysms showed complete and adequate occlusion rates of 30.6% and 63% respectively. 3 In comparison, the WEB-IT trial 4 which led to the FDA approval of the device and its commercial availability in the US in February 2019 reported a 12-month complete and adequate occlusion rate of 54% and 85% respectively with 1.4% morbidity and 0% mortality. Several other core lab adjudicated clinical trials and registries have shown similar favorable efficacy and safety profile for WEB4–8 and one recent study showed comparable outcomes for WEB versus SAC with a lower procedural complication rate for the WEB group. 9
A single implant for cerebral aneurysms with favorable outcomes and safety versus implantation of multiple devices has theoretical benefits of shorter treatment times and reduced radiation exposure as demonstrated for flow diversion. 10 , 11 Cost is another important parameter and all other things being equal this could be a determining factor in treatment selection. There is published literature on cost of endovascular and microsurgical treatment of cerebral aneurysms12–14 and also on comparison of flow diversion with a single implant such as Pipeline (Medtronic, Minneapolis, MN) versus coiling. 12 , 15 , 16 The objective of this study was to analyze operating room variables, radiation exposure and implant cost for the WEB device versus SAC for treatment of wide neck bifurcation aneurysms (WNBA).
Methods
The study was performed under an institutional review board approved protocol. The study design is a single center retrospective analysis. The sample for the study was generated from a prospectively maintained aneurysm database.
Inclusion criteria
Aneurysms involving the middle cerebral artery bifurcation (MCA), the anterior communicating artery (ACOMM), the internal carotid artery terminus (ICA-T), the basilar artery (BA) or the posterior communicating artery (PCOMM) treated with stent assisted coiling (SAC) or WEB (Microvention® Inc. Terumo, Aliso Viejo, CA) were identified from the database. Important to note that the PCOMM aneurysm location is off-label for WEB. However the reasons to include PCOMM aneurysms was that these have been previously classified in both the sidewall and bifurcation categories,17–19 have a more aggressive natural history than other internal carotid artery sidewall aneurysms 17 ,19–21 and have been successfully treated with the WEB device. 22 , 23 The aneurysm size was restricted to an average aneurysm diameter (obtained from two orthogonal measurements) between 3 and 10 mm because the WEB device is restricted to these sizes and this allowed for comparison of similar aneurysms. The majority of SAC cases were treated prior to the WEB availability in the US in February 2019.
This is because following the launch, the WEB was used as the first line treatment for bifurcation aneurysms and SAC was used if the WEB was not readily available. Due to limited availability of WEB after its launch, the device was not stocked on the shelf and had to be brought in on request. SAC was also used if the aneurysm size was outside of the WEB dimensions, however these cases with were excluded from analysis because of aneurysm size. Lastly in a minority of cases (n = 3), SAC was preferred to protect a side branch that could have been compromised by the WEB.
Procedure variables
The following operating room variables were recorded from the electronic medical records “event log” (Figure 1
An example of an “Event log” from an endovascular aneurysm treatment. The names of the staff and the physician have been redacted. The procedure related times (highlighted in red) were recorded from this log for each patient. The log also documents the radiation dose and fluoroscopy time for each patient (highlighted in blue). Operating room time – patient arrival in room to patient departure from room. Procedure duration – arterial sheath placement to arterial sheath removal. Anesthesia time – intubation to extubation.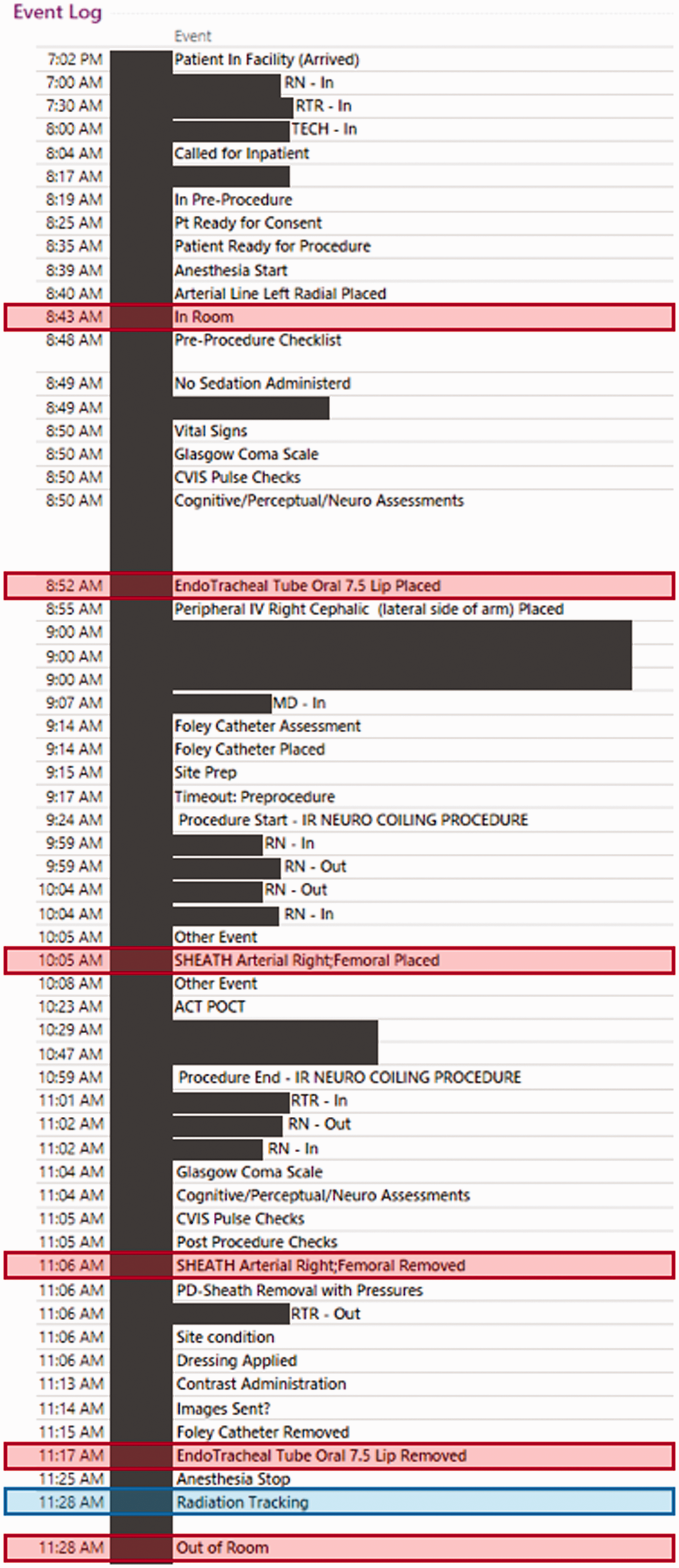
The two radiation related parameters automatically captured by the biplane angiography unit (Siemens Artis Q, Siemens Healthiness GmbH, Erlangen, Germany) and recorded in the event log included total fluoroscopy time for both planes recorded in minutes and the total radiation dose recorded in milli-gray (m-GY). The radiation dose and time was for the live or subtracted fluoroscopy use as well as the angiography runs including rotational angiography and DynaCT (proprietary low contrast high resolution imaging for visualization of the implant and the arterial vasculature).
Implant cost analysis
The implant cost included the
Statistical analysis
All data analysis was performed using JMP statistical software (JMP® Pro 14.0.0 – SAS Institute Inc., Cary, North Carolina, USA). The significance of simple bivariate associations was assessed using Fisher
Results
Distribution of treatment type for ALL bifurcation aneurysms (not just wide-neck) from 2015 onwards, before and after the commercial availability (February 2019) of the device in the US (p < 0.0001).
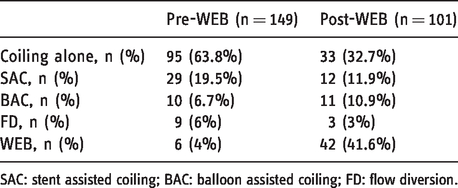
SAC: stent assisted coiling; BAC: balloon assisted coiling; FD: flow diversion.
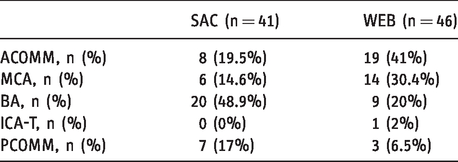
Distribution of aneurysms by location for the two treatment groups (p = 0.005).
The operating room time, anesthesia duration and procedure duration were significantly lower for the WEB group versus the SAC group (Figure 2
The operating room time (bottom) is the time spent by the patient in the interventional suite from arrival to departure. The anesthesia duration (middle) is from intubation to extubation and the procedure duration (top) is from arterial access to closure. All times are represented as hours: minutes. The fluoroscopy time (a), the radiation dose (b) and the implant costs (c) are presented.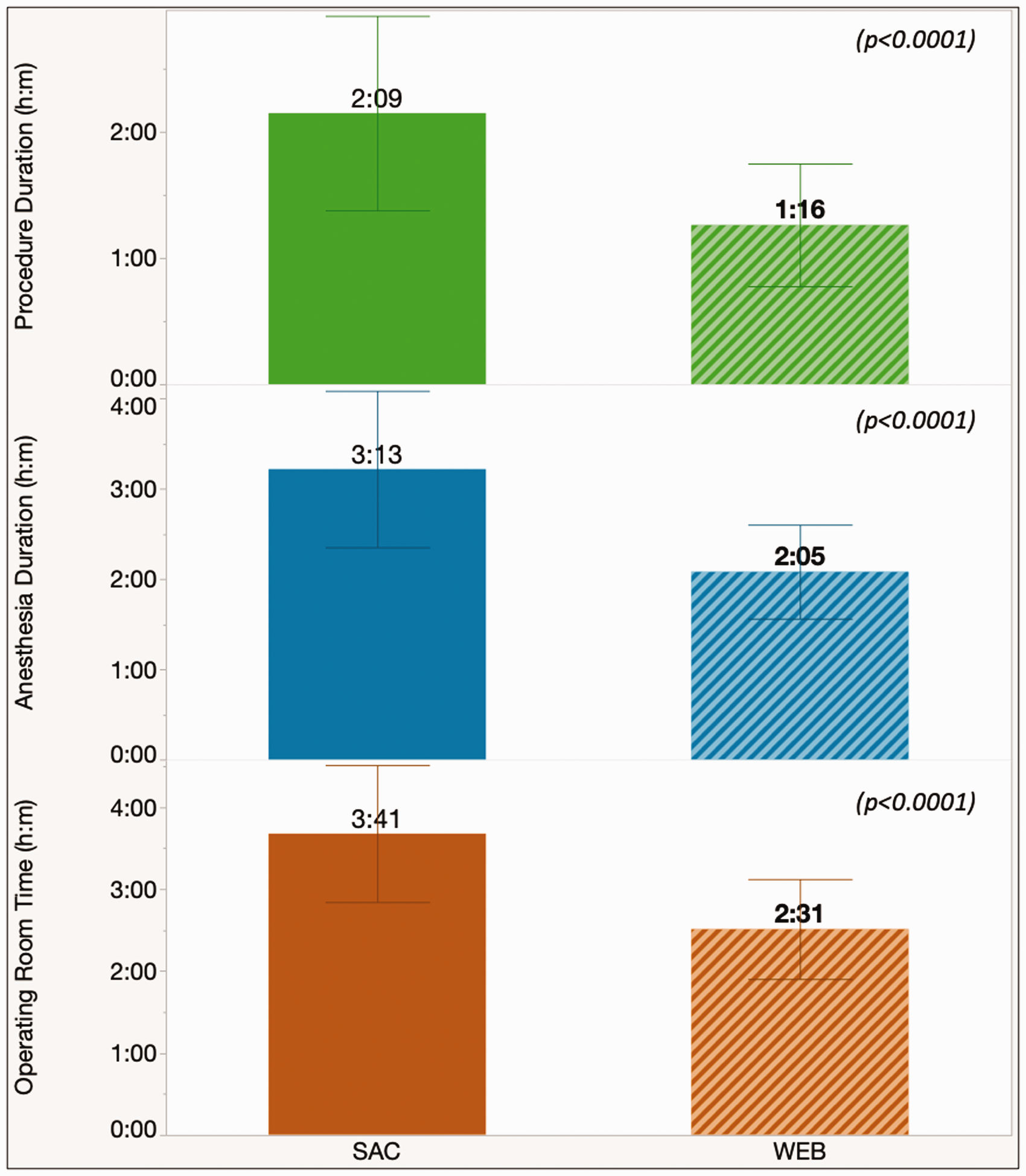
There were 5(11%) cases in the WEB group where the first device was not implanted because of size discrepancy and a second device had to be used. There was a 6th case where two WEB devices were implanted in a bi-lobed ACOMM aneurysm, one device in each lobe. There were three WEB cases where coils were also used to occlude a side lobe not completely covered by the device, in these cases the cost of coils was added to the total implant cost. None of the WEB cases required an adjunctive stent or balloon. In the SAC group (n = 41), a laser cut adjunctive device was used in 32 (78%) and a braided device in 9 (22%) patients. A Y-stent configuration was used in 2 (5%) patients. The average number of coils used in the SAC group was 6 (±3) and the median was 5 (IQR 4-8).
A follow up imaging study was available in 34(83%) patients in the SAC and 34 (74%) patients in the WEB group (p = 0.3). The median and mean follow up for the SAC group was 17(IQR 5–31) months and 19 (±15) months respectively compared to the WEB group that had a median and mean follow up of 6 (IQR 3–12) and 13 (±16) months respectively (p = 0.04). In the SAC group, a complete and adequate occlusion on follow up was seen in 21(62%) and 7(21%) patients respectively versus complete and adequate occlusion rates of 25 (74%) and 8(23%) in the WEB group (p = 0.1). There were 4 (10%) patients in the SAC group requiring a retreatment compared to none in the WEB group (p = 0.01). A sample comparison of the SAC and WEB cases is presented in Figure 4
Sample case comparison of SAC and WEB cases with procedure variables, radiation and cost listed adjacent to each case. The preoperative and follow up angiogram images are presented. All times are in hours: minutes. D/N: Dome-to-neck. The first case is of unruptured basilar apex aneurysms treated with stent coiling (top) and WEB (bottom). The second case is of left MCA bifurcation aneurysms that were treated with Y-stenting (top) and WEB (bottom). A single WEB device was used for both cases shown. *Implant cost is shown as the additional cost for the SAC compared to the WEB case.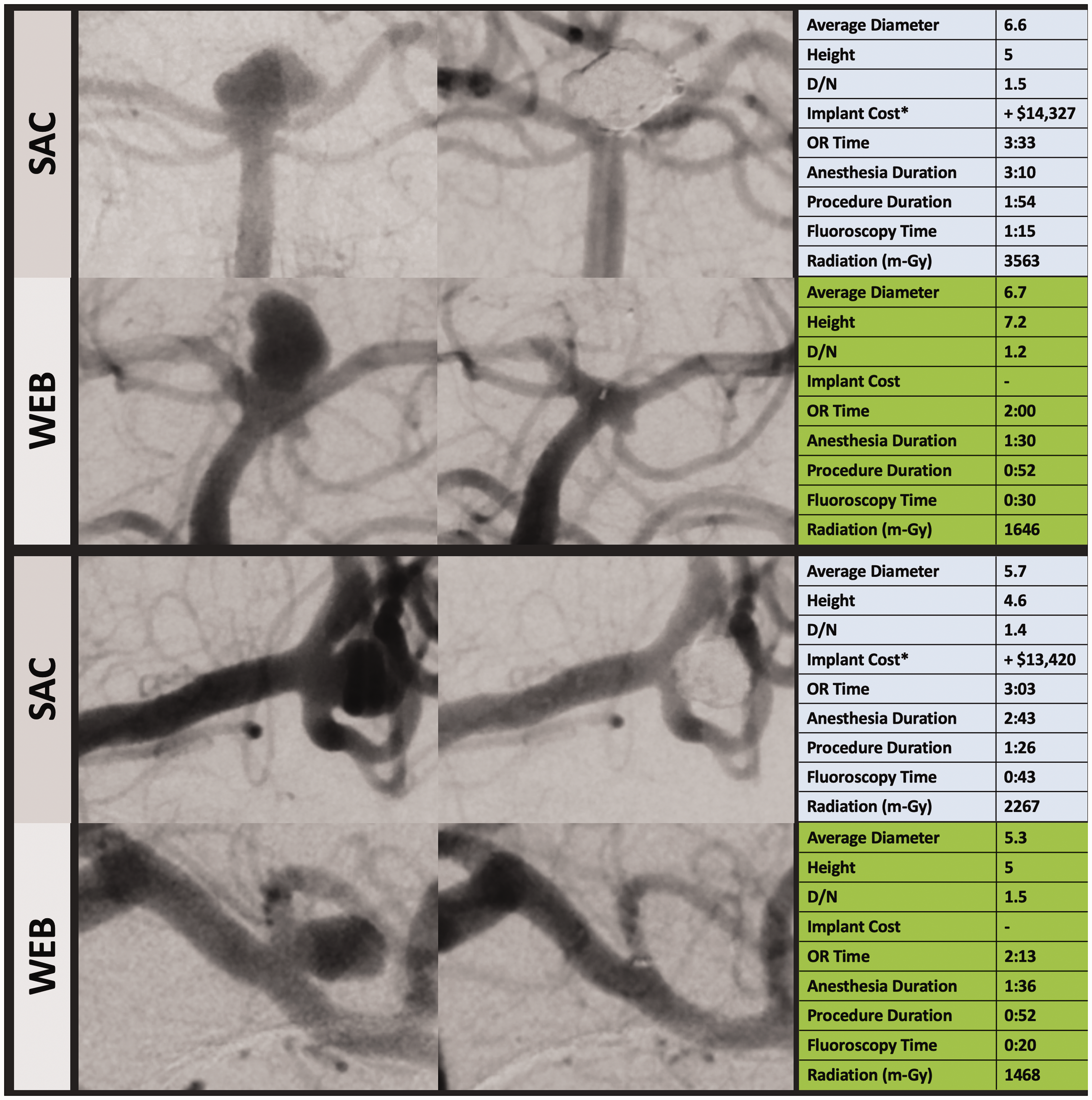
Discussion
The majority of cerebral aneurysms involve a bifurcation location 20 and the most frequent bifurcation locations are the MCA and the ACOMM complex. 24 The ISUIA study 20 showed that aneurysms at the MCA and ACOMM location constituted almost half of all the surgically treated aneurysms whereas these constituted only 21% of the aneurysms treated with an endovascular approach. 20 The study was published in 2003 and these trends have expectedly changed with more locations becoming accessible to endovascular therapy. These trends also vary by geographic location as microsurgical clipping of MCA and ACOMM aneurysms is likely more common in the US than Europe as demonstrated by a recent survey of cerebral aneurysm practice trends in the US. 25 A recent meta-analysis comparing clipping with endovascular therapy for unruptured MCA aneurysms showed comparable procedural complications and mortality for the two methods with an increased probability of good neurological outcomes for the endovascular treatment group. 26 In our study, there was a significantly higher proportion of MCA aneurysms in the WEB group because many of these were previously approached by surgical clipping. Availability of WEB expanded the scope of endovascular treatment for ACOMM and MCA aneurysms allowing endovascular therapy to match the disease incidence in terms of aneurysm location.
The use of WEB significantly shortened our operating room usage time, the time patient was under general anesthesia and the time of the procedure from arterial access to closure compared to SAC for similarly sized aneurysms. Though not calculated, reduced operating room and anesthesia times reduces indirect costs and overheads. This also reduces the opportunity cost as shorter operating room time per case potentially allows for more cases to be scheduled and shortens the lag time from decision-to-treat to the treatment itself. Shorter anesthesia times can similarly free up these resources for other cases. We show a significant reduction in radiation dose due to reduced fluoroscopy time. This is to be expected with reduced procedure times, a similar benefit was shown for the Pipeline embolization device over stent assisted coiling. 10 , 11 The average dose for WEB cases in our series was slightly lower than the average dose for the Pipeline cases. 10 Our fluoroscopy time of 34 minutes (±18) is similar to other WEB related studies. 27 , 28 For all variables related to procedure times and radiation, the use of single implant solutions versus implantation of multiple devices carries an intuitive advantage.
Our study showed a significant reduction in implant cost per case for the WEB device compared to stent assisted coiling. Almost our cases required a single WEB device and only three required additional coils, none of the WEB cases required a stent. It is expected that some of these cases may require an adjunctive stent, a technique that has been demonstrated 29 , 30 and will add to the implant cost. There are previous cost analyses for microsurgical clipping and endovascular treatment12–14 and we assume that the long-term cost effectiveness for WEB would be similar to other endovascular approaches because the length of stay and effectiveness of therapy should be similar. However one factor that could alter this assumption is the cost of post-operative dual antiplatelet therapy that is generally longer for SAC and typically not required for WEB cases. 31 The implant cost for WEB should stay constant for different sizes (within the device range) but the implant cost for SAC is potentially greater for larger aneurysms. In our series, WEB allowed the treatment of significantly more ruptured aneurysms than the SAC group. Excluding ruptured aneurysms from analysis favors the WEB group because procedure and OR times were higher for ruptured cases as it included complete angiographic evaluation of non-target arteries. A staged approached for SAC 32 is often used for wide neck ruptured aneurysms with primary coiling as the acute treatment followed by completion SAC at a later date. This multistage treatment understandably incurs a higher direct and indirect cost with duplication of the endovascular procedure versus a single stage treatment. The WEB device as a single treatment has been shown to be effective and safe for wide necked ruptured aneurysms. 33 , 34
Limitations
There are several limitations. First this is a retrospective analysis subject to operator bias in the choice of an endovascular treatment as compared to prospectively assigned treatment approach. The two cohorts of SAC and WEB were similar in size but differed in the aneurysm locations and rupture status. Significantly more MCA and ACOMM aneurysms were treated in the WEB group, this follows the incidence of aneurysms by location. There were more ruptured aneurysms in the WEB group which favors the SAC group as procedure, operating room and fluoroscopy times for these cases included complete angiographic evaluation of non-target vessels. The implant cost is specific to the institution and also dependent on operator preference. It is possible that the difference is less significant if an institution has a different cost structure or if the operator preferred the least expensive implant (stents or coils). Lastly, the implant cost was the cost of the device at the time for treatment and not adjusted for current costs which favors the SAC group since the cost of stents and coils has increased over time.
Conclusion
The WEB device increased the use of endovascular therapy for bifurcation aneurysms mainly by expanded use in MCA and ACOMM aneurysms. As a single implant, the WEB offers faster procedure times, shorter anesthesia duration and reduced operating room times over stent assisted coiling for aneurysm diameters between 3 and 10 mm. The radiation exposure and the implant cost per case was significantly lower for the WEB cohort. There was no need for long term dual antiplatelet therapy which further reduces the cost of treatment. More ruptured aneurysms were treated in the WEB group which has benefits over SAC and staged treatment of wide neck ruptured aneurysms. The two treatment approaches are not mutually exclusive and WEB may not replace SAC but offers an additional option that further enhances the scope of endovascular aneurysm therapy.
Footnotes
Acknowledgements
Jennifer Domico for diligently capturing and maintaining the research database.
Contributorship
ATR contributed to study design, data collection, analysis and manuscript preparation. RCT, RGB and SB contributed to data collection.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Both ATR and SB have a consulting agreement with Microvention and serve as proctors for the WEB device.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.