
Abstract
Background/purpose
The benefit of endovascular thrombectomy in acute ischemic stroke (AIS) therapy of proximal large vessel occlusions (LVO) is established. However, there are few prospective studies evaluating the use of a direct aspiration first pass technique in distal vessel occlusions. This post hoc analysis of the PROMISE study examines the safety and effectiveness of the Penumbra System with the ACE68 and ACE64 Reperfusion Catheters for aspiration thrombectomy in the M1 and M2 segments of the middle cerebral artery.
Methods
PROMISE is a prospective, multicenter study that enrolled 204 patients with anterior circulation LVO AIS-treated frontline with ACE68/ACE64 catheters. We compared clinical and angiographic outcomes, complications, and mortality in patients with M1 and M2 occlusions. The association of M1 and M2 location and functional independence or mTICI 2b-3 reperfusion was described in univariable and multivariable analyses.
Results
One hundred sixty-one patients (124 M1 and 37 M2 locations) met the study criteria. Post procedure mTICI 2b-3 reperfusion (93% vs. 92%, p = 1.00), functional independence (57% vs. 70%, p = 0.18), symptomatic intracranial hemorrhage (1.6% vs. 2.7%, p = 0.55), device- or procedure-related serious adverse events at 30 days (4.0% vs. 8.1%, p = 0.39), and mortality at 90 days (6.6% vs. 2.7%, p = 0.69) were comparable between M1 and M2 occlusions. In multivariable analysis, lower age, lower baseline NIHSS, and shorter time from onset to admission were independent predictors of functional independence.
Conclusions
For frontline aspiration thrombectomy of stroke, use of large-bore ACE68/ACE64 catheters for treatment of M2 occlusions appeared as safe and effective as for M1 occlusions.
Introduction
The role of endovascular therapy (EVT) in the treatment of acute ischemic stroke (AIS) secondary to large vessel occlusion (LVO) has been established.1–8 With distal occlusions, EVT may be more technically challenging, and the target artery’s vessel diameter, tortuosity, and wall thickness may impact periprocedural safety. In addition, IV rt-PA may be more effective in more distal M2 segment occlusions compared with other LVO locations. 9 As stroke therapy continues to advance, the role of EVT in the treatment of distal vessel occlusions is an area of current investigation.
The majority of prior randomized controlled trials (RCTs) involving EVT were designed to include only patients with LVO up to the M1 middle cerebral artery (MCA) location. Data on the natural history of M2 MCA occlusion strokes indicate that around half (54%) of the untreated patients would attain functional independence and the rates of six-month mortality are similar to M1 occlusions. 10 Several retrospective studies examining EVT for M2 occlusions found similar or greater rates of successful revascularization (mTICI 2b/3) and good functional outcome (mRS 0–2) at follow-up as compared to M1 occlusions.11–14 In a retrospective study of patients with M2 occlusions, Sarraj et al. 15 found that EVT resulted in significantly greater odds of functional improvement compared to medical management. Additionally, a meta-analysis of data from the HERMES collaboration examining outcomes of EVT in M2 MCA occlusions compared to medical management found a treatment effect in favor of EVT regarding good functional outcome (mRS 0–2 at 90 days). 16 These studies included primarily stent-retriever-based EVT.
More recently, ADAPT (A Direct Aspiration First Pass Technique), a thrombectomy approach in which aspiration is used frontline to remove the thrombus was introduced.17–19 Few prospective studies on aspiration thrombectomy have included patients with M2 occlusions. A post hoc analysis of the ASTER study (the first RCT to compare the safety and efficacy of aspiration thrombectomy vs. stent retrievers), found 54% functional independence and 90% mTICI 2b-3 with aspiration thrombectomy in M2 occlusions (n = 48) with no significant difference as compared to the M2 stent retriever (n = 31) group. 20
The Prospective, Multicenter, Observational, Single-arm European Registry on the ACE Reperfusion Catheters and the Penumbra System in the Treatment of Acute Ischemic Stroke (PROMISE) study was a prospective, multicenter registry examining real-world data on the safety and effectiveness of the Penumbra System with the ACE68/64 in patients with AIS from LVO, treated with the ADAPT technique. Overall results of the PROMISE study have been previously reported. 21 The goal of this post hoc analysis of the PROMISE study was to evaluate and compare the safety and efficacy of the ADAPT technique with large-bore catheter aspiration thrombectomy in M1 and M2 MCA occlusions.
Methods
PROMISE has been described previously. 21 Treatment consisted of the ADAPT technique with aspiration using ACE68 and ACE64 Reperfusion Catheters as first approach. For this study, we performed a post hoc analysis of the parameters: day-90 mRS 0–2, mTICI 2b-3, and safety for patients with isolated occlusions either in the M1 or M2 segments of the MCA. The core lab defined M2 as the continuation of the distal M1 trunk beyond a holotemporal or posterior temporal branch. 22 The target vessel was defined by the most proximal face of the clot. Patients with tandem occlusions were excluded. The association of covariates, including occlusion location (M1 or M2), and functional independence or mTICI 2b-3 reperfusion was tested in univariable and multivariable analyses.
Outcome measures
Primary endpoints were radiographic revascularization of the occluded target vessel to mTICI 2b-3 at immediate post procedure, as adjudicated by an independent Core Laboratory and functional independence (mRS 0–2 at 90 days). Secondary endpoints were any device- and procedure-related serious adverse events (SAEs) at 24 h and 30 days post procedure, all-cause mortality at 90 days, and symptomatic intracranial hemorrhage (sICH) at 24 h. Safety endpoints were adjudicated for severity and causality by an independent Clinical Events Committee (CEC) consisting of three members. All images were reviewed and adjudicated by an independent Imaging Core Laboratory for mTICI and for procedural and safety assessments (including identification and classification of intracranial hemorrhage).
Statistical analysis
Baseline clinical and imaging data were summarized using standard descriptive statistics. This included the number of observations, mean, median, standard deviation, minimum and maximum for continuous variables and counts and percentages for discrete variables. The association of M1 and M2 target vessel location and functional independence or mTICI 2b-3 reperfusion was tested in unadjusted and adjusted analyses. The tested univariable covariates (baseline and procedural) with a p-value < 0.20 were included in the multivariable model. The multivariable model utilized stepwise selection methods with all considered covariates with univariable p-value of < 0.20 to the outcome variables, with entry alpha value of 0.25 and stay alpha value of 0.05. All confidence intervals presented were two-sided. All statistical tests were two-tailed with a significance level of 0.05. Analyses were performed using SAS® software (version 9.4; SAS Institute). 23
Ethics statement
The patients or their representatives provided written informed consent, according to the local regulations. The following local and central Ethics Committees approved the PROMISE study: UMC Utrecht (approval waived), Ruhr University Bochum (15-5458), University of Münster (2016-319-b-S), TU Dresden (EK 73022016), University of Lübeck (16-026), Otto-von-Guericke University (101/16), University Hospital Virgen Arrixaca (2016-1-5-HCUVA), CEIC de Euskadi del País Vasco (PI2016005 (PS)), Kanton St. Gallen (2016-00457), Milano Area C (18-022016), Toscana Region (VV-TMF-11039), Province of Messina (VV-TMF-05240/-05238), Azienda Sanitaria Locale Brindisi (104/16), Ile-de-France III (2016-A01219-42), University Hospital Vall d’Hebron (PR(AG)219/2016), Hospital Clinic of Barcelona (PI2016005 (PS)), Midtjylland Region (1-10-72-182-16), Bayerischen Landesärztekammer (mb BO 16008), Comissão de Ética para a Saúde, CES (51/2017).
Results
Baseline and procedural characteristics.
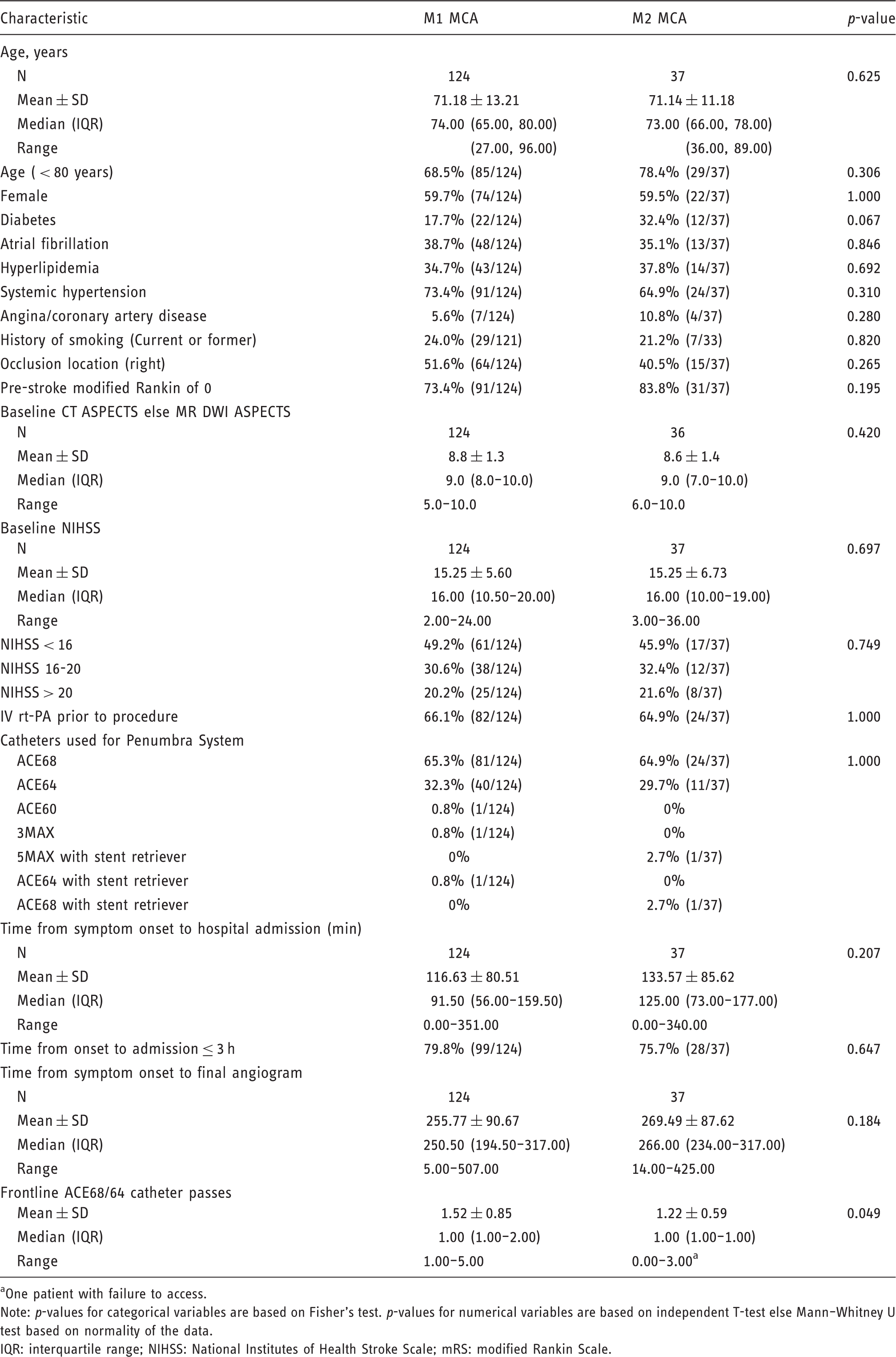
One patient with failure to access.
Note: p-values for categorical variables are based on Fisher's test. p-values for numerical variables are based on independent T-test else Mann–Whitney U test based on normality of the data.
IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin Scale.
Safety and efficacy outcomes.
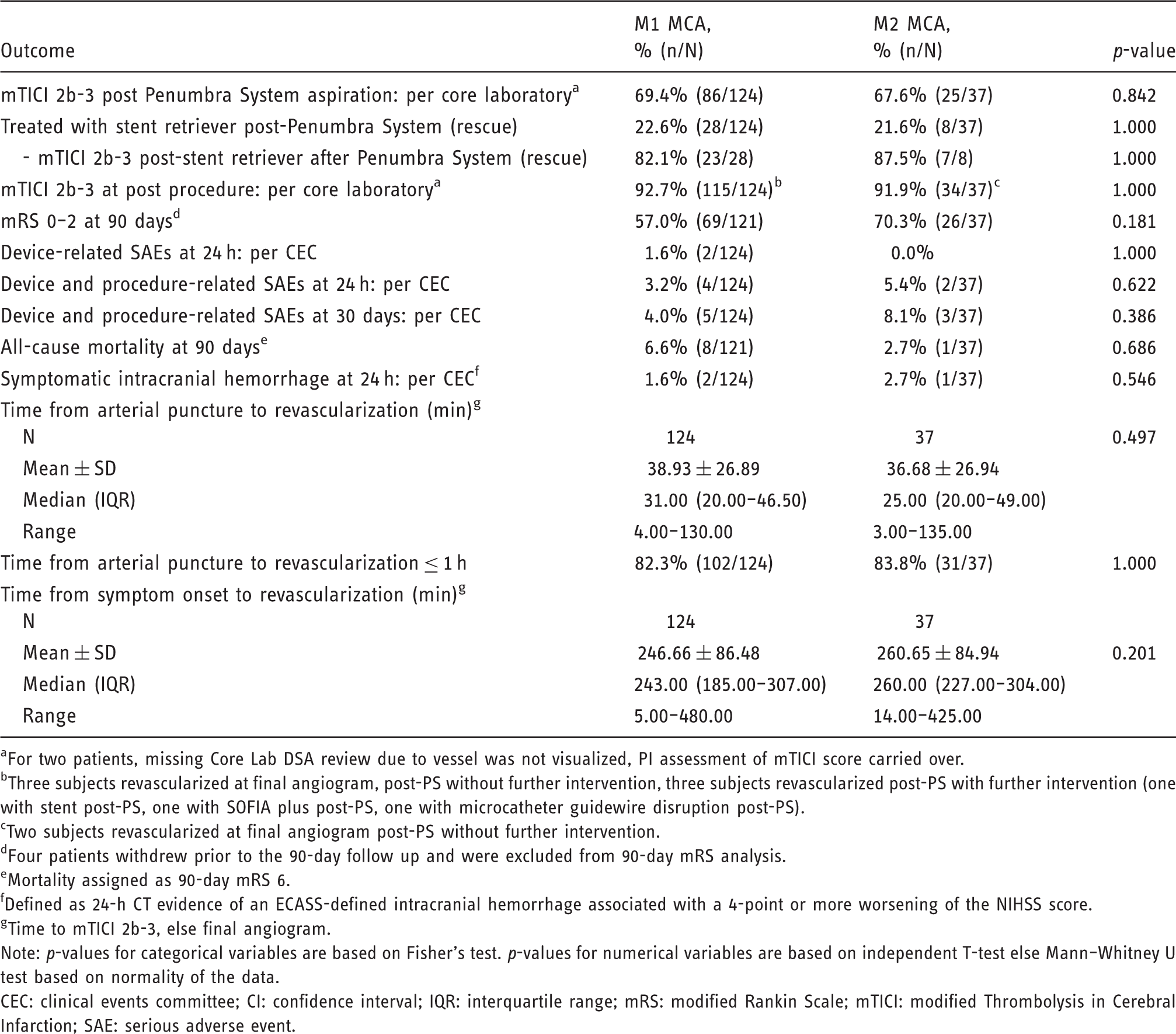
For two patients, missing Core Lab DSA review due to vessel was not visualized, PI assessment of mTICI score carried over.
Three subjects revascularized at final angiogram, post-PS without further intervention, three subjects revascularized post-PS with further intervention (one with stent post-PS, one with SOFIA plus post-PS, one with microcatheter guidewire disruption post-PS).
Two subjects revascularized at final angiogram post-PS without further intervention.
Four patients withdrew prior to the 90-day follow up and were excluded from 90-day mRS analysis.
Mortality assigned as 90-day mRS 6.
Defined as 24-h CT evidence of an ECASS-defined intracranial hemorrhage associated with a 4-point or more worsening of the NIHSS score.
Time to mTICI 2b-3, else final angiogram.
Note: p-values for categorical variables are based on Fisher's test. p-values for numerical variables are based on independent T-test else Mann–Whitney U test based on normality of the data.
CEC: clinical events committee; CI: confidence interval; IQR: interquartile range; mRS: modified Rankin Scale; mTICI: modified Thrombolysis in Cerebral Infarction; SAE: serious adverse event.
The times to revascularization data are shown in Table 2. The median reperfusion time (arterial access to mTICI 2b-3) was 31.0 min in M1 and 25.0 min in M2 occlusions. The median time from stroke onset to mTICI 2b-3 flow or final angiogram, if 2b-3 was not achieved, was 243.0 min and 260.0 min, respectively.
Predictive analyses for 90-day mRS 0–2.
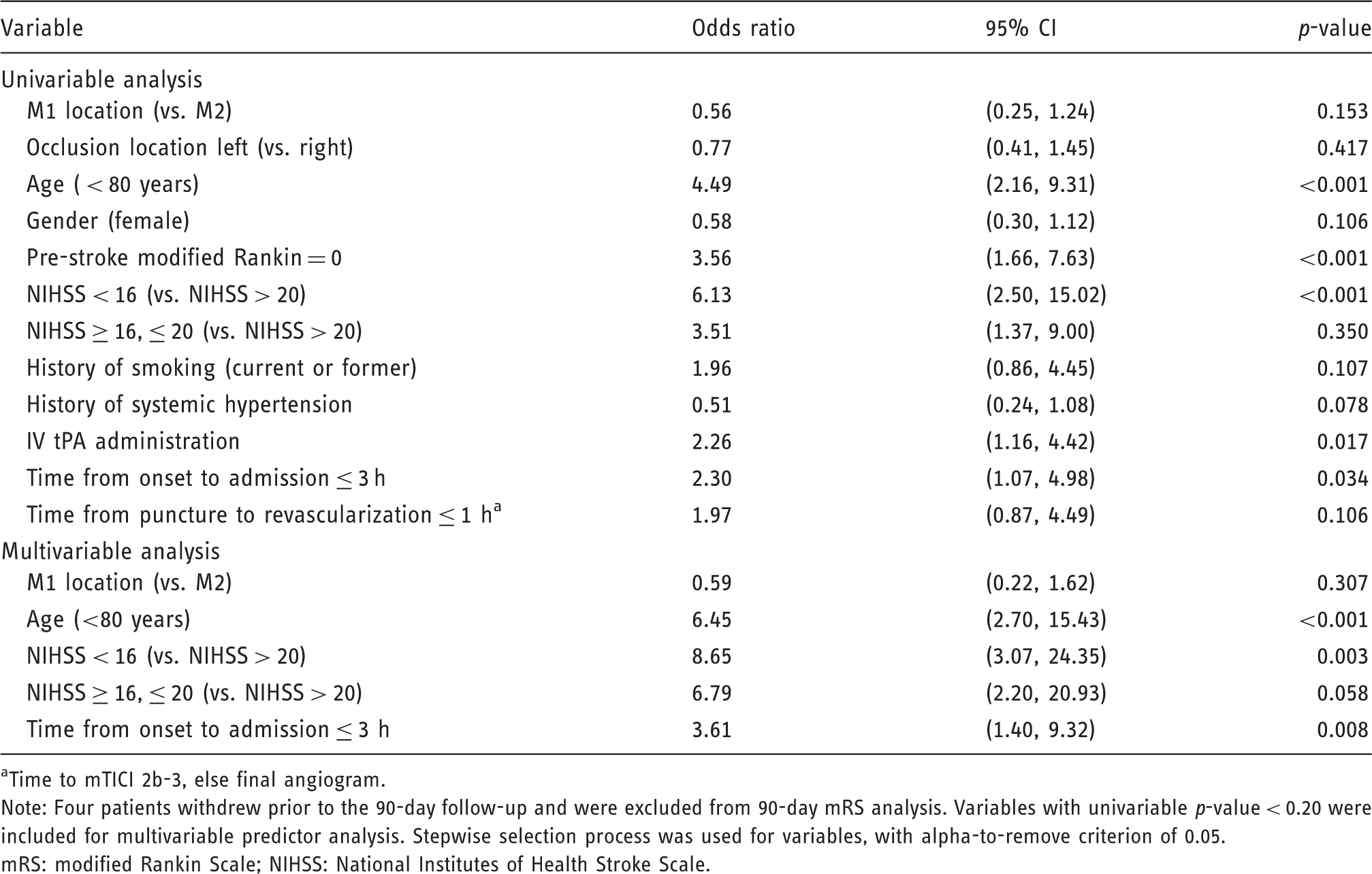
Time to mTICI 2b-3, else final angiogram.
Note: Four patients withdrew prior to the 90-day follow-up and were excluded from 90-day mRS analysis. Variables with univariable p-value < 0.20 were included for multivariable predictor analysis. Stepwise selection process was used for variables, with alpha-to-remove criterion of 0.05.
mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale.
Predictive analyses for mTICI 2b-3 post procedure.
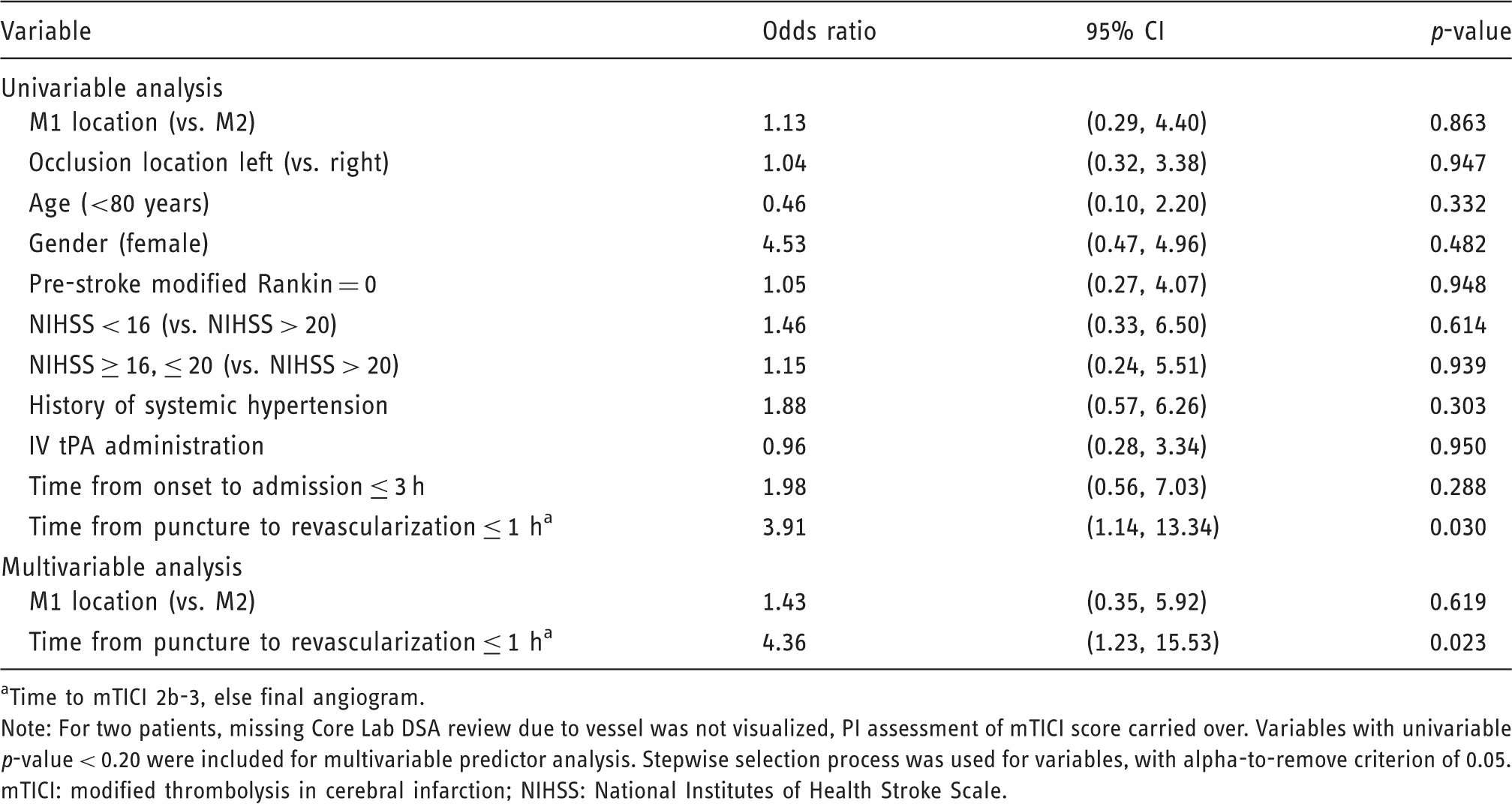
Time to mTICI 2b-3, else final angiogram.
Note: For two patients, missing Core Lab DSA review due to vessel was not visualized, PI assessment of mTICI score carried over. Variables with univariable p-value < 0.20 were included for multivariable predictor analysis. Stepwise selection process was used for variables, with alpha-to-remove criterion of 0.05.
mTICI: modified thrombolysis in cerebral infarction; NIHSS: National Institutes of Health Stroke Scale.
Discussion
Findings from the PROMISE study support using the frontline ADAPT technique in real-world practice with ACE64 and ACE68 reperfusion catheters in patients with AIS secondary to anterior LVO. 21 A sizeable percentage of PROMISE study patients (18%) had an occlusion in the M2 branch of the MCA. Our study suggests that clinical and angiographic outcomes are comparable between patients with M1 and M2 occlusions. Recanalization rate and time to recanalization were comparable between both groups. There was a significantly higher number of catheter passes in the M1 cohort as compared to the M2 cohort (mean 1.52 vs 1.22, p = 0.049). This phenomenon may be due to improved catheter-to-vessel size compatibility (e.g. catheter inner diameter more closely approximates vessel diameter), and the clot burden in M1 may be higher.
There was a non-statistically significant trend toward a higher percentage of good outcomes at 90-days in our M2 subgroup despite similar pre-treatment NIHSS between the groups. A potential explanation for this is that smaller infarct cores are expected with M2 occlusions. Similar NIHSS between groups may be multifactorial. First is the inherent limitation in the NIHSS which places a greater emphasis on left-sided functions (e.g. language) than on right. 24 Left-sided occlusions occurred more frequently in this study’s M2 cohort than the M1 cohort (59.5% vs. 48.4%, p = 0.265). Second is the large anatomic variation of MCA branching patterns, commonly one branch may be dominant, supplying a larger territory (in some cases dominant M2 diameter may even approximate the diameter of M1), and therefore leading to more severe clinical presentations.25,26 It is possible that a large number of M2 patients in our study were in fact dominant M2 branch occlusions. However, we are unable to verify this as this information was not collected as part of the PROMISE study. 21 Finally, because the PROMISE study enrolled subjects who underwent ADAPT using the ACE 64 or ACE 68 reperfusion catheters in accordance to site routine practice, some selection bias may exist, wherein distal occlusions with lower clinical severities or located in non-dominant M2 branches were more likely to be medically managed or treated with catheters not included in PROMISE (e.g. 3MAX) or stent retrievers.
To date, endovascular treatment of distal MCA stroke remains controversial due to smaller penumbra volumes, more favorable outcomes, and greater effectiveness of IV tPA in more distal occlusion strokes. The effectiveness of IV tPA, although higher than in the M1 segment, reaches only about one-third of patients treated. 9 Despite representing 20–41% of anterior circulation strokes, 27 M2 occlusions were greatly under-represented in major randomized trials that established the benefit of endovascular treatments for LVO strokes.1,3,28 In the European Stroke Organization (ESO)-ESMINT guidelines published in 2019, there was a consensus that mechanical thrombectomy would be reasonable for patients with M2 occlusion. 29
Use of direct aspiration in these territories may have the advantage of not crossing the occlusion and could be safer than stent retrievers. 30 It has also been suggested that aspiration has the potential for less endothelial damage. However, results from bench-top and animal studies have been mixed, with some finding significantly less endothelial trauma with aspiration and others finding non-significant levels of vessel damage between aspiration and stent retriever.31–34 Additionally, studies have not found increased endothelial damage to be associated with adverse clinical outcomes.35,36 Recently, a meta-analysis investigating the use of stent retriever or aspiration thrombectomy in M2 compared with M1 occlusions was published. 37 In the M2 subgroup (1080 patients), functional independence rate was 59%, recanalization rate was 81%, mortality rate was 16%, and sICH rate was 10%. There were no significant differences in the outcomes between M1 and M2 occlusions despite higher sICH rates in the M2 occlusions group. 37 In our study, the favorable clinical outcomes were noticeably higher, with a functional independence rate of 70.3%, a recanalization rate of 91.9%, a mortality rate of 2.7%, and a sICH rate of 2.7%. The improvements observed in our series may be due to improved technical skills from the higher volume of endovascular treatments, utilization of larger bore aspiration catheters, and/or improved patient processing times.
The increased sICH rates observed in some studies may reflect the risk associated with intervention on smaller and more fragile vessels. However, this has not been confirmed. A recently published meta-analysis comparing contact aspiration to stent-retriever thrombectomy on MCA-M2 occlusions reported a lower rate of sICH in the aspiration group (2.6%) compared to the stent-retriever group (5.7%) but without statistical significance (p = 0.18). 38 The recent development of the latest generation of large-bore catheters with improved trackability and better navigation requiring fewer manipulations may contribute to the favorable safety profile found in our study. These trends should be further assessed in a prospective randomized trial setting.
The definition of M2 is a critical aspect of any distal occlusion thrombectomy study. The PROMISE study core lab utilized a primarily anatomic definition. In routine practice, the definition of M2 can be more variable, and the operators commonly choose to define M2 as a vertical branch of M1 which originates entering the Sylvian Fissure and extends to its exit from this fissure. 39 In the PROMISE study, this resulted in some discrepancy between the site and the core lab reported occlusion locations (supplementary materials). Of the 161 subjects included here, sites reported 139 M1 and 22 M2 occlusions as compared with the core lab report of 124 M1 and 37 M2 occlusions. There were no significant differences in baseline characteristics, safety, or efficacy between the M2 and M1 groups except for history of angina/coronary artery disease (M2, 18% vs. M1, 5%; p = 0.047) when utilizing site assessment. When utilizing site reported occlusion location, in both univariable and multivariable analysis, occlusion location remained not predictive of 90 day mRS 0–2 (p = 0.37 and p = 0.51 respectively) and not predictive of successful revascularization (p = 0.58 and p = 0.66 respectively). In our study, utilization of site reported occlusion location did not result in any changes in conclusions for major outcomes (supplementary materials). However, the discrepancy between the core lab and site identified occlusion location highlights the fact that deliberate consideration of the location definitions is critically important when interpreting studies of this nature. CT/MR perfusion imaging was not collected in this study. It may be beneficial to include penumbral volume or ratio of ischemic tissue to infarct core as part of a future study. 40 Understanding the area of salvageable brain in distal occlusions may provide more information regarding benefit of revascularization therapy than anatomic clot location alone.
Strengths of the PROMISE study included imaging and adverse event evaluation by an Independent Core Laboratory and a Clinical Events Committee, and prospective consecutive enrollment of patients reflecting real-world clinical practice across Europe. The principal limitations, post hoc design, and lack of a randomized controlled comparison to a medical management arm should be taken into account when considering the conclusions of this study.
Summary
In this post hoc analysis of the PROMISE study, findings support frontline aspiration thrombectomy in the treatment of symptomatic patients with ischemic stroke from M2 MCA occlusion. In current practice, use of the ADAPT technique with large-bore ACE68/ACE64 catheters in M2 occlusions enabled comparable outcomes as in M1 occlusions. IV rt-PA should be used in M2 occlusions when indicated. Prospective M2-dedicated studies with aspiration thrombectomy are warranted to provide further clinical evidence.
Supplemental Material
INE894800 Supplemental Material - Supplemental material for ADAPT technique in ischemic stroke treatment of M2 middle cerebral artery occlusions in comparison to M1 occlusions: Post hoc analysis of the PROMISE study
Supplemental material, INE894800 Supplemental Material for ADAPT technique in ischemic stroke treatment of M2 middle cerebral artery occlusions in comparison to M1 occlusions: Post hoc analysis of the PROMISE study by Pedro Navia, Peter Schramm, Jens Fiehler and on behalf of the PROMISE Study Investigators in Interventional Neuroradiology
Footnotes
Acknowledgments
The authors thank Sophia S. Kuo, PhD, and Vincent K. Ho, MD, Penumbra, Inc., for their assistance during the manuscript preparation. They received salary support for this work.
Authors’ contributions
All authors made a substantial, direct, and intellectual contribution to the work.
Data sharing statement
Because of the sensitive nature of the data collected for this study, requests to access the dataset from qualified researchers trained in human subject confidentiality protocols may be sent to Penumbra, Inc. at promise@penumbrainc.com.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Navia reports being a consultant for Penumbra, Medtronic and Terumo and received research support from Penumbra. Professor Schramm reports being a consultant for Penumbra and Stryker and received research support from Penumbra, Philips and Siemens. Dr Fiehler reports being a consultant for Penumbra, Acandis, Boehringer Ingelheim, Cerenovus, Covidien, Medtronic, Microvention, Route92, Stryker, and received research support from the German Ministry of Science and Education (BMBF), German Ministry of Economy and Innovation (BMWi), German Research Foundation (DFG), European Union (EU), Hamburgische Investitions- und Förderbank (IFB), Medtronic, Microvention, Philips, and Stryker.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Penumbra, Inc. grant number [9508]. The corresponding author had full access to all the study data and had final responsibility for the decision to submit for publication.
Supplemental material
Supplemental material for this article is available online.
Role of the sponsor
Penumbra was involved in the conception, design, and conduct of the study; training of investigators; data monitoring including site visits; and was involved in drafting and revisions of the manuscript. The sponsor worked with stroke experts to design the trial, monitor, analyze, interpret, and present the data. The sponsor could not inhibit publication of the report even if the results were negative or detrimental to its products.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.