
Abstract
Background
In occupational therapy clinical practice there is often varied practice regarding thumb immobilization in a cast for nonsurgical management of nondisplaced or minimally displaced scaphoid fractures. The objective was to determine whether immobilization of the thumb in addition to the wrist for nonsurgical management of nondisplaced scaphoid fractures in adults is required to support good clinical outcomes including fracture union, hand function, wrist range of motion, pain, grip strength and scaphoid stability.
Methods
A systematic review of Embase, Medline, ProQuest, Scopus, Web of Science and a manual reference list search of retrieved studies was completed. Studies were included if participants were aged 16 years or older, received conservative treatment of the scaphoid fracture with immobilization, and evaluated the outcome measures of interest.
Results
Six articles were identified including four randomized control trials and two were one group pre-test-post-test crossover study designs, with methodological quality ranging from limited to strong. Limited evidence was found to support inclusion of the thumb in a cast for scaphoid management. Thumb inclusion did not promote better clinical outcomes regarding union rate and hand function. Thumb inclusion had no advantage over a no-thumb cast in relation to improving pain, grip strength, wrist range of movement and scaphoid stability.
Conclusion
Current evidence does not support immobilization of the thumb in addition to the wrist for nonsurgical management of nondisplaced scaphoid fractures by occupational therapists.
Introduction
The scaphoid is the most frequently injured carpal bone, accounting for approximately three quarters of all carpal fractures and two to seven percent of all fractures (Dennis et al., 2011; Garala et al., 2016; Rhemrev et al., 2011; Żyluk, 2023). Scaphoid fractures often occur due to falls in physically active males aged 25–35 years old and females over 40 years of age (Duckworth et al., 2012; Holloway et al., 2015; Swärd et al., 2019). Individuals who sustain a scaphoid fracture frequently experience pain and decreased range of motion in the upper limb (Hackney & Dodds, 2011).
Early detection of scaphoid fractures can be overlooked as diagnostic imaging of the fracture is subtle and initial symptoms are minimal (Kawamura & Chung, 2008). This increases the risk of nonunion occurring, which can result in scaphoid non-union advanced collapse, post-traumatic osteoarthritis or avascular necrosis (Alshryda et al., 2012; Berber et al., 2020). A decrease in upper limb function can negatively impact an individual’s physical, socioeconomic and psychological wellbeing (O’Hara et al., 2020). Early intervention by occupational therapists is required to support nonunion of the scaphoid fracture (Kawamura & Chung, 2008).
Conservative nonsurgical treatment immobilizing the upper limb has seen positive results in the management of minimally displaced or nondisplaced scaphoid fractures (Li et al., 2023; Modi et al., 2009; Żyluk, 2023). The type of cast or splints used varies based on the preference of the occupational therapist and medical team, as does the decision to immobilize the thumb. An immobilization time of approximately six to ten weeks is required for conservative treatment of nondisplaced or minimally displaced scaphoid fractures (Li et al., 2023; Sabbagh et al., 2019). Young, working and active adults are often non-compliant (Arora et al., 2007) with splint wearing regimes. As such there has been a shift to encourage more functional use of the hand in activities of daily living by removing the need for thumb immobilization in casting or splinting of scaphoid fractures.
The literature to date on the necessity of thumb immobilization in addition to wrist immobilization for nonsurgical management of nondisplaced scaphoid fractures in adults suggests that including the thumb in the cast does not significantly impact clinical outcomes (Deck et al., 2022; Li et al., 2023; Siotos et al., 2023; Żyluk, 2023). However, gaps remain in understanding the specific conditions under which thumb immobilization might be beneficial, such as in cases of proximal pole fractures or in patients with poor compliance. Additionally, the last systematic review search was completed in 2020 and included a pediatric population (Siotos et al., 2023), as such there is a need to review the literature to confirm these findings across diverse patient populations and fracture types to support occupational therapy practice. The objective was to determine whether immobilization of the thumb in addition to the wrist for nonsurgical management of nondisplaced scaphoid fractures in adults is required to support good clinical outcomes including fracture union, hand function, wrist range of motion, pain, grip strength and scaphoid stability.
Methods
Search strategy
This research adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guideline (Page et al., 2021). Studies included in this review were obtained through systematic searches of five electronic databases from their earliest available record (Embase from 1974, Medline from 1946, ProQuest from 1938, Scopus from 1970 and Web of Science from 1972) to March 2025. The main search terms were grouped into three main concepts. The first search concept included keywords such as “scaphoid” and “fracture”. The second concept included treatment modality of “non-surgical”, “nonoperative”, or “conservative”. The third concept included intervention keywords of “cast”, “brace”, “plaster”, “splint” or “orthoses”. All search terms were adjusted and truncated in order to match the database being searched. Searches were restricted to peer reviewed journal articles and articles in English language (see appendix). A manual search was conducted on all reference lists of retrieved studies. This review was registered with PROSPERO (CRD42021257031). Last search was completed in March 2025.
Inclusion and exclusion criteria
Studies were included if participants were aged 16 years and above (consistent with the age group treated at the authors local adult tertiary hospital) and if the intervention delivered to the participants included conservative treatment of a scaphoid fracture with immobilization of the upper limb using a cast, splint, orthosis or brace. Quantitative studies including randomized control trials (RCT), prospective and retrospective cohort and case-control studies were included in this review. Studies were excluded from this review if participants sustained an open or displaced fracture, had multi-trauma injuries, external fixtures or open reduction and internal fixation (ORIF). At least two authors independently reviewed all papers for inclusion. For the purpose of this review, the term ‘thumb cast’ will be used to describe a cast with immobilization of the thumb (wrist, forearm and thumb MCJ immobilization orthoses), and ‘no-thumb cast’ will be used to describe a cast without immobilization of the thumb (wrist and forearm immobilization orthoses).
Assessment of methodological quality
The quality of each study was independently assessed by at least two reviewers using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers developed by Kmet et al. (2004). The quantitative quality assessment consists of a 14-item checklist for assessing the quality of quantitative studies. The checklist scoring system provides a systematic, reproducible and quantitative means of assessing the quality of research encompassing a broad range of quantitative study designs (Kmet et al., 2004). Each item was scored on a scale from zero to two, where zero indicates that the criterion was not met, one indicates that it was partially met, and two indicates that it was fully met. The total score was then converted into a percentage. Any discrepancies were resolved through discussion between the authors. The quality of each study was described as strong (a score of above 80%), good (a score between 70 to 80%), adequate (with a score between 50 to 70%), or limited (a score below 50%) (Lee et al., 2008).
Data extraction and analysis
Data were independently extracted from each study using a piloted data extraction table by two authors and compared for accuracy. Data were extracted using the following headings: study design; study participants; intervention group; control group; outcome measures; results; methodological quality; and limitations. A narrative summary was completed to address six main outcomes including fracture union, hand function, wrist range of motion, pain, grip strength and scaphoid stability.
Results
Study selection process
Electronic searches found a total of 1014 articles using the key search terms (Figure 1). Sixty nine duplicate records were removed, and the remaining 945 articles were screened for eligibility based on their titles and abstracts. Nine hundred and one articles did not meet the inclusion criteria. Full text reviews were completed for the remaining 44 articles. Thirty eight articles were excluded for various reasons such as the age criteria being below 16 years old, article type was an information or commentary article, study design, type of intervention adopted (i.e. surgery) and fracture type (displaced fracture). Overall, six articles met the inclusion criteria and were included in this systematic review (Buijze et al., 2014; Clay et al., 1991; Hambidge et al., 1999; Karantana et al., 2006; Kawanishi et al., 2017; Schramm et al., 2008). PRISMA diagram depicting process of article selection.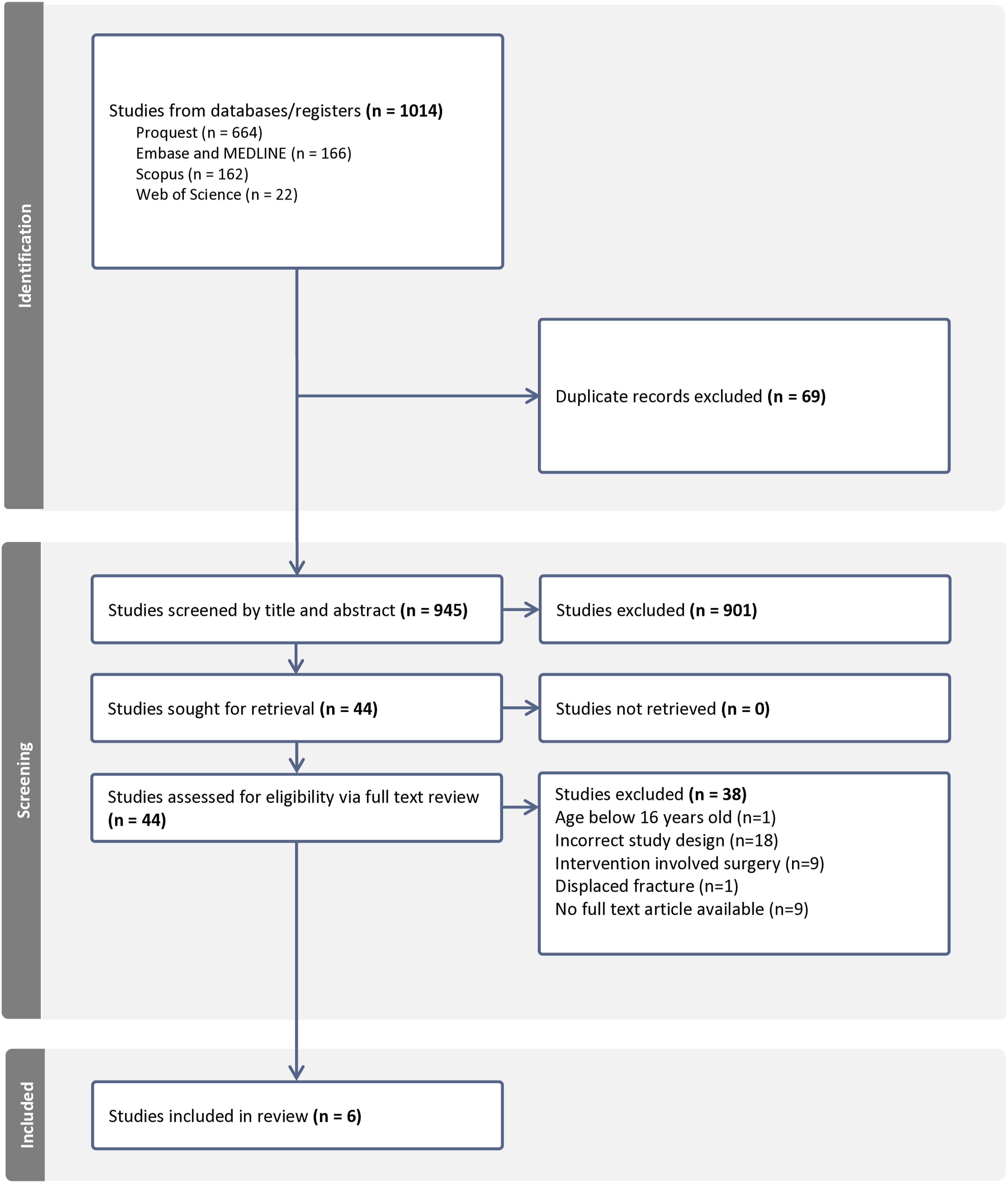
Characteristics of studies and study samples
Data extraction table of included studies.
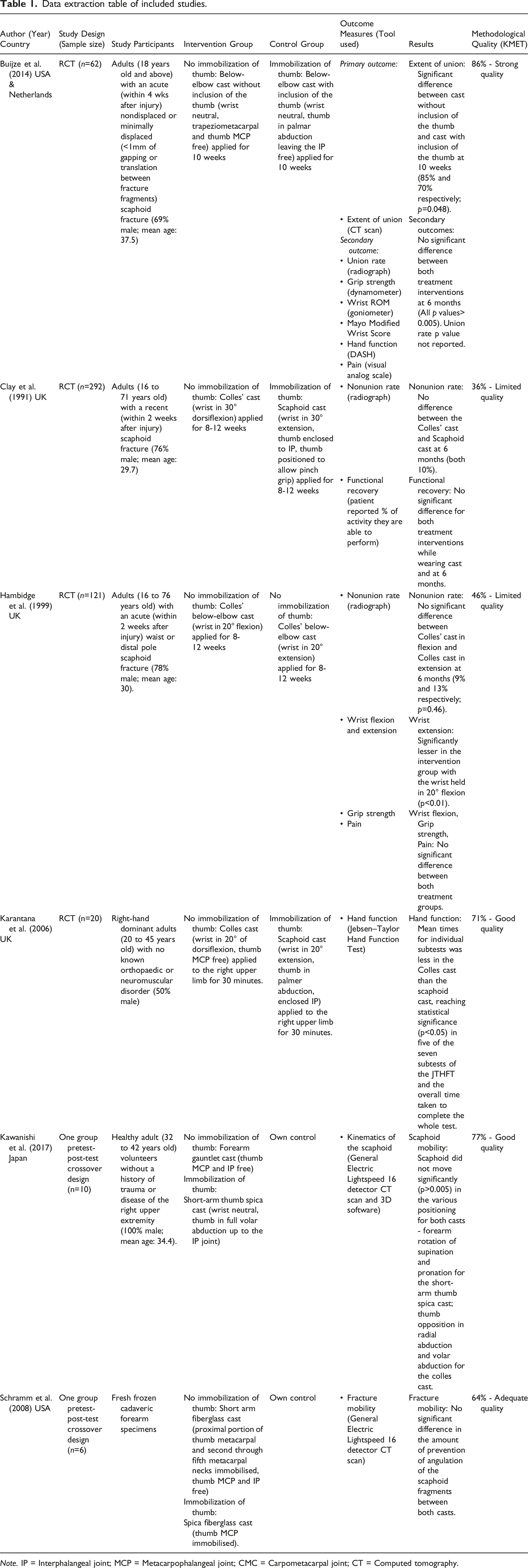
Note. IP = Interphalangeal joint; MCP = Metacarpophalangeal joint; CMC = Carpometacarpal joint; CT = Computed tomography.
The overall age of the study participants ranged from 16 years old to 76 years old (Buijze et al., 2014; Clay et al., 1991; Hambidge et al., 1999; Karantana et al., 2006; Kawanishi et al., 2017). The mean age of the majority of the studies (n = 4) ranged from 29.7 to 37.5 years old (Buijze et al., 2014; Clay et al., 1991; Hambidge et al., 1999; Kawanishi et al., 2017). Four studies had more male participants (at least 69% of study size) than females (Buijze et al., 2014; Clay et al., 1991; Hambidge et al., 1999; Kawanishi et al., 2017), with one study having an equal gender distribution (Karantana et al., 2006). No demographic information was provided for the cadaveric specimens (Schramm et al., 2008).
Methodological quality of included studies
The overall methodological quality of the six included articles ranged from strong to limited (Table 1, Appendix 2). Randomization and blinding of the study participants and investigators differed based on the nature of the study. Limitations of the high-quality studies included the power and effect size not sufficiently justified and lack of information describing method of subject and comparison group selection (Buijze et al., 2014; Karantana et al., 2006; Kawanishi et al., 2017). The limited quality studies had several limitations due to the lack of reporting of blinding of study participants and investigators as well as the study objective, subject characteristics, random allocation method, outcome measurement and results only being partially described (Clay et al., 1991; Hambidge et al., 1999).
Interventions
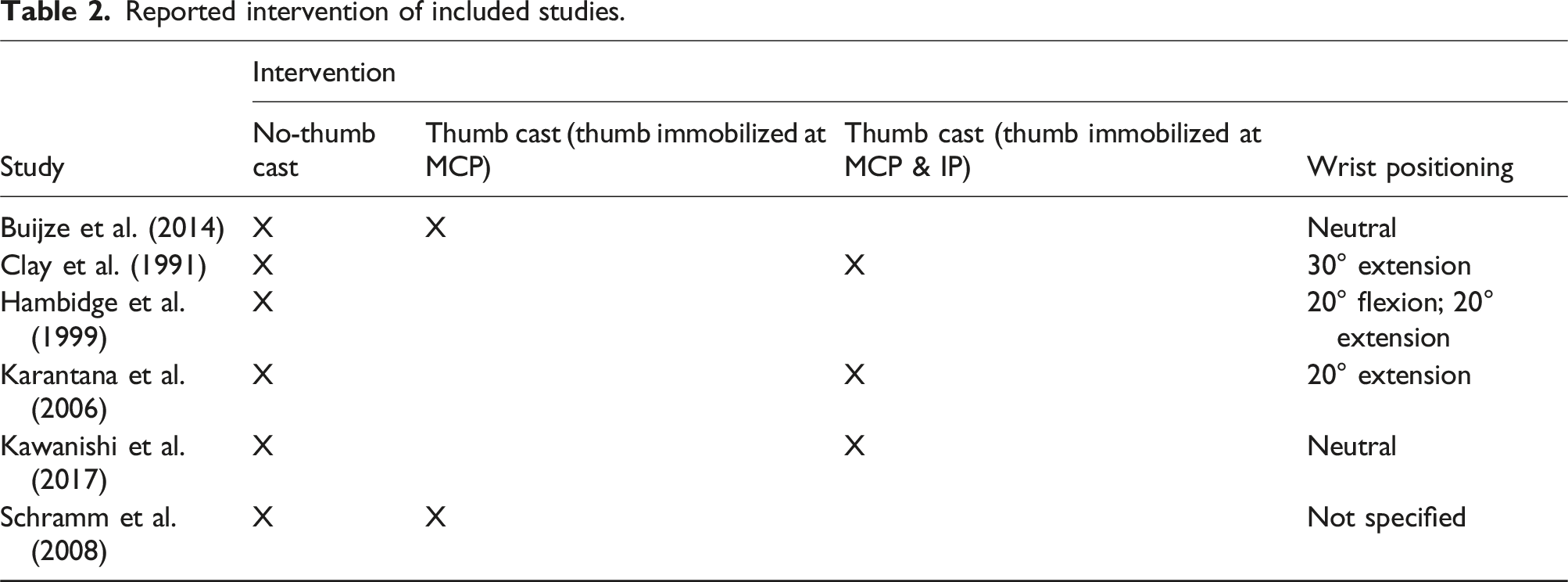
Reported intervention of included studies.
Outcome measures
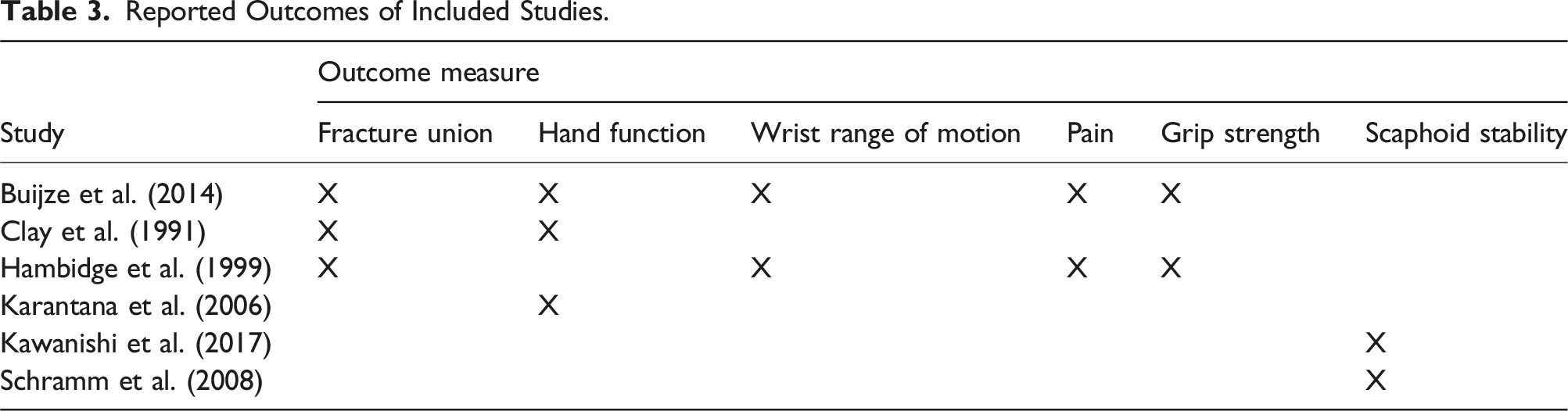
Reported Outcomes of Included Studies.
Fracture union
All three studies evaluating the union of minimally displaced or nondisplaced scaphoid fractures using a CT scan (Buijze et al., 2014) or radiography (Clay et al., 1991; Hambidge et al., 1999) indicated no significant differences between the intervention and control groups post intervention (Buijze et al., 2014; Clay et al., 1991; Hambidge et al., 1999). Two studies comparing the union rate of a thumb cast and no-thumb cast claimed there were no significant differences between both groups; however, both articles did not provide the estimate of variance values (Buijze et al., 2014; Clay et al., 1991). Hambidge et al. (1999) compared the no-thumb cast in either 20o flexion or extension reported the incidence of non-union was not influenced by positioning of wrist in immobilization with a p-value of 0.46. In another study, at 10 weeks, the no-thumb cast group showed significant improvement (p = .048) in the extent of union on CT (Buijze et al., 2014). Subgroup analysis was available for scaphoid waist fractures only, which makes up 90% of the no-thumb cast group, and 87% of the thumb cast group. No significant difference (p = .099) in extent of union at 10 weeks between both groups was found (Buijze et al., 2014).
Hand function
Despite using a variety of outcome measures, all but one of the three articles that evaluated hand function reported no significant difference between the two groups (Buijze et al., 2014; Clay et al., 1991). No difference in hand function was also found using subjective self-reported outcome measures. This included client reported evaluation of performance, measured in percentage of activities they could perform (Clay et al., 1991), and the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire with a p-value of 0.84 (Buijze et al., 2014). Clay et al. (1991) reported there was minimal difference in the client’s ability to complete activities of daily living (dressing, washing, and eating) regardless of the type of cast used. At six months post intervention, a therapist based scoring system of hand function using the Mayo Modified Wrist Score, which assesses pain, wrist flexion and extension, grip strength, and ability to return to regular employment and activities, also showed no significance difference (p = .20) between both groups (Buijze et al., 2014).
In contrast, Karantana et al. (2006) reported a significant difference (p < .05) in fine and gross motor hand function between both groups using the Jebsen–Taylor Hand Function Test (JHFT), with the Colles cast group having faster times recorded in the subtests and overall test timing. The study reported that the mean time taken to complete five of the seven subtests in the JHFT comparing results from the Scaphoid cast to the Colles cast were statistically significant (p-value ranging from 0.001 to 0.040), in activities that involved the use of a pinch grip function and fine co-ordination of pinch such as simulated page turning and stacking of counters (Karantana et al., 2006).
Wrist range of motion (ROM)
Two studies assessed the impact of cast immobilization (thumb enclosure or wrist position) on wrist ROM at six months post intervention (Buijze et al., 2014; Hambidge et al., 1999). Buijze et al. (2014) reported no significant differences in wrist ROM measured using a goniometer for wrist extension (p = .810), wrist flexion (p = .130), ulnar deviation (p = .026) and radial deviation (p = .600) between the thumb cast and no-thumb cast groups. Similarly, Hambidge et al. (1999) reported wrist positioning to have no influence on wrist flexion, though the outcome measure tool used and estimate of variance values were not provided. Conversely, Hambidge et al. (1999) reported wrist extension being significantly reduced (p < .01) when the wrist is held in 20° flexion compared to when the wrist is held in 20° extension suggesting wrist positioning can influence wrist extension six months post intervention.
Pain and grip strength
Two studies conducted by Hambidge et al. (1999) and Buijze et al. (2014) evaluated pain and grip strength as an outcome measure at six months, and both reported no significant differences between groups. Pain levels measured using the visual analogue scale (p = .530) (Buijze et al., 2014) or patient reported pain intensity of no pain, mild, moderate or severe (Hambidge et al., 1999) showed the type of cast used had no influence on pain. Additionally, grip strength measured using a dynamometer also showed no significant differences (p = .950) between the two treatment groups (Buijze et al., 2014). Hambidge et al. (1999) described similar findings, stating grip strength was not influenced by position of wrist immobilization.
Scaphoid stability
Angulation, translation and movement of the scaphoid did not differ significantly (p > .05) regardless of whether the thumb was immobilized in the cast (Kawanishi et al., 2017; Schramm et al., 2008). Both articles which assessed mobility of the scaphoid using the General Electric Lightspeed 16 detector CT scan when the upper extremity was positioned whilst in a thumb cast or no-thumb cast supported this finding of thumb and wrist motion not having a significant impact on scaphoid stability (Kawanishi et al., 2017; Schramm et al., 2008).
Discussion
Six articles were included in this systematic review which found some evidence, though limited, to suggest that immobilization of the thumb for nondisplaced or minimally displaced scaphoid fractures is not required for good clinical outcomes including fracture union, hand function, wrist range of motion, pain, grip strength and scaphoid stability. This review found evidence to suggest that the use of a no-thumb cast for stable scaphoid fractures promotes better clinical outcomes in relation to hand function and does not impact on union rates, when compared to use of a thumb cast. Our findings align with previous reviews (Deck et al., 2022; Li et al., 2023; Siotos et al., 2023; Żyluk, 2023) overall indicating that no-thumb casts do not impact fracture healing rates, long-term range of movement, strength or pain. Subgroup analysis of scaphoid waist fractures also showed no significant difference in the extent of union at 10 weeks via CT scan in one study (Buijze et al., 2014). Additionally patients wearing thumb casts had more functional limitations than patients who were able to use their thumb while casted (Deck et al., 2022).
Findings of this review also revealed that subjective patient reported outcome measures of hand function while wearing the cast found no significant difference between thumb cast and no-thumb cast groups. This finding remained consistent at six months post intervention as well. However, objective standardized assessment of hand function using the JHFT conducted while the clients were in the cast stated otherwise. A study investigating the functional outcomes of thumb immobilization in healthy volunteers using a patient reported outcome measurement information system and a typing assessment reported significant differences between the two groups in both outcome measures (Muppavarapu et al., 2017). Muppavarapu et al. (2017) supported the findings for the objective assessment but contested the result for the patient related outcome measures. These findings provide evidence to support the use of a no-thumb cast in stable scaphoid fractures, promoting better hand function. Increased function may also support patient compliance with the splint wear regime.
Overall, the use of a thumb cast has shown similar or worse clinical outcomes when compared to a no-thumb cast, which is indicative that immobilization of the thumb offers limited advantage which is consistent with the findings in previous reviews (Li et al., 2023; Modi et al., 2009; Siotos et al., 2023; Żyluk, 2023). This suggests that adoption of a no-thumb cast may be more effective. No joint should be immobilised unnecessarily as immobilization of any joint that is not injured can result in an increase in morbidity and stiffness (Mawdsley & Harrison, 2018). As a stable scaphoid fracture requires six to eight weeks of immobilization to heal completely (Żyluk, 2023), casting can lead to considerable economic impact in terms of time off work and lost productivity (Davis et al., 2006). Employing the use of a less cumbersome cast without the thumb immobilized, may be more appealing to clients, promote better functional capabilities of the individual and enhance their occupational performance (Buijze et al., 2014).
There is limited evidence to arrive at a definite conclusion that the thumb cast has no advantage over no-thumb cast in producing better outcome results in relation to pain, grip strength, wrist ROM and scaphoid stability for treatment of stable scaphoid fractures. The findings from this review are consistent with results from a previous systematic review and meta-analysis which showed no significant differences between the nonoperative treatment modalities for acute scaphoid fractures in regards to pain, grip strength, and range of motion (Doornberg et al., 2011). Both studies evaluating scaphoid stability were congruent in showing immobilization of the thumb at the MCP joint does not contribute to scaphoid stability.
Strengths and limitations
There was substantial heterogeneity between studies impacting on comparison, as participants varied significantly from healthy participants, to participants with a scaphoid fracture, to cadaveric specimens. The search results produced articles from the United Kingdom, or the United States of America, with only one study from Japan. This could result in biased estimates of effect and reduce generalizability (Jackson & Kuriyama, 2019). Next, the methodological quality assessment showed two of the six articles included had limited quality (Clay et al., 1991; Hambidge et al., 1999), highlighting the need for better robust methodologies in this area of research. There was also inconsistency with nomenclature used to describe orthoses impacting on comparison. Finally, the outcome measures were disparate across studies, and the lack of consensus in union rate definition, varying casting regimes coupled with the differing protocols used when applying the cast acted as a limitation to comparing results.
Conclusions
Overall, this systematic literature review highlights that there is limited evidence supporting immobilization of the thumb in addition to the wrist for nonsurgical management of nondisplaced scaphoid fractures. Current evidence suggests that immobilization of the thumb offers limited advantage and is not necessary to support good clinical outcomes. This research can support occupational therapists to advocate for patients and provide a cast that enhances their function and occupational performance, without impacting on fracture healing.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.