
Abstract
Introduction
Transition of senior adults from community into nursing homes (NH) is a challenging event for both the senior adults and their family. Even with the introduction of new service models, studies continued to advocate that the navigation of services should remain simple and streamlined. In relation to the ‘wicked problem’ that persist, design thinking methodology and tools can be adopted to address the unacceptably huge gap between the services that NH operators aim to deliver and the actual service that is delivered. The study aims to understand the experience of senior adults transitioning into NH from the design thinking approach.
Methods
A phenomenological research design was used with 10 senior adults recruited. The protocol consisted of three 8-h sessions, in-depth observations of the participants in an NH environment and a 45-min semi-structured interview with the participants to understand their experience of transition into a NH.
Results
Four distinct phases were unravelled to illustrate the transition process. Four personas were also created to represent the types of senior adults who are likely to transition into a NH. Main factors that influence the experience of transition include (1) emotions of the senior adults, (2) support provided during the transition, and (3) frequency of visitation by others.
Conclusion
The study validated the complexity of transition into a NH. Using the design thinking methodology and tools, such as interviewing with empathy and the creation of personas, findings can be used to develop a service model that addresses the challenges of seniors’ transition into a NH.
Introduction
The transition of senior adults from the community into nursing homes has been reported as a challenging event for both the seniors and their family members (Crawford et al., 2015; Johnson & Bibbo, 2014; Ramanathan & Fisher, 2016). While this process may unfold over months or even years before the actual move (Kokonya, 2018), senior adults are often given very little time to fully prepare for the transition, resulting in additional emotional and logistical challenges. From literature, issues (e.g., communication with senior adults on the transition) that eventually lead to a poorer transition into an NH typically arise after an admission into a hospital (Kokonya, 2018; Sun et al., 2021). In practice, it is also observable that many senior adults are often deeply satisfied with the independence and familiarity of community living, and may avoid considering a transition into a nursing home until a hospital admission makes it necessary.
Once admitted, the demands of the administrative steps to obtain a spot in a NH often take priority over the immediate needs of elderly individuals (such as losing their work-related roles) prior to their transition into the NH. These unmet needs may have a direct impact on the continuity of roles and activities valued by these senior adults, and subsequently ripple into a lower quality of life in the NH even after the transition period (Causey-Upton, 2015; Kokonya, 2018; Sun et al., 2021).
In the Asian context, for example in Singapore, most studies had focused on the issues of senior adults residing in NH but little has been done on the process of transition into a NH (Ang et al., 2006; Toh et al., 2017; Yap et al., 2003). Pertaining to the adjustment process for entering NH, research has predominantly focused on caregiver experiences, with minimal exploration of the perspective of elderly residents themselves, as far as is known (Ramanathan & Fisher, 2016).
The lack of understanding beyond the biomedical perspective of the senior adults had undermine the emotions of the person transitioning into the NH, especially so in an Asian context where senior adults are more likely to value family ties and desire to be living with their loved ones. The knowledge gap will also have a direct impact on continuity of roles and activities that is unique to the senior adults during and even after the transition.
Specifically, it is important for researchers to adopt a human-centric approach to empathise strongly with the pain points experienced by these senior adults throughout the transition process; and derive solutions to reconstruct the process experienced by them during the transition into a NH. In the paper, NH is referred to as a residential institution that provides care to senior adults who require nursing care for 24-hours a day, and unlike aged homes where senior adults are mostly independent in self-care.
Given the strong emphasis in the concept of human-centricity, design thinking is a useful approach to provide researchers with the framework to incorporate users’ feedback throughout the development process (Altman et al., 2018; Lewrick et al., 2020); thus suggesting it as a plausible approach to create a service model to transition senior adults into a NH (Berry, 2020; Roberts et al., 2018). To improve the experience of senior adults transitioning into NH, design thinking can solve complex issues that arose during the transition through an iterative process (Altman et al., 2018; Berry, 2020; Wolcott et al., 2020).
Deepening empathy refers to the understanding of feelings and experiences of the senior adults. It involves ‘putting self in their shoes’ to gain a deep understanding of their needs, desires, and challenges in the transition process. By creating personas, the design thinking process can ensure that solutions are tailored to the specific experiences and perspectives of those affected by the transition, ultimately leading to more effective and supportive care models.
At this phase of the research development, it is crucial to view the process of deepening empathy for senior adults transitioning into NH as an indispensable step to recreate the experience of transition into NH from a design thinking perspective. Therefore, in addressing the gap, the study aims to: [1] understand the lived experience of senior adults transitioning from community into NH, and [2] develop strategies to deepen empathy for these senior adults throughout the transition process using principles of design thinking.
Materials & methods
Methods
The study used a phenomenological research design through [1] an observation of ten participants using the AEIOU framework of design thinking (Lewrick et al., 2020), and [2] a 45-min semi-structured interview with the participants to understand their experience of transition into a NH (Creswell et al., 2007; Creswell & Poth, 2016). The study protocol was approved by the Institutional Review Board of Singapore Institute of Technology (SIT-IRB Project number: 2021025).
Recruitment of research participants
Potential participants were identified from three NHs in Singapore that had agreed for the study to be conducted under their premises. Convenience sampling was used over a three-month period to recruit eligible participants from these three NHs. These NHs operated as not-for-profit entities, with about 20% of their staff consisting of trained professionals like doctors, registered nurses, and allied health professionals. The residents received care within a community living setting, with volunteers interacting with them for roughly three business days each week.
Senior adults were recruited if they: [1] are at least 60 years and above, [2] had been admitted into the NH as long term care residents for 3 months or less, [3] have a minimum score of 18 out of 30 for Mini-Mental State Examination (Johnson & Bibbo, 2014; Meyer et al., 2019), and [4] are able to converse verbally either in English, Mandarin, or one of the main local dialects (e.g., Hokkien, Cantonese). Senior adults were excluded if they were admitted into the NH for: [1] respite care, [2] palliative care, or [3] under dangerously ill list (certified DIL).
According to a report on world population by the United Nations (2019), it is recommended to define senior adults as those aged 60 or 65 years and over for easy tracking of the ageing population. In this study, the inclusion for senior adults was decided at 60 years with reference from the recommendations from the United Nations and also with reference from local studies that studied senior adults in the context of a nursing home (Yap et al., 2003; Guna et al., 2022). Additionally, the cut off score of minimum 18 out of 30 for MMSE was decided as the inclusion criteria to ensure the cognitive functioning of the senior adults for the outcome measurements conducted. The minimum score was also adopted in other studies that have conducted interviews with senior adults residing in a nursing home (Johnson & Bibbo, 2014; Meyer et al., 2019).
Eligible senior adults were identified and referred to the principal investigator by the social workers of the NHs. Next, the principal investigator confirmed the eligibility of the senior adults referred before obtaining their informed consent for the study.
Over the three-month period, 10 out of 34 senior adults moving from community settings to NHs were recruited (Figure 1). Participant recruitment.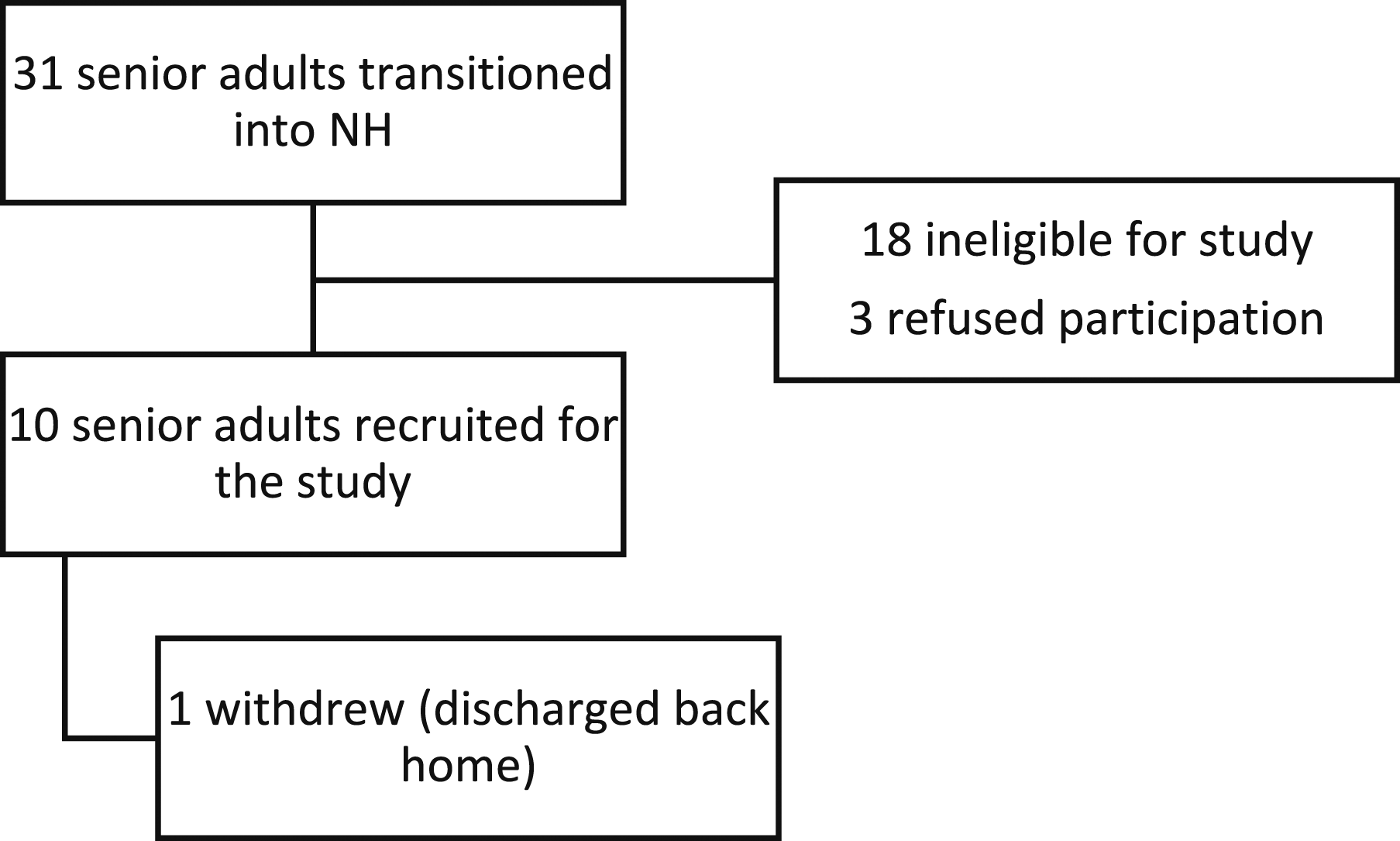
Data collection
All data (i.e., observations, interviews) were collected by the principal investigator, who is a male doctoral candidate and with more than ten years of clinical practice as an occupational therapist in NH practice. The participants only knew the principal investigator as a clinician conducting the study and had no prior established relationship before the data collection.
Observations of the participants were conducted for 24-h (i.e., 16-hour during a weekend and 8-h during a weekday) to deepen empathy for them as residents in a NH. To achieve a broad range of observation times, the 8-h weekday session was scheduled between 8:30 am to 4:30 pm when most staff working regular office hours were present. Conversely, the 16-h weekend session took place from 4 am to 10 pm, a time frame when most office-hour staff were absent, providing insight into how senior adults occupy their time during weekends.
AEIOU observation framework.
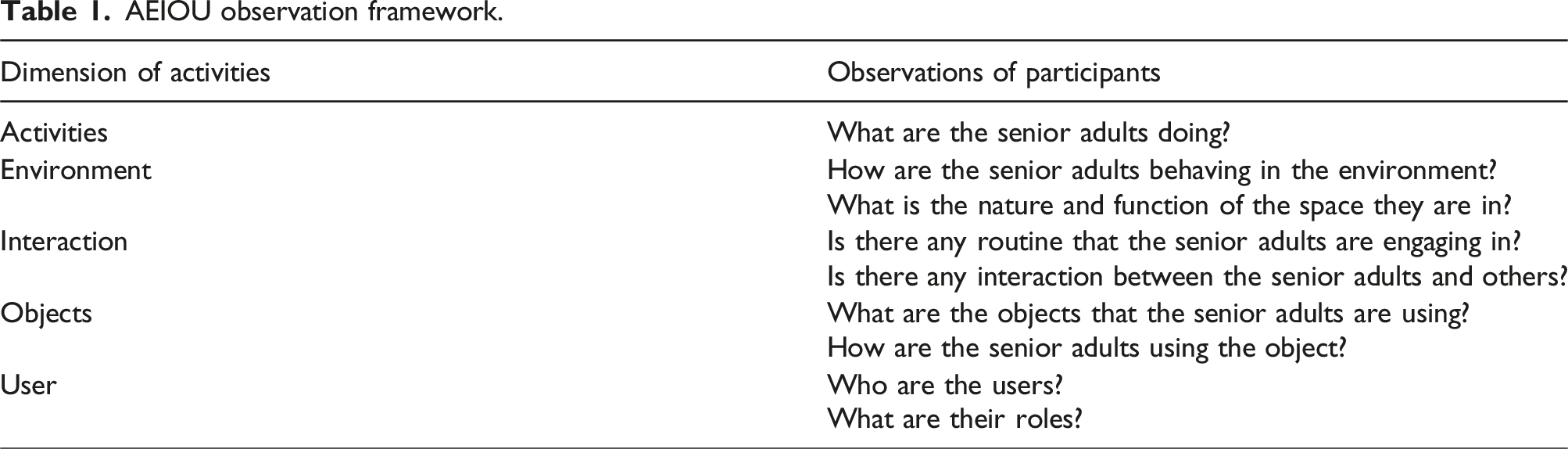
Observations took place at a corner using the established framework, ensuring not to disrupt the NH team’s workflow or the activities of the participants. The framework was used as entry point to capture all events involving the participants in the NH environment. To mitigate any potential participant-observer bias, all interpretations made during the observations were verified with the participants before analysis. A needs statement was formed with a problem statement and specific challenge for the observation before data analysis commenced.
A 45-min semi-structured interview was also conducted individually with the participants by the principal investigator to understand their experience of transitioning into a NH. The interviews were conducted in a conducive, quiet environment at their respective NH. All interviews were audio-taped and transcribed verbatim. The interviews were also videoed and referenced on the non-verbal expressions of the participants during the interview. In addition, field notes were also taken based on the principal investigator’s impression of the experience illustrated by the participants. All information interpreted from the interview were verified with the participants before analysis.
The interview questions were adapted from another study (Lee, 2001) of similar cultural context as the current study. Examples of questions asked during the interview were “could you share more about your involvement when the decision was made for you to transition into a NH?”, “how did you prepare yourself mentally or physically for the move?”.
Data was collected until data saturation, and that no further new information was gathered about the lived experience of senior adults through the transition process.
Data analysis
All data were analysed through thematic analysis (Braun & Clarke, 2012).
The transcripts were read and interpreted individually by the principal investigator to be familiar with the participants’ experience of transitioning into a NH. Sections that might be of potential interest to reflect the experience of senior adults transitioning into NH were then highlighted for thematic coding.
Next, thematic coding of the transcripts was done systematically using Microsoft Excel; with phrases used to describe data that potentially illustrate the experience of senior adults transitioning into NH. Salient themes were identified before searching for common themes that best describes the current lived experience of senior adults transitioning into NH.
From the observations and thematic analysis, personas were created based on the actual data collected from the participants; thus adding the human touch to what would largely remain as cold facts of the lived experiences of senior adults transitioning into NH. Specifically, ‘engaging personas’ were created, which examined the emotions of the users, their psychology, backgrounds and make them relevant to the task at hand. Creating persona profiles are important in this research to enable the understanding of patterns and synthesizes the type of senior adults transitioning into a NH (Chasanidou et al., 2015).
A key element in this process is the development of personas, detailed representations of the senior adults. These personas help deepen empathy by allowing researchers and design practitioners to better understand the unique needs, motivations, and challenges faced by the senior adults through the transition process.
Results
Deepening empathy for senior adults transitioning into nursing homes
From the thematic findings, it was found that senior adults are most likely to experience four distinct phases during their transition into a NH (Figure 2). Phases in transition process. Legend: T-2 = Before admission to the hospital; T-1 = Admission into the hospital; T0 = Initial transition into the nursing home; T6 = Beyond 3-month post admission into the nursing home.
Pre-transition Phase (T-2, Before admission to hospital)
Factors that influence the experience of transition into a nursing home.
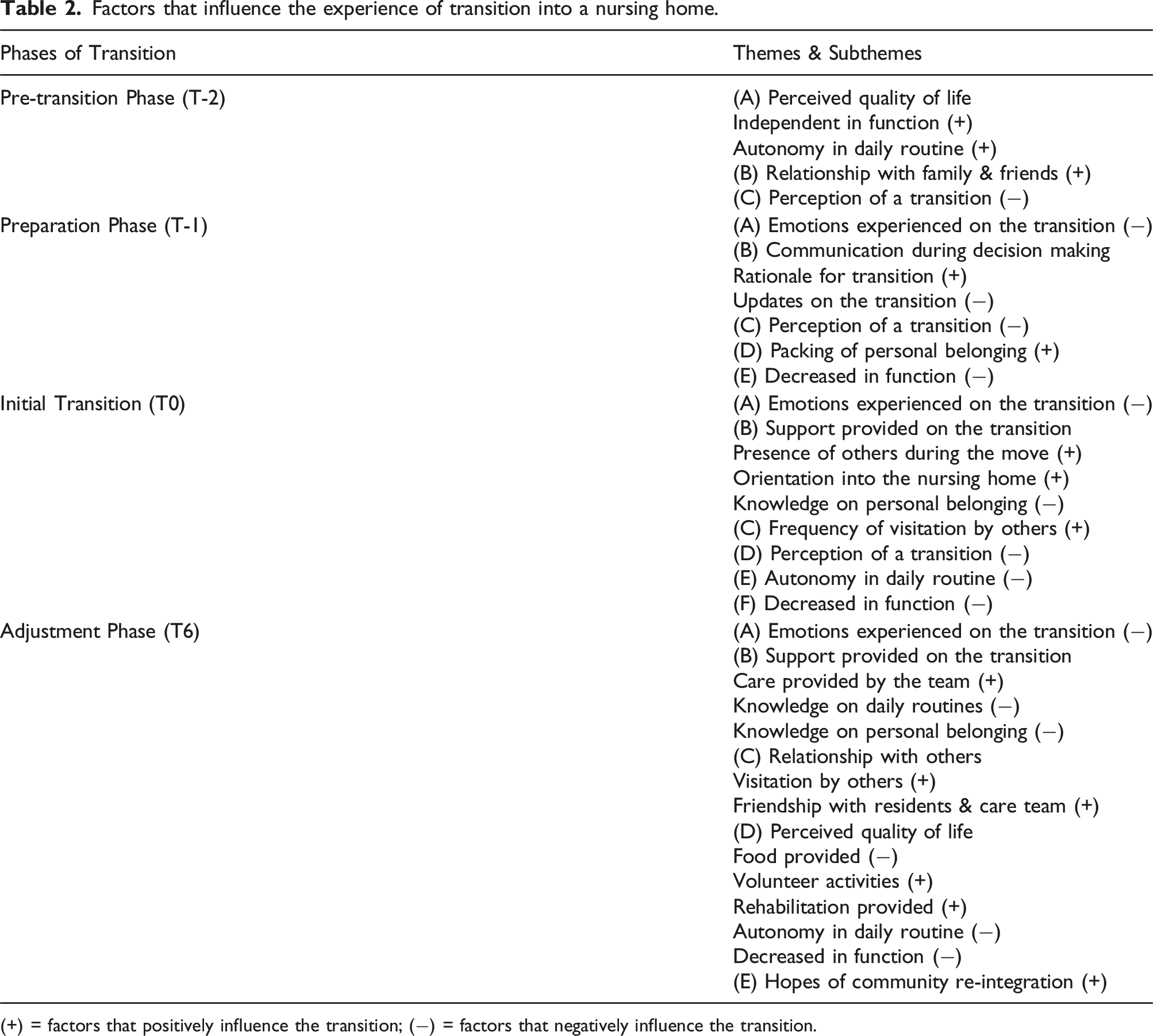
(+) = factors that positively influence the transition; (−) = factors that negatively influence the transition.
“P01: I cannot shower myself and there is no one to care for me. That’s why they sent me to a nursing home. (Translated).”
However, their acceptance of a transition into a NH still varied based on their social circumstances.
The findings also revealed important factors that can possibly influence the experience of senior adults transitioning into a NH (Table 2).
Preparation Phase (T-1, During admission in the hospital)
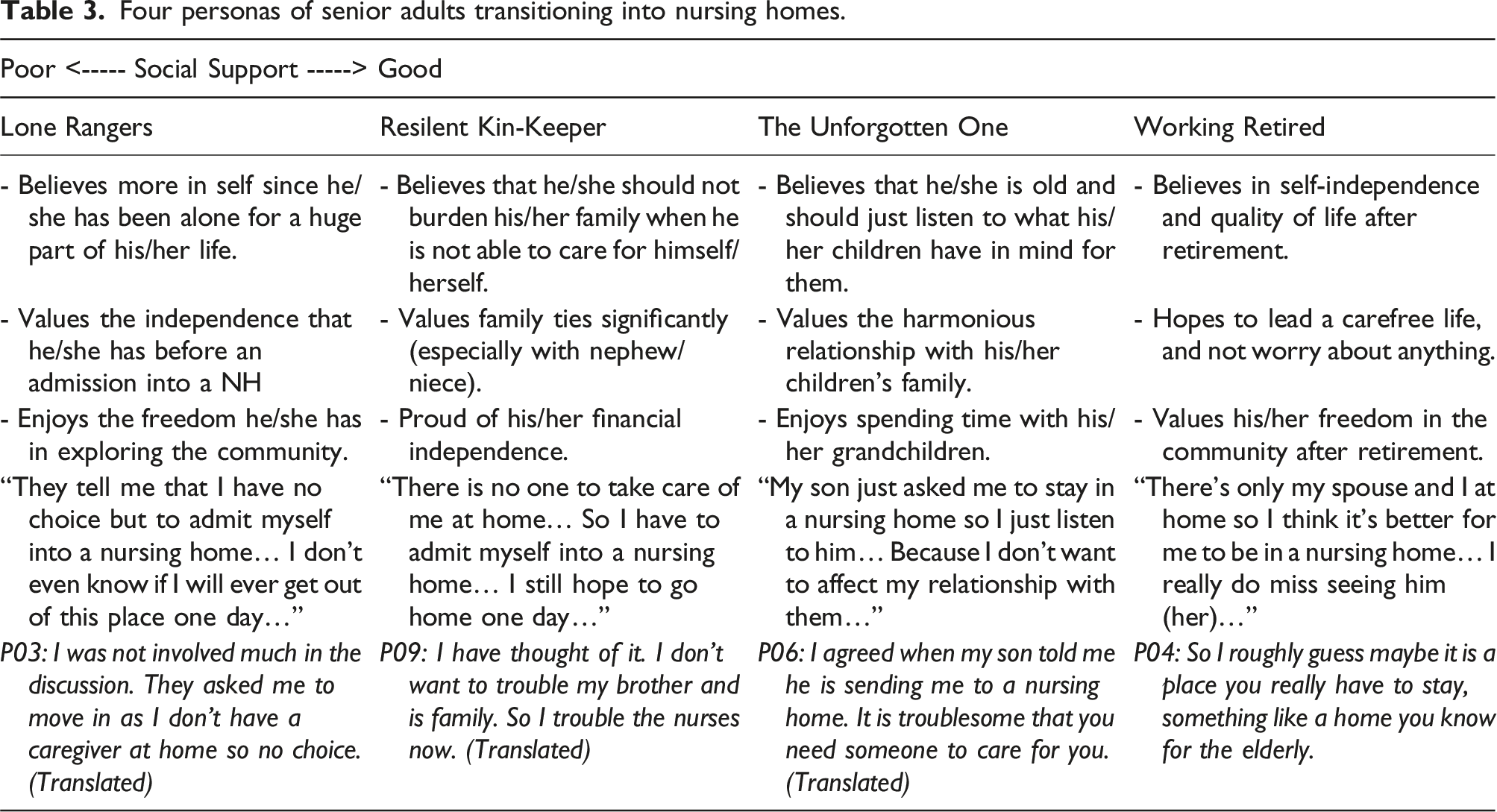
Four personas of senior adults transitioning into nursing homes.
“P07: I don’t know where I could go. I wanted to home but I can’t, so I stayed here (Translated).”
In addition, the administrative requirements of an admission into a NH often also superseded the emotional and biopsychosocial needs of the senior adults during the transition process.
Initial Transition (T0, First month of transition into the nursing home)
From the findings, six themes were identified as factors that will influence the experience of transition at T0 and possibly the quality of life perceived by the senior adults even after the transition (Table 2). At this phase, senior adults struggled with the challenges of living in a new environment while coping with the emotions that were unaddressed before the admission into the NH.
However, it was also reported that the efforts made by the NH team did facilitate a more positive experience throughout the transition process.
“P05: I feel good because there are nurses to take care of me.”
Adjustment phase (T6, Sixth month of transition into the nursing home)
At T6, five themes that influence the experience of transition were identified (Table 2). The phase is approximately six-month post-admission into the NH, and is also a turning point where senior adults gradually accept their transition into the NH.
“P08: No difference after a while, I don’t feel much difficulties in the nursing home. (Translated)”
At this phase, the senior adults had developed a perception of their transition as they formed their own identity as a resident in the NH.
Personas of senior adults transitioning into nursing homes
From the experiences of the participants, it was found that there were generally four types of senior adults transitioned into NH in an Asian context (Table 3).
The lone rangers
From the findings, the Long Rangers were senior adults who did not receive formal education and supported themselves as blue collar workers. They were mostly singles and did not have much contacts with their relatives. Lone Rangers agreed for the transition as there was no one to care for them in the community. After the transition, they typically spend most of their time on electronic devices. Lone Rangers tend to feel helpless in a NH as they did not understand who to seek help from in the NH.
The resilient Kin-keepers
Similar to Lone Rangers, the Resilient Kin-keepers were senior adults who did not have formal education and were blue collar workers. They were mostly singles or divorcees however had been living with their extended family before the transition. Different from Lone Rangers, Resilient Kin-keepers agreed for the transition as they did not want to burden their family for their care needs. After the transition, Resilient Kin-keepers spent most of their time in bed and only look forward to visitations by their family members. They would prefer to have more activities where they could participate in and have a more enriching lived experience in the NH.
The unforgotten ones
Similarly, the Unforgotten Ones were senior adults who did not have formal education and were blue collar workers. As different, they were mostly widowed and had been living with their children’s family before the transition. The Unforgotten Ones agreed for the transition as they felt obliged to follow the plans their children had planned for them. After the transition, the Unforgotten Ones felt helpless when there was no one around to help them with their daily needs. They also feel upset about not being able to engage in their previous roles in the community.
The working retired
Last but not least, the Working Retired were senior adults who had received a higher level of education (e.g., secondary school and above) and were working as white-collar workers. They were mostly married with or without children and were living alone with their spouse before the transition. They agreed for the transition to a NH as they believed that the NH will eventually be their destination before they pass on. After the transition, they spent most of their time engaging in activities available in the NH. They are only slightly concerned with the level of freedom given in a NH.
Discussion
The study sought to understand the current lived experience of senior adults transitioning into NH using principles of design thinking and establish the meaning of transition from the perspective of these senior adults. The findings of the study revealed four personas of senior adults who are likely to admit into a NH, and four distinct phases that they are likely to experience during their transition into a NH.
Phases experienced by the senior adults during the transition process
From the study, it was found that senior adults experienced emotional fluctuation throughout the transition process. The complexity of these emotions was also discussed by Ellis (2010) who identified nine stages of transition based on the concepts of transition developed by Fisher (1999, 2000). In the study, four phases were identified to distinctively illustrate the fluctuations experienced by these senior adults during the transition process. The finding is also consistent with a meta-analysis reported by Sun and colleagues (2021) that senior adults will undergo four phases during their transition into NH, and experience fluctuation in their emotions throughout the transition process as they adapt to the NH environment.
Pertaining to factors that influence the experience of transition, it was revealed that the pain points determining a successful transition typically begin from the point of admission into the hospital. Pain points such as the lack of communication during the decision-making process, and the lack of information about the NH as identified by the participants were also reported by studies conducted in other cultural context (Johnson & Bibbo, 2014; Lim et al., 2022; Ramanathan & Fisher, 2016). Hence, it can be learnt that the issues of transition are person-centric and might not be culturally dependent to a certain extent.
Factors influencing the experience of transition into nursing homes
In the study, factors that influence the experience of transition into NH were also uncovered at each phase. Unsurprisingly, the fluctuating emotions experienced by senior adults are one of the key factors that influence their experience during the transition into NH. Besides that, it can be learnt that issues of institutionalisation in NH is a major barrier of transition stemming from the point of admission to even after the transition into the NH.
The findings also confirmed that factors influencing the experience of transition is multifaceted and needs to be considered from a multidimensional perspective. Similarly, Schenk and colleagues (2013) had also reported that similar observations issues relating to quality of life extend far beyond a biomedical perspective. Specifically, under the theme on quality of life, autonomy was a key factor identified that had influenced the experience of senior adults transitioning into NH. The finding was also confirmed by Wang and colleagues (2016) that autonomy in NH has a negative association with depression and dependence on staff after their transition into NH. Therefore, the findings suggested that addressing issues of transition into NH can plausibly mitigate existing issues experienced by senior adults residing in NH.
Characteristics of senior adults transitioning into nursing homes
Unique to this study, insights on the type of senior adults transitioning into NH were presented from the perspective of a person, in comparison to previous studies conducted where the authors only described residents in a NH from a biomedical and functional perspective (Ang et al., 2006; Kamun & Lim, 2005; Yap et al., 2003). This approach exemplifies the use of design thinking in a nursing home setting and how it can potentially mitigate the long-standing issues that continue to persist during a transition into NH.
From the study, four personas were constructed to collate the distinct characteristics of senior adults transitioning into NH. The personas reflect a spectrum of senior adults with varying level of social support before their admission into a NH. For example, senior adults who are not educated and/or does not any family support are more likely to have a poorer experience of transitioning into NH in relative to their counterparts who are more educated and/or have a preconceived mind-set of an eventual admission into a NH. However, it is also suggested that the characteristics and journey of senior adults transitioning into NH can be unique to the cultural context of the study (i.e., Singapore).
Implications for practice
In contrast to studies that categories senior adults from a biomedical perspective, the study presented new evidence on the needs and desires of senior adults during the transition using principles of design thinking. Clinicians can utilise the findings to develop a transition plan for these senior adults during their transition into a NH.
Other than that, the study also confirmed that senior adults experienced a lower quality of life after the transition as compared to their perceived quality of life while in the community. Although a better transition will inevitably improve their perceived quality of life in the NH after the transition, it is still debatable if the senior adults had eventually accepted or ‘resigned’ to the fate of transitioning into a NH.
Nevertheless, clinicians can still use the findings and find innovative ways to emotionally support and transition the senior adults into the NH; thus encouraging a higher quality of life even after the transition period.
Limitation & future studies
In the study, the experiences of the participants were narrated retrospectively. Hence, the experience reported might be influenced by their perception of residing in the NH. Besides that, only senior adults with good cognition were recruited for the study. Therefore, the generalisability of the data to senior adults who have cognitive impairment or are non-verbal has to be handled with care.
Given that the study adopted the design thinking methodology and tools to uncover bigger and better opportunities for senior adults transitioning into NH, further studies are warranted to experiment and validate the data with other stakeholders (e.g., care team) in the NH.
Conclusion
Transition of senior adults into NH has been acknowledged as a complex process. In this study, design thinking was applied in the research to unravel the complexity of the transition process from the senior adults’ perspective. Through the process, it also confirmed that facilitating a positive transition at the initial phase of transition will significantly create a positive impact on the senior adults’ quality of life even after the transition period. With the current understanding on the transition process, a human-centric care model using the design thinking process and tools of inquiry can be developed to address the root issues of the problem and improve the experience of senior adults transitioning into NH.
Footnotes
Acknowledgements
We would like to thank the senior residents and staff of NTUC Health Nursing Homes for participation in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded under SIT-Research Scholarship Funding.