
Abstract
Objective
We aimed to assess how daily-living-related contextual cueing (DLCC) affects memory performance in three groups: healthy older adults (HA), those with subjective cognitive decline (SCD), and mild cognitive impairment (MCI), while accounting for age and education.
Methods
After gathering demographic information, participants underwent neuropsychological assessments including the Montreal Cognitive Assessment (MoCA), Everyday Cognition Scale (ECog-12), Mini Mental State Examination (MMSE), Geriatric Depression Scale (GDS), and Trail Making Test (TMT) to establish baseline characteristics. Participants were categorized into HA (N = 47), SCD (N = 54), and MCI (N = 43) groups based on MoCA and ECog-12 scores. Memory performance was evaluated through two components of the Contextual Memory Test (CMT): one with non-contextual cues and the other with daily-living-related contextual cues.
Results
Interaction effects between contextual cueing and group for immediate recall (p < .001), delayed recall (p < .001), and total recall (p < .001) were found. All recall scores were lower in the MCI group than in the other two groups in the contextual cueing, not non-contextual. The post-hoc results revealed that scores on immediate recall, delayed recall, and total recall were lower in the MCI group than in the other two groups in the contextual cueing condition but not in the non-contextual cueing one.
Conclusions
Daily-living-related contextual cueing benefited HA, SCD, and younger-adult MCI groups more than older-adult MCI group, particularly enhancing delayed and total memory performance.
Introduction
Contextual cueing refers to the process by which individuals use cues from their everyday environments to enhance memory and recall of associated items. This method evaluates whether people can detect and utilize contextual information spontaneously, such as recognizing a dining or bathroom setting, to improve memory performance in daily tasks. By understanding that providing clear context cues, like mentioning a restaurant scene, can significantly aid in recalling items embedded within that context, this approach highlights the importance of context in memory function.
Contextual cuing has been extensively applied in various ways to enhance memory performance. Some examples are the use of scenes of video or specific spoken sentences as environmental contextual cues (Farias et al., 2008; Glisky et al., 2001; Smith et al., 2014; van Harten et al., 2018), the colors or geometric shapes of backgrounds as visuospatial contextual cues (Manginelli et al., 2013; Shapiro & Levy-Gigi, 2016), or specific context-related instructions as contextual prompts (Bisol Balardin et al., 2009; de Lima et al., 2019). In our study, specific context-related instruction, namely, daily-living-related contextual cuing (DLCC), was employed. Contextual cues enhance information retrieval by associating information and providing additional points of association to aid in recall, thereby helping individuals organize and store information more effectively. Previous research using daily living situations as contextual cues has primarily focused on healthy adults (de Lima et al., 2019; Smith et al., 2014) and older individuals with depression (Bisol Balardin et al., 2009). Studies investigating the effects of contextual cues on individuals with cognitive impairment are rare. In addition, the contextual cues utilized in the previous studies, such as geometric shapes and colors, were unrelated to daily living (Kessels et al., 2010; Levy-Gigi et al., 2011). Our research intended to investigate the effectiveness of using daily living-related instruction as contextual cues in individuals with cognitive impairment.
Individuals with Mild Cognitive Impairment (MCI) often experience deficits in functional activities and social engagement. Research also indicates that they face challenges in performing activities of daily living, such as managing household tasks and using daily living technology products (Jekel et al., 2015). The previous studies indicate that individuals with MCI cannot benefit from contextual cues unrelated to daily living (Kessels et al., 2010; Levy-Gigi et al., 2011), but the benefits of contextual cues related to daily living remain unknown. Kessels et al. (2010) showed that individuals with MCI may not be able to utilize object-location information as contextual cues to enhance their memory performance and that their performance was significantly lower than the performance of age-matched healthy adults. Levy-Gigi et al. (2011) pointed out that individuals with MCI may have deficits in their ability to acquire information associations from the contextual cues of a geometric shape background.
Subjective Cognitive Decline (SCD) is considered a potential risk factor for the development of MCI in individuals who are initially cognitively unimpaired (Perez-Blanco et al., 2022)). SCD refers to the subjective perception of an individual’s own decline in their cognitive function, specifically in memory, but without objective evidence of impairment on standardized cognitive tests or clinical evaluations (Jessen, 2014). Individuals with SCD perceive their daily living performance as impaired, perceive low satisfaction with their own memory ability, and sense difficulty in completing complex real-world task (Rotenberg & Dawson, 2022). However, their accuracy in recognizing activities is similar to that of healthy individuals (Chi et al., 2022). Indeed, individuals with SCD may experience difficulty in accurately self-assessing their own memory abilities, but it is possible that they may also have no deficits in the use of memory cues.
In addition, age and education level are significant factors that influence memory performance (Shapiro & Levy-Gigi, 2016). Bisol Balardin et al. (2009) also showed that elderly adults perform as well as young adults after receiving daily-living-related contextual cuing in memory tasks but more poorly than them in a non-contextual cuing condition. Consideration of age and education level in the examination of memory performance is important for understanding how older adults with SCD and MCI cope with problems in the use of contextual cueing. Our study aimed to determine how daily-living-related contextual cueing influences memory performance in three groups (healthy older adults (HA), SCD, and MCI), with consideration of age and education level. We hypothesized that memory performance could be improved by daily-living-related contextual cuing for both individuals with SCD and MCI, and that age and education level could have a potential impact on the utilization of daily-living-related contextual cuing.
Methods
Participants
The participants were recruited from a daily care center, a local older adult’s community college, and a community center for retirees by the convenience and snowball sampling method. The inclusion criteria were: (1) age ≥55 years, (2) ability to comprehend the instructions and questions in the neuropsychology test used in our study, (3) no history of hospitalization in the previous 6 months, and (4) no documented central nervous system dysfunction. The exclusion criteria included: the use of psychotropic medication (including antidepressants or hypnotic drugs) within the previous 6 weeks, major unstable medical illness, or other neurological disorders (including stroke, Parkinson’s disease, seizure, head injury, or dementia). The study was approved by the local Institutional Review Board (IRB no.: C104062). All participants signed informed consent forms before participating in the study.
Measurements
Baseline measure
The study employed a comprehensive set of baseline assessments, including the Montreal Cognitive Assessment (MoCA), the Mini-Mental State Examination (MMSE), the Everyday Cognition Scale (ECog-12), the Geriatric Depression Scale (GDS), and the Trail Making Test (TMT), to evaluate cognitive function across a spectrum from intact cognition to MCI and SCD. The MMSE was administered to all participants to assess cognitive function, with a cut-off score of 24 or below (out of 30) indicating potential dementia concerns resulting in exclusion from the study (Guo et al., 1988). MoCA is particularly noted for its 90% sensitivity in early MCI detection (Jessen et al., 2020; Nasreddine et al., 2005). The study used the ECog-12 criteria set by van Harten et al. (2018) to diagnose SCD, where a score of 2 or higher suggests potential SCD; individuals identified with SCD maintained normal scores on both the MMSE and GDS, underscoring the need for a multifaceted approach in cognitive evaluations (van Harten et al., 2018).
Montreal cognitive assessment
The MoCA is a widely used cognitive assessment tool for identifying subtle cognitive deficits. Since its validation in the early 2000s, MoCA has been recognized as a sensitive instrument for the early identification of MCI (Jessen et al., 2020; Nasreddine et al., 2005). The test lasts about 10 minutes and assesses the following cognitive domains: short-term memory, visuospatial abilities, executive functions, attention, concentration, working memory, language, and orientation to time and place. Each domain has a different score, with the total test score ranging from 0 to 30 points. This measurement tool has good reliability and validity, and a certified Chinese paper version (MoCA-T) is available with established reliability and validity (Tsai et al., 2012).
Everyday cognition scale
The ECog-12 was used to evaluate SCD (Farias et al., 2008). The ECog-12 was administered through self-reporting by participants. It has been demonstrated to be a feasible tool for detecting SCD in older adults (Sternberg, 2016; van Harten et al., 2018). According to a previous study, the criteria for identifying SCD using the ECog-12 is any item with a score of 2 or more (van Harten et al., 2018). Additionally, the SCD group scored within the normal range on the MMSE and the GDS.
Mini-mental state examination
The MMSE, designed to assess cognitive functions including orientation, memory registration, attention with calculation, short-term recall, language understanding, and visuospatial capabilities, indicates the necessity of further cognitive evaluations for scores less than 24 (Folstein et al., 1975; Nasreddine et al., 2005). For this study, the Chinese version of the MMSE (MMSE-C), established by Guo et al., in 1988, was employed.
Geriatric depression scale
The Short Form of the 15-item GDS, translated into Chinese by Chan in 1996, is a concise survey designed to identify depressive symptoms among elderly individuals. This tool asks respondents to answer each item with a simple “yes” or “no” based on their feelings in the previous week. Scoring is straightforward, with each item worth one point, and a cumulative score above 6 points may indicate depression (Yesavage et al., 1982).
Trail making test
The TMT assessment is commonly employed to evaluate executive function in older adults and is composed of two segments (Faria et al., 2015). The first segment, the TMT-A, requires participants to connect 25 numbers in sequential order, while the second segment, the TMT-B, involves connecting numbers and letters alternately in sequence. Completion time in seconds is used to determine the score for each segment. Multiple studies have been conducted to establish the psychometric properties of the test, including its construct validity (Sánchez-Cubillo et al., 2009), normative data (Lu & Bigler, 2002), and test–retest reliability (Lemay et al., 2004).
Memory performance measure
To measure memory performance, we utilized specific components of the Contextual Memory Test (CMT). The CMT is a standardized assessment tool used to measure four aspects of memory performance: (1) self-awareness of memory ability, (2) memory performance after non-contextual cueing, (3) memory performance after daily-living-related contextual cueing, and (4) memory strategy use (Toglia, 1993). To achieve the objectives of our research, we employed two of these components, namely, memory performance after non-contextual cueing and memory performance after daily-living-related contextual cueing. Two picture cards in total have to be used. Each card contains 20 drawings of common items in a particular context. One is restaurant themed and the other is morning themed. Different instructions are used as contextual cueing in the corresponding condition. For “non-contextual cueing”, the participants are asked to view the drawings on the card for 90 seconds. For the contextual cueing, standardized instructions were provided, themed around either a restaurant or morning routine. For the restaurant scenario, participants were given the following prompt: “I will show you a picture card, and you will have 90 seconds to memorize the items in the picture. After 90 seconds, please tell me which items you remember. While you look at the pictures, imagine the scene in a restaurant and what might happen when someone enters the restaurant. If you are unsure of the name of any item, please tell me. Are you ready? Begin!” Similarly, in the morning scenario, the cueing was: “I will show you a picture card, and you will have 90 seconds to remember the items in the picture. After 90 seconds, tell me what items you recall. As you view the pictures, think about what someone might do when they wake up and prepare to leave the house in the morning. If you are unsure of the name of any item, please tell me. Are you ready? Begin!”
The psychometric properties of the CMT have been well-established, including construct validity among age groups (i.e., young, middle aged, and older adults) (Josman & Hartman-Maeir, 2000); discriminative validity for individuals with traumatic brain injury (Toglia, 1993), Alzheimer’s disease (Gil & Josman, 2001), and MCI (Liao et al., 2020); and cross-cultural validation for Israel (Josman & Hartman-Maeir, 2000). The test–retest reliability and the minimal detectable change (MDC) of the CMT in older adults with and without MCI have been reported (Liao et al., 2020).
Experimental procedures
Three occupational therapists performed the CMT assessments. Prior to testing, the raters received training on the proper use of all measures to establish both intra- and inter-rater reliability. The training included a lecture on introducing the measures and rating instructions, and both written and verbal instructions were provided before data collection. All raters viewed a video clip of the same older adults performing the test and were tasked with rating the observed trials to examine rater reliability. To minimize subjectivity in scoring, rating criteria for each assessment were reviewed, and any disagreements were addressed until all raters were able to perform the assessment consistently. A good level of rater reliability was demonstrated by an intraclass correlation coefficient (ICC) of 0.9.
The two memory tests of the CMT were administered as follows. For the first memory test, the non-contextual cueing test, the experimenter randomly presented one of the two picture cards for 90 seconds and asked the participant to recall the items immediately (immediate recall). The experimenter asked the participants to recall the items on the same picture card again after 15–20 minutes (delayed recall). During the 15–20 minute period, participants were free to engage in any activities unrelated to memory, such as drinking water, chatting, or taking a walk. Two to 4 days later, the second memory test, the contextual cueing test, was administered. The experimenter asked the participants to complete immediate and delayed recall tasks. The process and execution were the same as those of the first memory test, except for two differences. The first was that another scenario picture card was used. If the first memory test was based on the restaurant theme, the second memory test was based on the morning theme. The second difference was that context-specific prompts based on daily living scenarios were used. The examiner provided standardized instructions which clearly indicated the restaurant theme or the morning theme. The order of the tests was always the non-contextual cueing test followed by the contextual cueing test. The morning or restaurant version was used in either the first or second memory test in a randomized order for each participant (Toglia, 1993). Participants were assessed in a quiet room to minimize interference and required to rest during breaks.
Scoring
For memory performance after non-contextual cueing, immediate, delayed, and total recall were scored from the outcomes of the first memory test. Immediate recall and delayed recall scores were the numbers of items remembered immediately after the first memory test and after a 15–20 minute delay, with a score range of 0–20. Total recall was calculated by summing the immediate recall and delayed recall scores. For memory performance after contextual cueing, immediate, delayed, and total recall were scored from the outcome of the second memory test. All of these tests followed the same scoring procedures as those in the first memory test. The scoring procedures adhered to the guidelines specified in the CMT manual (Toglia, 1993).
Grouping participants
After collecting demographic data, all neuropsychological tests were administered to all participants. Subsequently, they were categorized into the HA, SCD, and MCI groups for statistical analysis based on their scores on the MoCA and ECog-12. Those with MoCA scores of 24 or lower were categorized into the MCI group (Julayanont & Nasreddine, 2017), while those with scores of 25 or higher were categorized into either the HA or SCD groups. Participants with MoCA scores of 25 or higher and an ECog-12 with any item scored 2 or higher were classified into the SCD group (Farias et al., 2008; van Harten et al., 2018), while the remaining participants were assigned to the HA group. The flow chart of the study is provided in Figure 1. Flow chart of the study.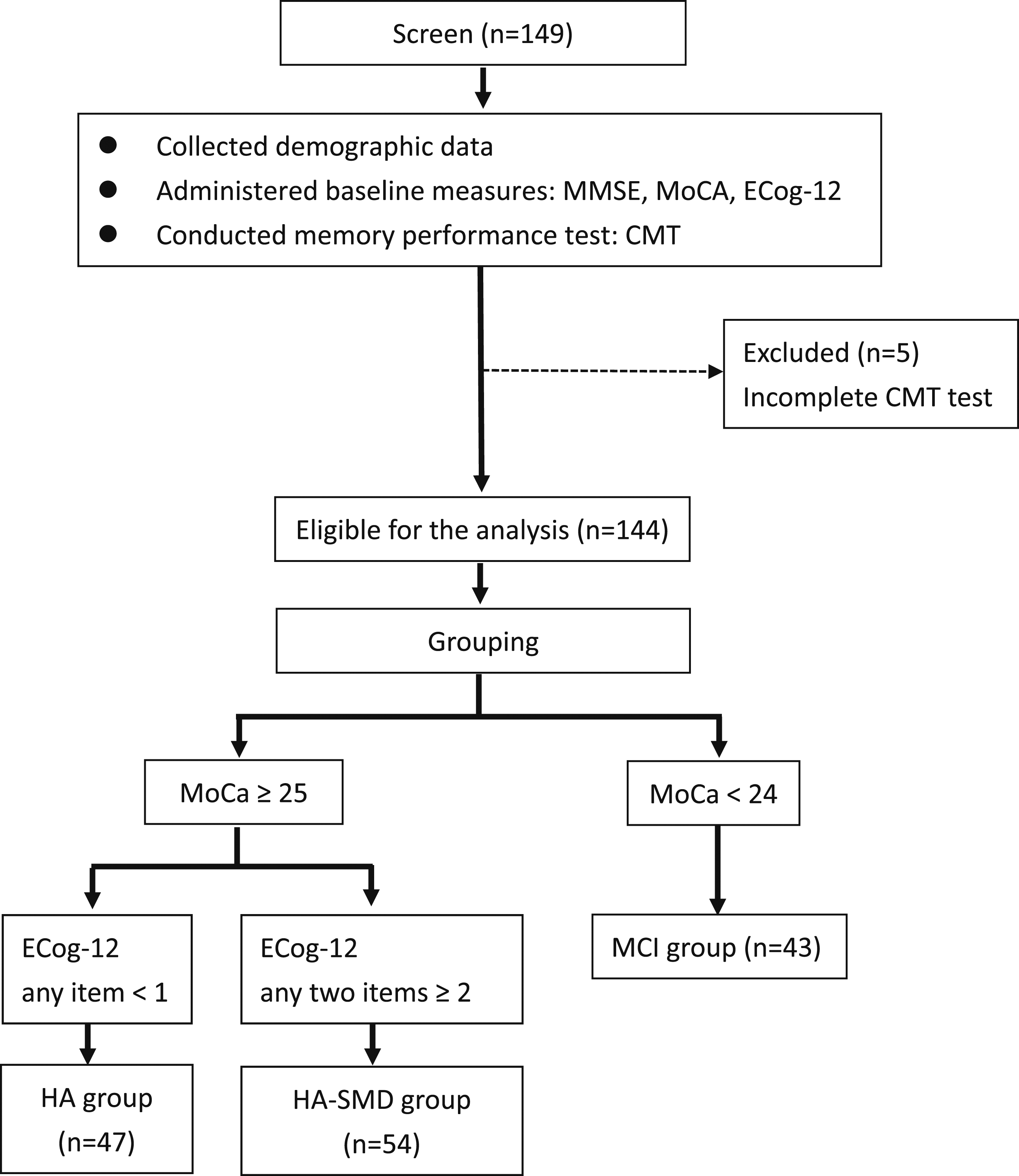
Data analysis
Demographic and neuropsychological characteristics were compared for each of the three groups (HA, SCD, and MCI) using one-way analysis of variance (ANOVA) followed by Bonferroni’s post hoc test if a significant difference was found. To investigate how contextual information, together with education and age, influenced immediate recall, delayed recall, and total recall among the three groups, 3 × 2 × 2 × 2 mixed repeated measures ANOVAs were performed with contextual information (non-contextual cueing and contextual cueing) as the within-group factor and group (HA, SCD, or MCI), age (≥65 or <65 years), and education (>12 or ≤12 years) as the between groups factors. Separate 3 × 2 × 2 × 2 mixed repeated measures ANOVAs were conducted for each type of memory performance (immediate, delayed, and total recall). Given that Taiwan mandates 12 years of compulsory education, we use this duration as one of the grouping factors in our study. Another factor is age, considering the definition categorizes individuals aged 65 and above as elderly. Therefore, we utilize age 65 as another criterion for differentiation (Orimo et al., 2006). Multiple comparisons among mean differences were checked with Bonferroni post hoc tests, as necessary. All analyses were performed in SPSS version 20.0 (IBM Corp; Armonk, NY). A p-value of less than 0.05 was considered to be statistically significant.
Results
The baseline characteristics of healthy older adults, participants with subjective memory complaints, and participants with mild cognitive disorders.
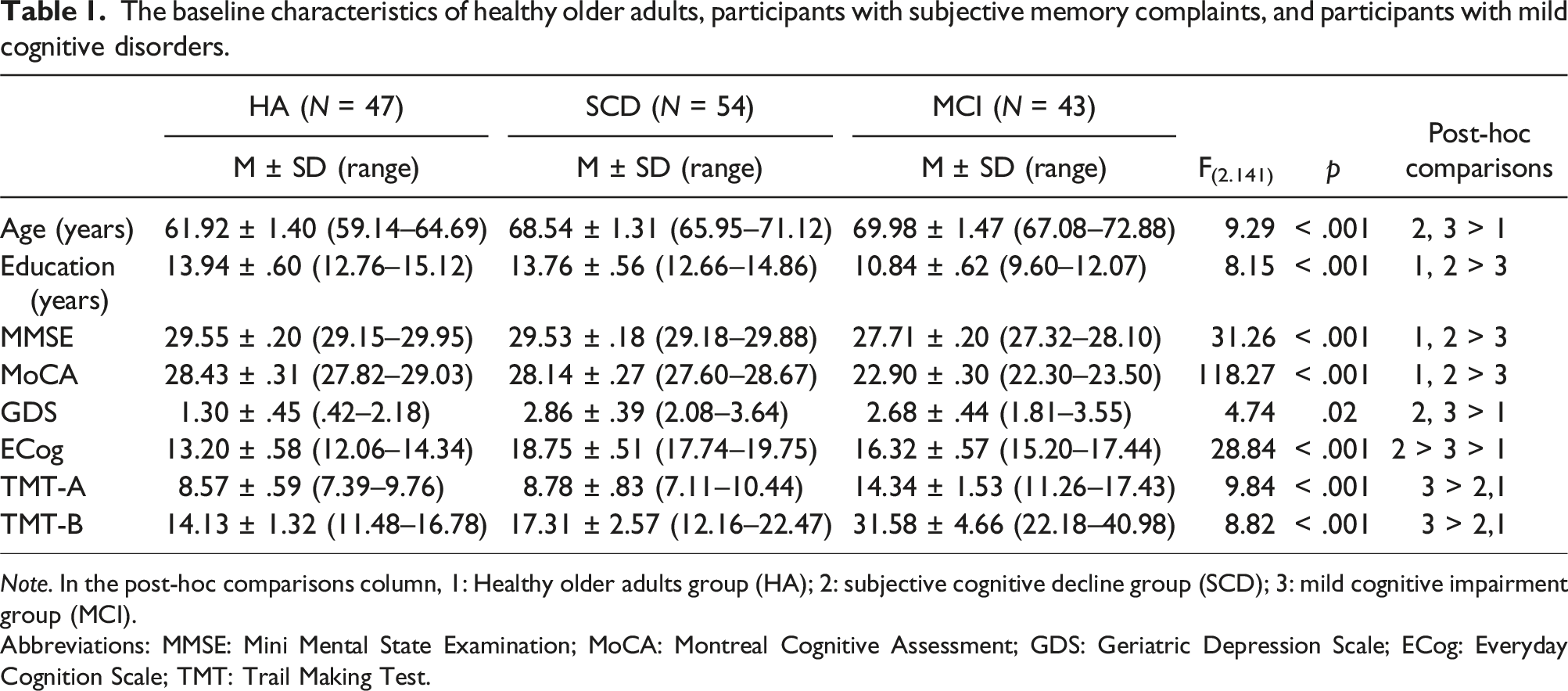
Note. In the post-hoc comparisons column, 1: Healthy older adults group (HA); 2: subjective cognitive decline group (SCD); 3: mild cognitive impairment group (MCI).
Abbreviations: MMSE: Mini Mental State Examination; MoCA: Montreal Cognitive Assessment; GDS: Geriatric Depression Scale; ECog: Everyday Cognition Scale; TMT: Trail Making Test.
Baseline characteristics of group factors
Table 1 summarizes the demographic and neuropsychological characteristics of the three experimental groups. There were significant differences in education years, MMSE scores, and MoCA scores among the three groups, with the lowest scores in the MCI group. There were significant differences in age among the three groups (p < .001). The post-hoc test revealed that the age was lower in the HA group compared to the other groups, with no significant difference observed between the SCD and MCI groups. Regarding neuropsychological characteristics, significant group differences were found in the ECog-12, GDS, TMT-A, and TMT-B scores. The post-hoc test showed that the ECog-12 scores were higher in the SCD than in the MCI group, and higher in the MCI than in the HA group. The GDS scores of the HA group were lower than those of the other groups. For the TMT-A and TMT-B, the scores were higher in the MCI group than in the other groups, and no difference was found between the HA and SCD groups.
Influences of contextual information, group, age, and education on memory performance
Comparisons of performance of the contextual memory test among healthy older adults, participants with subjective cognitive decline, and participants with mild cognitive impairment.
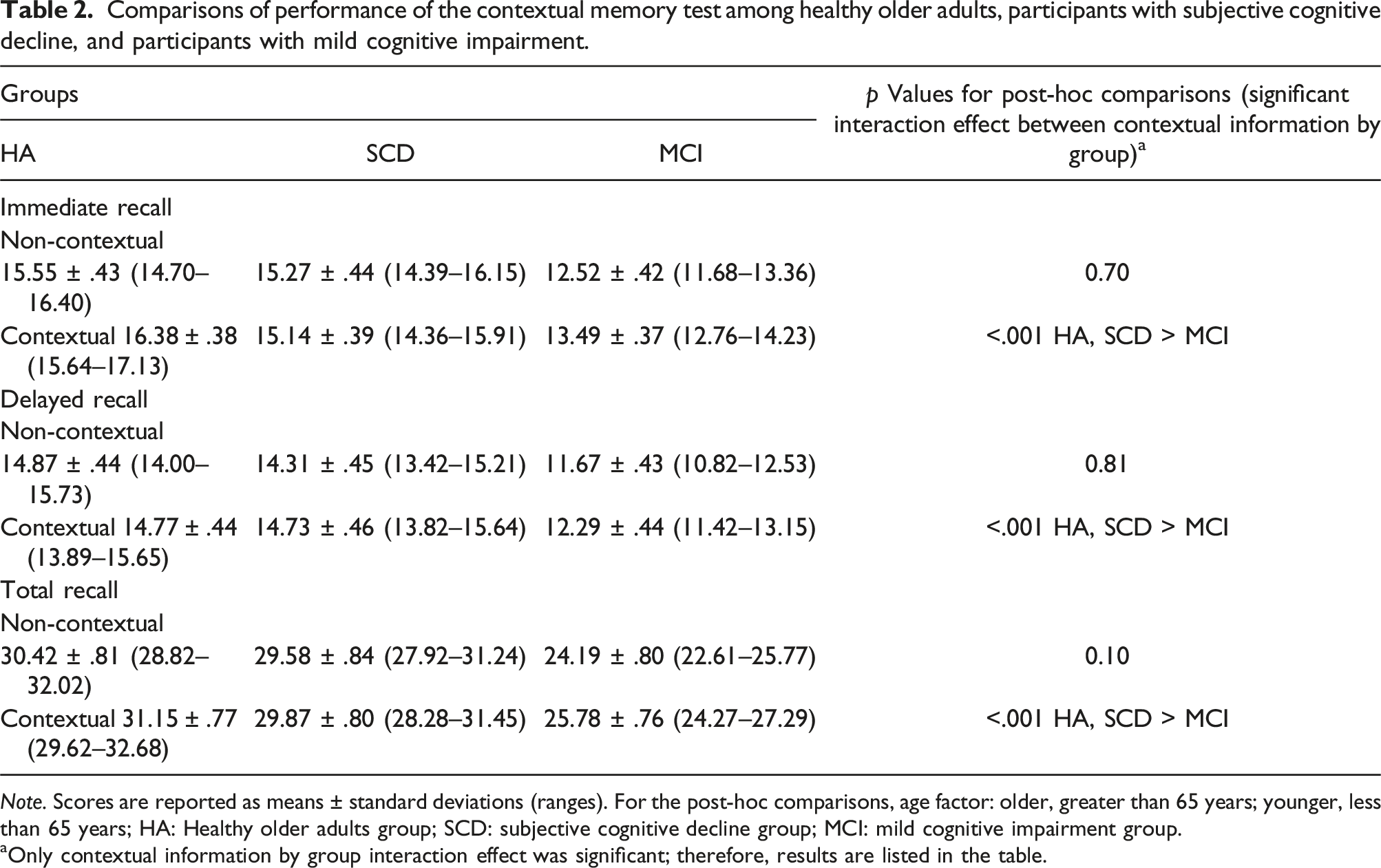
Note. Scores are reported as means ± standard deviations (ranges). For the post-hoc comparisons, age factor: older, greater than 65 years; younger, less than 65 years; HA: Healthy older adults group; SCD: subjective cognitive decline group; MCI: mild cognitive impairment group.
aOnly contextual information by group interaction effect was significant; therefore, results are listed in the table.
The interaction effect between contextual information and group was significant for all three types of memory performance (all p < .001). Further analyses revealed significant effects within the contextual cueing condition for immediate recall (p < .001), delayed recall (p < .001), and total recall (p < .001). The post-hoc results revealed that scores on immediate recall, delayed recall, and total recall were lower in the MCI group than in the other two groups in the contextual cueing condition but not in the non-contextual cueing one.
Discussion
This study aimed to compare the memory performance between daily-living-related contextual cueing and non-contextual cuing among older adults with HA, SCD, and MCI while considering age and education. We found significant interactions effect between contextual cueing and group factors in memory performance. The MCI group showed less ability than the other groups to use contextual cueing for immediate, delayed and total recall performance.
The impact of age-related characteristics on memory benefits from contextual cues
While considering the age factor, delayed and total memory performance were worse in the older-adult MCI subgroup than in the HA and SCD groups, but not worse than in the younger one, in the presence of contextual cues. Previous studies focusing on healthy adults have shown that elderly adults benefit from daily-living-related contextual cuing in memory tasks and perform as well as young adults (Bisol Balardin et al., 2009; Glisky et al., 2001). Other studies have evidenced that, in healthy elderly adults, performance was better after daily-living-related contextual cueing in memory tasks than after non-contextual cueing (Bisol Balardin et al., 2009; de Lima et al., 2019). The aforementioned findings for healthy adults are consistent with the interactive influence of daily-living-related contextual cues and age-related characteristics in our results.
While considering the age factor, for delayed recall and total recall after contextual cueing, a significantly lower scores in the MCI group than in the other two groups in the older adult group, but not in the younger adult group. Langley et al. (2008) reported that elderly adults used contextual cueing with a delay in timing. Our results showed that, among the young population, whether it’s the HA group, the SCD group, or the MCI group, the ability to utilize daily-living-related contextual cues to promote the delayed and total recall performance is equal.
The impact of cognition-related characteristics on memory benefits from contextual cues
While considering the cognition-related factors, immediate, delayed and total memory performance were worse in the MCI subgroup than in the HA and SCD subgroups when daily-living-related contextual cues were used. Previous research has shown that memory performance is lower in individuals with MCI than in healthy individuals (Kessels et al., 2010; Levy-Gigi et al., 2011). Individuals with MCI have demonstrated a lower ability to find the associations between information and context compared with healthy individuals. The use of contextual cues to enhance individuals’ memory is an internal memory strategy. Research indicates that individuals with MCI have less strategy knowledge and less counts of internal strategy use compared with healthy adults (Hutchens et al., 2012). Our findings suggested that the HA and SCD groups were more skillful in using daily-living-related contextual cueing to improve memory-related links and boost memory performance than was the MCI group. The individuals with MCI benefitted less from the use of daily-living-related contextual cues.
The poor performance of the MCI group in scenarios using contextual cues, compared to the HA and SCD groups, likely stems from their diminished ability to associate information with its context. This impairment in linking context with memory cues may explain why individuals with MCI did not exhibit the expected performance deficits in non-contextual cueing situations, where such associations are less critical. The TMT completion times for both parts A and B were significantly longer in the MCI group compared to the healthy adults and SCD groups, indicating potential deficits in central executive functioning and cognitive flexibility. The TMT is believed to assess a wide array of cognitive functions, including attention, visual search and scanning, working memory, psychomotor speed, and other abilities (Salthouse, 2011; Salthouse & Fristoe, 1995). These cognitive abilities are crucial for contextual-cueing scenarios, as participants need to recall real-world situations to facilitate memory and succeed in this test. Therefore, non-contextual tasks, which rely less on contextual associations, might not reveal the specific cognitive limitations of the MCI group as clearly as contextual tasks do. Participants often expressed that their strategy was to try hard to memorize as many items as possible, which might be less cognitively demanding for individuals with MCI.
We found the memory benefits from contextual cues to be consistent between the HA and SCD groups. The memory difficulty in the SCD group was self-perceived difficulty. A previous study stated that the SCD group perceived greater difficulty than the HA group did (Lehrner et al., 2015). In fact, the memory performance of the SCD group was consistent with that of the HA group (Rotenberg & Dawson, 2022). Therefore, the SCD group may have experienced a consistent memory practice process with the HA group, unlike their perceived difficulty, leading to the consistent memory performance reported after the memory test.
Limitations
The current study had several limitations. First, the convenience sample was area-specific and significantly different among the groups. To enhance the applicability of our findings, future research should employ a comprehensive sampling approach and gather substantial sample sizes. Second, participants were allocated to each group based on cognitive evaluation tests, including MMSE, MoCA and ECog. While cognitive test scores can provide valuable insights into potential cognitive decline, it is important to note that the participants in our study were not formally diagnosed. This could limit the generalizability of the current findings.
Conclusions
This study demonstrated that the HA, SCD, and younger-adult MCI groups benefitted more than the older-adult MCI group from daily-living-related contextual cueing to enhance memory performance in delayed and total memory performance. Contextual cueing may be applicable as a strategy for training memory performance in HA, SCD and younger-adult MCI groups in clinics.
In clinical practice, contextual cueing can help improve functional performance for individuals with cognitive complaints or impairments. Research indicates that familiar real-world spatial cueing offers memory benefits to individuals of all ages (Robin & Moscovitch, 2017) and enhances prospective memory (Bowden et al., 2021). In consistent environments, people are better at recognizing and responding to repeated visual stimuli, which can be advantageous for those with cognitive impairments. Interventions at home or in the community may assist in training daily activities. Current findings suggest that these interventions should be tailored to each individual’s cognitive status. Younger adults with MCI benefited from contextual cues similarly to healthy adults and those with SCD, suggesting that age may influence the effectiveness of these aids. This highlights the potential for early intervention strategies using contextual cues to support memory function, particularly for those at risk of cognitive decline. Customizing these strategies based on cognitive status and age could enhance cognitive rehabilitation outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Chang Gung Memorial Hospital (CMRPD1L0193, BMRP553, BMRPC 58), and Healthy Aging Research Center at Chang Gung University (URRPD1P0181).