
Abstract
Background
Substance use disorders (SUDs) may cause severe social and health problems. Therefore, providing adequate treatments for people with SUDs to change their drug use behaviors is important. This study examined the effectiveness of Kawa Model based therapy among people with SUDs in Taiwan.
Methods
Participants were recruited from people with SUDs who violated the Controlled Drugs Act in Taiwan were mandated to abstinence services by law from January 2016 through October 2021 in Southern Taiwan. Each participant selected a 2-hour for 4 times or 8-hour for one day compulsory treatments and received either the Kawa model based treatment (n = 55; 9 women; mean ± SD age = 36.73 ± 10.42 years) or psychoeducation courses (n = 42; 8 women; mean ± SD age = 27.57 ± 5.78 years), respectively. Stages of change was assessed using the University of Rhode Island Change Assessment before and after treatments.
Results
There were no significant differences in the stages of change scores at baselines between the 2 groups (p = .06–0.20). After treatments, participants who received the Kawa Model based treatment had higher scores in specific stages of change than did those who received the psychoeducation course in the domains of ‘contemplation’ (p = .001), ‘action’ (p = .001), and ‘readiness’ (p = .002).
Conclusion
The present study demonstrated initial and preliminary findings that the Kawa Model based therapy may improve readiness for changing drug use behaviors in people with SUDs.
Keywords
Introduction
Substance use disorders (SUDs) are a global concern. The United Nations Office on Drugs and Crime (2015) has updated global calls for action. People of different sociodemographic backgrounds and cultures may experience SUDs (Ünübol & Hızlı Sayar, 2021). The overall prevalence of using illicit drugs is about 1.29% in Taiwan and with rates of 1.9 %, 1.7% and 2.1% in the 18 to 24, 25 to 34, and 35–44 years old group, respectively (Chen et al., 2017), and the mostly used drugs are ketamine and amphetamines recently. People with SUDs may engage in criminal activities (e.g., stealing or dealing drugs) as means for buying drugs (Cheon et al., 2018; Olfson et al., 2018). This problem is especially serious in Taiwan given that substance use (except for nicotine/tobacco and alcohol) is a crime in Taiwan (Laws and Regulations Database of Taiwan, 2013). Because people with SUDs in Taiwan are afraid of being sent to a prison, they may not actively seek psychiatric treatment as this may increase their risk of being reported to the police by healthcare providers (Chen et al., 2021; Feng & Li, 2020). Therefore, healthcare professionals in mental health in Taiwan may experience significant challenges regarding providing effective care for people with SUDs.
Apart from reluctance for seeking formal treatment (e.g., visiting a psychiatrist, a psychologist, or an occupational therapist), people with SUDs may suffer from impaired health due to drug use. People with SUDs may experience both physical and psychological health problems (Hinson-Enslin et al., 2022; Marino et al., 2021). For example, they may experience infectious diseases (e.g., hepatitis B virus, hepatitis C virus, and human immunodeficiency virus diseases) relating to intravenous use or risky sexual behaviors, drug-induced psychotic symptoms, stigma, impaired quality of life (QoL), and low self-esteem (Chang et al., 2019, 2020, 2022; Chang & Lin, 2015; Yang et al., 2019). Therefore, when caring for people with SUDs, healthcare professionals in mental health should provide appropriate treatments for their physical and mental health problems in addition to addressing their SUDs.
In order to tackle the health issues of people with SUDs and their hesitancies to receive treatments, adequate programs that can address the motivation, engagement and adherence for treatment are warranted. A potential treatment based on occupational therapy concepts and theory - the Kawa (aka river in Japanese) Model (Iwama, 2006; Iwama et al., 2009) is suggested. The Kawa Model could motivate people’s willingness to receive treatment as it takes the river as a metaphor for life (Iwama, 2006). The attractiveness of using the river as a metaphor is that it may generate vivid images regarding how people have experienced their lives. By describing life experiences through a river metaphor with flow space, driftwoods, banks, and rocks, the elements of the individuals’ sociocultural environments, their expectations and aspirations, and their assets and limitations may be clarified (Iwama et al., 2009). Thus, the Kawa Model represents a client-centered and culture-responsive approach for occupational therapists (Gregg et al., 2015). With narrative features, the forms of the river may help individuals address what they find to be significant and connected to the overall goals of their life.
For people with SUDs, using Kawa Model provides them a sense of safety instead of feeling judged or stigmatized when they are interviewed to disclose their histories and experiences of using drugs. In other words, using Kawa Model approach can prevent from triggering their defensive reactions and reluctance to seek help.
Farhoudian et al. (2022) investigated the barrier and facilitators to SUD treatment and summarized that low motivation, denial, and resistance are frequently seen as typical difficulties of individuals with SUDs. It is suggested that medical professionals can facilitate the individuals and enhance their motivation by establishing a therapeutic connection based on mutual respect and the client’s autonomy while simultaneously assuming a consultation role. The service-related issues of treatment providers (e.g., failure to ground programming in the lived experiences, legal barriers, and policy constraints) also pose barriers to achieve positive treatment outcomes. To connect the lived experiences of the persons who have had used drug in life, the Kawa Model treatment process is of great potential to improve the motivation and engagement for treatment in people with SUDs. With river metaphor and narratives, substance use and related health impairments may be better visualized as a condition instead of a problem or a stigma in the process (Hsiao et al., 2023).
Implementation of the Kawa Model for treatment in people with SUDs includes the following procedures (Iwama et al., 2009). First, the therapist invites people with SUDs to draw a picture of a river, imagining that the river represents their life and their present situation. Within this process, the therapist develops a dialogue around the circumstances and contexts of people with SUDs, using the river as a metaphor of the view of self and reality among people with SUDs. The meanings of water, rocks, drifting woods, and river bottom are then explained (Step 1). After people with SUDs grasp the metaphorical meanings, they draw a cross-sectional image of their rivers at the present moment. The cross-sectional view with the elements in the river provides the therapists and people with SUDs an opportunity to clarify the symbolic meanings of each element and the relevance to themselves and their circumstances (Step 2). After further discussion, issues related to current circumstances are prioritized according to the perspectives of people with SUDs. The relationships among these elements are explored to gain an accurate, detailed description of the problems for people with SUDs (Step 3). After the information about life experiences is supported, target goals and priorities to change for further intervention may be better recognized by people with SUDs (Step 4). The major goals that are centered to the concerns of people with SUDs are then formulated as treatment goals in the therapy. The therapist and people with SUDs may work on establishing skills/habits, maintaining or promoting health, modifying task requirements, or creating a supported environment for change afterwards (Step 5). The final stage is the evaluation of satisfaction about change, that is, people with SUDs evaluate their rivers and their satisfactions in receiving the Kawa Model based therapy. Like water in the river, some problems may remain and may not be without impediments, but life still moves on to its destination (Step 6).
It can be noted from the above that the Kawa Model may help people with SUDs to pursue stages of change. Specifically, the Transtheoretical model proposes that behavioral change may have at least four stages, including ‘precontemplation’, ‘contemplation’, ‘action’, and ‘maintenance’ (Chan et al., 2007; Prochaska et al., 1992). ‘Precontemplation’ indicates that an individual does not have sufficient insight or readiness to observe his or her behavioral problems. ‘Contemplation’ indicates that an individual has found that there is something wrong in his or her behaviors; however, the individual is hesitant and reluctant to change their behaviors. ‘Action’ indicates that an individual has acknowledged the behavioral problems and is taking action to change their behaviors. ‘Maintenance’ indicates that the individual can maintain the changed behaviors (DiClemente et al., 2004; Velicer et al., 1998). Because the Kawa Model may assist people with SUDs in making behavioral changes, it may promote readiness for change in people with SUDs.
This study aimed to investigate the initial effects of a program designed based on the Kawa Model’s approach on behavioral changes (stages of change) and health-related outcomes (self-esteem, craving, and QoL) among people with SUDs. A quasi-experimental study design, including an intervention group and a control group without random assignment, was adopted in this study. We hypothesized that people with SUDs would demonstrate increases in stages of change, improvement in self-esteem and QoL, and reductions in craving after receiving the Kawa Model based therapy.
Methods
Participants and recruitment procedure
Participants were recruited from people living in Southern Taiwan who violated the Controlled Drugs Act (Laws and Regulations Database of Taiwan, 2013) and were mandated to abstinence education program by law, from January 2016 through October 2021. Participants, who mainly used ketamine or amphetamines, were referred to outpatient treatment programs by the local health bureau. There were two schedules of treatment for them to choose - one is a one-day class of 8 hours, and the other is 4 two-hour group on alternate weekends. Apart from scheduled treatment, there were no additional treatment mandates for them. They registered for either schedule by their time preference without knowing that the contents of the program - an education program and an outpatient treatment program offered by a psychiatric center. The implementing schedules were mandatory according to the policy guidance on controlled drugs implemented by the local health bureau. The primary goal of the programs was to educate knowledge regarding the harmfulness of illegal drugs to the participants and to increase their motivations for abstinence. The outpatient program, which was the intervention group in this study, was a group therapy program based on the Kawa Model whereas the education program, which was the control group in this study, was a lecture-based class. Moreover, all the participants signed a written informed consent to express their willingness to participate in the study. The study protocol has been approved by the Institutional Review Board in the Jianan Psychiatric Center (IRB No: 15–028).
Inclusion criteria for recruitment were: 1) reading Chinese without difficulties, 2) without intellectual disability, and 3) without neurological histories or unstable mental status. A total of 107 participants were enrolled in the study, 7 participants were excluded for not meeting the inclusion criteria, 3 participants dropped out before the study began. Ninety-seven eligible participants were consented to participate in this study, with 55 in the intervention group receiving the Kawa Model based therapy and 42 in the control group receiving the lectures. Both groups were assessed using the same measures. Figure 1 shows the study flowchart. Flow chart of research process. Note. All participants (55 in Intervention group and 42 in Control group) were used for the generalized estimating equations to satisfy the intention-to-treat analysis. 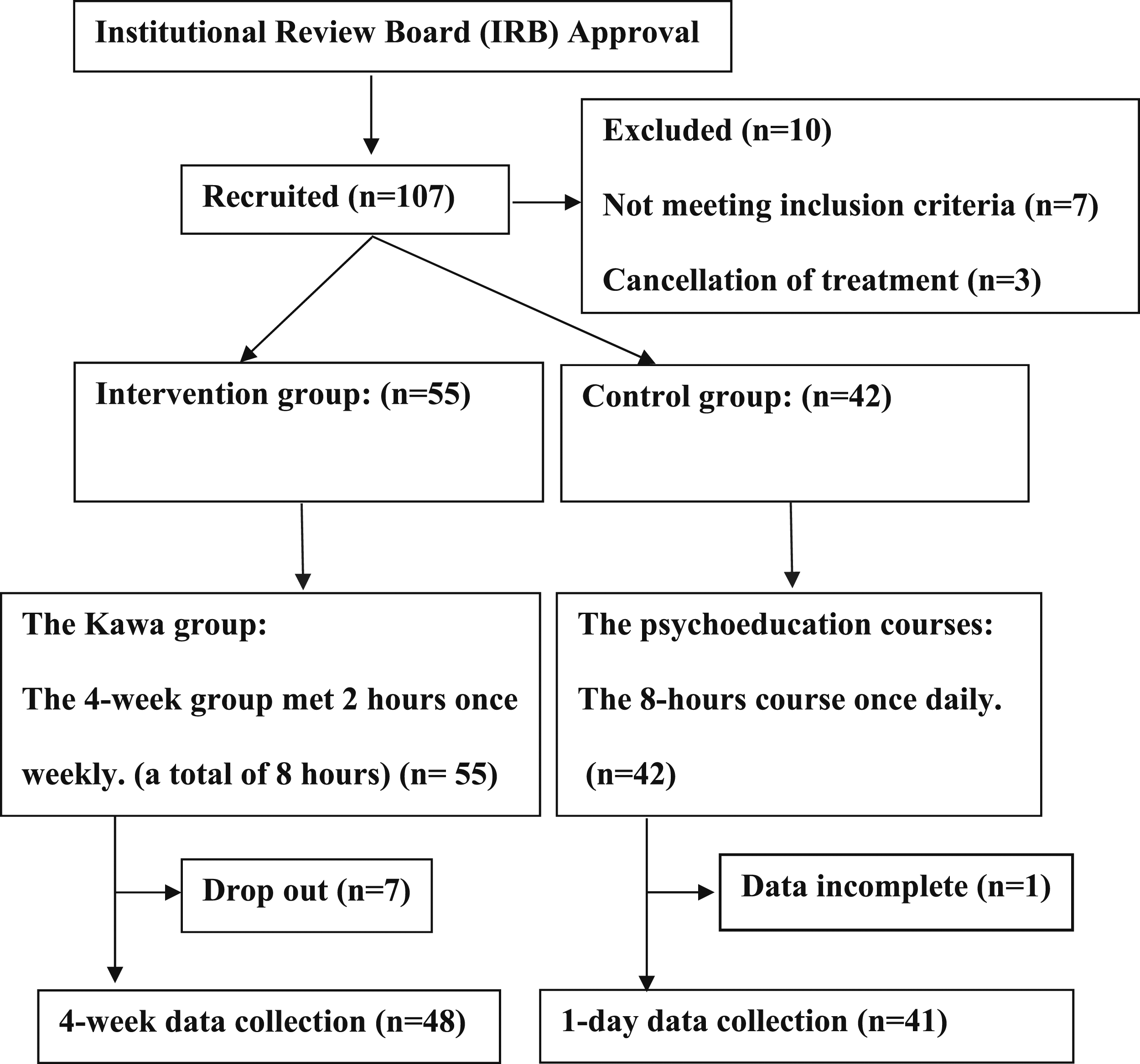
Intervention program using the Kawa model
Fifty-five participants attended the 2-hour Kawa Model based therapy group weekly, for a total of 4 weeks. Due to time constraints and program goals set by the bureau, the objectives were to complete procedures of the Kawa Model from Steps 1 to 3 to help the participants be aware of the danger of using drugs in order to increase their motivation to change. Steps 4 to 6 are about goal setting and change, which is beyond the scope of the mandates program. Therefore, steps 4 to 6 were not included in the present study. The first meeting of the intervention included a pre-test, group orientation, introduction of members and sharing of personal profile of responsibilities, living areas, hobbies, and any information participants wanted to share within the group. At the second meeting, participants were given an overview of the Kawa metaphor and its connection to early life circumstances. Then, they were asked to draw their life flow such that group members could later share their perspectives of their life trajectories based on their drawings. The third meeting continued the previous work by drawing the details of the elements within a cross-sectional view, with the images of water, flow space, driftwood, banks, and rocks that illustrated the barriers and beneficial things in their recent experience interweaved with substance-related concerns and abstinence. At the last group meeting, members prioritized important factors, listed their strengths, and made two to three achievable goals involving rethinking their expectations for now and the near future. The post-test questionnaires were completed immediately after treatment. In the Kawa Model based therapy group, the narratives of life trajectories and issues related to substance use were explored in the context of the river drawing. Participants shared their river images as well as their life experiences with others. The discussions about these emerging life issues and the roles of drugs in their lives were also discussed.
Program for the control group
Forty-two participants attended the lectures in the control group. The 8-hour course was arranged in one day. The psychoeducation courses included topics such as “How drugs affect our body”, “Addictive behavior and how to stop/change”, and “Introduction to the regulations of drug use”, etc. The pre- and post-test questionnaires were completed immediately before and after the lectures.
Sample size calculation
We assumed a large effect size (i.e., Cohen’s d at 0.8), with a two-tailed test and allocation ratio between the two groups at 1:1 to estimate the sample size. Considering the aforementioned assumptions and setting type I error at 0.5 and power at 0.95, the estimated sample was 42 for each group. Therefore, we targeted to recruit at least 42 participants in each group. Finally, we had recruited 55 participants in the intervention group and 42 in the control group.
Outcome measures
Primary outcome: Stages of change
The University of Rhode Island Change Assessment (URICA)
The URICA is an assessment that measures the stages of change based on the Transtheoretical Model. It has 32 items, and 8 items average in each subscale corresponding to the sequence of stages: precontemplation, contemplation, action, and maintenance. Participants rated their response on a 5-point Likert-like scale ranging from 1 (strongly disagree) to 5 (strongly agree). Sample questions include: “As far as I’m concerned, I don’t have any problems that need changing.” (Precontemplation), “I think I might be ready for some self-improvement.” (Contemplation), “I am doing something about the problems that had been bothering me.” (Action), and “It worries me that I might slip back on a problem I have already changed, so I am here to seek help.” (Maintenance). In this study, we summed participants’ scores on each subscale as Stage scores. These scores represent attitudes and activities related to the stages of change and not precisely affirm status. The higher Stage scores reflect greater readiness for change on the stages of contemplation, action, and maintenance. Additionally, a readiness score was calculated by subtracting the mean precontemplation score from the summation of the means of other three stages. The higher readiness score indicates the more readiness to change. The URICA (Chinese version) has demonstrated acceptable internal consistency (Cronbach’s α of .65–.73), with test-retest reliability ranging from .63 to .75 (Chan et al., 2007).
Secondary outcomes
We measured participants’ self-esteem, cravings for drug use, and QoL before and after the program. Measurements used for the secondary outcomes are listed below.
Rosenberg Self-Esteem Scale (RSES)
The Rosenberg Self-Esteem Scale (RSES) is a 10 item, using a 4-point Likert scale per question, which measures one’s global self-esteem. Responses are rated from 1 (strongly disagree) to 4 (strongly agree). The scale was found to have good test-retest reliability (r = .85) (Torrey et al., 2000), and high internal consistency (Cronbach’s α = .81) (Schmitt & Allik, 2005).
The Craving Beliefs Questionnaire (CBQ)
The 10-item Taiwanese CBQ measures a person’s beliefs regarding his or her drug cravings. The 10-item CBQ is derived from the original 20-item CBQ and has been commonly used in substance addiction services in Taiwan. The 10-item CBQ has demonstrated good internal consistency (Cronbach’s α of .81–.92) and test-retest reliability (r = 0.8) (Chang et al., 2011). Answers are given on a 4-point Likert-like scale (4 = completely agree and 1 = completely disagree). Lower scores suggest lower resistance against drug use and thus lower tendencies to change. A sample item of the CBQ is “Craving is a physical reaction; I cannot resist it.”
Taiwan version WHOQOL-BREF
The World Health Organization Quality of Life Questionnaire (WHOQOL-BREF) is a generic QoL questionnaire that can be used for multiple populations, including people with SUDs (Chang et al., 2014; Lin et al., 2019; Su et al., 2014). It is comprised of 26 questions, including 2 general items (i.e., ones assessing general QoL and another overall health), and the remaining 24 questions are distributed in 4 domains: physical, psychological, social relations and environment. Ratings are based on five-point Likert-like scales with specific responses such as “very dissatisfied” to “very satisfied”, “not at all” to “an extreme amount”, and “never” to “always”. Transformed domain scores resulted in a 4–20 scale in which higher scores reflect higher QoL (Yao et al., 2002). The Taiwan Version of the WHOQOL-BREF was validated with its four-factor (physical, psychological, social, and environment) confirmed (Chang et al., 2014; Yao et al., 2002). The scale demonstrated acceptable internal consistency, with Cronbach’s α ranging from .70 to .77 for the four domains. The test–retest reliability for each domain ranged from .76 to .80 (Yao et al., 2002).
Statistical analyses
Descriptive statistics were used to summarize participants’ characteristics and scores on primary and secondary outcomes. Independent t-tests were used to examine potential differences in participants’ characteristics, outcome measure scores at baseline, and outcome measure scores in changes (i.e., the differences between post-test and baseline scores). Analyses of covariance (ANCOVAs) were used to examine if the post-test outcome measure scores were significantly different when baseline scores were controlled. Finally, several generalized estimating equations (GEEs) were constructed with adjustments for age and gender to examine if the two groups had significantly different slopes between baseline and post-test scores for any outcome measures. The GEEs were used as intention-to-treat analysis. When a significant interaction effect (i.e., a significantly different slope) between groups (i.e., intervention and control groups) and across time (i.e., baseline and post-test) was identified, it reflected the effects of the Kawa Model based program. All statistical analyses were performed using IBM SPSS 20.0 (IBM Corp, Armonk, NY).
Results
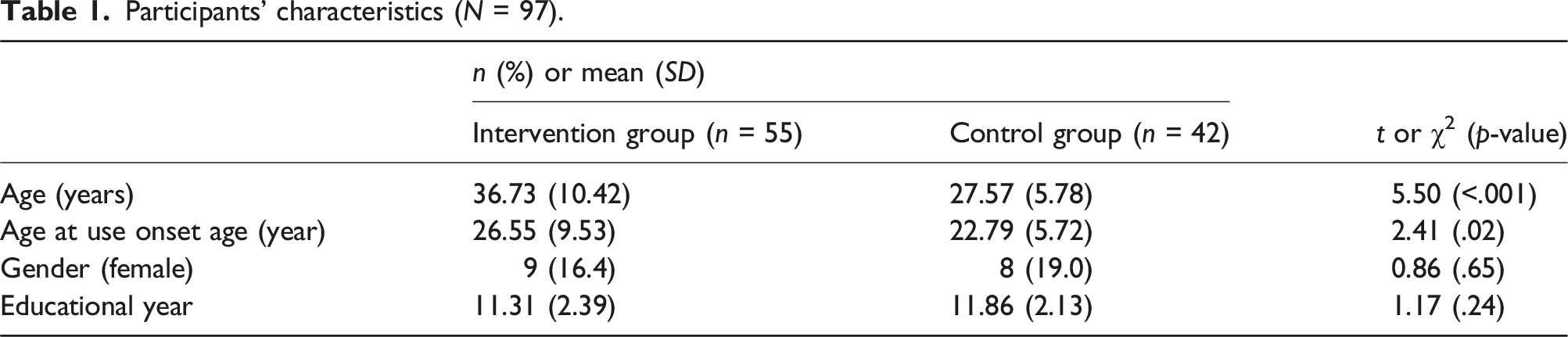
Participants’ characteristics (N = 97).
Outcome variables at baseline between the two groups.
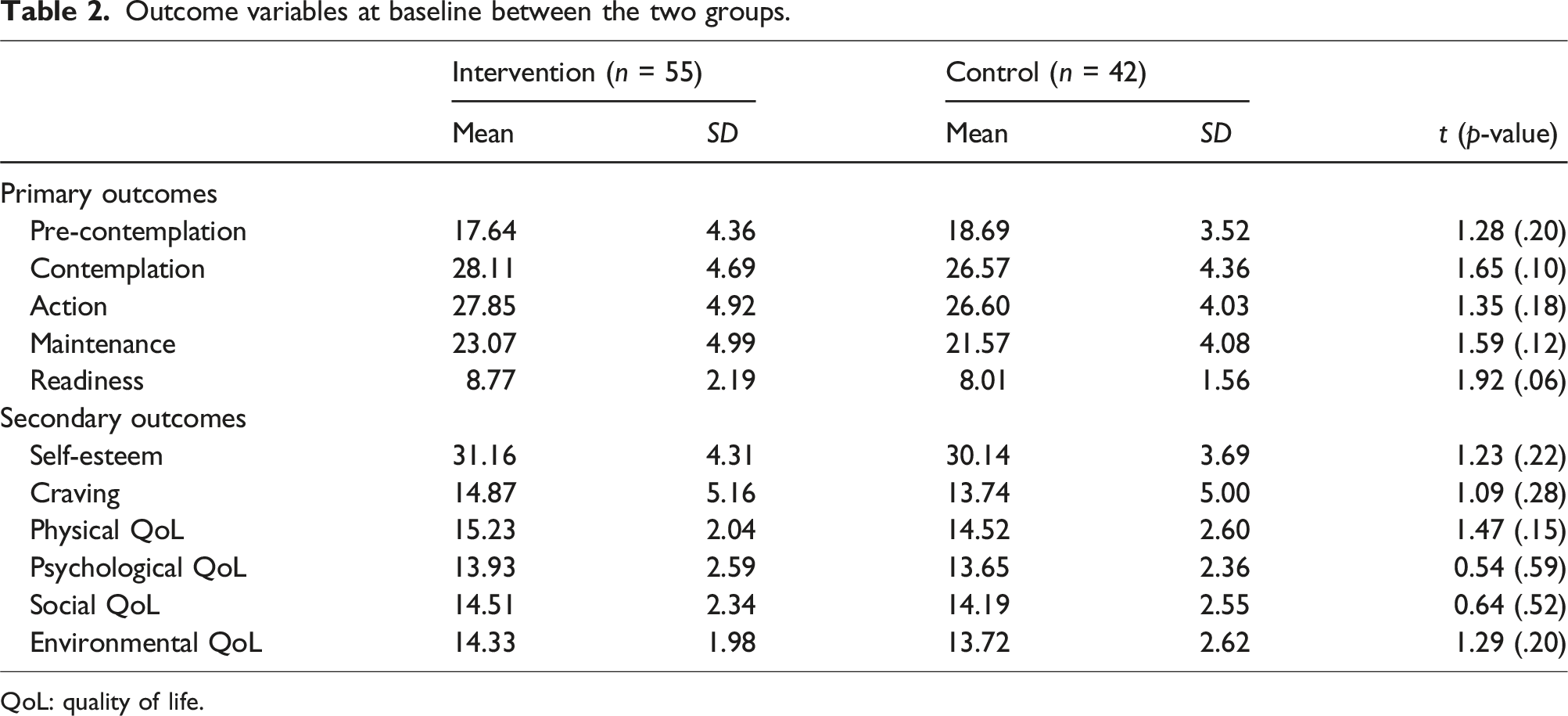
QoL: quality of life.
Outcome variables at post-test and outcome variable changes between the two groups.
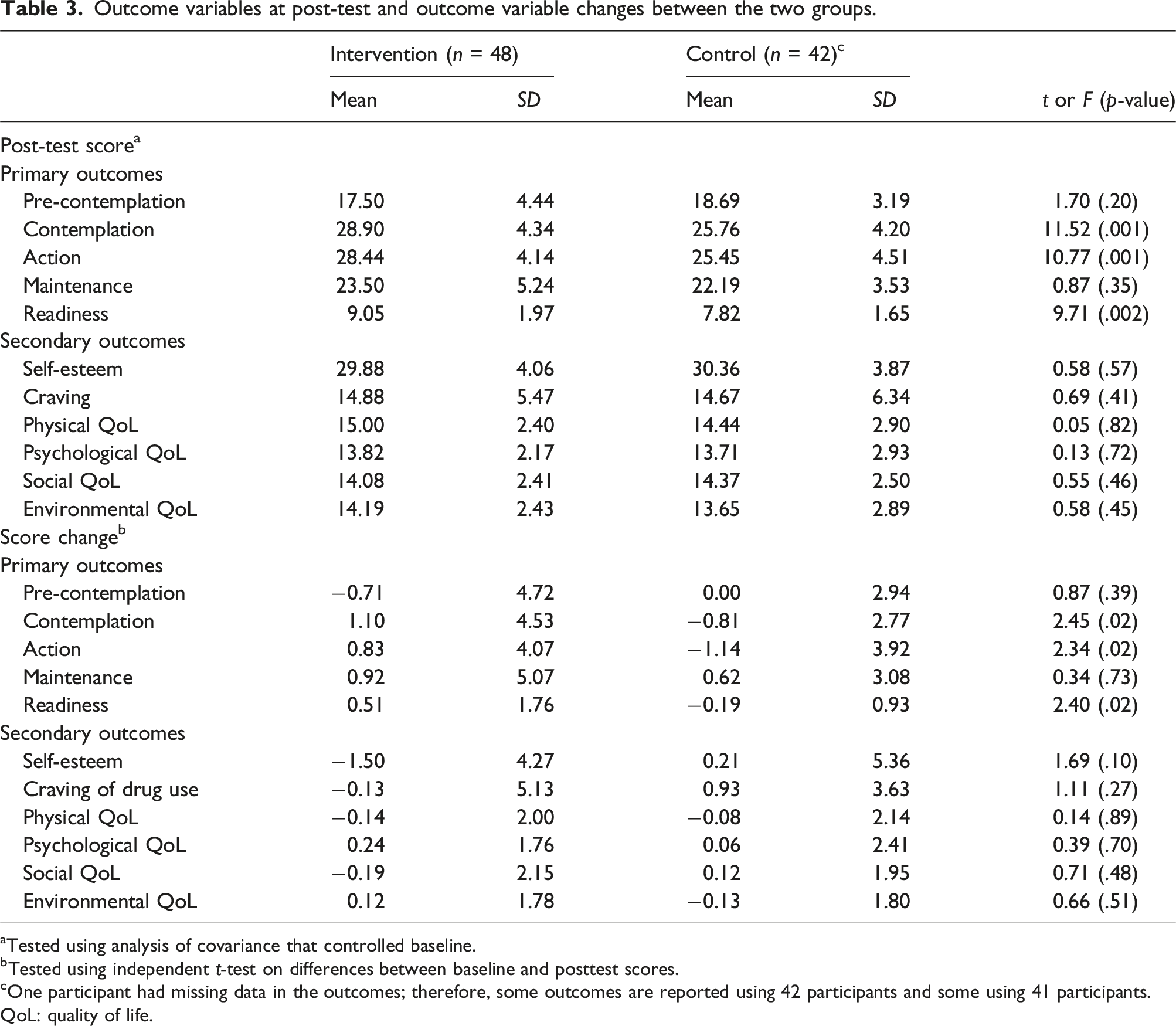
aTested using analysis of covariance that controlled baseline.
bTested using independent t-test on differences between baseline and posttest scores.
cOne participant had missing data in the outcomes; therefore, some outcomes are reported using 42 participants and some using 41 participants.
QoL: quality of life.
Generalized estimating equations in examining the treatment outcomes.
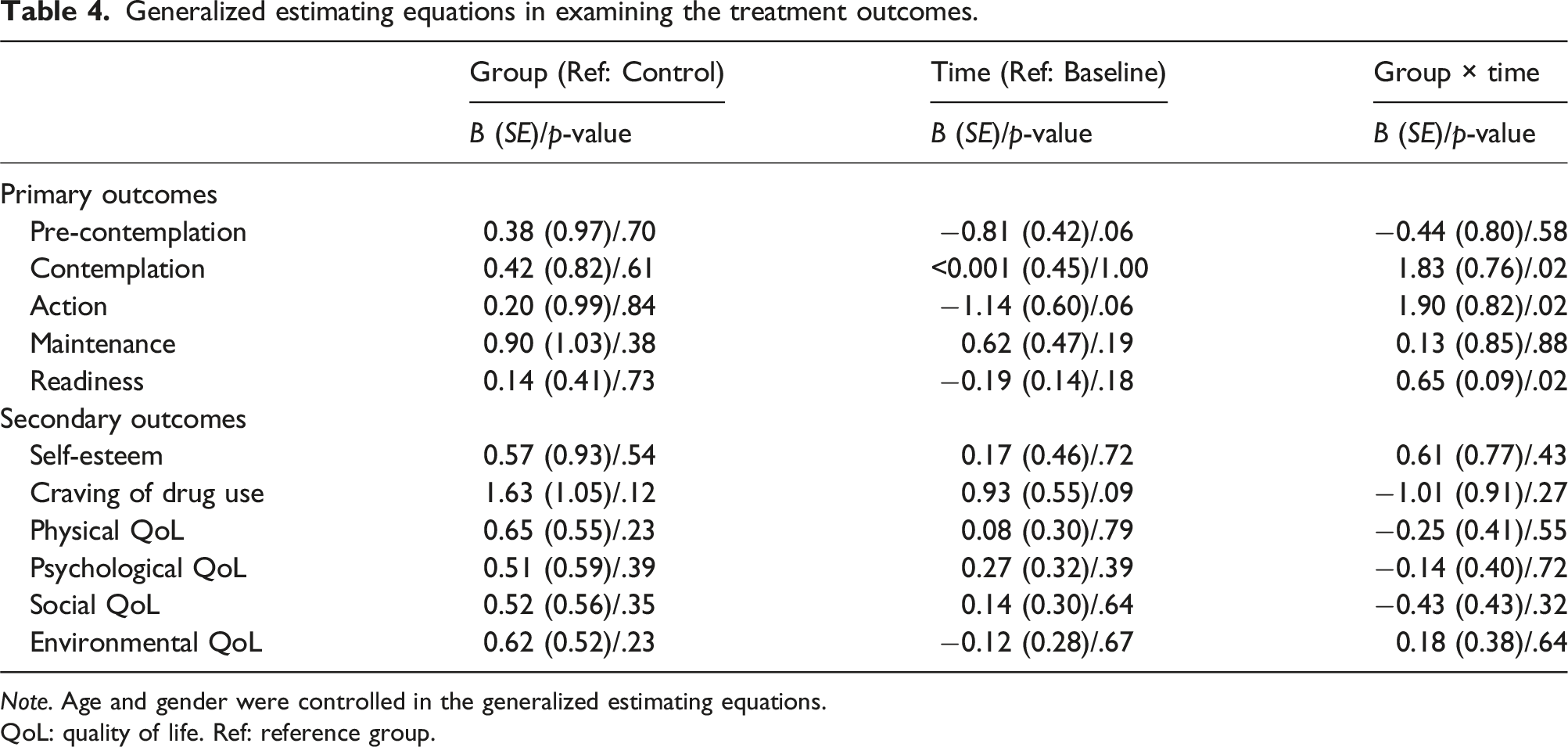
Note. Age and gender were controlled in the generalized estimating equations.
QoL: quality of life. Ref: reference group.
Discussion
Using a quasi-experimental design, the present study showed that Kawa Model therapy could be used to design an effective program to increase readiness for behavioral changes among people with SUDs. Specifically, people with SUDs who received the Kawa Model based therapy after treatment had higher scores on readiness to change in contemplation (identifying their behavioral problems relating to drug use), active (had begun to change drug use behaviors), and readiness (i.e., had prepared for changing drug use behaviors) domains than those who only received psychoeducation (i.e., the control group). However, the present study did not observe any improvements in self-esteem, drug craving or QoL after receiving the Kawa Model based therapy as compared to psychoeducation. Implications are discussed below.
Advanced readiness in stages of change found in the present intervention group could be explained by features of the Kawa Model. Using a river as a metaphor for life in the Kawa Model (Iwama, 2006; Iwama et al., 2009) may increase participants’ motivations to identify, disclose or share information, and subsequently to reflect upon their drug use and related problems. This may improve their understanding towards the negative effects of drug use, which could promote their motivations to quit drug use. Other occupational therapy models, e.g., Model of Human Occupation [MOHO] and Canadian Model of Performance [CMOP]), often address client’s problems with interview questions, observation, and self-report questionnaires (Creek, 2014). All of these contacts are verbal and individual-based, with judgment ratings from good to poor. It is difficult for the healthcare professionals to build rapport and engage with people with SUDs or involuntary clients in a short time, especially in groups. Also, people with SUDs may be hard to be approached using self-reported assessments, especially for those who have not yet developed therapeutic rapport with healthcare professionals. Similar concern is also applied to CMOP (although CMOP and Kawa Model both address person, environment, and occupation participation) as the CMOP was developed under Western culture, with individualism as its core and emphasized more on developing one’s ability (Iwama, 2006).
The client-centered approach in the Kawa Model (Gregg et al., 2015) allows one’s autonomy to make decision on what to draw and what to say. The drawing is different from art therapy or art activities. Specifically, drawing in the art therapy was used as a medium to help participants reveal their emotional conflict or needs. In contrast, the Kawa Model does not use drawing to identify participants’ emotional issues; instead, drawing in the Kawa Model intends to help participants use the metaphoric expression of river as life. Subsequently, drawing in the Kawa Model helps participants develop narratives regarding their life journeys and adaptations. With the river drawing, OTs could help one to explore how his/her river flows and where the density is (life purpose). In summary, use of Kawa Model with river as a metaphor for life circumstances may ease tensions and reduce stigma in people with SUDs while they disclose sensitive information in treatment. Accordingly, people with SUDs in the intervention group appeared more prone to acknowledge their problems related to using drugs. This may motivate acceptance and promote progression through stages of change as shown in the present findings that people with SUDs in the intervention group had higher scores in contemplation, action, and readiness than those in the control group.
However, the present findings did not support the effects of the Kawa Model based therapy on improvements in self-esteem and QoL. Both the intervention and control groups had similar levels of self-esteem and QoL after the programs. The nonsignificant findings could be explained by the following reasons. First, the present study did not implement a full model of the Kawa Model therapy. Conceptually, the first three steps of the Kawa Model were administered parallel to the first three stages of change (Prochaska et al., 1992) including drawing a life river and identifying problems/goals, and the interventions for changing problems are included in later steps. Due to the pragmatic issue, the present study could only conduct the first three steps of the Kawa Model therapy instead of a six-step Kawa Model therapy (Iwama, 2006; Ober et al., 2022). Specifically, the programs received by either the intervention or control group were supported by government resources that funded only 8 hours of intervention. Therefore, the incompleteness of the Kawa Model based therapy may lead to limited outcomes. Additional treatment beyond the 8-h group might be needed to induce treatment effects on health-related measures. Second, health improvements may occur considerably following drug cessation (Manning et al., 2019). Therefore, people with SUDs may observe health improvements after a more prolonged period of follow-up. Given that the present study did not assess longer-term follow-up outcomes, it is possible that some health-related changes might have occurred later. In brief, Kawa Model is based on the Eastern philosophy and has been applied to occupational therapy process in Asian as well as in Europe (Hsiao et al., 2023; Iwama et al., 2009; Janus, 2017; Tripathi et al., 2017). It has been proved as a culturally responsive model that uses visual creations as a tool for self-expression. Unlike other therapies (e.g., cognitive-behavioral therapy), the Kawa Model does not specifically target outcomes like craving. As such, the Kawa Model based therapy may have synergistic effects with other therapies, and this should be examined in future studies.
This study has a few limitations. First, this study was not a randomized controlled trial. Participants registered for the two programs by their time preference without knowing the contents of the program in advance. That may minimize the selection bias to the effect of treatment. However, unequal group size could still confound the present findings. For example, people with SUDs who chose to attend the small-group intervention group might have had higher levels of motivation to change their drug use behaviors (even though baseline URICA measures were comparable across groups) due to more individual attention and personal interaction, and this might have led to overestimation of intervention effects. Second, although both groups received equal amounts of time in treatment (i.e., 8 hours in total for each group), the arrangements of the eight-hour programs were different. The intervention group received four sessions across four weeks with each session lasting 2 hours; the control group received one eight-hour session of lecture. Therefore, the intervention group might have had more time to reflect on the information they received from their eight-hour Kawa Model based therapy, whereas the control group might have fatigue and could not fully absorb information from the single-session, eight-hour program. Third, the present study did not have follow-up assessment, therefore, the longer-term effects of the Kawa Model based therapy were not examined. Specifically, it is unclear if the treatment effects found in the Kawa Model based therapy might be maintained over time. Fourth, the participants were mandated for treatment in Taiwan. The extent to which the findings extend to other conditions such as voluntarily seeking treatment, or from other jurisdictions/cultures warrants examination. Fifth, the individuals had a mixture of SUDs (mainly involving ketamine and amphetamines). The extent to which the findings extend to people with other SUDs is worth to explore in future. Sixth, co-occurring disorders and other possible treatments (e.g., medications) were not assessed, and the potential presence and impact of these should be considered in future studies. Lastly, all measures were self-reported. Therefore, social desirability and other biases warrant consideration.
Conclusion
The present study demonstrated initial and preliminary findings that the Kawa Model based therapy promoted readiness for changing drug use behaviors in people with SUDs. However, our study did not conduct the full program of the Kawa Model based therapy, i.e., only the first three steps of the six-step in the model were implemented. Therefore, future studies should directly evaluate the efficacy of the full 6-steps Kawa Model based therapy in the form of randomized controlled trials involving people with SUDs. Given the promising preliminary results, healthcare professionals in the mental health field may consider adopting the Kawa Model based therapy when treating people with SUDs.
Footnotes
Author’s note
Dr Potenza discloses the followings. He has served as a consultant or adviser for Opiant/Lakelight Therapeutics, Idorsia, AXA, Addiction Policy Forum, Game Day Data, and Baria-Tek and has served as a consultant for legal and gambling entities on issues related to impulse control disorders; he has been involved in a patent application between Novartis and Yale; he has received research support from Mohegan Sun Casino and the Connecticut Council on Problem Gambling; he has edited journals and journal sections and has given academic lectures in grand rounds, CME events, and other clinical or scientific venues; and he has generated books or book chapters for publishers of mental health texts.
Author contributions
H-Y H—Conceptualization; Methodology; Software; Validation; Investigation; Resources; Data curation; Writing-Original draft; Writing-Review & editing; Visualization; Project administration; Funding acquisition. T-Y W—Conceptualization; Methodology; Software; Validation; Investigation; Resources; Writing-Original draft; Writing-Review & editing; Visualization; Supervision; Project administration; Funding acquisition. C-H L—conceptualization; Validation; Investigation; Resources; Data curation; Writing-Review & editing; Visualization; Project administration; Funding acquisition. Y-C L—methodology; Validation; Resources; Data curation; Writing-Review & editing. Y-C H—Methodology; Validation; Resources; Data curation; Writing-Review & editing. Y-C C—Methodology; Validation; Resources; Data curation; Writing-Review & editing. MN. P—Methodology; Validation; Writing-Review & editing. C-Y L—conceptualization; Methodology; Software; Validation; Formal analysis; Writing-Original draft; Writing-Review & editing; Visualization; Supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the Jianan Psychiatric Center Research Grant 2015-D04.
Data availability statement
The data that support the findings of this study are available on reasonable request from the corresponding author, T-YW.