
Abstract
Aim
This study aimed to investigate the association between occupational participation and depressive symptoms among middle-aged adults in Hokkaido, Japan.
Methods
Community-dwelling adults aged 40–64 years were recruited using snowball sampling, and 165 participants who returned the questionnaires and met the selection criteria were included in the analysis. Depressive symptoms were assessed using the Center for Epidemiologic Studies Depression (CES-D) scale. Occupational participation, including three domains (leisure, productivity, and self-care) and three aspects (occupational control, occupational balance, and satisfaction of performance), was assessed using Self-completed Occupational Performance Index (SOPI) questionnaire.
Results
Multivariate-adjusted regression analysis revealed that depressive symptoms were associated with lower occupational participation in the productivity domain (β = −0.34, p < .001), whereas analysis of each aspect of the SOPI showed a significant association of depressive symptoms with lower occupational control in productivity domain (β = −0.33, p < .001), occupational balance in productivity domain (β = −0.25, p < .001), and satisfaction with performance in leisure domain (β = −0.16, p = .045) and productivity domain (β = −0.35, p < .001).
Conclusion
Depressive symptoms was significantly associated with low occupational participation in productivity domain in middle-aged adults. In the domains of leisure and self-care, significant associations were found only between depression symptoms and satisfaction of performance. Occupational therapy interventions for middle-aged adults targeting the maintenance and improvement of participation in productive activities may help preventing depressive symptoms.
Introduction
According to the World Health Organization (WHO), depression is a commonly occurring mental disorder worldwide, and 3.8% of the global population is currently experiencing or has previously experienced depressive episodes (WHO, 2023). The prevalence of depression increased by 18.4% (>300 million individuals) from 2005 to 2015 (WHO, 2017), reflecting the overall global population growth and a proportionate increase in the age groups with a higher prevalence of depression. In Japan, an estimated 3,256,955 (2.7%) people were diagnosed with depressive disorders in 2019 according to the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) (Global Burden of Disease Study 2019 Result, 2020). By age group, the prevalence rates in the 40s and 50s age groups are 2.9% and 2.8%, respectively (Global Burden of Disease Study 2019 Result, 2020), indicating that the prevalence is higher in the middle-aged groups than in the other age groups.
According to Erikson’s theory on psychosocial development, middle-aged adults who are not productive and nurturing, with no interest in the next generation, can lose sight of the meaning of their lives (Erikson, 1979). Studies based on Erikson’s theory have shown that ego integration contributes to a reduction in depressive symptoms and improvement in indicators of well-being (Darling-Fisher, 2019; Westerhof et al., 2017). To prevent depression, focusing on subthreshold depression, which does not meet the criteria for depression but is characterized by the presence depressive symptoms, is important (Herrman et al., 2022; Zhang et al., 2023). According to previous studies, subthreshold depression leads to lifetime suicide attempts (An et al., 2022), major depression (Zhang et al., 2023), and increased mortality (Cuijpers & Smit, 2002). However, these studies have not clarified which lifestyle behaviors are associated to depressive symptoms, including subthreshold ones, in middle-aged adults.
Previous studies investigated psychosocial interventions for preventing depressive symptoms. Meta-analyses have indicated that interventions such as cognitive behavioral therapy, problem-solving therapy, and psychoeducation have been able to prevent depression at a statistically significant level, with a modest effect size (Conejo-Cerón et al., 2017). Although in some circumstances professional intervention is not possible, coordinating one’s own activities and participation in life events is crucial. For middle-aged adults, physical and leisure activities have been associated with positive mental health, including the reduction of negative mood for psychological distress (Kekäläinen et al., 2020; Takeda et al., 2015). Besides carrying out an activity, receiving recognition from others as part of social support could effectively improve depressive symptoms (Israel et al., 2022). Furthermore, increased social activity is negatively correlated with depressive states, and interrelationships with others are important for middle-aged adults (Nakamine et al., 2017). In addition, job satisfaction (Liu et al., 2023) and environmental components such as workplace harassment, psychological safety, and support from colleagues (Shiga et al., 2022) significantly affect depressive symptoms. Conversely, depression is associated with loss of work productivity, even in cases where a diagnosis has not yet been made (Asami et al., 2015). Therefore, participation in leisure and social activities has been shown to be negatively associated with depressive symptoms. Furthermore, since depressive symptoms and related factors have been reported to be dependent on age, sex, family structure, education level, employment status, and health status (Best et al., 2021; Cohen et al., 2020; Infurna et al., 2020), studies should also include the analysis of demographic information.
Occupational therapy for health promotion focuses on the management of daily life performance. The Canadian Model of Occupational Performance (CMOP) promotes client-centered practice that focuses on the interactions among the person, environment, and occupation to enhance occupational performance (Canadian Association of Occupational Therapists, 1997; Townsend & Polatajko, 2007). In this model, occupations are divided into three domains: leisure, productivity, and self-care. Occupational participation refers to an individual’s ability to engage in meaningful activities with self-control while balancing other activities and with a sense of satisfaction (Canadian Association of Occupational Therapists, 1997; Imai & Saito, 2010). Previous studies have reported a negative association between participation in leisure and social activities and the depressive symptoms (Fukita et al., 2021; Luo, 2011; Nakamine et al., 2017) but did not examine perspectives on engaging in meaningful activities based on the CMOP, such as self-control, balancing, and sense of satisfaction. Such research is relevant given the hypothesized association between productive activity, which is said to play an important fluidity in parenting, caregiving, and paid work, and depressive symptoms (Infurna et al., 2020; Wister et al., 2022). Identifying their relationships may be important when considering forms of occupational participation in preventive occupational therapy for mental health. Therefore, not consequently, this study aimed to investigate the association between occupational participation and depression in middle-aged adults in Hokkaido, Japan.
Methods
Research design
This study used a cross-sectional design and an anonymous self-administered questionnaire. Data were collected from July to November 2022.
Participants
The participants were adults aged 40–64 years old residing in Hokkaido, Japan, and were recruited using snowball sampling; potential participants were predominantly parents of undergraduates and their friends or colleagues at a university. The exclusion criteria were age <40 or ≥65 years old and history of central nervous system disease or mental illness. The estimated sample size for generating a medium effect size was 114, with alpha type I error rate = 0.05, power = 0.80, and effect size = 0.15, based on the results of previous studies (Kekäläinen et al., 2020; Luo, 2011; Shiga et al., 2022). When a pilot study was conducted with the parents of undergraduates using snowball sampling, the response rate was estimated to be 60%. Therefore, the questionnaire needed to be distributed to more than 190 people.
Measurements
Depressive symptoms
Depressive symptoms were screened using the Japanese version of the Center for Epidemiologic Studies Depression (CES-D) (Shima et al., 1985), which is an internationally used scale for assessing the degree of depressive symptoms (Radloff, 1977). The CES-D comprises 20 items that assess the frequency of depressive symptoms, using negative or positive questions that are scored according to the duration of symptoms as 0 (for <1 day), 1 (for 1–2 days), 2 (for 3–4 days), and 3 (for 5–7 days) in the past week. The total score is 0–60 points, with higher scores indicating higher levels of depressive symptoms. The cut-off point for the CES-D was 15/16, where a total score of 16 or higher indicates that the participant has depressive symptoms, with a sensitivity of 88.2% and specificity of 84.8%. The CES-D has shown good concurrent validity in relation to other depression scales and high reliability in the test-retest and split-half methods (Shima et al., 1985). To address the issue of missing data on the CES-D, imputation methods including item and person averaging, were performed, resulting in CES-D scores that were similar to those obtained from participants with no missing data (Bono et al., 2007).
Occupational participation
Occupational participation was assessed using the Self-completed Occupational Performance Index (SOPI) (Imai & Saito, 2010), which was based on the framework of the CMOP (Canadian Association of Occupational Therapists, 1997; Townsend & Polatajko, 2007). The SOPI consists of nine items, including three related to occupational participation (occupational control, occupational balance, and satisfaction of performance) in three domains (leisure, productivity, and self-care). Occupational control indicates that the participant decides for him/herself when and how to perform the activity. Occupational balance indicates that participants balance the time and energy spent on the activity per his/her life. Satisfaction of performance indicates that the participant actually performs the activity competently. The SOPI assessed occupational participation in the past month using a 5-point Likert scale (1 = not satisfied at all, 5 = highly satisfied). The example question was “Whether you can decide on your own activities in the leisure of the past month.” The SOPI showed good construct validity and relationship with the health-related quality of life and high reliability, with a Cronbach’s α of 0.93 (Imai & Saito, 2010).
Demographic information
Demographic data, including age, sex, family composition, education level, employment status, and health status, were collected using questionnaires. The education level was stratified as high school graduate or higher education. Family composition was determined by a yes/no response to the question, “Do you live with your child/children?” Employment status was defined as employed (full-time or part-time) or unemployed. Health status was ascertained by a yes/no answer to the question, “Do you have any chronic diseases such as hypertension, diabetes, heart disease, stroke, liver disease, cancer, etc.?” (Epidemiology and Prevention Division & National Cancer Center, 2010).
Statistical analysis
First, participant characteristics were calculated as mean and standard deviation (SD) for continuous variables and as frequency and proportion (%) for categorical variables. Second, Spearman’s correlation analysis was performed to clarify the relationship between the CES-D and SOPI. Third, a hierarchical multiple regression analysis was performed with the CES-D total score as the dependent variable and demographics (age, sex, family composition, educational level, employment status, and health status) as the independent variables in Step 1. Next, the three domain scores of the SOPI were input as the independent variables in Step 2. Then, additional multiple regression analysis was conducted to clarify the association between CES-D and each domain of the three aspects of the SOPI (occupational control, occupational balance, and satisfaction of performance) because Spearman’s coefficients for the correlation between the items of the three aspects in one domain were high (ρ = 0.77-0.83). Therefore, a multiple regression analysis was conducted with CES-D as a dependent variable and SOPI and the covariates as independent variables, using Model 1 with the occupational control in three domains, Model 2 with the occupational balance in three domains, and Model 3 with the satisfaction of performance in three domains. The covariates included age, sex, family composition, educational level, employment status, and health status. SPSS version 27.0 (IBM Inc., Armonk, NY, USA) was used for all analyses, and the significance level was set at 0.05.
Ethical considerations
This study was approved by the Sapporo Medical University Ethical Review Board (approval number 3-1-73). Consent was obtained by reading the written research instructions and by answering and posting the questionnaire sheet. The participant’s anonymity was consistently preserved. This study adhered to the Declaration of Helsinki.
Results
Participants Characteristics (n = 165).
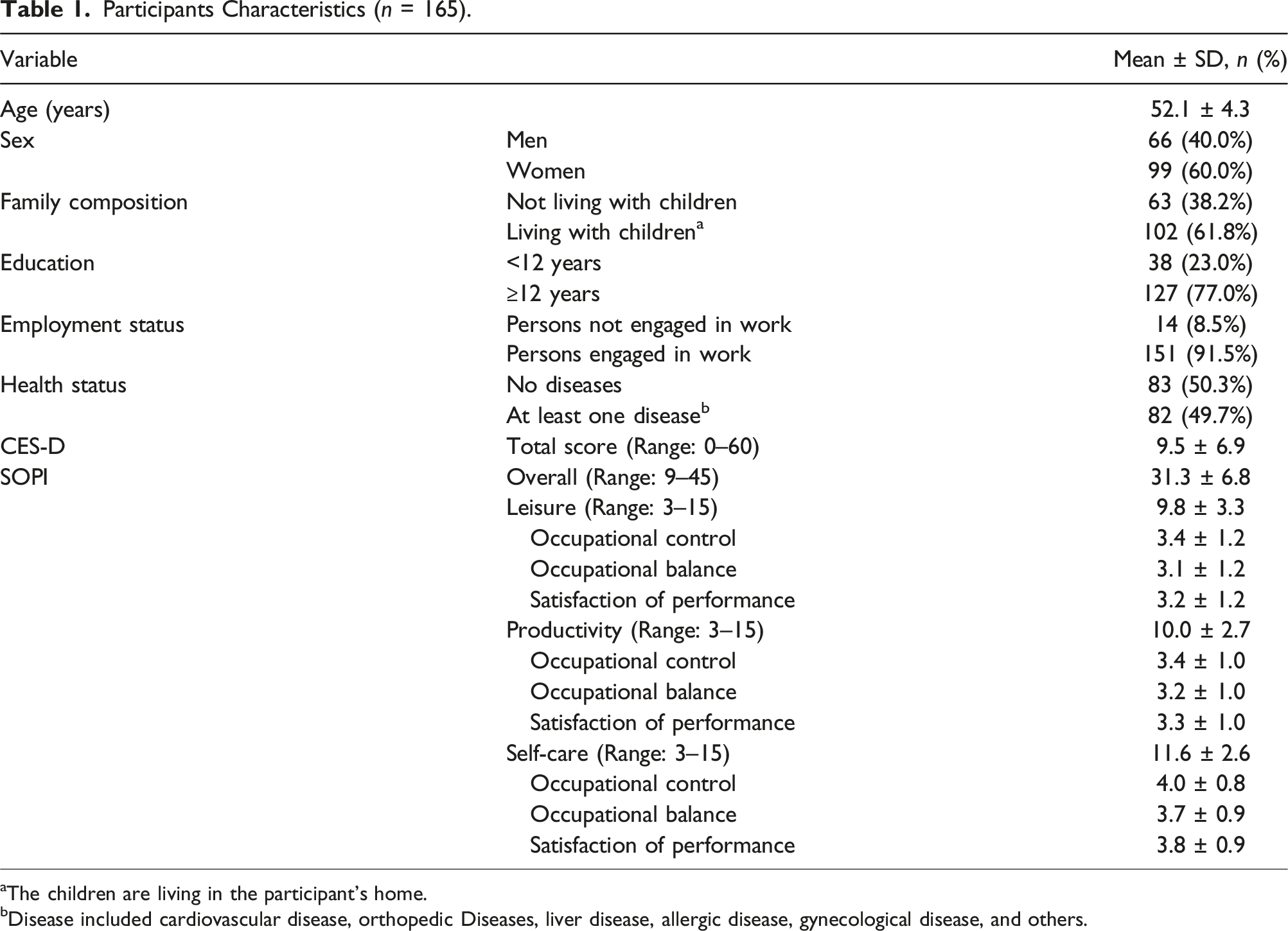
aThe children are living in the participant’s home.
bDisease included cardiovascular disease, orthopedic Diseases, liver disease, allergic disease, gynecological disease, and others.
The Correlations Between SOPI and CES-D.
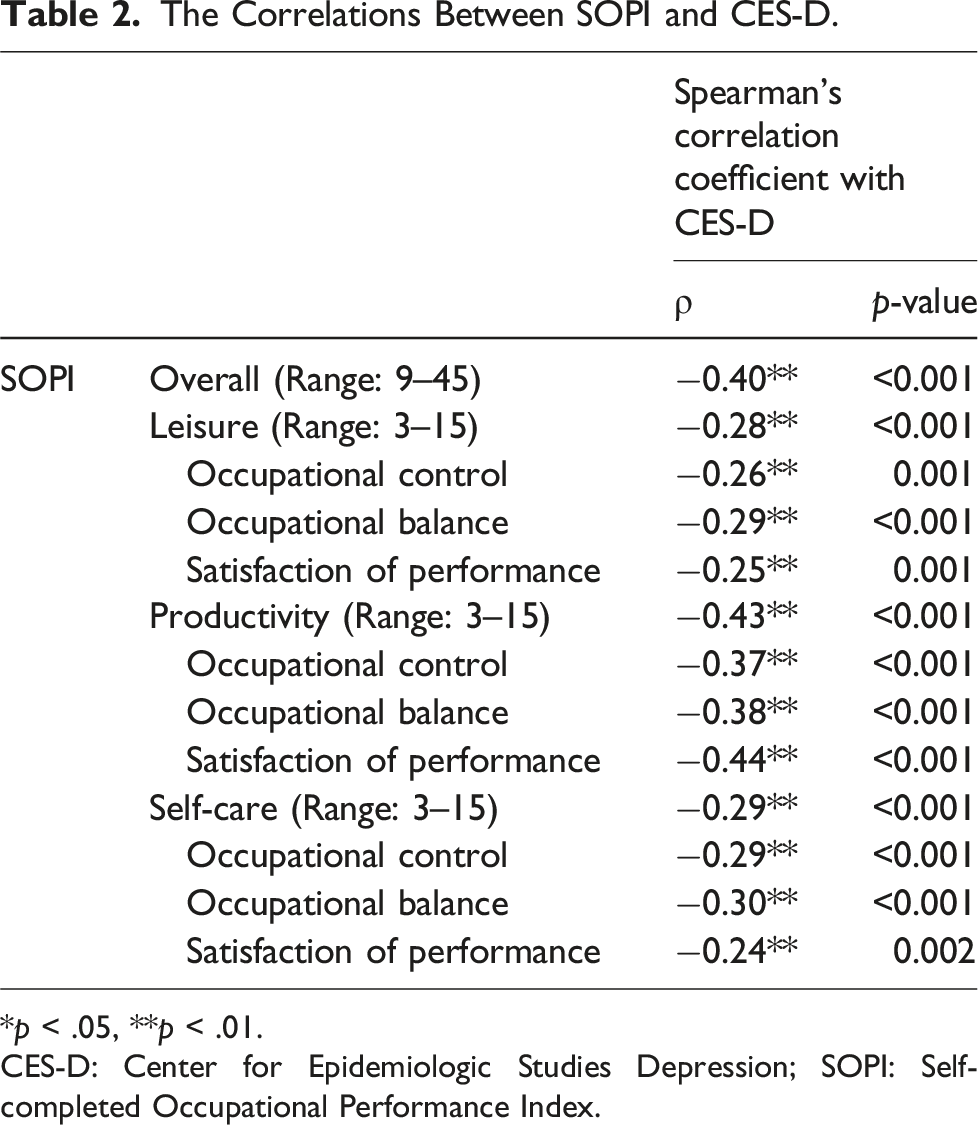
*p < .05, **p < .01.
CES-D: Center for Epidemiologic Studies Depression; SOPI: Self-completed Occupational Performance Index.
Hierarchical Multiple Regression Model for Depressive Symptoms According to Occupational Participation.
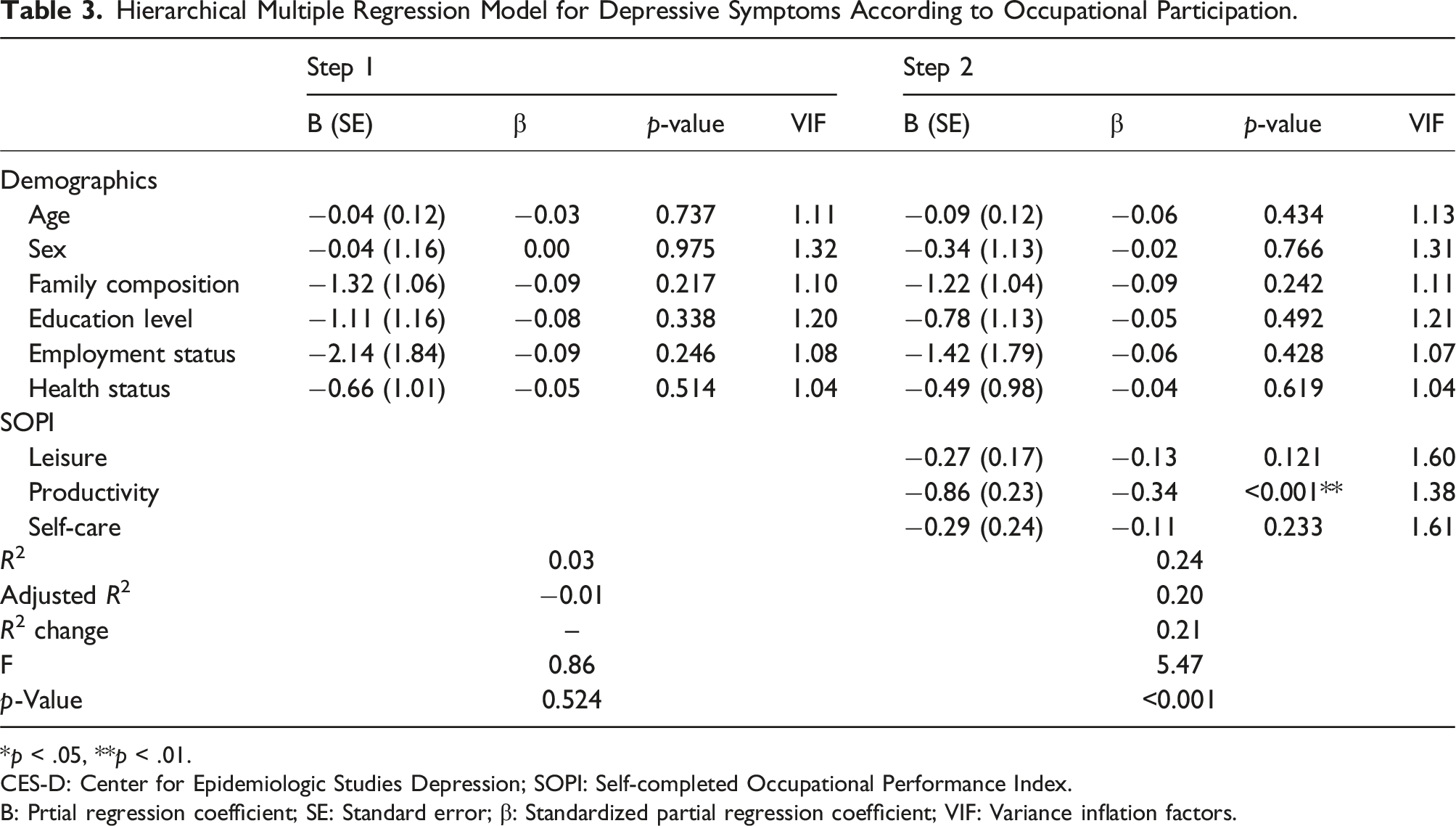
*p < .05, **p < .01.
CES-D: Center for Epidemiologic Studies Depression; SOPI: Self-completed Occupational Performance Index.
B: Prtial regression coefficient; SE: Standard error; β: Standardized partial regression coefficient; VIF: Variance inflation factors.
Multiple Regression Model for Depressive Symptoms According to the Aspects of Occupational Participation.
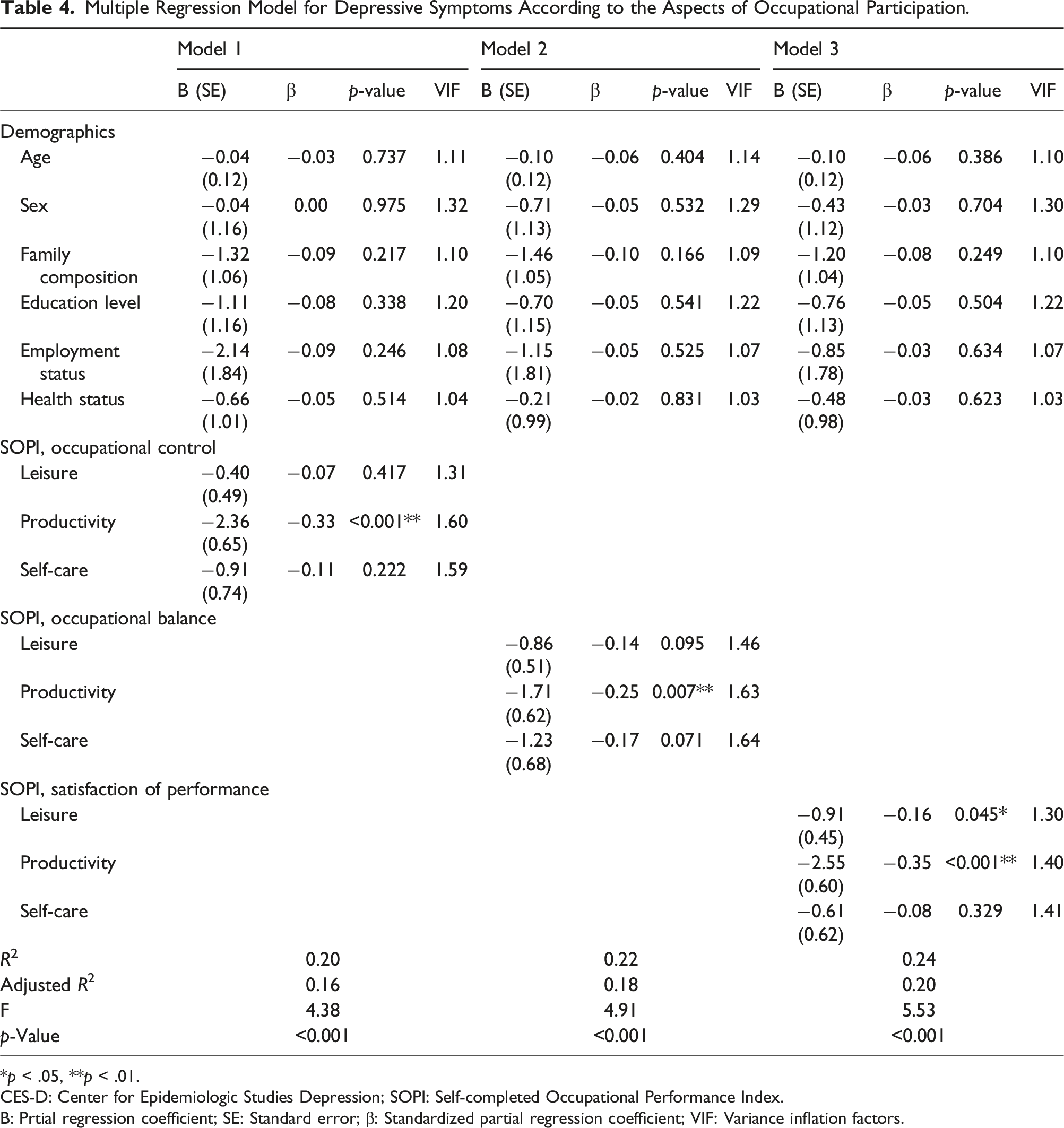
*p < .05, **p < .01.
CES-D: Center for Epidemiologic Studies Depression; SOPI: Self-completed Occupational Performance Index.
B: Prtial regression coefficient; SE: Standard error; β: Standardized partial regression coefficient; VIF: Variance inflation factors.
Discussion
This study examined the association between occupational participation and depressive symptoms among middle-aged adults in Hokkaido, Japan. Regarding occupational participation, the SOPI, based on the COMP, was used to assess the factors related to engagement in meaningful activities (Imai & Saito, 2010). Using the SOPI to examine the association with depressive symptoms, it is possible to examine which aspects of occupational participation may provide clues for countermeasures. The mean CES-D score of the participants in this study was 9.5, which is a low score compared to the previously reported scores of 14.8 for those in their 40s and 13.8 for those in their 50s in the general Japanese population (Tomitaka et al., 2016). The mean SOPI score was 31.3, which was slightly lower than the 35.2 score in a previous study on middle-aged and older adults (Imai & Saito, 2010). The study was conducted during the COVID-19 pandemic in 2022, and this may have contributed to the lower scores, considering the restriction of various activities as the number of infected individuals increased.
Occupational participation in productivity, but not leisure or self-care, was significantly associated with depressive symptoms in this population. According to Erikson’s “Stages of Psychosocial Development”, the middle-aged stage comprises generativity that refers to concern for the future, need to nurture and guide younger people, and desire to contribute to the next generation (Erikson, 1979), indicating that activities that contribute to others and society could help meet the needs of middle-aged individuals. The results of this study support this theory, as the results show a significant association between occupational participation in productivity and depressive symptoms. Productive activities include working, housework, childcare, and other endeavors that contribute to social or economic well-being and have a positive effect on living a meaningful life (Imai, 2016). However, social responsibilities are the greatest in labor and childcare (Ministry of Health, & Labour and Welfare, Japan, 2006), which can also be a stressor that is associated with poor mental health (Infurna et al., 2020; Yang et al., 2020). Therefore, it is important for middle-aged adults to identify the productive activities they engage in daily and engage in productive activities while controlling any excessive stressors that may be caused by engaging in these activities to counteract the depressive symptoms.
Based on the analysis of occupational participation (occupational control, occupational balance, and satisfaction of performance), all aspects of productivity were significantly associated with depressive symptoms. Currently, in Japan, work−life balance (WLB) has been proposed in response to the problems of balancing work and life, such as “suffering from health problems due to physical and mental fatigue at work” and “difficulties in balancing work and childcare” (Cabinet Office, 2008). WLB refers to one’s ability to fulfill one’s professional responsibilities with a sense of satisfaction while simultaneously being able to choose and realize diverse ways of living at each stage of life, including family and community life (Cabinet Office, 2008). WLB has a mediation effect on the associations between workaholism and depressive symptoms (Yang et al., 2020). These concepts of WLB are included in the three aspects of occupational participation, and the results of this study support the promotion of WLB among middle-aged adults. Therefore, it is important to monitor which of the three aspects of occupational participation in productive activities cause barriers and distress to undertake countermeasures against depressive symptoms.
Furthermore, the results revealed that satisfaction with leisure activities was negatively associated with depressive symptoms. These findings suggest that the implementation of satisfactory leisure activities is associated with lower depressive symptoms. Leisure-time physical activity (Kekäläinen et al., 2020), hobbies (Fukita et al., 2021), leisure satisfaction, and meaningfulness (Luo, 2011) are negatively related to depressive symptoms. While a wide variety of leisure activities can be effective against depressive symptoms (Fukita et al., 2021; Kekäläinen et al., 2020), whether middle-aged adults find these activities satisfactory depends on individual perspectives. Therefore, identifying the types of leisure activities that are more satisfactory and then incorporating them into daily life are likely to be related to strengthening positive moods and countering depressive symptoms.
Limitations
This study had several limitations. First, the results of this study cannot establish a causal relationship between improving occupational participation and preventing depressive symptoms because this was a cross-sectional study that used snowball sampling conducted in a specific region of Japan. Second, the data on employment status were collected as it relates to the context of productivity, but not on economic factors (e.g., income and mortgage) that are associated with employment status in Japan (Honjo et al., 2020; Nishikitani et al., 2022; Statistics Bureau of Japan, 2022). The results may differ when other covariates are included in the multivariable model. Third, based on previously reported methods, occupational participation was measured using a questionnaire; therefore, the specific life activities assumed by the participants in each area may differ. The association between specific activities and depressive symptoms is unclear. Furthermore, longitudinal studies are required to clarify the meaningful activities by interviewing instead of a self-reported questionnaire and the association between those activities and mental health, including depression in middle-aged adults over a broad range of areas.
Conclusion
This study investigated the association between occupational participation and depressive symptoms among middle-aged adults in Hokkaido, Japan. Depressive symptoms were significantly associated with low occupational participation in the productivity domain but not in the leisure and self-care domains. Furthermore, depressive symptoms were significantly associated with all aspects of the SOPI in the productivity domain as well as satisfaction of performance in the leisure domain. However, this finding requires further clarification through longitudinal studies. Preventive and rehabilitative services for middle-aged adults should consider developing strategies for depressive symptoms by supporting occupational participation in productive activities, such as contributing to social or economic well-being, employment, household chores, childcare, and volunteer activities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Sapporo Medical University and received no grant from any funding agency in other sectors.