
Abstract
Breast cancer is the most prevalent malignant disease in women worldwide, accounting for 24% of new cancer cases and 15% of cancer-related deaths in 2018 (Heer et al., 2020). Overall 5-year survival from breast cancer is, in more developed regions, well over 80%, while in other regions, like India or South Africa, is reported as less than 70% and than 50%, respectively (Wilkinson & Gathani, 2022). Breast cancer has numerous physical, psychological and social repercussions, affecting professional performance and limiting participation in self-care, work, and leisure activities, decreasing health-related quality of life (HRQoL) (Hwang et al., 2015; Kasven-Gonzalez et al., 2010; Lai et al., 2021; Nascimento et al., 2019). The process, from detection and diagnosis to treatment and subsequent follow-up, negatively impacts occupational performance, disrupts daily life and reduces the HRQoL of individuals diagnosed with breast cancer (Baxter et al., 2017; Fernández Machado, 2014; Keesing et al., 2018).
Despite the increase in cancer survival rates and the need to develop new intervention strategies that address the occupation needs and daily functioning of patients, there are still few studies addressing this issue in occupational therapy (OT) (Lozano-Lozano et al., 2023; Sleight & Duker, 2016). The perceived needs of breast cancer survivors are a predictor of HRQoL, with unmet needs exerting a greater impact than the sociodemographic or clinical characteristics of the individuals (Lam et al., 2011; Park & Hwang, 2012). Principal needs of women with recurrent breast cancer, can be categorized as follows: (1) healthcare system and information needs, such as being informed about recovery options, minimizing waiting times for clinical appointments, timely communication of test results and having access to healthcare staff members for discussions about the disease, treatment and follow-up; (b) psychological needs, mainly related to concerns of cancer recurrence and fears of physical disability or deterioration; and (3) patient care and support, including being treated as individuals rather than just another case (Park & Hwang, 2012). Additionally, breast cancer survivors have reported other difficulties in resuming meaningful roles and activities they had before their diagnosis (Keesing et al., 2018).
OT is effective in improving the HRQoL of individuals with breast cancer through assessing occupational roles to enhance significant occupational performance and modifying lifestyles habits (Dilworth et al., 2014). Specifically, it improves functionality, participation, and reduces cancer-related distress through guided relaxation programs and anxiety management (Sleight & Duker, 2016). Therefore, cancer patient care models propose incorporating the detection of functional limitations (Cheville et al., 2011) to enhance the quality of life in these patients, such as the disability-driven cancer rehabilitation model (Silver & Gilchrist, 2011) and the prospective surveillance model (Stout et al., 2012). In this regard, occupational therapists could assess and develop interventions considering the patient’s context and environment to increase and improve their participation in activities. They focus on developing skills necessary for carrying out different adaptations, modifying daily activities or occupations, and optimizing the patient’s performance and quality of life (Lai et al., 2021). OT interventions also address physical sequelae, including lymphedema, pain, fatigue, cognitive decline, and psychosocial deficits resulting from cancer (Muñoz-Alcaraz et al., 2022). Occupational therapists can implement family education programs, enhance skills for returning to work, and conduct home assessments, among other interventions like stress management, cognitive stimulation, or socioemotional support ((Lai et al., 2021; Longpre, 2011; Sleight & Duker, 2016).
Information and communication technology (ICT) is a resource used to enhance health, well-being and functional capacity. The development and widespread adoption of ICT can be considered a significant social phenomenon in recent years. The progressive integration of technological devices into our daily lives is an emerging reality, especially in developed countries (Fagnilli & Farias, 2011; Lozano-Lozano et al., 2019; Ramsten et al., 2020). Advances in ICT applied to healthcare are starting to transform the traditional methods used by health professionals and have the potential to completely revolutionized practices in the future, particularly due to the impact on the demand for healtcare services (Gathercole et al., 2021; Lai et al., 2021; Sánchez Rodríguez et al., 2018). Technological developments offer healthcare an opportunity to provide more personalised, participatory and preventive services (Ministerio de Sanidad, 2021). Occupational therapists can leverage new technologies to achieve therapeutic goals, promoting personal autonomy across various aspects of individuals’ lives and enhancing their HRQoL (Resta et al., 2021). For example, smartphones or smartwatches can serve as reminders for activities and provide guided instructions for individuals with mental disabilities (Gathercole et al., 2021; Resta et al., 2021). Telecare systems can assist people with dementia (Gathercole et al., 2021), and technology can be applied in rehabilitation programs for individuals with heart failure (Dalal et al., 2021). Technology can be used to assist a variety of patients with performing activities of daily living. For instance, people with dementia who can initially follow simple instructions can benefit from monitoring their activity, receiving reminders to complete tasks, or being encouraged to carry out additional ones like taking their medications, having a shower, having breakfast, or walking. Technological support can be considered a promising strategy to improve treatment outcomes, follow-up, and monitoring, ultimately enhancing the HRQoL of women with breast cancer (Lozano-Lozano et al., 2016; Roldán Jiménez, 2017). Low adherence to healthy lifestyles has been observed among women with breast cancer, according to clinical practice guidelines (Kelly et al., 2020). Thus, future interventions should aim to develop effective strategies that promote healthy lifestyles (Demark-Wahnefried et al., 2015).
ICT includes mobile devices in the form of mobile applications (App), which can be utilized as complementary tools in telehealth to provide clinical services by connecting clinicians with clients for purposes such as assessment, intervention or consultation (Lai et al., 2021; «Telehealth in Occupational Therapy», 2018). The healthcare category encompasses approximately 97,000 Apps, positioning it as the third fasted-growing category after games and general applications (Sánchez Rodríguez et al., 2018). To the best of our knowledge, there is currently no App specifically designed to address the functioning and participation in daily life based on the perceived needs of individuals who have undergone breast cancer surgery. Therefore, the aim of this study was to investigate the usability of a newly developed App in the smartphone for occupational therapy services that would focus on their perceived needs and interests of breast cancer survivors and to identify the needs of breast cancer survivors in their activities of daily living.
Methods
Study design
A cross-sectional usability study was conducted. The first study was to investigate the feasibility of developing an App with data collected through online questionnaires with breast cancer survivors. The first study aimed to identify the occupational needs to maintaining an active life in women with breast cancer, with the subsequent development of an App for mobile devices, tablets, and personal computers. A second cross-sectional study was conducted to assess the usability of the developed App, named MAIA. The mobile app was designed to be used as a tool for occupational therapists and breast cancer patients (Figures 1–4). The testing was conducted on versions of the mobile app hosted on preproduction testing servers. MAIA was designed with input from subject matter experts (including the authors), patients eligible for this study, user experience designers, and mobile app developers. MAIA underwent iterative user interface revisions based on participant feedback on usability. Register and self-report MAIA for patients. Clinical information, ADL and patient progress. MAIA for occupational therapists. Follow-up for therapists.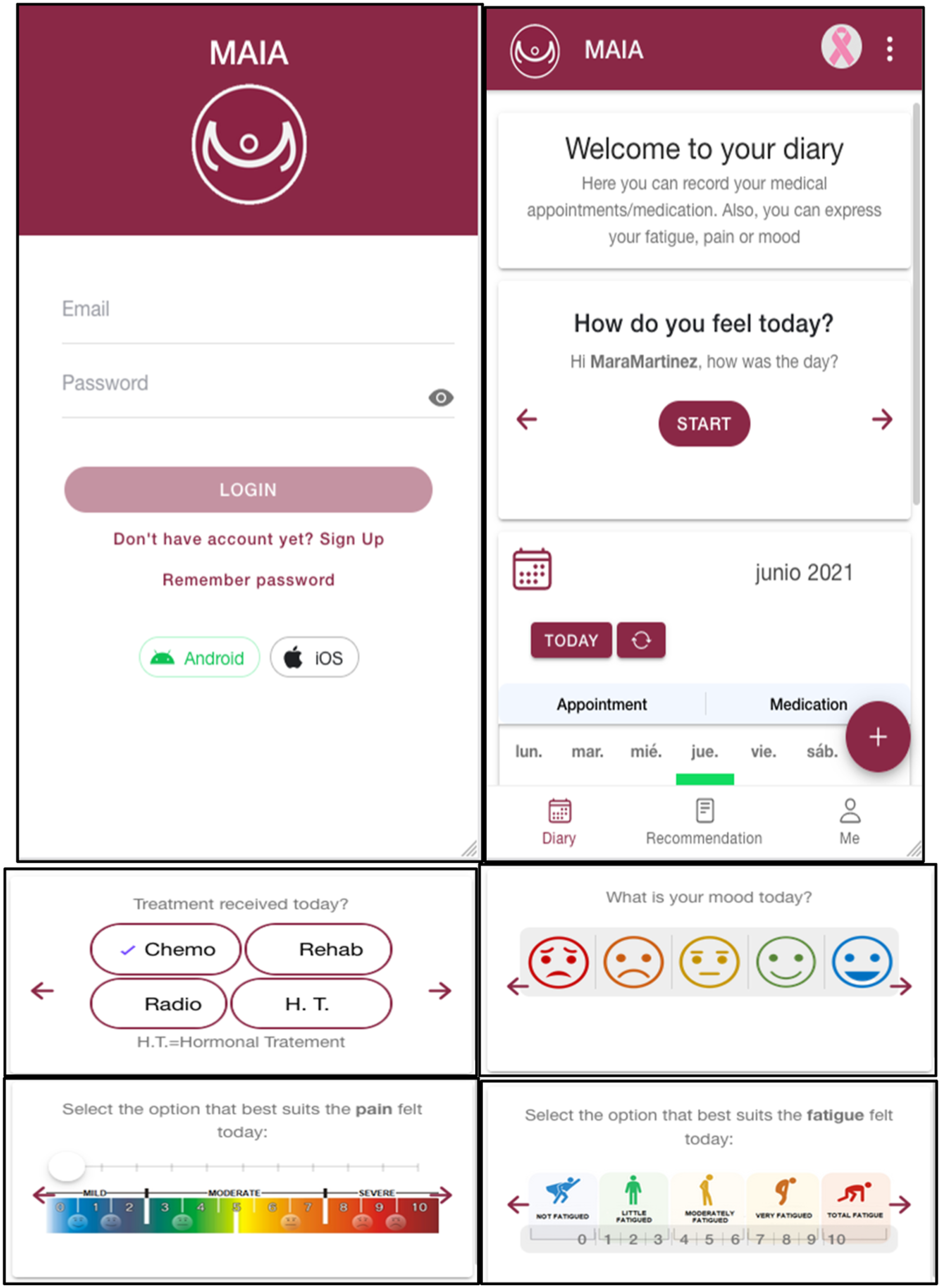
Participants
The sampling method was intentional, not probabilistic. After developing the questionnaire, the Breast Cancer Association assisted with the distribution among eligible patients who met the following criteria: (a) being a woman over 18 years of age; (b) having a diagnosis of breast cancer; (c) belonging to a health area in Spain; (e) having access to social networks. The exclusion criteria were: (a) being a terminal patient; and (b) not providing informed consent. All participants were fully informed about the purpose of the study and the anonymized use of the collected information throughout the entire process. Subsequently, those participants who agreed to participate, completed the online questionnaire.
Instruments
First study
A questionnaire was developed to collect sociodemographic data and to evaluate the occupational needs of breast cancer survivors based on the Occupational Therapy Practice Framework: Domain and Process Fourth Edition («Occupational Therapy Practice Framework», 2020). It consisted of 20 questions, including both multiple-choice options and open-ended responses. The completion time for the questionnaire was approximately 15–20 minutes. The questions aimed to gather information on (1) symptoms experienced during the disease; (2) cognitive and emotional deficits; (3) adequacy of information received regarding diagnosis, prognosis and treatment; (4) type of treatment received, (5) involvement in post-surgical OT; (6) availability for the patients of guidelines for instrumental activities of daily living (IADLs) and home management; (6) personal support received during the rehabilitation process; (7) social participation; (8) difficulties in ADLs; (9) sleep and rest difficulties; and (10) work difficulties.
Second study: A pilot study on usability of MAIA
Usability refers to the extent to which a product enables users to accomplish their goals effectively (Abran et al., 2003). To assess the usability of the MAIA App, the System Usability Scale (SUS) was used. The SUS consists of ten questions that provide a unique composite measure of usability, with two factors identified: usable (items 1, 2, 3, 5, 6, 7, 8, and 9) and learnable (items 4, and 10) (Grier et al., 2013; Lewis & Sauro, 2009). The SUS total score ranges from 0 to 100, with larger scores being better (Grier et al., 2013).
To characterize the functionality and occupational performance of breast cancer survivors, various standardized tests were used: the Engagement in Meaningful Activities Survey; the Occupational Balance Questionnaire; the General Self-Efficacy Scale; the Functional Assessment of Cancer Therapy – General; and the Disabilities of the Arm, Shoulder and Hand.
Engagement in Meaningful Activities Survey (EMAS) (Eakman, 2012; Goldberg et al., 2002). This tool is a 12-item self-report questionnaire designed to assess the extent to which an individual’s activities are personally important and aligned with their values and the social context. Participants respond using a five-point Likert-type scale, ranging from 1 = never up to 5 = always. The maximum score on the EMAS is 48, with the higher score, the higher sense of meaningful in one’s daily activities. The Cronbach’s Alpha of the EMAS is .91, indicating a high internal consistency. Furthermore, the EMAS demonstrates good temporal stability, as evidenced by a high intraclass correlation coefficient score of .76 (Prat et al., 2019).
Occupational Balance Questionnaire (Wagman & Håkansson, 2014). The assessment of occupational balance was conducted using the Spanish version of the Occupational Balance Questionnaire (OBQ-E) (Peral-Gómez et al., 2022). It has been established as a suitable tool for measuring occupational balance in the Spanish population. The OBQ-E focuses on capturing an individual’s perception of the quantity and variety of their daily occupations. It consists of 13 questions that are rated on a six-point Likert scale, ranging from 0 “strongly disagree” to 5 “strongly agree”. The instrument can be scored at the item level or by summing the responses to obtain a total score, which ranges from 0 to 65, where a higher score indicates greater occupational balance (Peral-Gómez et al., 2022).
General Self-Efficacy Scale (Schwarzer & Jerusalem, 1995) was designed to assess an individual’s optimistic sense of self-confidence, which refers to their belief in their ability to successfully perform new or challenging tasks and overcome life’s adversities. It is a one-dimensional scale comprising 10 Likert-type response items, ranging from 1 to 4 points. A score of 1 indicates that the item is incorrect or not applicable, while a score of 4 represents the item being correct. The scale has demonstrated good internal consistency, with Cronbach’s alpha values ranging between .76 and .90.
Functional Assessment of Cancer Therapy - General (FACT-G) is a self-administered questionnaire consisting of 27 items (Cella et al., 1993). It assesses the HRQoL of cancer patients in the following domains: physical, social, emotional and functional well-being. One advantage of this tool is that it can be completed in 5–10 minutes and is specifically designed for cancer patients. It has demonstrated good psychometric properties, including sensitivity to change, internal consistency and discriminant validity, according to disease stage and functional status (PSR).
Disabilities of the Arm, Shoulder and Hand (DASH) is a 30-item self-report questionnaire designed to assess a patient’s ability to perform activities using their upper extremities (Gummesson et al., 2003). Patients are asked to rate the degree of difficulty they experience in performing these activities on a regular basis, using a 5-point Likert-type scale. It has shown good psychometric properties and provides scores that can detect a minimal clinically important difference.
Procedure
The study was conducted from February 2016 to December 2021. Based on a literature search and the clinical experience of three occupational therapists, a questionnaire was designed to assess perceived needs in occupational performance following a breast cancer diagnosis. Data on perceived occupational needs were collected between February to June 2016. Subsequently, using the information gathered, the architecture and design of the App were developed. A client-server model based on the concept of service was implemented to create the App. The second study was conducted in the final year of the study period. The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by both organizations involved. Informed consent was obtained for all subjects included in this research.
Data analysis
Descriptive statistics were used for the sociodemographic and occupational performance data of the study. Frequencies and percentages were used to describe categorical variables. Mean and standard deviation were used to describe quantitative variables. Statistical analysis was performed using the IBM SPSS version 28.
Results
First study
Results of occupational needs in women of breast cancer survivors in the first study (n = 78).
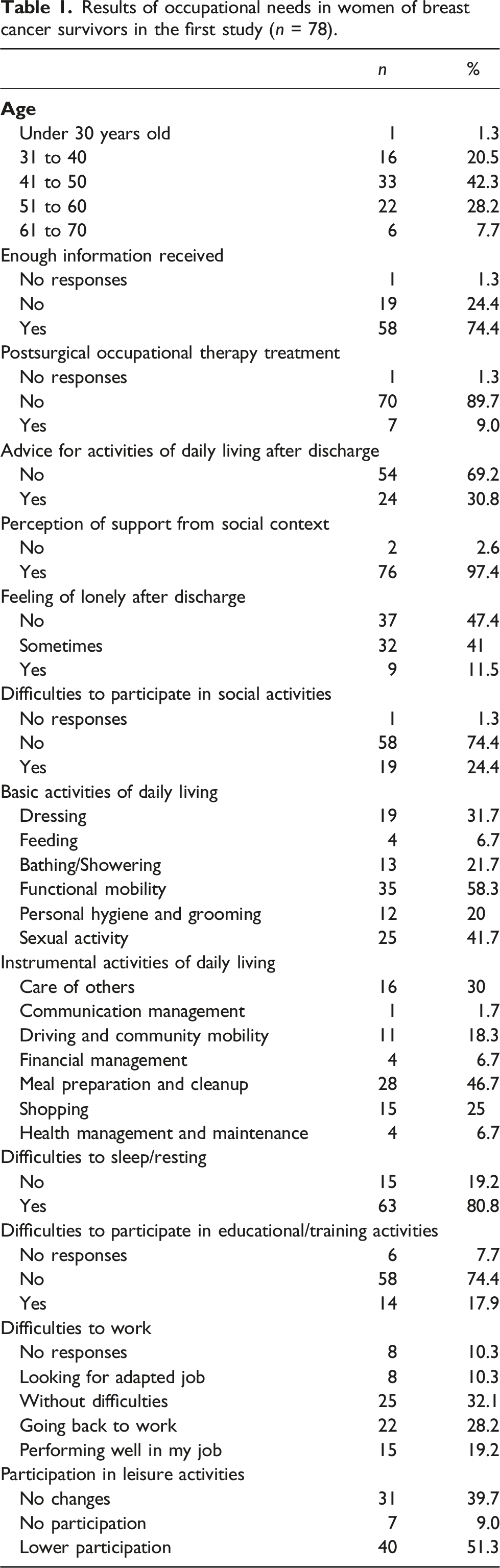
Regarding physical symptoms reported during the disease, fatigue was present in 71% of women, difficulty in healing in 66%, and decreased muscle strength in 62% of women. In terms of psychological functioning, 70% referred memory deficits, 60% referred attention deficits, 48% reported alterations in body image, 62% of the women reported anxiety as their main symptom, 54% decreased of libido and 31% had experienced depression.
Table 1 shows the perceived occupational needs of breast cancer survivors based on the Occupational Therapy Practice Framework: Domain and Process-Fourth Edition (2020). Regarding ADLs, 22% reported difficulties with bathing or showering; 32% with getting dressed and undressing; 20% with personal hygiene and grooming; 7% with eating; 58% with functional mobility; and 42% with the resumption of sexual activity. Regarding IADLs, 30% of the women indicated difficulties with child-rearing; 47% reported difficulties with meal preparation and clean-up; and 25% indicated difficulties with shopping. Fifty-three percent reported difficulties in the domain of health management, specifically related to social and emotional health promotion and maintenance. Concerning rest and sleep, 80% of breast cancer survivors reported difficulties in this area. In terms of work performance, 36% of women had no issues continuing working, while 31% experienced difficulties returning to work. Regarding participation in educational activities, 19% reported difficulties in participating in training and/or educational activities. Finally, 25% mentioned a decrease in social participation after being diagnosed, as a consequence of tiredness, fatigue and mood changes. These findings indicated that the area of greatest impact on breast cancer survivors’ occupational needs was sleep and rest, followed by social and emotional health promotion and maintenance, community mobility, resumption of sexual activity, and meal preparation.
Based on the identified needs, our aim was to design an App that could support and address some of these needs complementing occupational therapy. Therefore, the development of the application involved creating a client-server architecture, where communication between the two entities occurs through the HTTP protocol. Two types of web clients were developed: a patient web client and a therapist web client (MAIA for occupational therapists). Additionally, mobile applications for both IOS and Android were generated. MAIA was developed as a secure and private telemedicine tool. For user authentication, authorization and administration across the web and mobile applications, Amazon Cognito was used. This Amazon Web Service ensures data protection by using SSL/TLS protocols for communications, secure API access settings, and encryption of data in transit and at rest. By adhering to the conditions set by HIPAA and complying with the requirements of standards such as PCI DSS, SOC, ISO/IEC 27001, ISO/IEC 27017, ISO/IEC 27018 and ISO 9001, Amazon ensures the security and integrity of the system’s data. Only authorized research team members have access to the system’s data through their designated accounts, thereby guaranteeing the confidentiality and security of registered users’ information.
MAIA for patients
The “MAIA” App for patients (Figures 1 and 2), enables patients to manage their medication and appointments using a calendar. In addition, it allows therapists to record information regarding mood, pain, fatigue, other clinical data and occupational performance difficulties. A key feature of the App is that patients can access personalized advice created by their occupational therapists and filter them based on duration or interest. MAIA aims to enhance the personalized monitoring of breast cancer patients, improve communication between patients and their therapists, facilitate calendar management for patients and promote better rehabilitation outcomes through personalized recommendations.
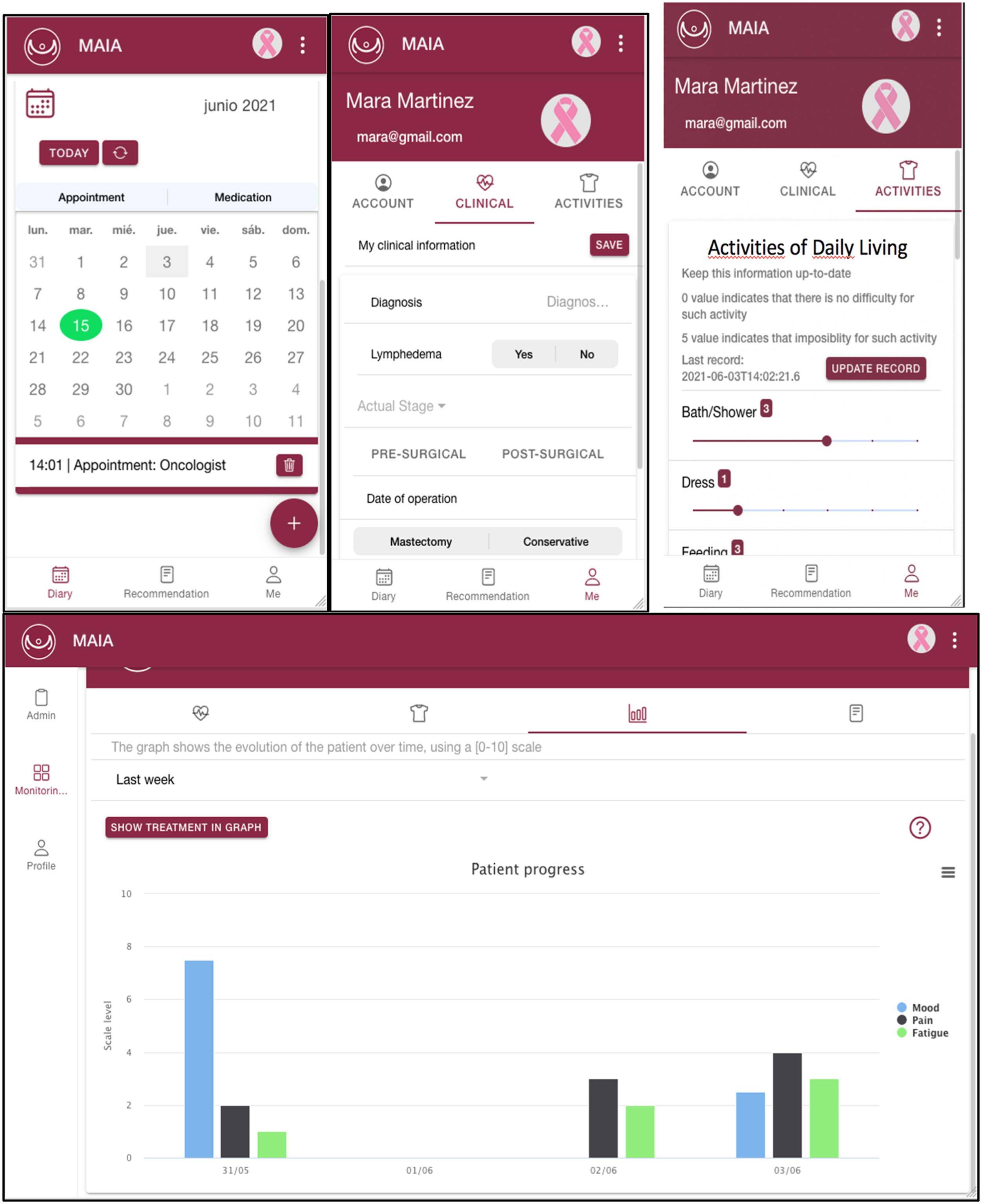
Once the patient logs in, they are automatically redirected to the agenda screen. On this screen, the patient can create appointments or record medication. Through the calendar, they can view or delete these appointments or medications. They can also search for a specific date or appointment name using the search engine located in the central area of the screen. Additionally, on the agenda screen, the patient can register how they felt during the day in the central section. This log is displayed only once a day. By using the menu located on the left side, the patient can navigate through the different screens of the application. On the recommendations screen, they can view and sort personalized recommendations, created by their therapist.
Finally, there is the “Profile section”, where the patient can click on the image to the right of their name to change their profile picture. This screen consists of three subsections. The first subsection, “Account”, allows the patient to update their profile data, access system settings, and log out. The second, “Clinical”, enables the patient to register their clinical data and update them over time. The third, “Activities”, allows the patient to record their difficulties in occupational performance and update this record once a day. A demonstration video of the MAIA App for patients is at: https://youtu.be/P_eFxoSsHyw.
MAIA for occupational therapists
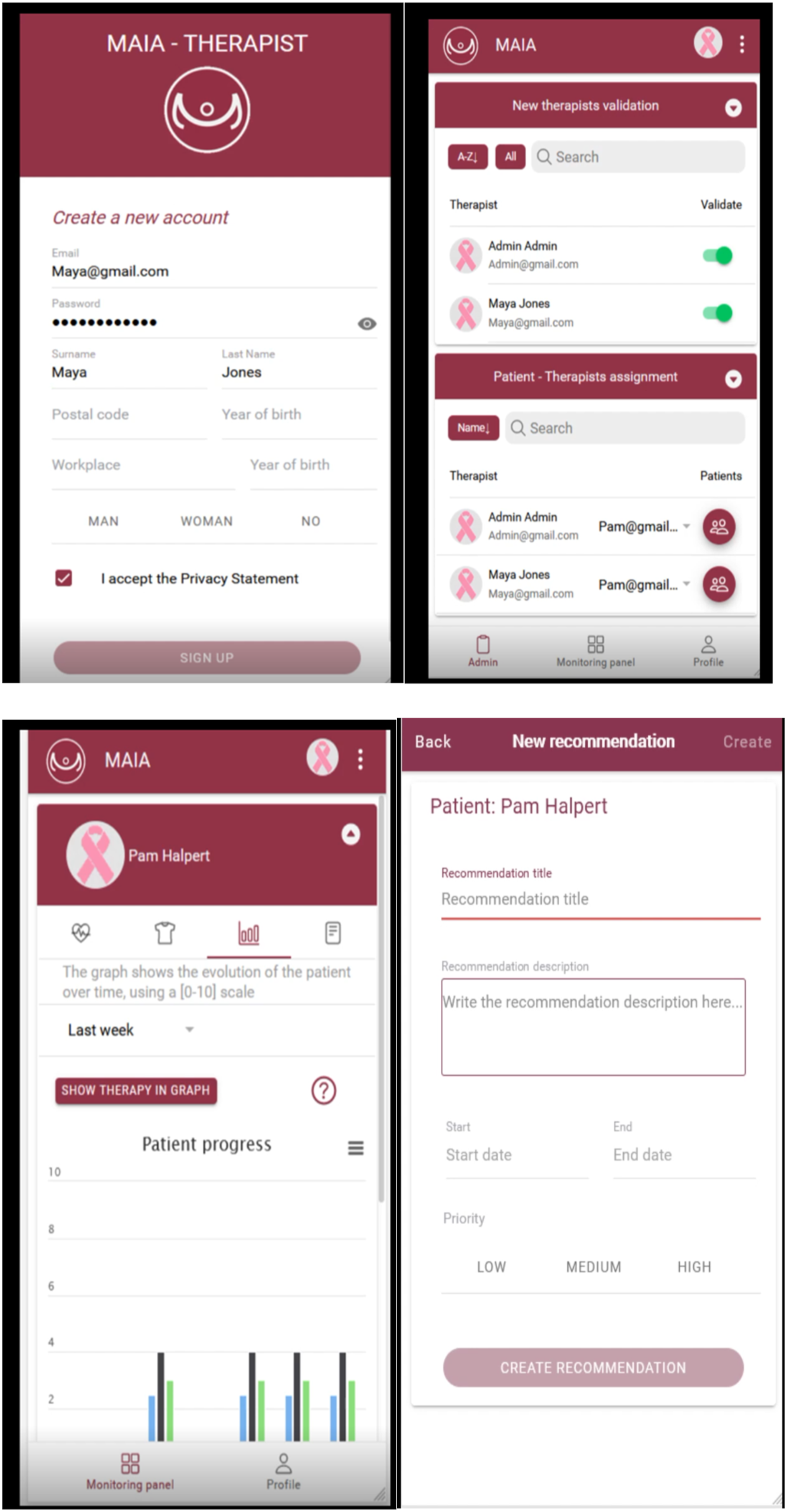
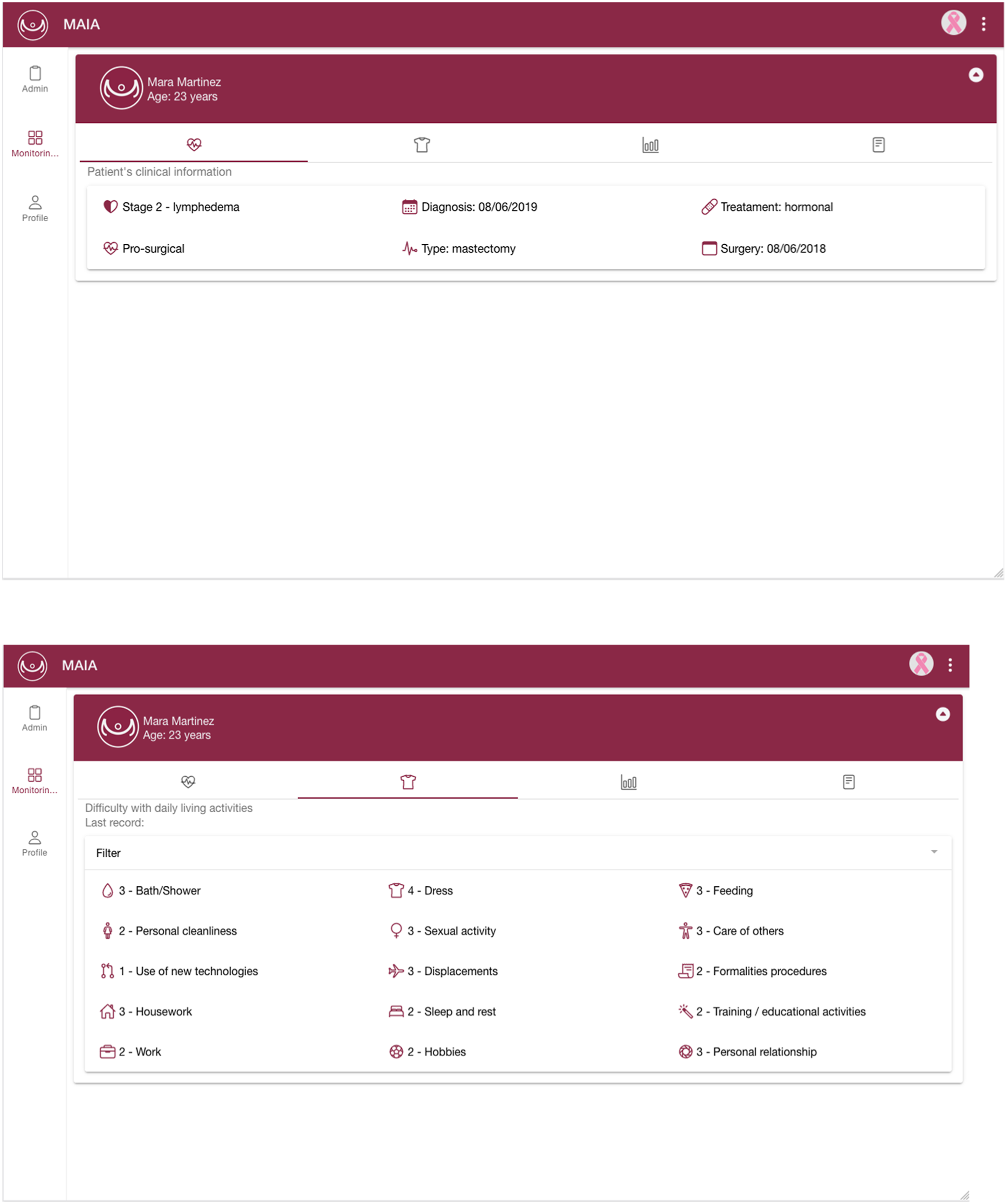
The “MAIA” App for occupational therapists enables them to access the clinical status and the difficulties reported by patients in performing ADLs (Figures 3 and 4). In addition, therapists can review the patient’s mood, fatigue or pain through graphs and even download these graphs in various formats. This information allows the therapists to create personalized recommendations for each patient. Finally, if the user is an administrator of the application, they can validate new therapists and manage the assignment of patients to therapists.
Similar to patients, therapists need to register in the system and complete the corresponding form. However, unlike the patient’s web client, therapists do not need to verify their account but instead, wait for an administrator to validate it. Once their account has been validated, they can log into the system. Once logged in, therapists are automatically redirected to the Control screen. In this section, they can access patient information and navigate through three submenus. The first submenu displays the patient’s clinical information. The second allows therapists to review the patient’s difficulties in occupational performance, with the option to filter based on specific difficulties. The third section shows statistics for mood, fatigue and pain recorded by the patient. Therapists can generate statistics for the past week, previous week, last two weeks or last month, among other filters. They can download these graphs in different formats such as JPEG or PDF. This section displays the recommendations for the selected patient, allowing therapists to delete existing recommendations or create new ones. If the therapists have an administrator role, they can also assign new patients or validate new therapists. A demonstration video of the MAIA App for therapists is at: (https://youtu.be/v8WM79YDM-c).
Occupational therapists can provide personalized recommendations to each patient based on their individual profile, specific difficulties in different occupational areas, and symptoms they experience, such as pain, fatigue, and limitations in upper limb function for occupational performance. Whenever a patient registers, an occupational therapist is assigned, and an alert is triggered. The therapist can access the patient’s information regarding clinical characteristics and mental state to make the necessary recommendations. Once the therapist sends the recommendations, the patient is notified and can start following them. The therapist has the ability to update recommendations at any time, and the patient receives an alert when this occurs. This enables the patient to promptly access and review the updated recommendations. The recommendations address both the clinical symptoms and the patient’s functional and emotional recovery. Furthermore, the patient can request additional support or consultation if deemed necessary, whether it is for functional or emotional reasons.
Second study: A pilot study
Health related quality of life, occupational and functional status of sample in the second study (n = 29).
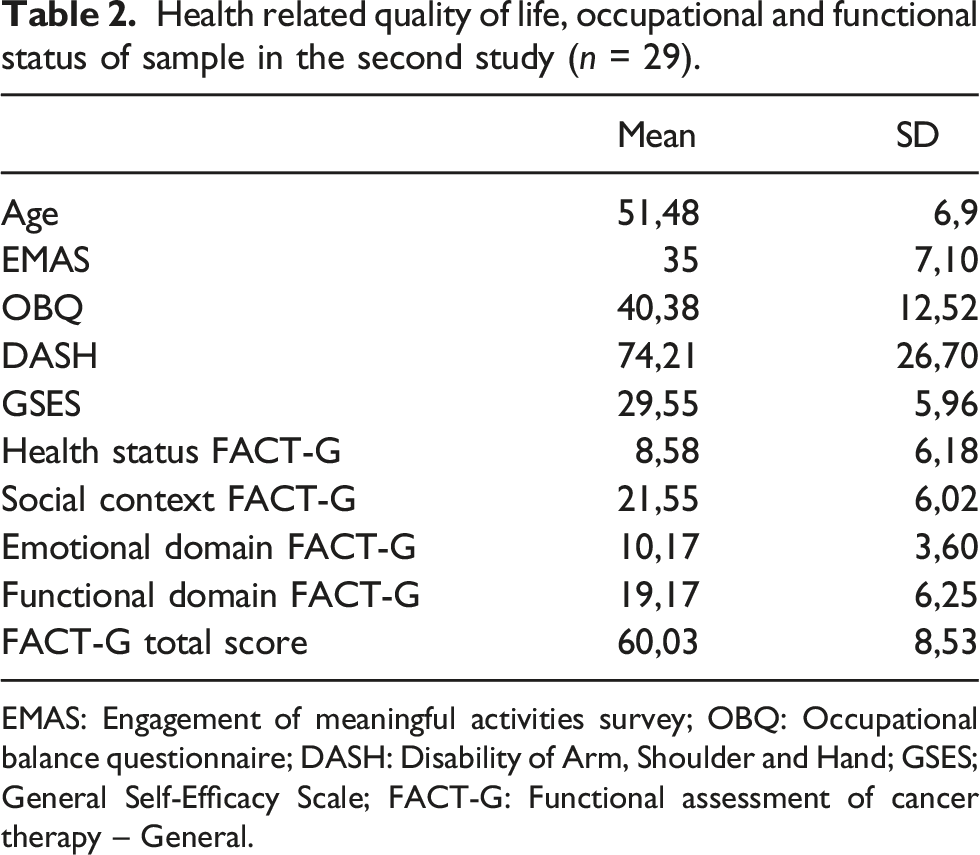
EMAS: Engagement of meaningful activities survey; OBQ: Occupational balance questionnaire; DASH: Disability of Arm, Shoulder and Hand; GSES; General Self-Efficacy Scale; FACT-G: Functional assessment of cancer therapy – General.
The mean SUS score was 63 points (SD = 12, 2). The mean score for the learnable dimension was 3.12 (SD = 1.38), being similar to the usable dimension (
Discussion
Several studies have shown that cancer survivors often experience unmet occupational needs in areas such as personal care, instrumental activities, social participation, work, and education (Algeo et al., 2021; Brick et al., 2022; Loubani et al., 2022; Stevens et al., 2020). Thus, OT interventions for breast cancer survivors should primarily focus on enhancing occupational performance and improving HRQoL (Lai et al., 2021; Loubani et al., 2022). The main objective of this study was to examine the impact of breast cancer on occupational performance in order to develop an App aimed at improving functionality and occupational performance. A second aim was to assess the usability of the MAIA App.
The results obtained from the analysis of 78 questionnaires, response indicated that women diagnosed with breast cancer reported experiencing physical, cognitive, psychological and social symptoms that could potentially interfere with their occupational performance (Table 1). Apps can serve as a useful strategy for improving the HRQoL of breast cancer survivors by enhancing their health, well-being, functional capacity, and occupational performance (Brandt et al., 2016; Lozano-Lozano et al., 2016; Yuen et al., 2006). The integration of Information and Communication Technologies (ICT) in healthcare has revolutionized traditional rehabilitation methodologies (Lai et al., 2021). Several studies have demonstrated the positive effects of telehealthcare on patients (Brandt et al., 2016; Yuen et al., 2006). It is also known that telerehabilitation can yield comparable outcomes to conventional rehabilitation programs (Roldán Jiménez, 2017). Additionally, mobile applications and telehealth systems can enhance patient motivation by providing feedback, support, and monitoring (Lai et al., 2021; Lozano-Lozano et al., 2016). The healthcare sector has the opportunity to transform itself by providing more personalized, participatory, and preventive services to patients while promoting greater patient engagement, treatment adherence, and disease management (Pergolotti et al., 2016). Unlike the MAIA app, which provides personalized recommendations for improving occupational performance under the supervision of an occupational therapist, there are other apps that focus on promoting healthy habits. For instance, the BENECA (ENErgy Balance on Cancer) m-Health app aims to enhance eating habits and physical exercise in women undergoing breast cancer treatment, considering the prevalence of energy imbalance in this population (Lozano-Lozano et al., 2023).
The findings of this study are consistent with previous research, demonstrating that breast cancer is a complex and serious disease with physical, psychological, and social implications (Lai et al., 2021). These effects can significantly impair patients' ability to engage in self-care activities such as personal hygiene, eating, and dressing, as well as household chores, work-related tasks, sleep, sexual activity, maintaining relationships with family and partners. Moreover, breast cancer presents challenges to social participation and leisure activities, impacting the overall quality of life (Lai et al., 2021; Morrison & Thomas, 2014; Nascimento et al., 2019; Palmadottir, 2010).
To date, most studies on OT for breast cancer survivors have primarily focused on addressing physical symptoms with physical rehabilitation exercises to increase resistance, strength and joint range of motion (Lattanzi et al., 2010; Yoon et al., 2015). However, cognitive impairment and emotional distress are prevalent in 10–50% of patients (Player et al., 2014), and this aspect is often neglected in most interventions. This highlights a gap in addressing the emotional well-being of these individuals (Loubani et al., 2022), who also experience anxiety due to changes in social support and the fear of cancer recurrence or death (Lattanzi et al., 2010).
Occupational therapists approach the rehabilitation of breast cancer patients from a holistic perspective, considering not only physical symptoms but also cognitive, emotional, and social aspects that influence the recovery process (Désiron et al., 2015; Loubani et al., 2022; Lozano-Lozano et al., 2023). This approach takes into account roles, interests, habits, routines, performance contexts, competencies, physical and emotional abilities, as well as personal backgrounds («Occupational Therapy Practice Framework», 2020). Unlike other apps, MAIA has the potential to provide guidance and advice on adaptations and supportive tools to enhance occupational performance. This includes exercises to prevent lymphedema and improve mobility, relaxation techniques and support messages for emotional well-being, emotional self-regulation, and pain relief. MAIA also offers a forum where patients can share doubts and experiences with other individuals facing a breast cancer diagnosis. Additionally, the app’s diary feature can be used to set reminders for appointments and medical management, as well as help monitor the progression of the disease.
In this regard, technological support can be a promising strategy to address challenges such as distance, time constraints, costs, and motivational aspects like feelings of isolation. MAIA is a customizable app that can be accessed through both mobile devices and computers. Furthermore, MAIA is available in multiple languages, including English and Spanish. MAIA is a telehealth system that offers personalized recommendations specifically tailored to the activities of daily living needs of breast cancer survivors.
Although the usability of MAIA is adequate it could be improved (Friesen, 2017; Grier et al., 2013). In general, scores below 58 indicate that usability can be improved, while scores above 68 indicate that usability is good. On the other hand, the score on learnable on the use of MAIA may be due to the short period in which the App was tested, where they were still learning to use and integrate it, so it would be necessary to check if this score could change with a longer follow-up.
This research has a series of limitations since it is the first to be conducted with the new App developed, MAIA, as a pilot study and has focused on the experience of women breast cancer survivors in Spain. It would be advisable to perform new studies with a larger sample, with a prolonged time of use, monitoring the evolution, adherence to treatment and recommendations. User-centred designs enable the development of rehabilitation technology solutions, including different Design-Evaluation-Redesign cycles that iteratively engage actual end-users and healthcare professionals to refine and optimize technology solutions. In addition, future research could differentiate the needs according to the evolution of the disease and whether or not the patients are in the active period of the disease and the time elapsed since it.
Conclusions
Women survivors of breast cancer showed difficulties in performance and occupational participation. MAIA is an App designed to meet these occupational needs and it could be a new useful resource for the rehabilitation of breast cancer survivors. In light of the above, occupational therapists should take into account not only physical deficits but also cognitive ones (specifically memory and attention deficits). Additionally, they should conduct a thorough assessment of the impact on ADL with the goal of providing advice adjusted to the specific daily needs of women with breast cancer. Furthermore, it is important to promote programs aimed at enhancing social participation and implementing group interventions that offer socioemotional support. Finally, the use of mobile apps, such as MAIA, could be a complementary resource within occupational therapy interventions.
Footnotes
Acknowledgements
We would like to express our gratitude to the Breast Cancer Associations for their collaboration in sharing their personal experiences and guiding the conduction of this study. We also extend our thanks to the reviewers, designers, and all the professionals involved in making this publication possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.