
Abstract
Purpose
To examine the consistency between patient- and occupational therapist-reported judgments of patients’ ability and change in ADL abilities.
Materials
Patient- and therapist-reported ADL abilities were assessed using a Visual Analogue Scale, whilst the changes in patients’ ADL abilities were reported by patients and therapists using a 15-point Likert-type scale.
Methods
Repeated assessments at a 3-week interval were used. 88 inpatients with stroke and 16 occupational therapists were recruited from rehabilitation wards in a medical center.
Results
Moderate correlations (rs = .53–.56) were found between the patient- and therapist-reported ADL abilities. The patient-reported scores were significantly lower (ds = .45; ps < .001 at follow-up) than the therapist-reported scores. Only low correlation (r = .33) was found for the change scores.
Conclusions
Our findings indicated that there was only a moderate to low correlation between the patients' reports and the therapists' judgments regarding the patients' ADL ability and its change. Because both patients’ reports and therapists’ judgments affect decisions on rehabilitation, frequent communication may be beneficial for reaching consensus and helpful in managing the interventions.
Introduction
Stroke is a common cause of dependence in activities of daily living (ADL). ADL has been shown to be positively correlated to subjective well-being and quality of life in patients with stroke (Hsieh et al., 2012, Hsueh et al., 2013, Raju et al., 2010), and reducing the level of dependence in ADL is often a focus of rehabilitation programs. Therefore, the ADL outcome is important for clinical decision-making and for monitoring intervention outcomes (Hsieh et al., 2002).
Assessments of ADL can be divided into at least two distinctive concepts or constructs: ability and actual performance (Holsbeeke et al., 2009, Hsieh et al., 2012, Wade & Collin, 1988). Ability targets whether individuals can perform ADL tasks (Michielsen et al., 2009, Wade & Collin, 1988). On the other hand, actual performance refers to whether individuals perform ADL tasks in real-life situations (Holsbeeke et al., 2009, Hsieh et al., 2012, Michielsen et al., 2009). Assessments targeting actual ADL performance, such as the Barthel Index or Activities of Daily Living Computerized Adaptive Test (ADL CAT), are usually assessed by thorough interview (Hsieh et al., 2012). Among these two constructs of ADL, ability might be more crucial for clinical settings because it helps to detect patients’ inability to perform ADL tasks and thereby guides the corresponding intervention programs (Hsieh et al., 2012). Thus, assessments of ability are a priority in clinical settings.
Therapist’s subjective judgments and patient’s self-reports of the patients’ ADL ability may be generated during therapy sessions. Both of them are easily-accessible, time-saving and less complicated (for administering) ways to obtain valuable ADL information (Dean & Unsworth, 2009, Garland et al., 2003, Haas et al., 2016, Potter et al., 2011, Swinkels et al., 2011). These two subjective assessments may affect the therapists’ clinical decision making and patients’ satisfaction with rehabilitation (Liu et al., 2004).
The consistency between therapist’s subjective judgments and patient’s self-reports of patient’s ADL ability is particularly crucial for the interpretation of patients’ ADL function yet has seldom been examined. When therapists' judgments and patients' reports align, it indicates a shared perception of the patients' ADL functions. Therefore, the intervention plans formulated based on this consensus between therapists and patients are more likely to be appropriate. On the other hand, if there is a disparity between the results of therapists’ judgments and those of patients’ reports, it may lead the therapists to make inappropriate ADL-related decisions (e.g., treatment goals). Moreover, because ADL performance is an outcome indicator for stroke rehabilitation (Hsieh et al., 2012), consistency between ADL performance and two subjective assessments of ADL ability is crucial for clinicians.
To address these issues, we developed three hypotheses on the consistency between therapists’ subjective judgments and patients’ reports of ADL abilities: (1) the correlations of ADL ability between the patient’s self-report and the therapist’s subjective judgment would be moderate (Dean & Unsworth, 2009, Hsiao et al., 2020) at baseline and follow-up assessments, (2) the correlations of ADL change in ability between the patient’ s self-report and the therapist’s subjective judgment would be moderate (Farin, 2009), and (3) the correlations between the patient’s self-report and the therapist’s subjective judgment of ADL ability and the patient’s actual ADL performance would be moderate at both time points. Furthermore, we hypothesized that there would be no significant differences among patient’s self-reported ADL ability, therapist’s subjective judgment of ADL ability, and patient’s actual ADL performance.
Methods
Participants
We recruited patients who were admitted to the rehabilitation ward in a medical center in Taichung, Taiwan, as well as their occupational therapists (OTs). All participants were recruited from December 2014 to March 2016. The patients were included if they: (1) were diagnosed with ischemic stroke or cerebral hemorrhage; (2) had first onset of stroke within 6 months (subacute stage of stroke); (3) scored 20 points or more on the Mini-Mental State Exam (MMSE) (Hsiao et al., 2020). Patients who had communication problems or other major diseases which might affect their cognition were excluded. The criteria for the OTs were that they: (1) had at least 5 years of experience treating patients with stroke; (2) had treated the recruited patients for at least one week. This study was approved by the institutional review board of the medical center. We obtained informed consent from the patients and their OTs in person.
Procedure
The MMSE was administered to the patients by a blinded trained research assistant to assess their eligibility based on the study criteria (scored 20 points or more). The patients and the OTs treating them completed a 20-cm Visual Analogue Scale (VAS) to report patients’ overall ADL ability at the baseline and follow-up assessments. The patients were assessed twice with the Activities of Daily Living Computerized Adaptive Test (ADL CAT) by the same research assistant. The ADL CAT was used to describe patients’ ADL actual performance. These three (patient- and therapist-reported VAS and ADL CAT) assessments were performed when patients were admitted to (baseline) and discharged from the rehabilitation wards (follow-up), an interval of about 3 weeks. Furthermore, at the follow-up assessments, the patients and their OTs assessed the ADL changes between the two assessments on a 15-point Likert-type scale.
Instruments
20-cm visual analogue scale
Patients and OTs used a 20-cm horizontal VAS to assess the patients’ ADL ability at baseline and follow-up assessments (McCormack et al., 1988). The VAS ranges from 0 (labeled “worst ADL ability”) to 20 (“best ADL ability”). To avoid possible memory effects from the baseline assessment, this follow-up assessment only targeted the patients’ current ability of ADL without comparison to the baseline assessment. The horizontal VAS has demonstrated acceptable test–retest reliability for assessing shoulder pain in patients with stroke (Dorman et al., 1998, Turner-Stokes & Rusconi, 2003).
15-point Likert-type scale
Patients and OTs assessed the extent of change of patients’ ADL ability between baseline and follow-up assessments on a 15-point Likert-type scale (−7 to 7) (Jaeschke et al., 1989). At the follow-up assessments, the patients and OTs were asked the following question: “Compared with your (for the patients)/the patient’s (for the OTs) ADL status at the baseline assessment, have there been any changes in your/the patient’s ADL ability?” Responses ranged from 7 (a very great deal better) to −7 (a very great deal worse), and at the center of the scale were 1 (almost the same, hardly any better), 0 (no change), and −1 (almost the same, hardly any worse). We chose to use both methods (VAS and Likert-type scale) because existing studies have not determined definitively which method is more robust in evaluating ADL changes. Moreover, Likert-type items are commonly used and psychometrically satisfactory for patients with stroke (Duncan et al., 1999, Williams et al., 1999).
Activities of daily living computerized adaptive test
The ADL CAT was used to assess ADL actual performance (one of the outcome indicators of stroke rehabilitation) in daily life through interview. The ADL CAT was used to describe patients’ ADL actual performance in this study. The item bank of the ADL CAT consists of 34 tasks, including 11 basic ADL tasks and 23 instrumental ADL tasks (Hsueh et al., 2013). This measure was chosen because many of the IADL tasks (e.g., watching television, using a telephone) are suitable for inpatients. The ADL CAT outputs a T score (mean = 50, SD = 10), with higher scores indicating better ADL performance. For comparison with the VAS scores, ADL CAT scores were linearly transformed into the same scale as the VAS (0–20) to create ADL CAT transformed scores. The ADL CAT demonstrates good psychometric properties in patients with stroke (Hsueh et al., 2013, Lee et al., 2014).
Mini-mental state examination
The MMSE was administered to screen patients’ cognitive status. It has 11 items assessing orientation, attention, memory, language and visual construction (Folstein et al., 1975). The total score of the MMSE ranges from 0 to 30. Higher scores indicate better cognitive function. The psychometric properties of the MMSE are satisfactory in patients with stroke (Grace et al., 1995, Zwecker et al., 2002).
Statistical analysis
We examined the correlations and differences between ADL abilities assessed in 2 different ways: patients’ self-reports and OTs’ judgments. Moreover, we also examined the correlation between the scores of ADL ability (patients’ and OTs’ subjective judgments using patient- and OT-reported VAS scores) and those of patients’ ADL performance (i.e., the ADL CAT) at two assessment times (baseline and follow-up). Pearson’s correlation coefficients were applied to the subsequent analyses. Regarding the change between two assessment times, the correlations among the scores obtained from the patient-assessed Likert-type scale, the OT-assessed Likert-type scale, and the change scores of the transformed ADL CAT were used. The strength of the correlations was classified as follows: r ≥ .8, very strong; r ≥ .7, strong; .5 ≤ r < .7, moderate; .4 ≤ r < .5, fair; .3 ≤ r < .4, low correlation and r < .2 considered weak or negligible (Akoglu, 2018, Schober et al., 2018).
Furthermore, we used paired t-test to compare the scores among the patient-reported VAS scores, the OT-reported VAS scores and the transformed ADL CAT scores. A p-value of < .017 (.05/3) was considered statistically significant. Effect size (Cohen’s d) was used to estimate the magnitudes of difference for three pairs of scores (i.e., the patient- and OT-reported VAS scores; the OT-reported VAS scores and the transformed ADL CAT scores; the patient-reported VAS scores and the transformed ADL CAT scores). The scale for the effect size was set at .2, .5, and .8 to indicate small, medium, and large, respectively (Cohen, 2013).
Results
Demographic and clinical characteristics of patients in this study.
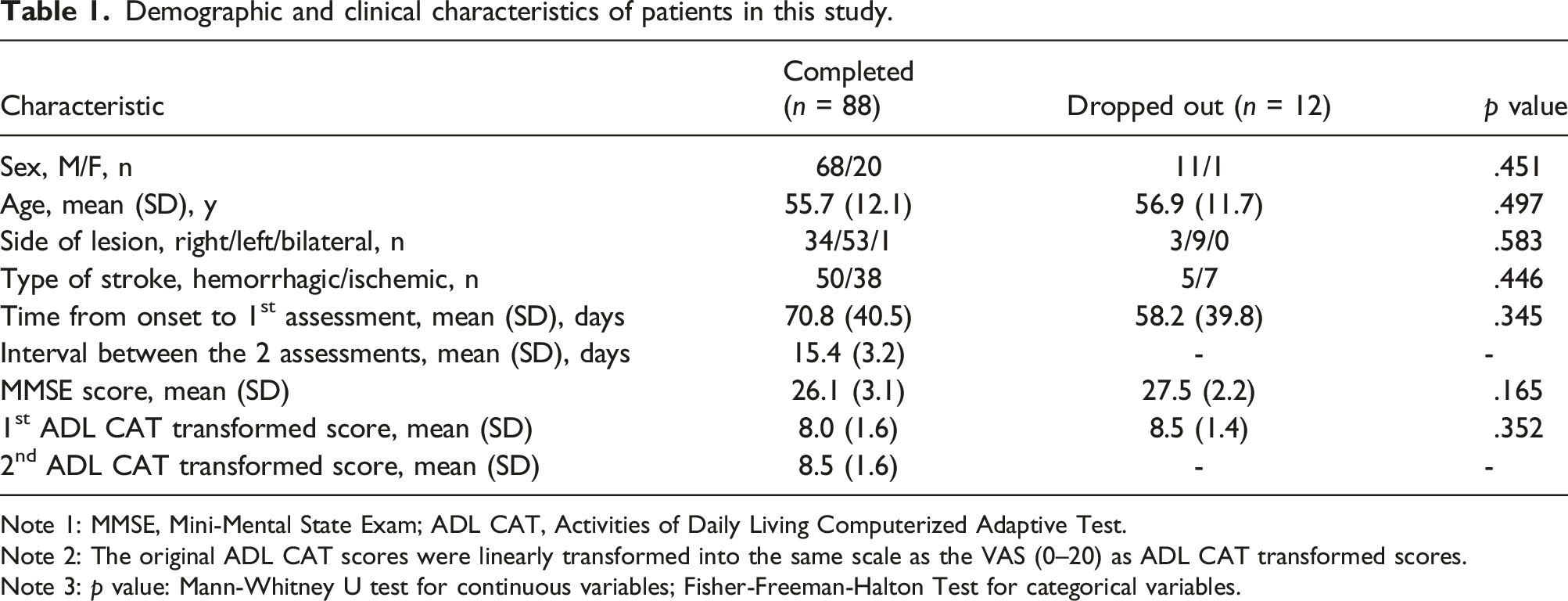
Note 1: MMSE, Mini-Mental State Exam; ADL CAT, Activities of Daily Living Computerized Adaptive Test.
Note 2: The original ADL CAT scores were linearly transformed into the same scale as the VAS (0–20) as ADL CAT transformed scores.
Note 3: p value: Mann-Whitney U test for continuous variables; Fisher-Freeman-Halton Test for categorical variables.
Correlations between the scores of the ADL CAT and the VAS.
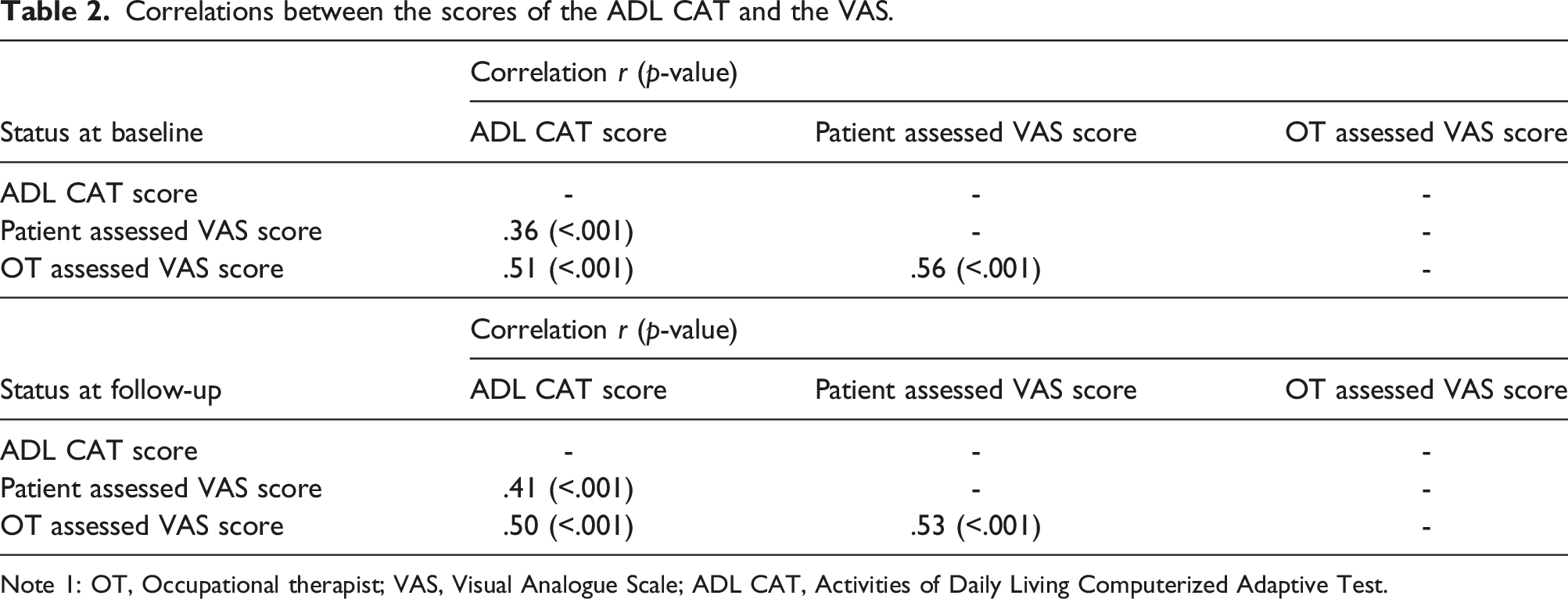
Note 1: OT, Occupational therapist; VAS, Visual Analogue Scale; ADL CAT, Activities of Daily Living Computerized Adaptive Test.
Differences between the scores of the ADL CAT and the VAS.

Note 1: Data are expressed as Mean (SD).
Note 2: OT, Occupational therapist; VAS, Visual Analogue Scale; ADL CAT, Activities of Daily Living Computerized Adaptive Test.
Note 3: *p < .017; **p < .001.
Correlations and differences between the change scores of the ADL CAT and the likert-type scale.
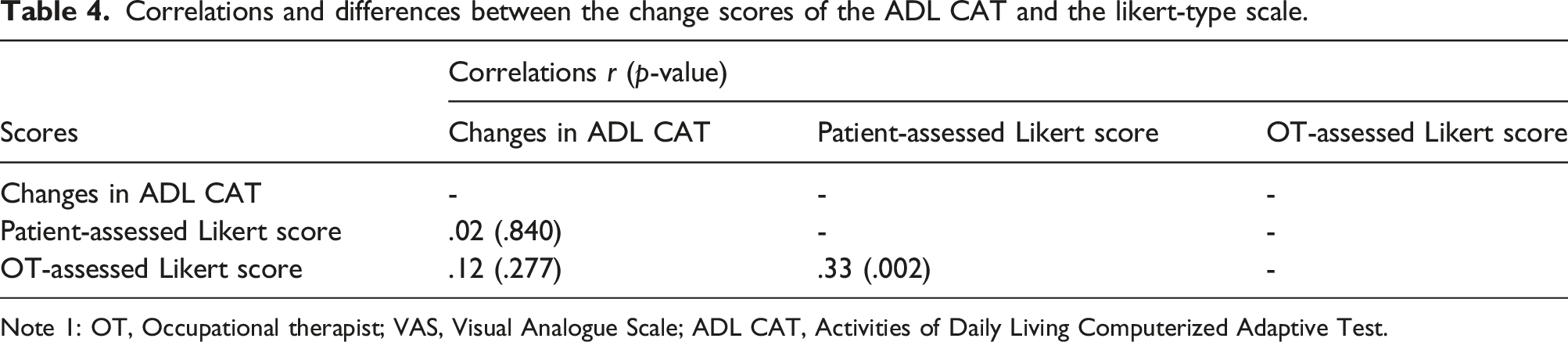
Note 1: OT, Occupational therapist; VAS, Visual Analogue Scale; ADL CAT, Activities of Daily Living Computerized Adaptive Test.
Discussion
The results of our study presented a blend of outcomes, some of which aligned with our hypotheses, while others deviated from our initial predictions. Firstly, as anticipated, we observed moderate correlations between the OTs and patients' subjective judgments. Secondly, contrary to our hypothesis, we found low correlations between OT and patients-assessed ADL change scores. Thirdly, our hypothesis regarding the moderate correlations between the patient’s self-report and the therapist’s subjective judgment of ADL ability, and the patient’s actual ADL performance (measured by ADL CAT) at both time points was not fully supported. Our results indicated low to moderate correlations in these relationships. Furthermore, at the baseline assessments, we did not find any significant differences among the scores obtained from the three assessments (patient’s self-reported ADL ability, therapist’s subjective judgment of ADL ability, and patient’s actual ADL performance), which aligns with our expectations. However, at the follow-up assessments, significant differences were observed among the scores obtained from the three assessments.
The subjective judgments from the OTs and the patients were only moderately correlated (r = .53 and .56 at the baseline and follow-up, respectively). Similar findings were reported in Hsiao et al.’s study, which found that patients with stroke tended to underestimate their ability in the follow-up (Hsiao et al., 2020). These findings indicate that patients’ and therapists’ judgments on patients’ ADL ability could be different. This different understanding of ADL ability may have caused difficulties in achieving consensus on treatment goals and thereby decreased patients’ satisfaction with the interventions. Thus, to manage the effectiveness of ADL interventions, identification and investigation of this discrepancy should be considered.
Four possible reasons may explain the inconsistency between patients’ perceptions and therapists’ judgments on patients’ ADL ability, as follows. First, the patients might have expected to have “fully recovered” the lost abilities after stroke, so they might have appraised their ADL ability conservatively. An alternative explanation may be that the patients were depressed about the loss of functions after stroke (Towfighi et al., 2017), so they were not ready to change their focus to the present and future recovery. Third, the family member might have performed every ADL task for the patients. Therefore, the patients might not have viewed their ADL ability positively because they had few chances to do their ADL routines. Fourth, the OTs may have had more optimistic perceptions of the patients’ ADL, which may have resulted from the OTs anticipating positive outcomes (Haas et al., 2016) and/or having relatively limited opportunities (only in clinics) to thoroughly observe the patients’ abilities. Nevertheless, our results showed that the OTs’ judgments were inconsistent with the patients’ perceptions regarding their ADL abilities. Therefore, frequent communication regarding the treatment progress of ADL ability and proper management of the patient’s psychological state, such as stress or grief, could be beneficial for reaching mutual consensus on patients’ ADL-related decisions.
Considering the correlations between the other two subjective judgments (patient- and OT-reported VAS) and the assessment of patients’ actual performance (the ADL CAT), low to moderate correlations were found for the baseline (r = .36 and .51 for patients and OTs, respectively) and follow-up (r = .41 and .50 for patients and OTs, respectively) assessments. These limited correlations seem to be reasonable because the subjective assessments and ADL CAT represent two distinct ADL constructs (ability vs. performance) (Hsieh et al., 2012). Nevertheless, these findings further support the differences between ADL ability and actual performance. Thus, assessments of ADL ability and actual performance should be conducted and interpreted separately to provide a comprehensive overview of patients’ ADL status. Moreover, because patients’ self-perceived ADL ability may affect their interpretations of treatment progress, more communication is needed to minimize the discrepancy. Specifically, therapists should continue to spend time exploring patients’ status with the patients so that both parties have the best possible understanding of the patients’ ability and the outcome of therapy (Dean & Unsworth, 2009). Finally, incorporating patients’ perspectives into measuring outcomes and treatment planning might be able to provide therapists more insight for making clinical decisions on ADL management (Lee et al., 2010, Liu et al., 2004).
The findings on the change scores were contrary to our hypothesis. Specifically, low correlations (r = .33) were found between the scores of the patient-assessed and the OT-assessed Likert-type scale. This considerable disparity might be ascribed to the OTs having taken the patients’ improvement in physical function into consideration, which in turn would affect their judgments of the patients’ changes. Given that patients and therapists had different feelings about the patients’ improvement in ADL ability, more communication about the progress of recovery is required to minimize misinterpretations.
The findings on the change scores between the scores of ADL ability and performance were different from our expectations. Negligible correlations were found between the two subjective scores of ADL ability (patient-assessed Likert-type scale and OT-assessed Likert-type scale) and that of ADL performance (ADL CAT) (rs < .12). Therefore, subjective scores of ADL ability seem to be irrelevant to those of ADL performance. This very weak correlation could be due to the fact that the subjective assessments and the ADL CAT assess two different constructs, as mentioned in the previous paragraph. Our findings suggest that changes in subjective ADL ability are irrelevant to those in ADL performance. Thus, assessments of both ADL ability and performance are required to provide comprehensive profiles of patients’ ADL function.
A limitation of the present study was that our patients were recruited via convenience sampling of inpatients. In addition, we recruited patients in the subacute stage only and excluded both patients who had communication difficulties and those who were unable to fill out the VAS and Likert-type scale. Therefore, our results might not be generalizable to the entire stroke population.
Conclusion
Three major findings were revealed in this study. First, the correlations between the scores of subjective ratings (i.e., patient- and OT-reported VAS) were moderate. Second, the correlations of OT- and patient-reported ADL changes were low to negligible. Third, OT- and patient-reported ADL ability showed low to moderate correlations with the patients’ actual performance. These findings indicate that the OT’s judgments are somewhat inconsistent with the patients’ perceptions of ADL ability and its change. Therefore, we recommend frequent communications regarding the treatment progress of ADL ability to increase the consistency between patient- and therapist-reported judgments of ADL ability.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chung Shan Medical University (CSMU-CMMC-108-04); Chi Mei Medical Center (CMCSMU-10806).