
Abstract
Background
Sleep problems are a health issue worldwide. Based on the Person-Environment-Occupation-Performance model, we developed an occupation-based sleep programme to promote awareness of sleep hygiene factors, promote an environment conductive to sleep, and restructure participation in daytime activities with a focus on occupational balance.
Method
This study uses a non-equivalent group design to evaluate the effectiveness of an occupation-based sleep intervention among community-dwelling adults with insomnia, when compared with a treatment-as-usual (TAU) group which focused on sleep hygiene, and relaxation.
Results
When compared with the TAU group (n = 20), the intervention group (n = 22) had significant improvement in sleep duration, occupational balance, and reduction in mood symptoms at both post treatment and 1-month follow up.
Conclusion
The results demonstrated that an occupation-based programme is an effective treatment for insomnia disorder and demonstrated the role which occupational therapy could play in primary health care service.
Background
Sleep is crucial for people’s health and well-being. Sleep problems are associated with raised risks in diverse medical conditions, such as obesity, heart disease, high blood pressure, and diabetes (Gallicchio & Kalesan, 2009; Yaggi et al., 2006). Lack of sleep can adversely affect people’s cognitive performance (Kyle et al., 2017; Low et al., 2019), and poor sleep is a significant contributing factor to depressive mood and related emotional disorders (Pemberton & Fuller Tyszkiewicz, 2016). In recent years, insomnia has become a major public health issue, indicated by a world-wide prevalence ranging from 10 to 30% in modern societies (Bhaskar et al., 2016; Cunnington et al., 2013; Ellis et al., 2012). A population studies estimated the weighted prevalence of insomnia among Hong Kong adults is 39.4% (Wong & Fielding, 2011). While insomnia has become an alarming public health issue, there have been few examples of occupational therapy interventions and evidence-based research in this area (Ho & Siu, 2018; Leland et al., 2014). There are also few theories of occupational therapy which discuss how sleep could be a kind of occupation, and if occupational therapy could have a role in management of sleep problems (Fung et al., 2013; Leland et al., 2014). In this study, we designed an occupation-based sleep intervention programme based on theories of occupational balance and the Person-Environment-Occupation-Performance (PEOP) model. Through an evaluation of the occupation-based programme for insomnia, we explored the role of occupational therapists in a primary care mental health team.
The American Occupational Therapy Association (2008) definite Rest and Sleep as activities related to obtaining restorative rest and sleep that supports healthy active engagement in other areas of occupation. According to the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) (DSM-5) (American Psychiatric Association, 2013), the key symptoms of insomnia disorder include difficulty falling asleep, intermittent awakenings or difficulty in maintaining sleep during the night; and early morning awakening and inability to sleep again. In addition, sleep difficulties need to persist for at least three nights per week and have been ongoing for at least 3 months; lead to significant distress and disruption to daytime functioning; but is not related to any medical, mental, or physical disorder, or the use of substances.
It is common for people with sleep problems to use alcohol, complementary medicine or over-the-counter hypnotic drugs to cope with sleep problems (Cheung et al., 2014). However, many people who seek help with sleep problems tend to prefer non-pharmacological intervention, due to concerns about potential dependence on sleep medication (Liu, et al., 2016). Thus, there is growing demand for non-pharmacological interventions for insomnia around the world. (Hrehová & Mezian, 2021).
While there is a rising health care need of people with sleep problems and insomnia around the world, few occupational therapy interventions were developed to address these needs (Fung et al., 2013). Sleep is not a commonly mentioned facet of occupation, and there have been discussions of how sleep could fit into the domains of practice of occupational therapy (Fung et al., 2013). In recent years, there is a developing consensus that sleep and rest could be defined as restorative occupation (Howell & Pierce, 2000), and sleep is an occupational need which support daytime occupations (Green, 2008; Leland et al., 2014). Furthermore, ongoing disruptions in sleep and rest could impact on people’s choice, performance, and participation in variety of occupations, i.e., one’s occupational balance (Dhas & Wagman, 2020; Ho, Dür, Stamm, & Siu, 2020). Reviews (e.g., Ho & Siu, 2018; Smallfield & Molitor, 2018) showed that the range of occupational therapy interventions for sleep problems include sleep hygiene education, cognitive-behavioural therapy for insomnia (CBT-i) (Eakman et al., 2017), prescription of sleeping aids (e.g., quilt, Dreampad pillow or weighted blankets) (Bolic Baric et al., 2021), physical activities, mind-body activities and mindfulness training, and lifestyle interventions (Leland et al., 2016). While there is a growing interest to develop sleep intervention programme in occupational therapy, these reviews showed that many programmes were not designed or organised based on occupational therapy theories (Ho & Siu, 2018).
The multi-disciplinary Integrated Mental Health Programme (IMHP) teams in primary care clinics in Hong Kong, are the first points of contact for providing care to patients with insomnia and other sleep problems. Since 2012, occupational therapist joined the team in these primary care clinics, which aims to screen patients with mood and sleep problems and provide timely interventions. The occupational therapy programme in the primary care clinic used to compose of short-term sleep hygiene education and relaxation training. In recent years, the occupational therapy team re-designed the sleep programme based on concepts of occupational balance and the application of coaching strategies.
Insomnia could result from a combination of individual (such as unhelpful thoughts about insomnia, unable to relax), environmental (such as issues in sleep environment or equipment), and occupational factors (occupational participation and balance). We adopted the Person-Environment-Occupation-Performance (PEOP) model in design of the occupation-based programme as the model provides a comprehensive framework for organising and considering individual, occupational, and environmental strategies to address insomnia and sleep hygiene issues. In the person domain, we used psychoeducation to raise awareness and knowledge about sleep science, such as physiological and psychological factors related to sleep problems, sleep hygiene practices, and what methods are often effective in coping. Provision of accurate information helps people to take note of factors linked to insomnia and consider adopting more effective coping strategies.
In the environment domain, we assist the client to modify the sleep environment and select appropriate sleeping aids or adaptations (Gutman et al., 2017; Schoen et al., 2017). In the Occupation and Performance domains, we aim to facilitate participation in meaningful activities and promote occupational balance, using coaching strategies like self-exploration, action planning, and self-monitoring (Eklund et al., 2017). Occupational coaching is regarded as a core therapy skill in enabling occupations and participation under a client-centred approach (Kessler & Graham, 2015). Lifestyle coaching in this programme, is a form of occupational coaching that aims to facilitate self-understanding, encourage new experience and the formation of new habits, and is most suitable in promoting lifestyle redesign (Losch et al., 2016).
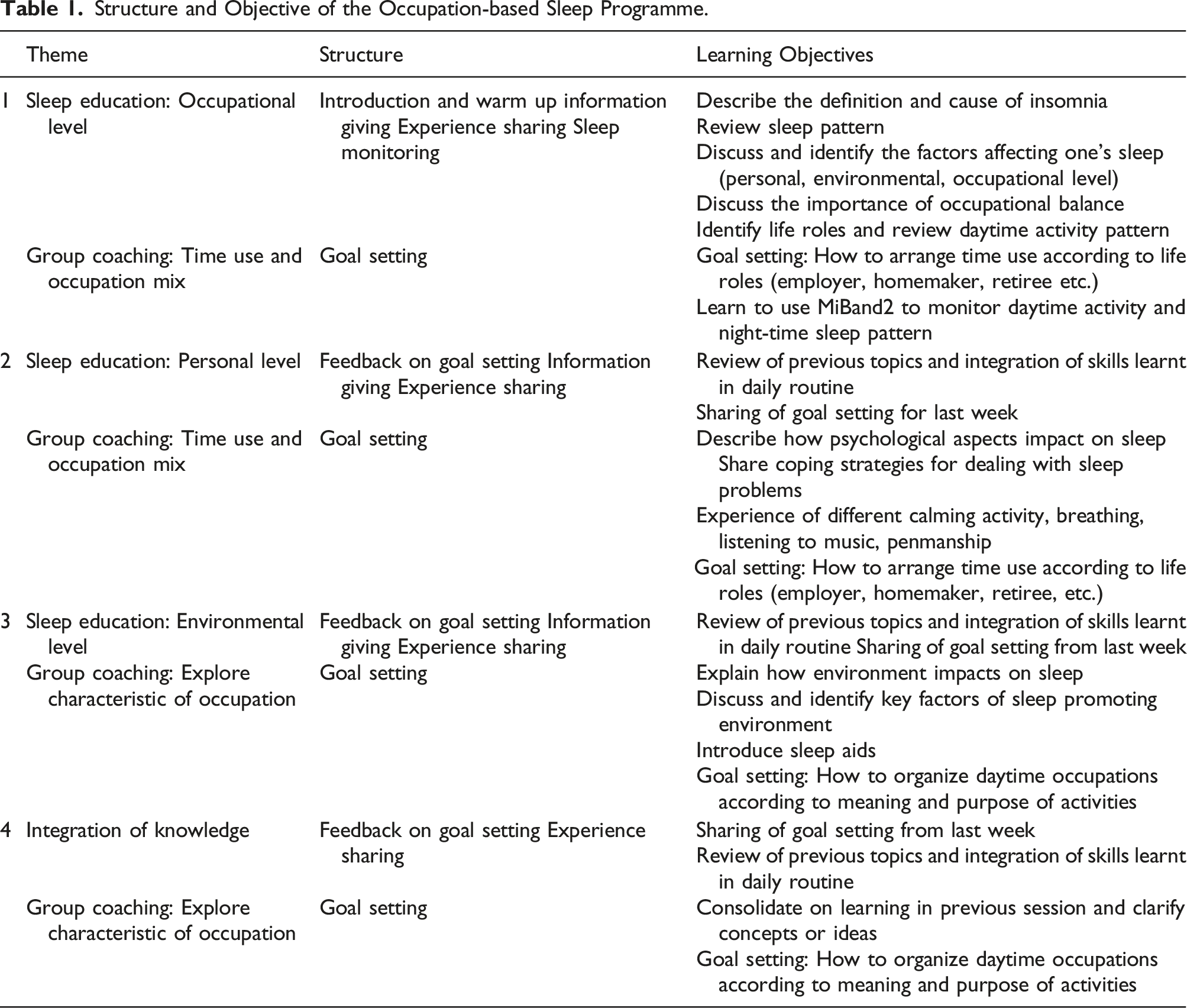
Structure and Objective of the Occupation-based Sleep Programme.
Method
This study investigated the effectiveness of an occupation-based sleep programme for patients with insomnia. It compares the treatment outcomes of sleep pattern, mood, and occupational balance between an intervention group (occupation-based sleep programme) and a Treatment as Usual (TAU) group (sleep hygiene education and relaxation training) upon completion of their respective programmes and at one-month follow up.
Due to practical limitations and feasibility issues, this study uses a quasi-experimental (non-equivalent group) design instead of a randomised controlled trial. The participants of the intervention group attended the occupation-based sleep programme in general outpatient clinic A, while participants in the comparison group received TAU in a general outpatient clinic B of another district. The three time-points for collection of outcome data are at baseline (T1), after the intervention (week 8) (T2), and a one-month post intervention follow up (week 12) (T3). (Figure 1). There is no randomisation of participants, and we implement single blinding of the assessors who conducted the outcome measures. Written consent was collected from participants and the study was conducted in accordance with the ethical protocol approved by the ethics committees of Hospital Authority in Hong Kong and the Institutional Review Board of the Hong Kong Polytechnic University. CONSORT flow diagram of sample selection.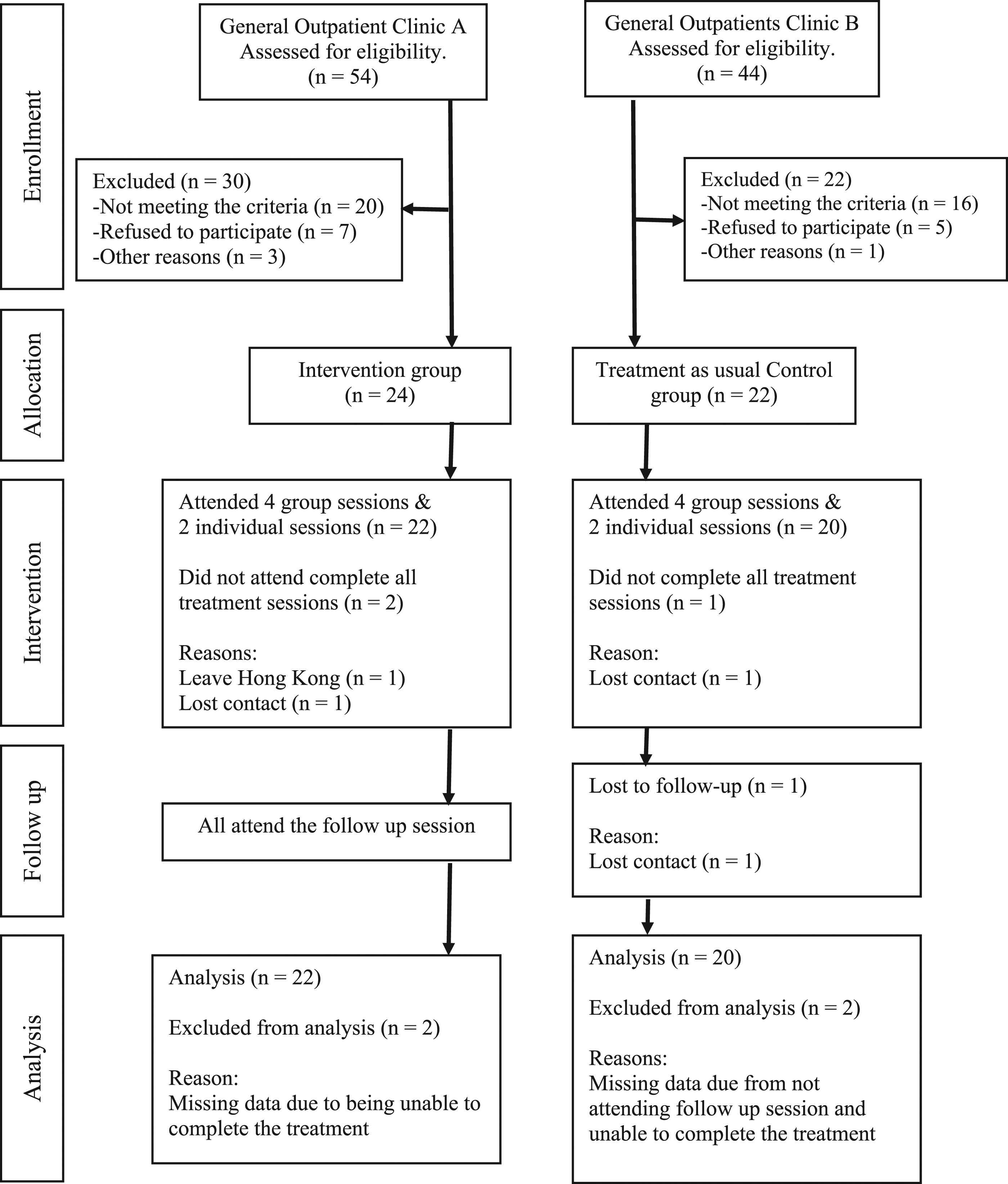
Participants
The required sample size was calculated based on the effect size of sleep quality improvement in a nonpharmacological sleep intervention, such as the CBTi. The meta-analysis by Okajima et al. (2011) suggested that nonpharmacological sleep intervention had a moderate to large effect on sleep quality in three RCTs based on the primary outcomes of sleep quality. Assuming α is .05 for a two-tailed test and a moderate effect size, we estimated that a the sample size of at least 17 participants is need for each group. (Cohen, 1988; Hintze, 2013). Assuming an attrition rate of 20%, it is proposed that each group comprise 22 participants. We need to conduct four intervention groups to cover 22 participants in each group, as four to six patients joined each intervention group.
The inclusion criteria for recruitment of participants are: (1) diagnosis of insomnia disorder, (2) referral by general practitioner; (3) aged 18–65 years old; (4) Insomnia Severity Index score over 14; (5) regularly uses a smartphone, which enable data synchronization with the MiBand2 activity wristband; (6) able to complete self-administered study questionnaires and (7) able to communicate in Cantonese. The exclusion criteria are: (1) diagnosis of severe mental illness; (2) Personal Health Questionnaire 9 (measures depressive symptoms), score over 19 and/or anxiety symptoms (General Anxiety Disorder 7 score over 15); (3) On regular pain medication during the last month, for more than 3 days per week); (4) sleep affected by respiratory disease or (5) regular user of alcohol or addictive substances.
Ninety-eight clients were referred to the programme in the two clinics during the recruitment period September 2018 to March 2019. Forty-six clients met the criteria in joining the study, including 24 from clinic A (intervention group) and 22 from clinic B (TAU group). Twenty-two participants in the intervention group and 20 participants in TAU completed their treatments, as well as all the assessments at three check points (Figure 1).
Instruments
The primary outcome measures of the study are insomnia and sleep quality, and the secondary measures are measures of occupational balance, depression, and anxiety. The questionnaires were distributed to participants by personal care workers in the general outpatient clinic after they attended the treatment sessions. Participants stayed anonymous as they were not required to provide personal identification on the questionnaires.
Cantonese Version Insomnia Severity Index (C-ISI)
The C-ISI is a self-report questionnaire that measures the severity of insomnia. Previous studies have reported adequate psychometric properties for both the English and Chinese versions (Baghyahi et al., 2011; Bastien et al., 2011). Internal consistency is excellent (α = 0.89–0.91). Sensitivity and specificity at cut-off score of 10 were 86.1% and 87.7%, respectively.
Chinese Version Pittsburgh Sleep Quality Index (C-PSQI)
The C-PSQI is a self-report questionnaire that measures sleep quality. The questions focus on seven aspects of sleep: (1) quality; (2) latency; (3) duration; (4) efficiency; (5) disturbance; (6) use of sleep medication; (7) daytime dysfunction. The psychometric properties of the PSQI have been well documented (Backhaus et al., 2002). The Chinese translated version demonstrated good internal consistency (α = 0.82–0.83), and acceptable test-retest reliability over a 14- to 21-day intervals (r = 0.77) for patient with insomnia. It demonstrated good convergent validity, with significant correlations with sleep quality-visual analogues scale and sleep diary. It could differentiate people with and without insomnia, with a sensitivity of 98% and a specificity of 55% (Tsai et al., 2005).
Activity Wristband
Activity wristbands are a type of commercial activity monitor (CAM) commonly used for measuring activity level and sleep pattern. Recent research stated that several types of CAM were good at detecting the actual time spent in bed for sleep research (Ameen & Hauser, 2019). MiBand2 was selected for this study as it could monitor a user’s sleep and physical activity and is affordable. It provides objective data on sleep duration on a weekly basis, including information about sleep duration, number of night-time awakenings, and typical sleeping habits.
Occupational Balance Questionnaire (OB-Quest)
The OB-Quest was developed to measure occupational balance in daily life. The internal consistency of the OB-Quest is 0.9, and test-retest reliability is also 0.9 (Dür et al., 2014). We have conducted a translation and validation study of the Chinese OB-Quest (Ho, Dür, Stamm, & Siu, 2020) which showed that the instrument demonstrated excellent test–retest reliability (ICC= 0.98) and good internal consistency (Cronbach’s α = 0.80). The instrument has a single-factor structure and could differentiate groups with different levels of insomnia severity and without insomnia.
Personal Health Questionnaire 9 (PHQ9)
PHQ9 is a self-administered questionnaire and is part of the Primary Care Evaluation of Mental Disorders (PRIME-MD) diagnostic instrument for common mental disorders (Kroenke et al., 2001). The PHQ9 has good reliability and validity for screening depression. PHQ9 (Elings, 2006; Löwe et al., 2004). The psychometric properties for patients with depression in a Chinese population were found to be acceptable to good (Chen et al., 2006).
General Anxiety Disorder 7 (GAD 7)
GAD7 is also part of the PRIME-MD diagnostic instrument for common mental disorders (Spitzer et al., 2006). GAD7 is good at screening a range of anxiety disorders in primary care (Kroenke et al., 2007). Previous studies have shown GAD7 to have a high degree of reliability and validity, as well as high internal consistency (Löwe et al., 2008).
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) (Version 25) was used for data analysis. Descriptive statistics were used to describe the demographic characteristics and outcomes. The baseline of the two groups were compared by t test and Chi-square. Repeated measure ANOVA (General Linear Model) was used to compare the effectiveness of the programme versus TAU group over the baseline, post treatment, and one-month follow-up. Post-hoc pairwise comparisons were conducted to examine specific changes in outcomes between different time points of measurement.
Results
Demographic Characteristics and Baseline Comparisons
Comparison of the Socio-demographic Characteristics of Intervention and TAU groups.
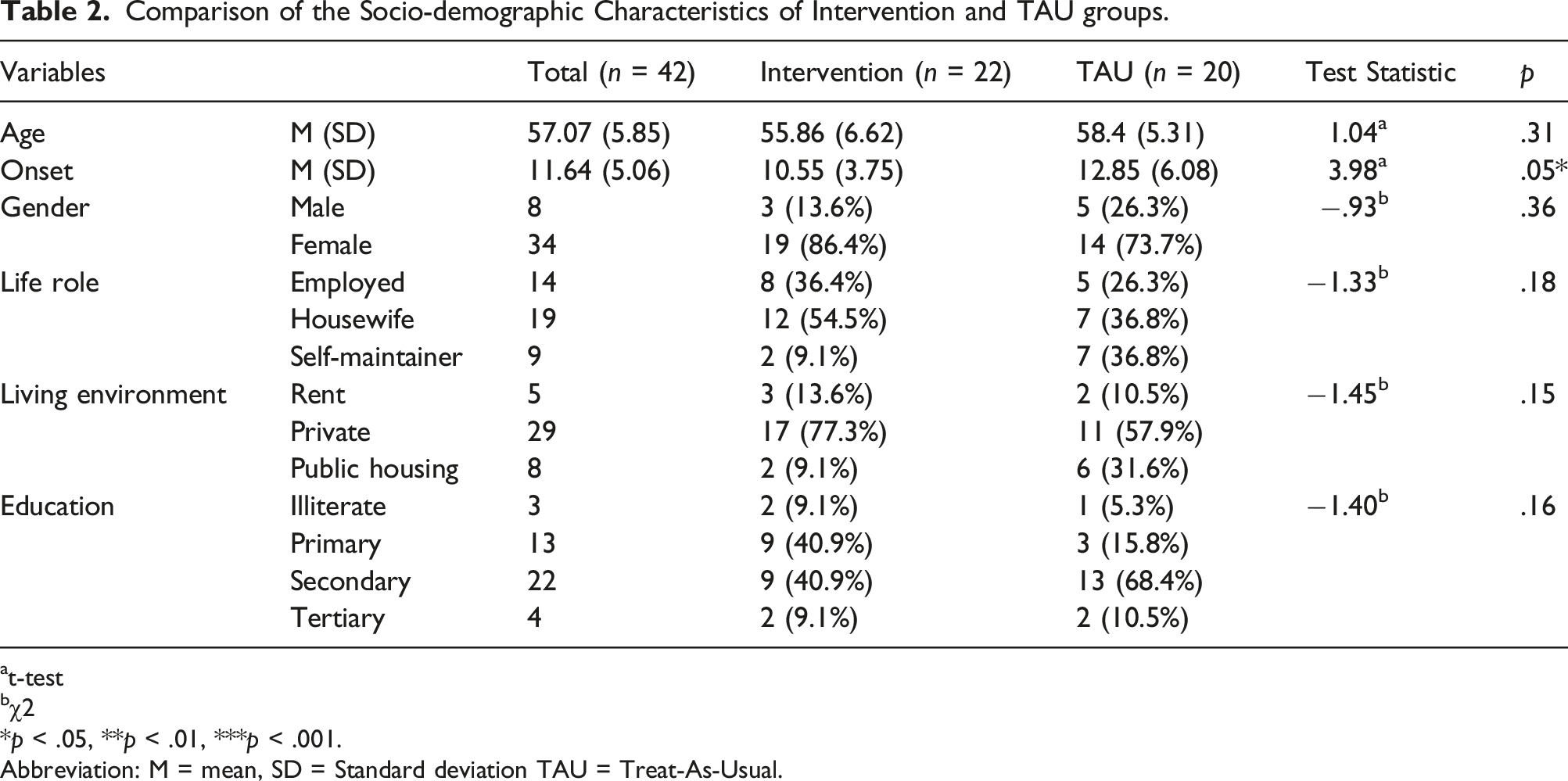
at-test
bχ2
*p < .05, **p < .01, ***p < .001.
Abbreviation: M = mean, SD = Standard deviation TAU = Treat-As-Usual.
Comparison of the Baselines in Sleep and Insomnia, Occupational Balance, and Mood Outcomes Between the Intervention and TAU Groups.
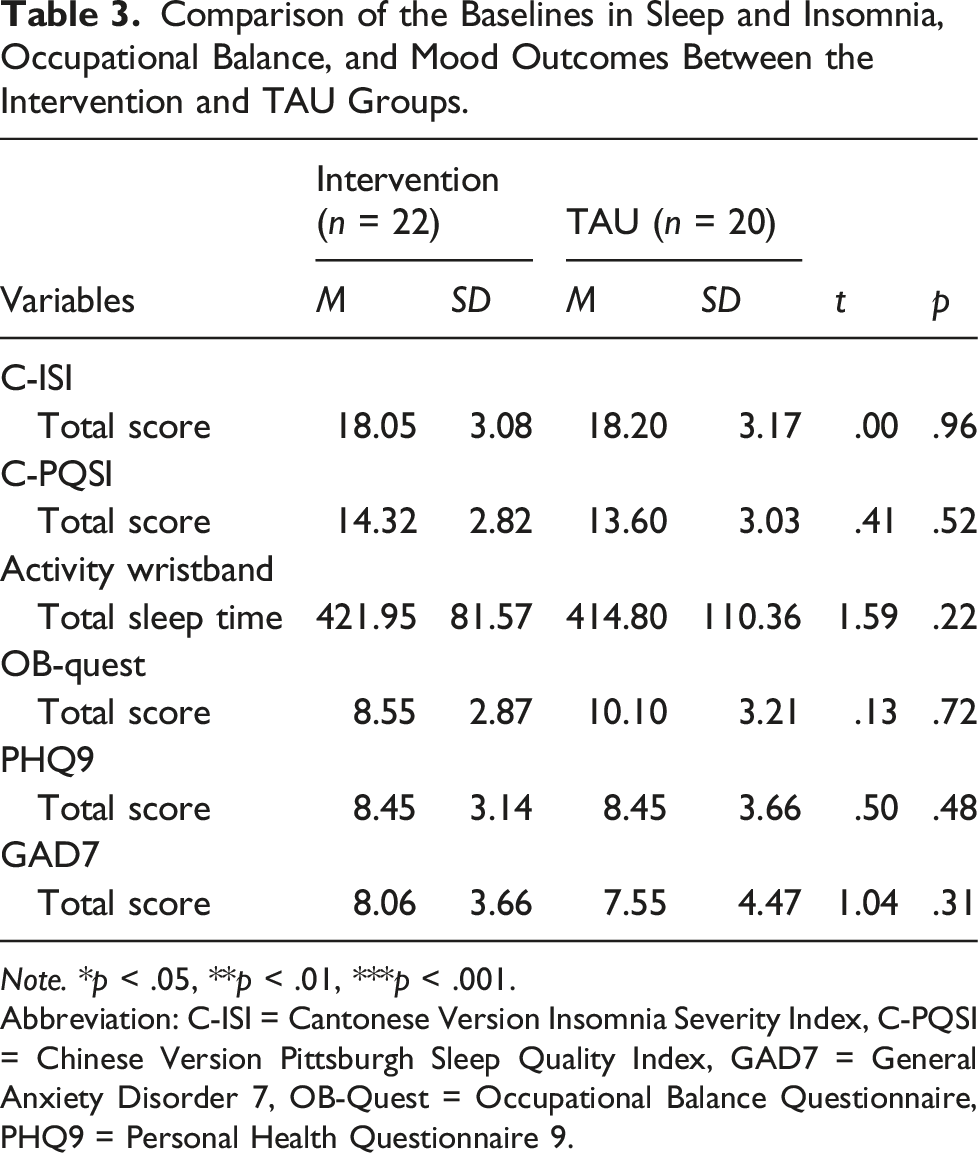
Note. *p < .05, **p < .01, ***p < .001.
Abbreviation: C-ISI = Cantonese Version Insomnia Severity Index, C-PQSI = Chinese Version Pittsburgh Sleep Quality Index, GAD7 = General Anxiety Disorder 7, OB-Quest = Occupational Balance Questionnaire, PHQ9 = Personal Health Questionnaire 9.
Changes in Sleep
Comparison of the Effects on Sleep Between Groups Among Three Repeated Measures Occasions.
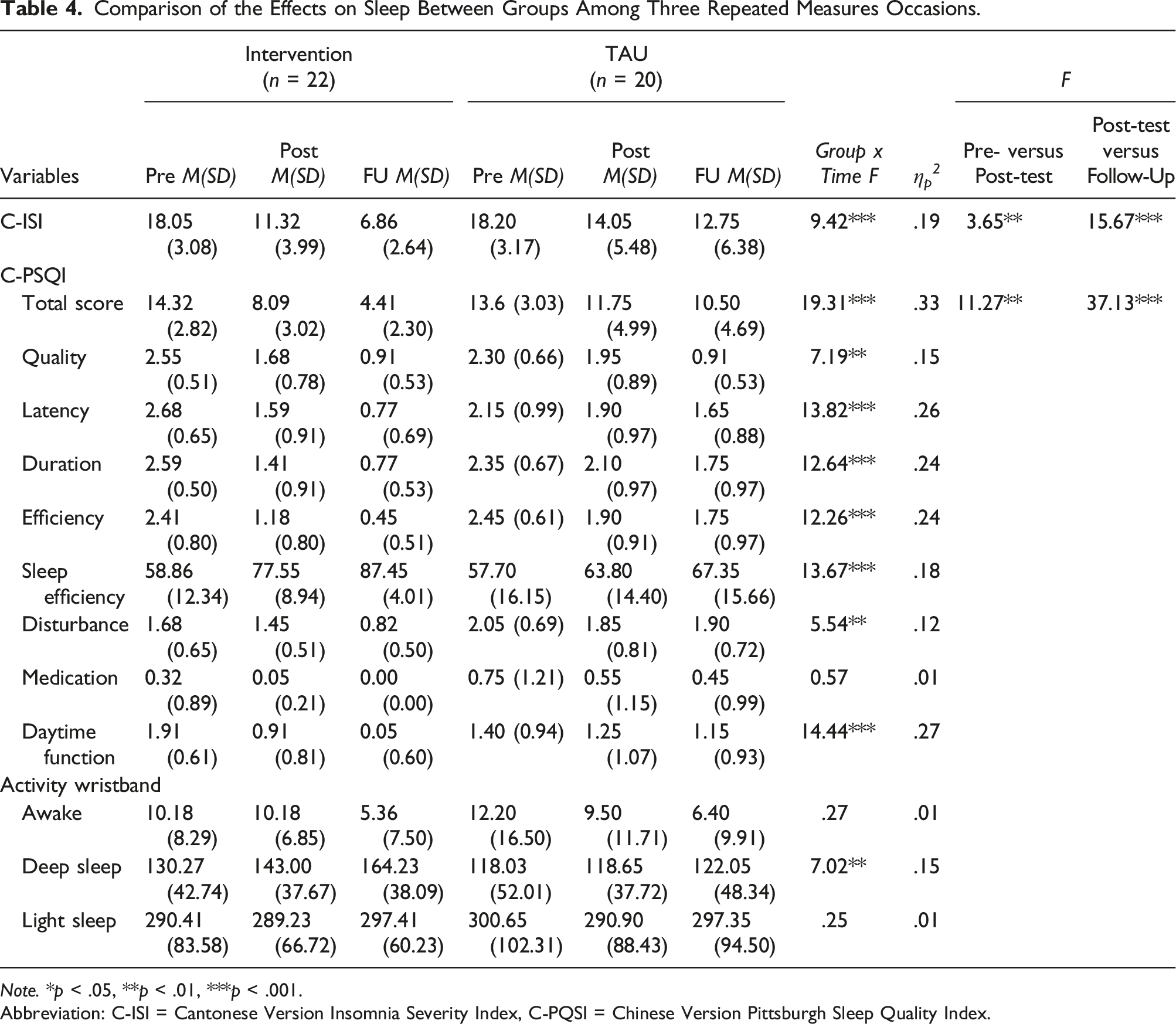
Note. *p < .05, **p < .01, ***p < .001.
Abbreviation: C-ISI = Cantonese Version Insomnia Severity Index, C-PQSI = Chinese Version Pittsburgh Sleep Quality Index.
The sleep pattern data captured by MiBand2 showed that there was significant difference between the two groups during the treatment period, but only for the deep sleep sub score (F = 7.02, p < .01) (Table 4). Total sleep time of treatment group increased from 422 minutes to 433 minutes at post treatment (n.s.), and then to 464 minutes at 1-month follow up (p < .05), demonstrating a clear trend of increasing sleep duration. For the TAU group, total sleep time remained unchanged during the study.
Changes in Occupational Balance
Comparison of Changes in Occupational Balance Between Groups Among Three Repeated Measures Occasions.
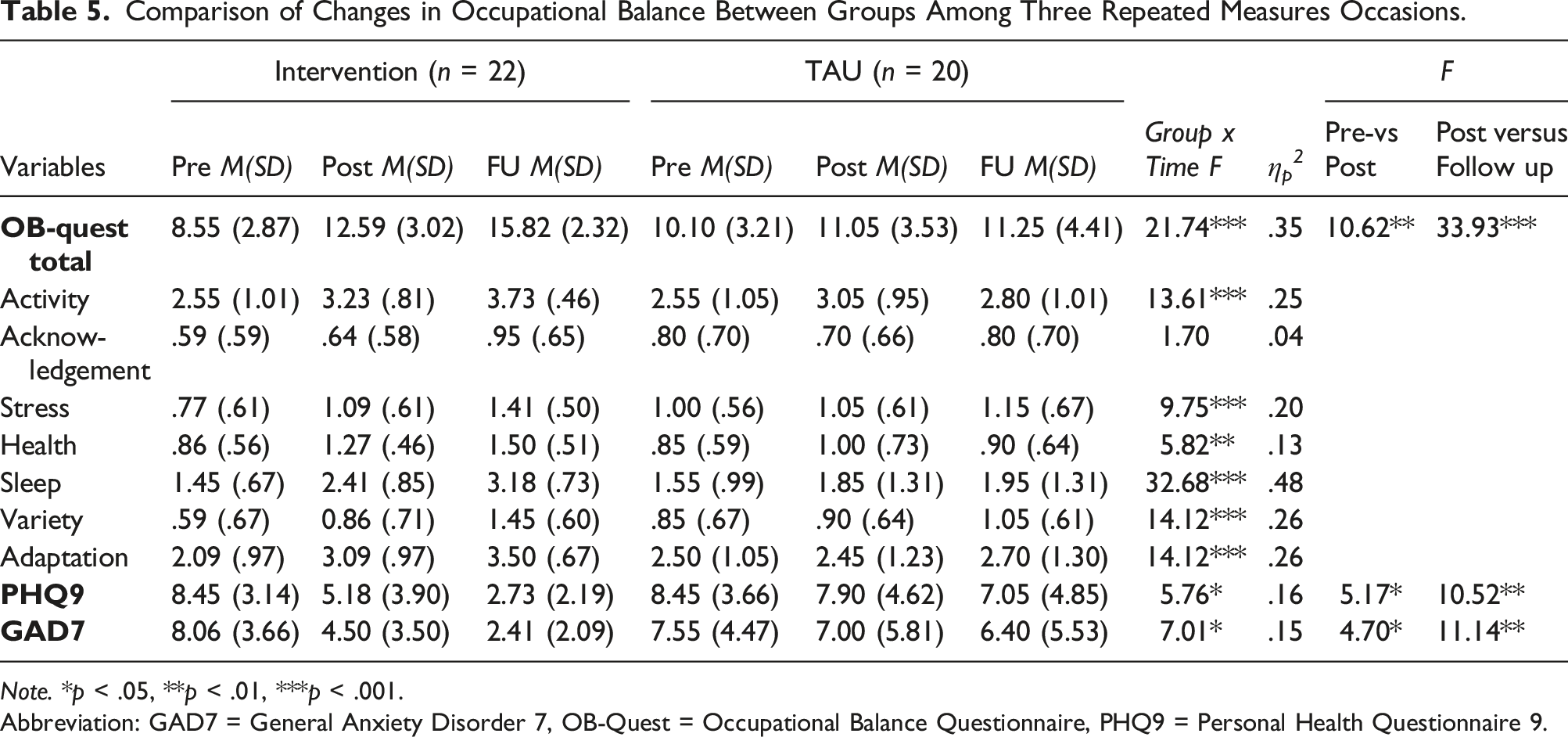
Note. *p < .05, **p < .01, ***p < .001.
Abbreviation: GAD7 = General Anxiety Disorder 7, OB-Quest = Occupational Balance Questionnaire, PHQ9 = Personal Health Questionnaire 9.
Changes in Mood
There was significant reduction in both GAD7 (F = 7.01, p < .05) and PHQ9 (F = 5.76, p < .05) in treatment group when compared with TAU group (Table 5). When we examined the contrasts among baseline, post-treatment and follow-up, there were significant and bigger changes between post treatment and follow-up period (p < .01), than between baseline and post treatment period (p < .05) for both PHQ9 and GAD7 (Table 5).
Discussion
There are several observations from the results of this study. First, the newly designed occupation-based sleep programme is more effective than the previous sleep hygiene programme (TAU). Sleep hygiene education often adopts the stress management framework and covers how substance use, sleep wake regularity, avoidance of daytime naps, and stress reduction methods may affect sleep. In fact, recent systematic reviews found that sleep hygiene programmes for insomnia are popular, but the effect size of these programmes tends to be small (Chung et al., 2018). The current occupation-based programme does incorporate elements of sleep hygiene education, but also add elements of daytime activity engagement, and modification of sleep environment and lifestyle. The significant improvement in outcomes in the occupation-based programme could be the effect of these additional elements.
Second, there are few published clinical trials of based sleep management programmes in occupational therapy, especially if it is designed for people with insomnia disorder. Many studies employed only a single type of intervention, such as sleeping aids (environmental modification), or Cognitive-behaviour Therapy for insomnia (CBT-I) (Ho & Siu, 2018; Smallfield & Molitor, 2018). The occupation-based intervention programme in this study reported a moderate effect size, which is lower than the high effect size reported in a recent study of an occupational therapist-led CBT-I intervention for veterans (Eakman et al., 2022). The differences in effect sizes between the CBT-I study and the current study, could be due to the differences in participants (veterans with chronic insomnia vs. adults with insomnia disorders, or cultural differences) as well as the interventions involved.
Third, this occupation-based sleep programme is developed based on theories of Person-Environment-Occupation-Performance (PEOP) and occupational balance (Baum et al., 2015; Eklund et al., 2017; Ho & Siu, 2018), and we theorise that it is important to work on occupational balance of people with insomnia. A large effect size of change in occupational balance is observed, especially over the follow-up period. The results are consistent with the hypothesis that occupational balance is closely linked to one’s sleep, and a change of activity mix during the day could improve occupational balance. This supports that occupational balance measures could be used as a regular outcome of occupational therapy programmes for insomnia, on top of standard outcomes like sleep duration and quality, or mood.
Fourth, we observed that the application of the coaching approach in the treatment group is crucial to the success of the occupation-based sleep programme. This contrasts with the TAU, which is mostly conducted using a psychoeducational approach. Over the coaching process, clients could gradually take up a more active role in goal setting and action planning for more engagement in meaningful activities during the day, and in management of their occupational balance. During the workshops, patients could learn from experience of each other, and the group interaction reinforced the engagement and motivation for change. This is consistent with research on coaching strategies in health care, which supported that it is an effective way to manage lifestyle health problems including obesity, diabetes, chronic ulcer, and chronic pain (Prah et al., 2017; van de Glind et al., 2012). Further studies could further examine how occupational coaching strategies could be systematically integrated into programmes for insomnia (Kessler & Graham, 2015).
Occupational therapy has long focused on activities of daily living, work, social and leisure activities, but few have focused on sleep (Ganjikia & Gansor, 2015). In view of the rising needs of people with insomnia in modern societies, there is a need to develop standardized occupation-based sleep programme in primary care. The current study illustrates the importance of developing a new programme based on integration of theoretical framework and clinical experience. The results of this study demonstrate that an occupation-based sleep management programme could be implemented effectively in a primary care setting. The standardization of the programme and teaching materials can facilitate the training of primary care therapists. To further consolidate the role of occupational therapist in primary care, more attempts need to be made to design new programmes and conduct evidence-based research.
Study Limitations
This study has several limitations. First, the participants of TAU and intervention group were recruited from two primary care clinics and the two programmes were conducted at the two settings by two different therapists. We used a non-equivalent group design for this study as the ethics committee of the clinics did not support the randomization of participants or the delayed treatment of patients (such as use of waiting-list control group). Thus, there was no randomization of subjects and could introduce bias to subject allocation for the two groups. To address these weaknesses in the experimental design, we compared the differences of the two groups at baselines to see if there might be systemic differences between groups affecting the outcome measures.
Second, we only had a one-month follow-up on the outcomes, as we did not have the resources to conduct a longer follow-up on the subjects. The results showed that improvements in sleep, mood, and occupational balance were larger between post treatment to 1-month follow up, when compared with the TAU group. A three-to six-month follow up would be more favourable for examining changes in occupational balance and lifestyle. Third, the activity wristband data only measured an individual’s activity level, it was not a direct measure of sleep time or quality. If budget allows, researchers could use research-grade actigraphs for measuring activity or electroencephalograms for measuring sleep (Brand et al., 2014), which would provide more precise outcome measures of sleep and insomnia.
Third, due to limitations of time and manpower, the sample size was small but it was sufficient to meet the minimum power requirement. In future, a multicentre study with a larger sample size over a more extended period could be conducted to reinforce the statistical analysis and the generalizability of the results.
Conclusion
An occupation-based sleep programme was developed based on the Person-Environment-Occupation-Performance model and theory of occupational balance. Our findings showed that the occupation-based sleep programme was more effective than the TAU (sleep hygiene programme) in increasing sleep duration, improving occupational balance, and in reducing mood symptoms. In general, there were more positive changes in the follow-up outcomes than during the intervention period. Coaching strategies that were delivered individually and in groups, are possible drivers of the change during the intervention.
The results of the present study demonstrated positive outcomes in treating insomnia in the Hong Kong Chinese population and could be adopted as a standard treatment in primary care. The design of occupation-based sleep management programmes should address the issues of occupational balance and lifestyle on top of conventional psychoeducation on sleep hygiene or environmental modifications. This study proposed a model of sleep management which combined group intervention with individual coaching on occupational balance, and demonstrated the role of occupational therapy in sleep management in primary health care which could be added to the evidence of occupational therapy in mental health.
Footnotes
Author Contributions
EH researched literature, conceived the study, designed the treatment programme. Both EH and AS were involved in protocol development, gaining ethical approval. EH conducted patient recruitment and the interventions. Both AS and EH were involved in the data analysis. EH wrote the first draft of the manuscript, and AS further improved the draft for submission. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Full ethics approval of this study was obtained from the Institutional Review Board of the Hong Kong Polytechnic University (Reference Number: HSEARS20180610001). The procedures followed were in accordance with the ethical standards of relevant institutional or national bodies and consistent with the revised (2000) Helsinki Declaration.
Informed Consent
All subjects were informed of the study’s risks and benefits, and written informed consent were obtained; the participation of subjects was voluntary, and that their identity would not be disclosed. The research data was only accessible and handled by the authors, who followed guidelines in keeping data confidential, encrypted, and secured.
Trial Registration
The study was registered on ClinicalTrails.gov (Identifier: NCT04940975).