
Abstract
Objective
To examine the effect of different management methods on the effectiveness of care preventive programmes for community-dwelling older adults.
Methods
This study comprised two facilitator-led (FL) and one participant-led (PL) preventive care classes in Japan. All participants received the intervention for approximately 12 weeks. Functional assessments, occupational dysfunctions, and subjective health were measured before and after the interventions. A two-way mixed design analysis of covariance (ANCOVA) was adopted to examine the effect of the interventions, adjusted for previous experiences with preventive care services. The level of significance was set at P < 0.05.
Results
Fourteen participants in the PL group (76.64 ± 6.48 years, 92.9% women) and 29 participants in the FL group (76.55 ± 5.75 years, 75.9% women) were included in the statistical analysis. ANCOVA showed significant group × time interaction effects in the Five Times Sit-to-Stand Test (FTSST), the Timed Up & Go (TUG), occupational deprivation of the Classification and Assessment of Occupational Dysfunction Scale, and self-rated health. Simple main effect tests showed that the TUG decreased significantly in the PL group, while occupational deprivation and self-rated health scores improved significantly. In contrast, FTSST scores significantly improved in the FL group.
Conclusion
PL-type management may be more appropriate for preventing social isolation and withdrawal, while FL-type management may be more appropriate for preventing physical frailty. Selecting not only adequate programmes but also an appropriate management type that matches the service purpose can help provide more effective care preventive services.
Introduction
Japan has the fastest ageing population and highest ageing rate in the world (Statistics Bureau Ministry of Internal Affairs and Communications Japan, 2018). The ageing rate was 28.1% in 2018, and about one in four people was an older adult (Cabinet Office Japan, 2015). Per Saito et al. (2019, p. 570), ‘the measures for long-term preventive care that the Japanese government had introduced in 2006 were unsuccessful because of the failures to identify high-risk individuals and to enrol enough participants in the community prevention programme’. The Japanese government shifted its primary strategy from a high-risk strategy to a community-based population strategy in 2015 by reforming the Long-term Care Insurance Act (Saito et al., 2019), including increasing the emphasis on community-based care and social determinants of health and requiring support from rehabilitation professionals to strengthen preventive care efforts.
One preventive care service offered by municipalities is a day-care programme for community-dwelling older adults called ‘preventive care class’, supported by professionals (Health and Welfare Bureau for the Elderly & Ministry of Health Labour and Welfare, 2016). The cost ranges from zero to several hundred dollars. The programme includes lectures, exercise, and recreational and creative activities. Previous studies have shown that such programmes, especially those focusing on physical activity, had positive effects on motor function (Chan et al., 2016; Fujimoto et al., 2011; Kamegaya et al., 2016), instrumental activities of daily living (IADL; Fujimoto et al., 2011), social participation (Araújo & Ribeiro, 2011; Uchiyama et al., 2011), cognitive function (Kamegaya et al., 2012, 2016), and subjective health (Araújo & Ribeiro, 2011; Chan et al., 2016), and prevented the occurrence of care-requiring conditions (Fujimoto et al., 2011; Yamada et al., 2012) and depression (Uchiyama et al., 2011). Thus, although research has progressed on the development of effective preventive care programmes, studies that measured programme effectiveness made little reference to their management.
Recently, clients’ active participation in their own medical treatment and health research has been recommended (Mader et al., 2018; Vayena et al., 2016). Clients usually understand their disease and lifestyle better than many healthcare professionals and have a unique perspective on what benefits them most (Mader et al., 2018). Regarding patient-led diabetes control, studies reported improvements similar to (Riveline et al., 2012) or better than (Garg et al., 2015) physician-led control. Additionally, regarding rehabilitation for older clients, patient-led therapy has been reported to increase self-management level and self-rehabilitation time (Tijsen et al., 2019). Client-led treatments and therapies can motivate clients (Sønsterud et al., 2019) and increase their engagement (Hambleton, 2016).
Taguchi et al. (2019) conducted a literature review of programmes that train community volunteers for preventive care activities, divided into two types: one in which the planner determined activities beforehand and one in which participants were involved in planning activities. Taguchi et al. (2019) conducted a programme based on the latter, and reported significant improvements in participants’ understanding of community issues and confidence in tackling their own preventive care. However, the two types’ effect on programme effectiveness has not been clarified. Therefore, we conducted two programmes, one led by participants and the other by facilitators. We focused on the impact of these participant-led (PL) and facilitator-led (FL) programmes on intervention effects in preventive care programmes. Understanding the impact of these types could enable more effective operation of preventive care programmes.
This study clarifies the effects of the PL and FL management types on the effectiveness of long-term care preventive programmes for community-dwelling older adults.
Materials and methods
Participants
In B Ward, A City, Hokkaido, we asked preventive care centres commissioned by A City and providing preventive care services in B Ward to participate. We introduced one PL and two FL preventive care classes. The study purpose was explained to participants, and their participation was requested. The selection criteria were age ≥ 60 years, independently living in a community, and having adequate cognitive and Japanese language capabilities for effectively responding to questioning. The exclusion criterion was the inability to answer the questionnaire on their own. Twenty-nine participants in the PL class and 62 in the FL classes provided verbal and written consent to participate.
Programme content and two operation types
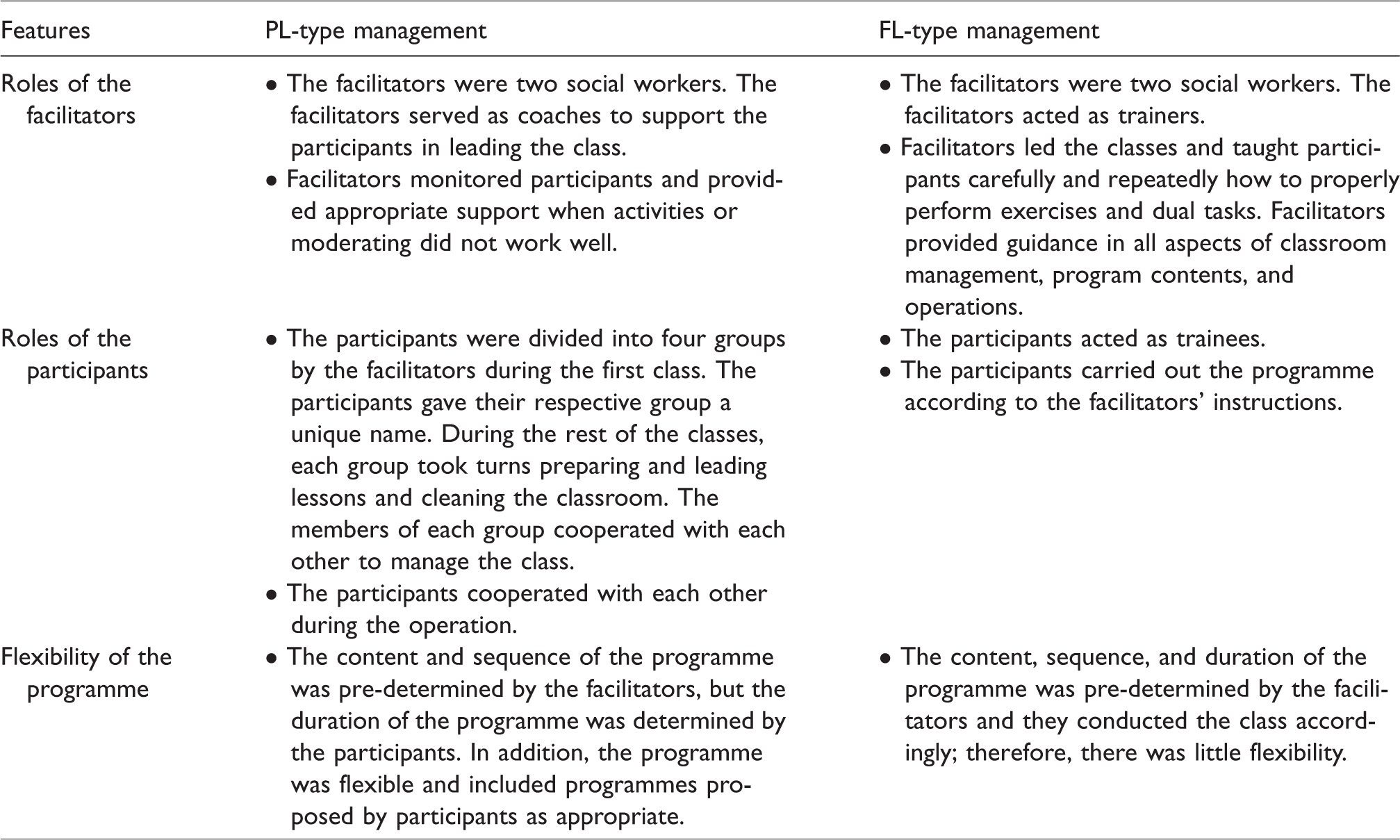
The classes were 90 minutes long and held once weekly or biweekly for a total of 10-12 classes from September to November 2018. All classes comprised the following contents: three types of preventive exercises, dual exercise and cognitive tasks, recreation, group work, and lectures. All preventive exercises were created in that location, were performed on the spot in a sitting or standing position, and involved no walking. The programme content was standard practice in B Ward’s prevention classes. All groups had two social workers as facilitators. The roles of each group’s participants and facilitators and the programme flexibility are summarised in Table 1.
Features of participant-led (PL) and facilitator-led (FL) management types.
All facilitators were trained in preventive care knowledge and skills. Additionally, the first author, an occupational therapy student, and/or the second author, an occupational therapist, conducted supplementary observation of the operation status of both groups.
The Ethics Committee of the Faculty of Health Sciences at Hokkaido University approved the study protocol (Approval number 18-53-1).
Measures
Participants completed a demographic questionnaire (age, gender, and previous participation in a long-term preventive care class). The effectiveness of the preventive care programme was measured through functional assessments, occupational dysfunctions including IADL, and subjective health, which previous studies have shown to be effective (Araújo & Ribeiro, 2011; Chan et al., 2016; Fujimoto et al., 2011; Kamegaya et al., 2012, 2016; Uchiyama et al., 2011; Yamada et al., 2012).
Functional assessments
Physical functions were assessed with the Five Times Sit-to-Stand Test (FTSST) and Timed Up & Go (TUG). The FTSST assesses functional lower extremity strength, transitional movements, balance, and fall risk. Participants are asked to stand up straight as quickly as possible five consecutive times without resting in between. The TUG is evaluates balance and fall risk. Participants are asked to stand up and move as quickly as possible along a three-metre path, walk back, and sit in the chair correctly with their back resting against the chairback while being timed.
Automatic thoughts, a psychological function, were assessed by the Automatic Thoughts Questionnaire-Revised (ATQ-R; Kendall et al., 1989). The Japanese version’s reliability and validity have been verified (Eguchi & Kunikata, 2015; Kodama et al., 1994). This questionnaire assesses the frequency of automatic positive (10 items) and negative (30 items) statements about oneself. All items are scored on a 4–point Likert scale, simplified for older adults, where 1 represents ‘not at all’ and 4 ‘all the time’. Higher scores reflect a greater number of positive and negative automatic thoughts.
Occupational dysfunctions
The Classification and Assessment of Occupational Dysfunction Scale (CAOD), a self-reported questionnaire, assesses occupational dysfunction status, defined as having negative experiences during daily activities (Teraoka & Kyougoku, 2014). This assessment includes four items for each of four occupational dysfunction domains: occupational imbalance, deprivation, alienation, and marginalisation (Teraoka & Kyougoku, 2014, 2015). All items were scored on a 7–point Likert scale, with 1 representing ‘not at all’ and 7 ‘all the time’. The cut-off point was set to 52, with a higher score reflecting greater occupational dysfunction risk. The Cronbach’s alpha was 0.902, indicating acceptable internal consistency.
The Japan Science and Technology Agency Index of Competence (JST-IC) (Iwasa et al., 2015, 2018) assesses occupational dysfunctions in social occupations and includes four domains: technology usage, information practice, life management, and social engagement. Each has four items scored with 1 representing ‘yes’ and 0 representing ‘no’.
Subjective health
Self-rated health was measured by one item, ‘How do you feel about your health condition,’ with response options of 1 ‘very good’, 2 ‘good’, 3 ‘fair’, 4 ‘poor’, and 5 ‘very poor’. This index is a simple five-step evaluation method that older adults can easily answer (Kodama et al., 2018) and is used in the Ministry of Health Labour and Welfare of Japan’s ‘Basic Survey of Living Conditions of the People’ (2019).
Statistical analysis
To examine the difference between the groups before the intervention, the demographic variables and each scale’s outcome score at baseline were statistically compared by an unpaired t-test or chi-squared test.
Sixteen participants who attended similar programmes before were included in the FL group. Landi et al.’s study (2018) suggests that people who have habitual physical activity show better physical performance. Therefore, to examine intervention effects and regulate the effect of prior preventive care services, we adopted a two-way mixed design analysis of covariance (ANCOVA). We set group (PL or FL) and time (pre- or post-intervention) as factors and previous preventive care services experiences (yes or no) as a covariate assigned a set of dummy variables (No = 0, Yes = 1).
We focused on the group-by-time interaction because our interest was the intervention programme’s effectiveness. Significant interactions indicate that the intervention programme’s effects differ in each group. If significant interaction was found, simple main effect analysis was conducted.
Participants with missing values in pre- or post-intervention assessments were removed from the statistical analyses (pairwise deletion). Statistical analyses were performed using SPSS Statistics 22.0 (IBM SPSS Inc., Chicago, IL, USA). The level of significance was set at P < 0.05.
Results
Ninety-one participants were recruited (29 PL and 62 FL). Nineteen participants dropped out after the first few sessions (eight PL and 11 FL), and 29 did not complete the post-evaluation because of emergent health problems, schedule conflicts, or inconvenient accessibility due to heavy snow (seven PL and 22 FL). Ultimately, 43 participants (14 PL and 29 FL, 47.3% of recruited participants) were included in the statistical analysis.
Table 2 shows the results of the basic characteristics at baseline and a comparison of each assessment score between groups. The average ages were 76.64 ± 6.48 years in the PL group (92.9% women) and 76.55 ± 5.75 years in the FL group (75.9% women). The PL and FL groups were significantly different in total JST-IC score (t = −2.072, P = 0.045) and occupational deprivation (t = 2.075, P = 0.045). No statistically significant difference was observed for any other variable.
Sample demographic characteristics.
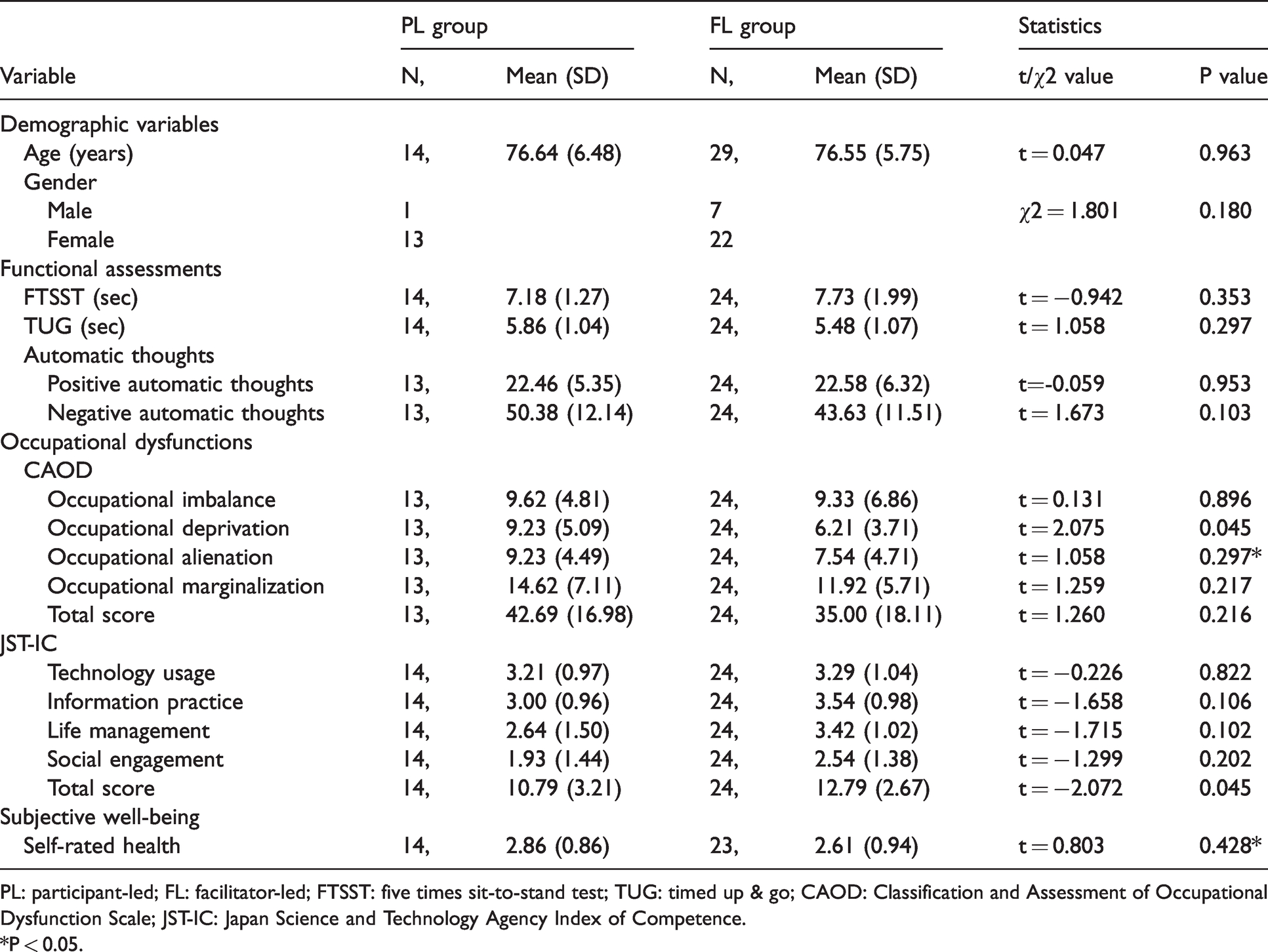
PL: participant-led; FL: facilitator-led; FTSST: five times sit-to-stand test; TUG: timed up & go; CAOD: Classification and Assessment of Occupational Dysfunction Scale; JST-IC: Japan Science and Technology Agency Index of Competence.
*P < 0.05.
All PL participants participated in the preventive care class for the first time, while 44.8% of the FL participants had previously participated. Table 3 shows ANCOVA results after regulating the effect of the previous experiences of preventive care services. Significant group × time interaction effects were observed in FTSST (F (1,35) = 4.726, P = 0.037), TUG (F (1,35) = 12.443, P = 0.001), self-rated health (F (1,34) = 4.155, P = 0.049), and occupational deprivation measured by CAOD (F (1,34) = 14.860, P = 0.0005) scores. Additionally, significant main effects of time were observed in positive automatic thoughts score (F (1,34) = 7.445, P = 0.010). The positive automatic thoughts score declined after intervention for both groups.
Results of the two-way mixed ANCOVA for all clinical variables.
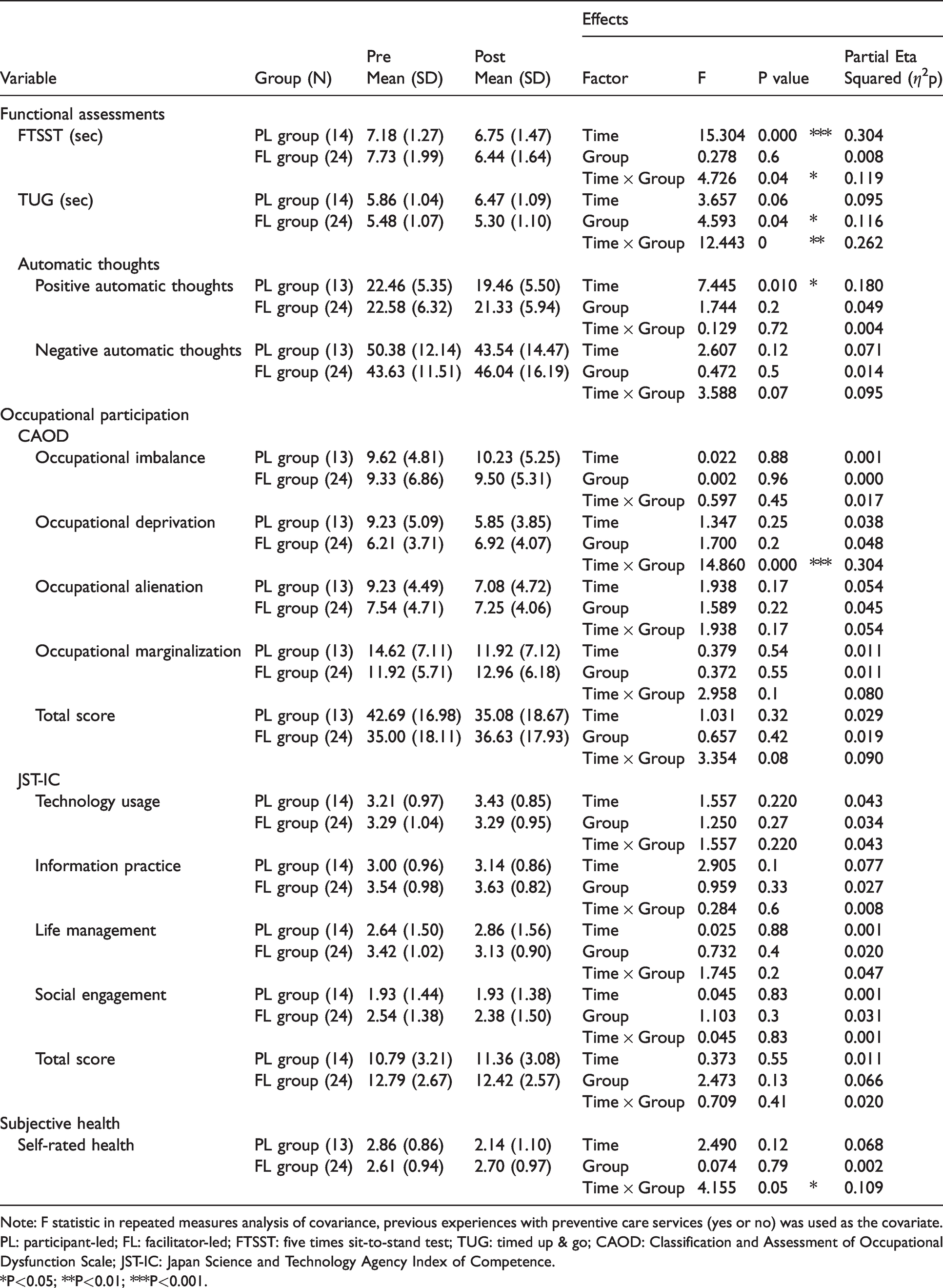
Note: F statistic in repeated measures analysis of covariance, previous experiences with preventive care services (yes or no) was used as the covariate.
PL: participant-led; FL: facilitator-led; FTSST: five times sit-to-stand test; TUG: timed up & go; CAOD: Classification and Assessment of Occupational Dysfunction Scale; JST-IC: Japan Science and Technology Agency Index of Competence.
*P<0.05; **P<0.01; ***P<0.001.
To further examine the interaction, a simple main effect test was performed for the FTSST, the TUG, self-rated health, and occupational deprivation (Figure 1).
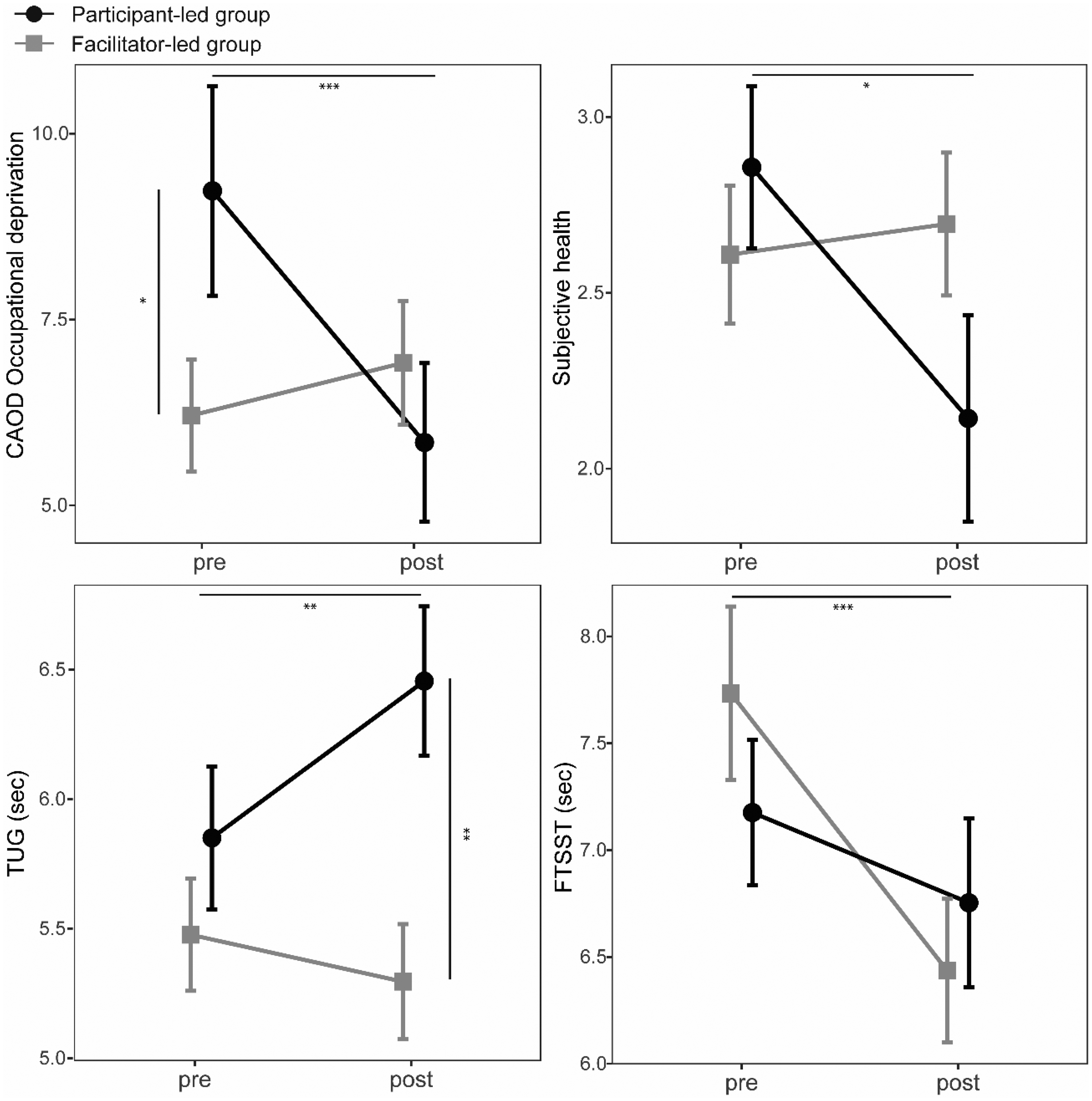
Score plot for FTSST, TUG, subjective health, and occupational deprivation on intervention time between groups. Previous experiences with preventive care services (yes or no) was used as the covariate. The x axis shows assessing time as pre-intervention and post-intervention; the y axis shows the score of each variable. FTSST: Five Times Sit-to-Stand Test. TUG: Timed Up & Go. Dot and square reflect mean values. Error bars reflect standard errors. *P<0.05. **P<0.01. ***P<0.001.
For the FTSST, the simple main effects of time in the FL group were significant (F (1,35) = 26.485, P < 0.001). The FL group’s FTSST time became shorter after intervention.
For the PL group’s TUG, the simple main effects of time (F (1,35) = 13.144, P = 0.001) reached significance. The simple main effects of group at post-intervention also reached significance (F (1,35) = 8.575, P = 0.006). After the intervention, the PL group’s TUG scores declined, and the FL group had better scores than the PL group.
For the PL group’s self-rated health, the simple main effects of time were significant (F (1,34) = 5.954, P = 0.020). Their self-rated health improved after intervention.
For the PL group’s occupational deprivation, the simple main effects of group at pre-intervention (F (1,34) = 7.423, P = 0.010) and of time (F (1,34) = 15.897, P < 0.001) reached significance. That is, their score for occupational deprivation was significantly higher than the FL group’s at pre-intervention and improved significantly after intervention.
Discussion
This study investigated preventive care classes in Japan to examine the effects of PL and FL management types on the effectiveness of long-term preventive care programmes for community-dwelling older adults. ANCOVA showed significant group × time interaction effects for the FTSST, the TUG, occupational deprivation measured by CAOD, and self-rated health. Simple main effect tests showed that the PL group’s TUG decreased significantly, while occupational deprivation measured by CAOD and self-rated health scores improved significantly. In contrast, the FL group’s FTSST significantly improved. Additionally, there was a main effect of time on positive automatic thoughts, and its scores significantly decreased in both groups.
Occupational deprivation is a lack of opportunity for daily activities, such as hobbies, favourite activities, or activities one values, beyond the individual’s control (Teraoka & Kyougoku, 2015; Whiteford, 2000). ANCOVA showed significant interaction effects for occupational deprivation, and PL group scores were significantly improved. For PL group participants, this may suggest that the preventive care class itself became their important occupation. While the FL group participants acted in the classes under the guidance of the facilitators, the PL group participants had to be more actively involved in class operations. This autonomy difference may explain how the class became an important occupation for participants. Occupational deprivation involves the violation of the occupational right to participate in a range of occupations for health and social inclusion (Townsend & Wilcock, 2004). Our results indicate that PL-type preventive care services could promote social inclusion of older participants by improving their occupational deprivation.
Older adults are more susceptible to loneliness and social isolation and are at higher risk of various health and social problems directly linked to loneliness (Dury, 2014). Mentoring and friendship-making models have shown evidence for improving older adults’ loneliness and social isolation (Dury, 2014). PL participants were divided into groups, and the group members cooperated with each other to manage the class (Table 1). This may have facilitated mentor-mentee and friend-to-friend relationship development. Therefore, PL-type management is more appropriate for preventive care services aimed at preventing social isolation and withdrawal among community-dwelling older adults.
The PL group also showed significant self-rated health improvement compared with the FL group. In Ronzi et al.’s (2018) literature review, interactions, relations, and feeling valued were identified as potential mediators of improved health outcomes for interventions that foster respect and social inclusion in community-dwelling older adults. The participants played the leading roles in the PL-type management, and they and the facilitators were responsible for management (Table 1). Therefore, PL management not only promoted good relations among participants but may also have provided opportunities for feeling valued. Additionally, the qualitative research on older adults’ subjective health experience included remaining in familiar surroundings and having a sense of belonging (Ebrahimi et al., 2013). The opportunities for good interactions and feeling valued may have increased participants’ feelings of belonging. Thus, we believe that PL management improved participants' subjective health.
FL participants had more experiences of being supported by facilitators, while PL participants had more experiences supporting others because they partook in class management. Abolfathi Momtaz et al. (2014) found that supporting others had a twofold effect on the improvement of older adults’ subjective health compared with being supported by others. Therefore, the PL group’s subjective health might have improved more than that of FL group.
Regarding motor function, the PL group’s TUG significantly decreased, while the FL group’s FTSST significantly improved. The programme affecting motor function consisted mainly of three types of preventive exercises, all performed on the spot without walking. The movements these exercises required were more similar to those required in the FTSST than the TUG. This may have resulted in better FTSST improvement. Additionally, FL participants were able to learn and implement appropriate exercise programmes under facilitator guidance. In the PL group, however, detailed guidance may not have been provided because the participants were responsible for moderating the exercises. Thus, FL participants may have received more appropriate effects from the exercise programmes. The programmes were conducted from autumn to winter, and post-intervention assessments were conducted during the snowfall season. The average number of steps taken by older adults in northern Japan is significantly lower during the snowfall period than during the non-snowfall period (Hasegawa et al., 2018). PL participants may not have fully benefitted from the exercise program, and their TUG scores may have worsened due to decreased activity related to the weather.
Eyssen et al. (2013) noted that a client-centred intervention was associated with improved client satisfaction, but the effect on functional health-related outcomes was not well evaluated. They compared client-centred and usual care occupational therapy with a client-centred process framework in clients with multiple sclerosis. There was no significant difference in measures of disability, participation, or autonomy, but fatigue (physical scale and total scale) and health-related quality of life (bodily pain and vitality) were better in the usual care group.
Miller and Fritz (2019) argues that patient-centred care should not mean patient-led care. He noted that patient-led care can have adverse outcomes, including harm via lack of responsibility, neglect, a widening health gap, missed diagnoses, and mental health impact. Occupational therapy is a client-centred health promotion (World Federation of Occupational Therapists, 2018), and a client-based approach is undoubtedly important. However, client-led and client-centred approaches may need to be understood separately. Leone et al. (2013) argue that experts can consider objective clinical data to make a priori decisions regarding physical function regardless of the client's subjective experience with the disease, even when occupational therapy is client-centred. Similarly, regarding preventive care, providing expertise and guidance through the FL approach, especially in areas that can be measured by objective indicators such as motor function, may result in participant-centred care. These results suggest that appropriate facilitator guidance is important in preventive care services aimed at maintaining and improving participants’ motor function and that FL management is more effective.
There were no significant changes in JST-IC scores in either group. The PL group had 70% and the FL group had 80% of the functional capacity to reach the performance indicators for living actively in the community (Table 1). Because the average for a 75-84 year old was about 50% in a national-level survey (Iwasa et al., 2015), our participants were high-functioning community-dwelling older adults who had few difficulties in daily occupational performance. The participants’ IADL performance may already have been high before the intervention and, thus, JST-IC scores were not improved. However, their functions also may have been maintained in both groups.
Finally, our results showed a significant reduction in positive automatic thoughts in both groups. Positive automatism was reported to have decreased in depressed patients (Beshai et al., 2016; Jolly & Wiesner, 1996). In Lindsay-Smith et al.’s (2019) study, no changes in psychological health-related quality of life were observed after six and twelve months in groups of community-dwelling older adults who performed physical or social activities. However, group interview results suggested that both programmes’ social aspects offered benefits in terms of stress mitigation and psychological health. This result is contradictory to ours, in which participants' positive automatic thoughts were reduced through programmes that included physical and social activities, regardless of how they operated. Our study period was about 12 weeks, considerably shorter than that of the previous study. The differences in the duration of the interventions may have caused inconsistencies with the previous results. In this regard, it is necessary to collect qualitative data, such as more detailed participatory observations and interviews on the situation of the exchange between group members and its change over time.
Limitations
In this study, the intervention was conducted with referrals from three preventive care classes with different management methods (PL and FL). Therefore, the allocation of participants could not be controlled, and all PL participants were participating in the preventive care class for the first time, while some FL participants had previously participated. This might have led to significantly lower occupational deprivation scores in the FL group relative to the PL group pre-intervention. Hence, the previous experience of participation in preventive care services was analysed by adjusting for a covariate in ANCOVA, with consideration given to reducing its impact.
In PL-type management, participants determined the duration of each programme. Additionally, some programmes designed by participants were added. As a result, strictly speaking, the programme contents were different between the two groups. This difference may impact the programmes’ effects. In PL management, participants’ autonomy is respected. This was a limitation because PL-type management would not be possible if the programme were completely controlled.
In this study, 47.3% of the originally recruited participants were ultimately included in the statistical analysis. As there were many absences and the sample size was small, it is important to examine the larger sample in detail. Other limitations of this study were that snowfall likely restricted access to the venue and that participants were often absent due to poor health. In addition, about 20% of the participants dropped out after the first few sessions, leaving room for improvement in the programme. Further exploration of the reasons for continuing or discontinuing the class will lead to programme improvements, including higher participation rates. Moreover, 92.9% of PL participants and 75.9% of FL participants were women. As most participants were female, our results may not be generalisable to male participants. Future research is needed to determine whether men have similar tendencies.
Conclusion
PL management significantly promoted improvements in participants’ occupational deprivation and subjective health compared with FL. In contrast, FL management significantly improved the participants’ motor function compared with PL. Furthermore, regardless of the programme management type, group activities reduced participants' expression of positive automatic thoughts. To achieve more effective preventive care services, it is important to not only offer programmes but also use an appropriate management type that matches the service’s purpose.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Hong Kong Occupational Therapy Association is currently covering the publication costs for all authors'.