
Abstract
Background
Psychological factors contribute to chronic pain and may lead to physical inactivity and poor functional outcomes.
Purpose
We conducted a non-randomized controlled study to evaluate the effectiveness of goal setting and achievement following occupational therapy (OT) intervention to improve pain, psychological factors, and physical activity among patients after high tibial osteotomy (HTO).
Method
We analyzed the data of 31 patients who underwent HTO, allocated into OT intervention and control groups. Goal achievement was encouraged through OT in the intervention groups; the control groups did not receive OT intervention. Outcome measures included the Canadian Occupational Performance Measure (COPM) score (before and after the OT intervention), walking pain, pain catastrophizing, anxiety, depression, pain self-efficacy, and physical activity level.
Results
OT significantly improved the COPM score, depression, and physical activity. At the final assessment, the depression score was lower while the step count and physical activity time were significantly higher in the intervention group than in the control group (p < 0.05).
Conclusion
Embedding goal setting and achievement as part of an OT intervention improved the outcomes after HTO.
Keywords
Introduction
High tibial osteotomy (HTO) is an accepted procedure for the treatment of medial knee osteoarthritis with varus malalignment (Korn, 1996). Nevertheless, an epidemiological survey regarding musculoskeletal chronic pain in Japan revealed an 11.1% rate of patient complaints with approximately 30% of these patients reporting chronic pain and morbidity at ≥5 years after surgery, requiring ongoing treatment (Nakamura et al., 2014). Similarly, van Leishout et al. (2019) reported a rate of persistent pain at four years after HTO of 26%. Although negative psychological factors such as anxiety, depression, and pain catastrophizing have been associated with chronic pain after total knee arthroplasty (TKA) (Sullivan et al., 2011), it is unclear if these same factors play a role in the development of chronic pain after HTO.
Previous research regarding psychological factors and quality of life (QOL) of patients after HTO revealed that patients who are highly depressed tend to have difficulty returning to work (Saier et al., 2017). Another study reported that 62% of patients reported some limitations in their activities related to ongoing issues with their knees after HTO, with self-efficacy identified as a contributing factor to their perceived limitations (Bonnin et al., 2013). These findings suggest that psychological factors such as anxiety and self-efficacy are likely to play roles in the development of chronic pain and activity limitation after HTO and therefore should be evaluated in this clinical population.
Investigators previously reported a relationship between the Canadian Occupational Performance Measure (COPM) score and pain catastrophizing after TKA (Hiraga et al., 2015). The COPM is based on an explicit model of OT – the Canadian Model of Occupational Performance and Engagement – in which occupational enablement and a client-centered approach are paramount (Law et al., 1990). Notably, improvement in ‘helplessness in a painful situation’ was recognized by occupational therapists (OTs) as contributing to improvements in goal setting and achievement on the COPM in a quasi-randomized controlled trial (Hiraga et al., 2016). Improvement in goal setting and achievement has been identified as an important contributing factor in improving helplessness in a painful situation in another study as well (Witjes et al., 2019). These findings suggest that goal setting and goal achievement can improve psychological factors and activity level, and could play a role in preventing the development of chronic pain. Nevertheless, because these previous studies focused specifically on patients after TKA, it is not known whether the benefits of goal setting and goal achievement would apply to patients after HTO.
Therefore, it is necessary to clarify the effects of goal setting and achievement on pain, psychological factors, and activity levels, specifically in patients after HTO. Accordingly, this study aimed to determine whether the use of goal setting and achievement as part of an OT intervention after HTO would reduce pain and improve psychological and physical performance in this patient population.
Materials and methods
Study design
This study was a non-randomized controlled trial, with patients allocated to the intervention group (OT practice) or control group; Randomization of the subjects was not possible as the study was conducted within the participating hospital.
Ethical considerations
All study patients provided written informed consent to participate in the study. The study design was approved by the appropriate ethics review board at Fukuoka Rehabilitation Hospital (Ref no.: R-013).
Power analysis
The power analysis programme G*Power 3 (Faul et al., 2007) was used to perform a preliminary power analysis and to estimate the required sample size. The power was set at 0.8 and the significance level (α) was set at 0.05 (Cohen, 1992). The effect size was set at 0.25, a moderate standard for a two-way analysis of variance. To identify a significant effect of the intervention, 24 patients (12 per group) were required for pre- and post-OT evaluations.
Description of the study group
The study group included patients who underwent HTO at our institution between October 2018 and August 2019. Over this period of observation, 35 patients were eligible, with those who underwent HTO between October 2018 and February 2019 assigned to the control group, and those treated between March 2019 and August 2019 assigned to the intervention group. All patients were screened to exclude those with a diagnosis of dementia and obvious mental illness (e.g., depression) that would interfere with completion of the questionnaire. We also excluded those who refused OT treatment, as well as those who developed postoperative complications (such as nerve injury and deep vein thrombosis), those with significant medical conditions that interfered with postoperative rehabilitation, those with histories of prior HTO (either to the same or opposite limb), and those for whom HTO was performed for causes other than knee joint degeneration (such as rheumatoid arthritis or bone necrosis). After screening, a total of 33 patients were enrolled in our study; two of the 35 eligible patients were diagnosed with dementia and therefore were excluded. These patients were allocated by convenience to either the intervention group (n = 15; two men; age, 67.3 ± 2.1 years) or the control group (n = 18; three men; age, 68.1 ± 1.9 years) as previously described.
Management
The surgery was performed under general anesthesia in all patients. All patients received non-steroidal anti-inflammatory drugs (dose, 60 mg, three tablets per day) for two weeks postoperatively. All patients followed the same rehabilitation protocols after surgery. All patients (intervention and control groups) began physical therapy on postoperative day 1, including knee range-of-motion exercises (flexion-extension) and stretching; approximately three weeks post-operation, walking using a walker was possible. Approximately five weeks post-operation, walking with a cane or alone was possible, and the patient was discharged from the hospital. All physical therapy interventions required 40 min per day.
OT intervention with goal setting and achievement
OT treatment was initiated in postoperative week 3 for improving goal achievement for goal setting (intervention group). For the intervention group, we used a previously reported method for goal setting and goal achievement (Hiraga et al., 2016). The COPM (Law et al., 1990) was used to identify five target goals and for prioritization of these goals. After the goals were prioritized, performance on each goal was evaluated on a 10-point scale, with anchors at ‘1’ (not possible) and ‘10,’ (very good). Satisfaction was also evaluated on a 10-point scale, with anchors at ‘1’ (not satisfied) and ‘10’ (very satisfied).
Each goal was progressed based on each patient’s capacity. As an example, for a patient who identified ‘I want to be able to go shopping’ as a goal, the intervention would progress from facilitating standing to walking outdoors and managing the environment for shopping. Through repeated practice, the patient is supported and encouraged to achieve this goal to be able to shop. A similar procedure was performed for every goal. OT intervention was delivered by six occupational therapists with > 3 years of experience in treating patients undergoing HTO. The OT intervention was performed only during hospitalization. All OT interventions required 20–40 min per day.
Assessment
The assessment was performed at the baseline (during the first three weeks after HTO) and post-intervention (five weeks post-operation; upon leaving the hospital). All outcome measures shown below had been validated for reliability and validity.
Pain
Pain during walking was evaluated using the 11-point numerical rating scale (NRS) (Jensen et al., 1994), with anchors at ‘0’ (no pain) and ‘10’ (worst imaginable pain).
Pain catastrophizing
The Pain Catastrophizing Scale-6 (PCS) (Nishigami et al., 2017) was used for the evaluation of pain catastrophizing. The PCS consists of six items, with the patient reporting the time spent in each itemized state on a five-point scale, with anchors at ‘0’ (not at all) and ‘4’ (all the time). A high score is indicative of strong pain catastrophizing.
Anxiety and depression
The Hospital Anxiety and Depression Scale (HADS) (Zigmond & Snaith, 1983) was used to evaluate anxiety and depression. The HADS consists of 14 questions, with the patient reporting the time spent in each itemized state on a four-point scale, with anchors at ‘0’ (not at all) and ‘3’ (most of the time). Both the total and subscale scores of the HADS were used for analysis.
Pain self-efficacy
The Pain Self-Efficacy Questionnaire-2 (PSEQ-2) (Nicholas et al., 2015) was used to evaluate self-efficacy for pain. The PSEQ-2 consists of two items scored on a seven-point scale, with anchors at ‘0’ (not at all confident) and ‘6’ (completely confident).
Physical activity levels
An activity meter (Active Style Pro; OMRON Corp., Kyoto, Japan) was used to evaluate physical activity. The activity meter was worn at the waist for 24 h. Steps and physical activity were measured and converted into a measure of metabolic equivalents (METs) per min. Ohkawara et al. (2011) reported on the high reliability of using the Active Style Pro to measure step count and physical activity level.
Statistical analysis
A t-test was used to evaluate significant differences in age and body mass index (BMI) between the OT intervention and control group. Between-group differences in demographics (sex, employment, smoking, and alcohol consumption) were evaluated using the chi-square test. A t-test was used to evaluate the change, from baseline, in the COPM satisfaction score and performance score in the OT intervention group. The effects of the intervention protocol on outcome measures was evaluated using a 2 × 2 (time (baseline and pre- to post-OT) × group (intervention and control groups)) analysis of variance. Post hoc Bonferroni tests were used for specific comparisons, and the two-sided significance was determined. Statistical analyses were performed using the JMP statistical package (version 14.0; SAS Institute Co., Ltd.).
Results
The flow chart depicting patient enrollment into the study is shown in Figure 1. In total, 35 eligible patients were screened, with two excluded based on our study criteria. The remaining 33 patients were enrolled into the study and non-randomly allocated to either the OT intervention group (n = 14) or control group (n = 17). One participant from each group withdrew from the trial, and these data were excluded from the analysis. Finally, our analysis was based on the 14 patients in the OT intervention group and 17 in the control group who completed the study.
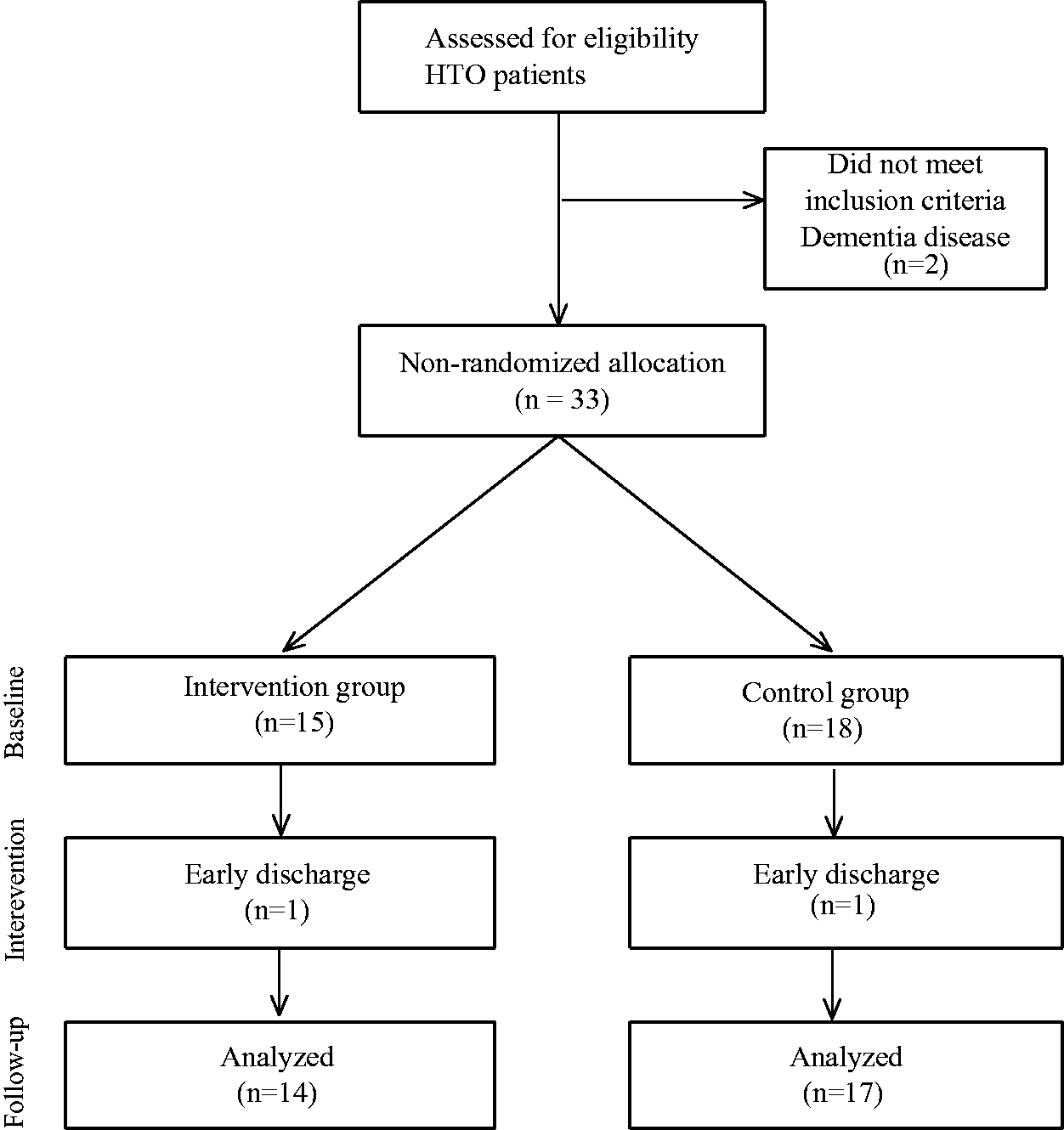
Patient recruitment and flow through the study.
Baseline characteristics
The baseline characteristics of the patients forming the study group are summarized in Table 1. There were no significant differences in terms of age, sex, BMI, employment, smoking, alcohol consumption, pain intensity, psychological status, or physical activity between the two groups.
Baseline characteristics of patients by group.
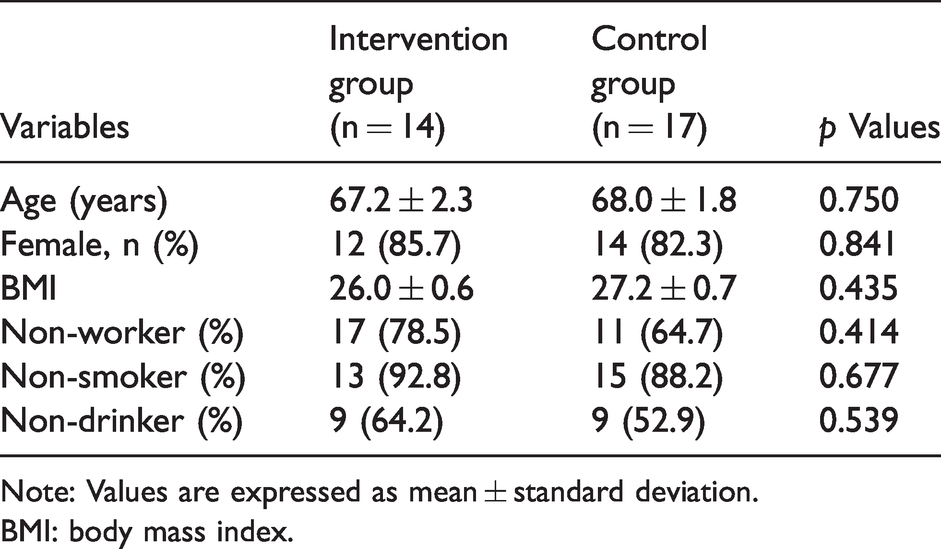
Note: Values are expressed as mean ± standard deviation.
BMI: body mass index.
Intervention group effects
The COPM goals set are reported in Table 2. Of these, 14.6% were related to personal care, 18.1% to walking, 14.6% to social life, 7.2% to work, and 21.9% to housework. With regard to leisure activities, none of the goals addressed playing (e.g. playing sport), with 1.8% being about static recreation, 16.4% active recreation, and 5.4% sociability. The COPM performance score in the OT intervention group improved from 2.6 ± 1.6 (at baseline) to 8.0 ± 1.2 (after OT; p < 0.01), with the satisfaction score improving from 2.0 ± 1.3 (at baseline) to 8.0 ± 1.3 (after OT; p < 0.01).
Goal classification on the COPM.
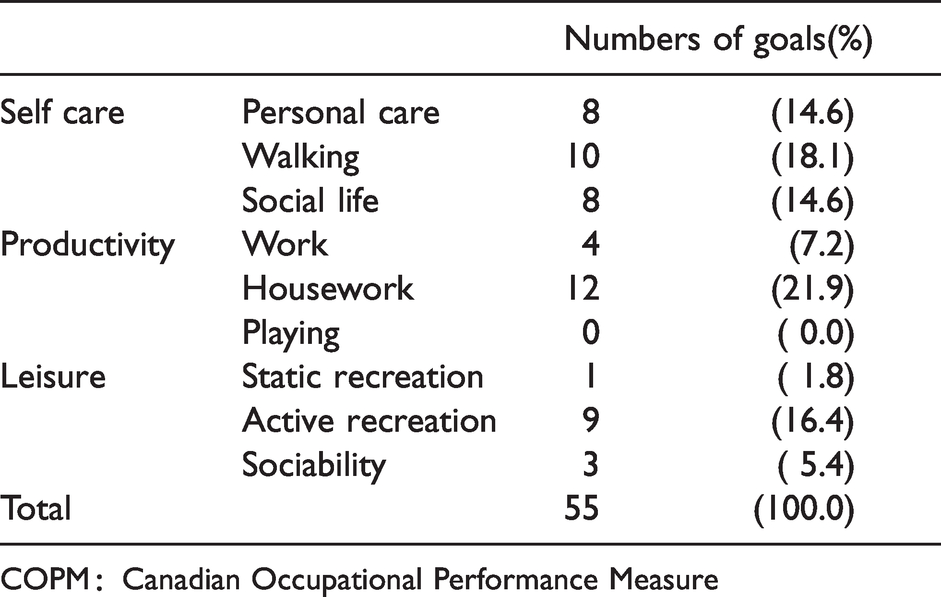
COPM:Canadian Occupational Performance Measure
Between-group comparisons
The effects of goal setting and practice on measured outcomes before and after intervention in the OT intervention group and at the same time points in the control group are reported in Table 3. The mean HADS depression score was significantly better after the OT intervention (p < 0.05) and was significantly higher after the OT intervention than that for the control group (4.4 ± 2.5 vs. 8.2 ± 2.9; p < 0.05). The mean daily step count and physical activity time were also significantly better after the OT intervention (p < 0.05), and better for the OT intervention than the control group: daily step count, 3708.4 ± 1552.5 vs. 1889.0 ± 633.0 (p < 0.01) and physical activity time, 998.5 ± 212.1 min vs. 764.8 ± 199.9 min (p < 0.05).
Pre-and post-OT outcomes, by group.
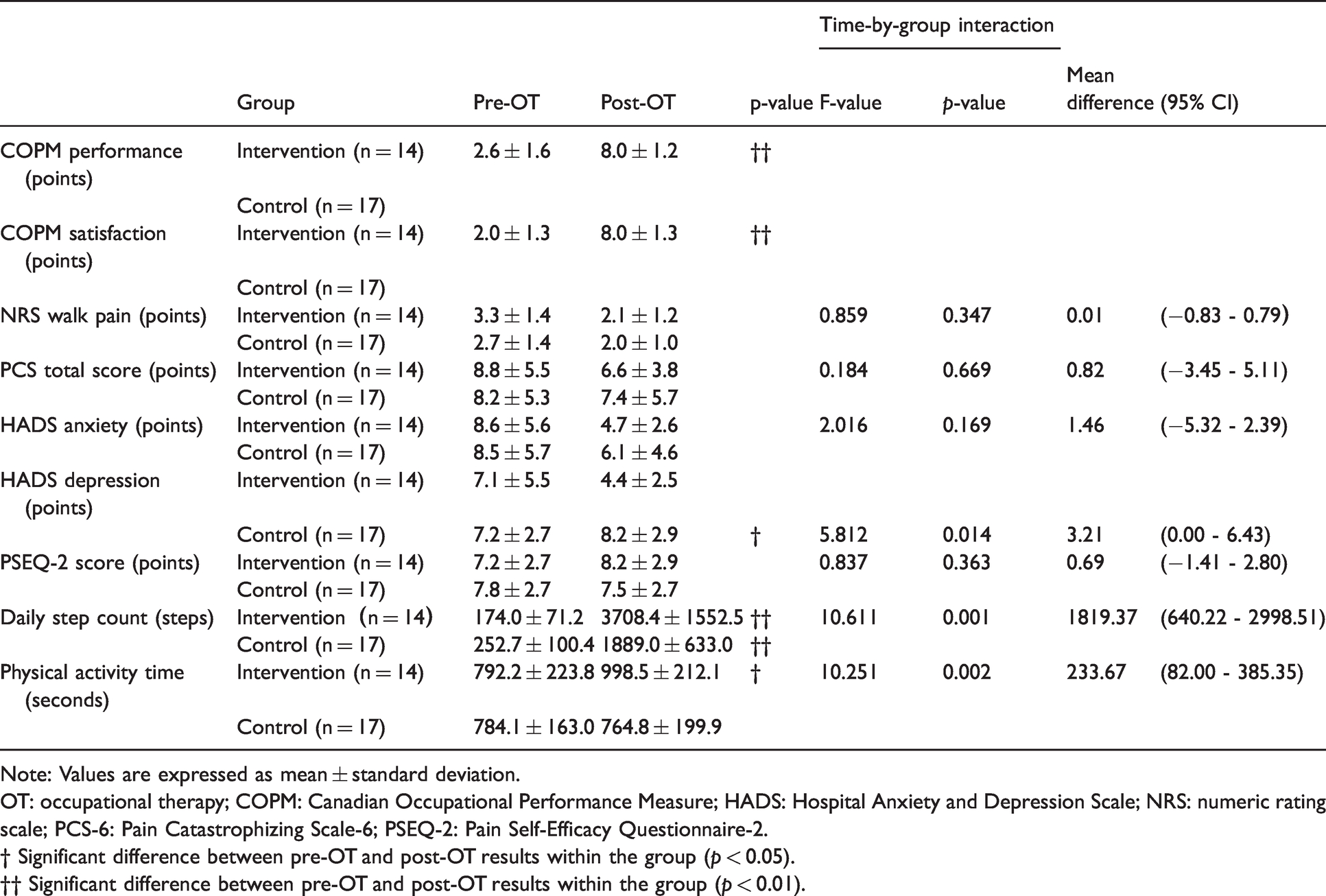
Note: Values are expressed as mean ± standard deviation.
OT: occupational therapy; COPM: Canadian Occupational Performance Measure; HADS: Hospital Anxiety and Depression Scale; NRS: numeric rating scale; PCS-6: Pain Catastrophizing Scale-6; PSEQ-2: Pain Self-Efficacy Questionnaire-2.
† Significant difference between pre-OT and post-OT results within the group (p < 0.05).
†† Significant difference between pre-OT and post-OT results within the group (p < 0.01).
Discussion
Our findings suggest a beneficial effect of using goal setting (based on the COPM) and achievement, provided within an OT intervention, to improve psychological factors and physical activity after HTO. The COPM goals set by patients addressed housework 21.9%, walking 18.1%, active recreation 16.4%, personal care 14.6%, social life 14.6%, work 7.2%, social 5.4%, and static recreation 1.8%, with none of the goals relating to play 0.0%. Our findings of the majority of goals being around housework, walking, active recreation, and personal care are largely consistent with the COPM-based goals identified by Edwards et al. (2007) among patients after a femoral neck fracture, with walking (24%), bathing (22%), and washing (20%) being the principal goals identified. The inclusion of active recreation and social life among the top goals in our study group likely reflects differences in the attributes of patients in the different studies, as well as factors unique to the Japanese culture.
Goal setting and achievement, as part of the OT intervention, significantly improved COPM performance and satisfaction scores as well as the HADS depression score, daily step count, and physical activity time. Moreover, patients in the OT intervention group reported significantly better HADS depression scores, daily step counts, and physical activity times than those in the control group. Based on these findings, we conclude that goal setting and practice, based on the COPM, is a beneficial component of an OT intervention for patients who have undergone HTO.
A previous study reported improvement in activity limitation and mental health with an OT-based intervention for musculoskeletal pain management using an intervention focused on activity training (Persson et al., 2014). It has also been shown that psychological factors such as depression are improved by an activity-based program (Deirdre et al., 2018). These results support the use of an activity-based OT intervention in patients with HTO, including goal setting and achievement, in reducing depression symptoms. The findings of our own study further confirmed an improvement in the HADS depression score, daily step count, and physical activity time with the used of goal setting and achievement in an OT intervention based on the COPM. Long-term effects of OT intervention on activity limitation after chronic pain remains unknown, with our study addressing the short-term effects of OT intervention. Moreover, apart from physical therapy, the effects of medication had not been considered in this study. In addition, demographic data such as the duration of illness was not taken into account; future research should therefore consider these factors.
Conclusion
Our results suggest that the use of goal setting and achievement in OT in patients after HTO provides significant improvements in the HADS depression score, daily step count, and physical activity time over the use of a general OT programme.
Footnotes
Acknowledgments
The authors thank all the researchers who conducted trials involved in the study.
Data availability
The clinical trial registration information of this research is available online. The documents can be viewed at UMIN (ID number UMIN000036712).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.