
Abstract
Background
Given the growing role of family caregivers in meeting the increasing demand for ageing-related care in Japan, the occupational adaptation of family caregivers needs to be evaluated.
Methods
This study developed the Occupational Adaptation Questionnaire for Family Caregivers (OAQC) and evaluated its reliability, validity, and effectiveness. To develop the OAQC item pool, the construct ‘Occupation of nursing care engaged in by family caregivers’ was evaluated. Using the Delphi method, 8 experts evaluated 64 items and confirmed that 41 items adequately represented the domain. The scale was then completed by 216 family caregivers of users of outpatient service establishments affiliated with hospitals in the Chubu region. The validity of the scale items was tested, and statistical analysis was performed. The construct validity and internal consistency of the OAQC were examined using exploratory factor analysis and the ω coefficient, respectively.
Results
The discrimination ability and difficulty level were calculated using the item response theory. The findings showed that the scale’s reliability and validity were satisfactory. Construct validity was acceptable for 16 items with 5 factors. The OAQC also had high internal consistency, reliability, and effectiveness. The item slope parameters and difficulty parameters revealed good item response, indicating that the scale could effectively measure family caregivers’ occupational adaptation.
Conclusion
The scale was compatible with the data obtained from family caregivers. Given its overall effectiveness, data obtained using the OAQC can contribute towards implementing personal care support programs for caregivers and enriching their lives by offering support from an occupational adaptation perspective.
Keywords
Introduction
Ageing is an international phenomenon. Further, since developing countries are undergoing rapid social and economic development, their demand for social services is increasing (Silva et al., 2019; World Health Organization, 2017). A meta-analysis conducted as part of an international study found that 10.7% of older people suffered from frailty (Collard et al., 2012). Physical weakness is a predictor of negative health outcomes, such as increases in the risk of death, hospitalization rates, and social withdrawal, as well as a decrease in the activities of daily living (Carneiro et al., 2017). With the increase in the number of frail older people worldwide, the provision of nursing care will become a serious global issue.
Japan is facing problems that are associated with a ‘super-ageing’ society. It is estimated that one in three people will become 65 or more years old by 2030 (Shigesato, 2012). Moreover, as a leading nation attemping to solve the problems associated with ageing, Japan has been responding to issues such as low fertility rates, an ageing population, and the growing old age burden for several decades (Parsons & Gilmour, 2018). Despite these efforts, Japan’s population continues to age. In 2025, the country will introduce ‘Community-based integrated care systems’, a policy that enables home care recipients to live at home (Ministry of Health, Labour and Welfare, 2013). In this context, it is necessary to focus on family caregivers’ caregiving ability. Japan is facing problems pertaining to the provision of adequate nursing care (Kimura et al., 2019). In order to improve the current situation, a social support system for family caregivers is necessary.
Occupational therapists (OTs) can support family caregivers since they focus on human occupations and have the ability to provide support for occupational adaptation (O’Brien & Kielhofner, 2017). It is important for caregivers to have optimal occupational adaptation. To provide support for family caregivers, it is necessary to have an evaluation tool that clarifies the problems that they face. Therefore, the Occupational Adaptation Questionnaire for Family Caregivers (OAQC) was developed.
The OAQC was developed according to the Consensus-Based Standards for the Selection of Health Status Measurement Instruments (COSMIN) checklist, a health-related patient-reported outcome (Mokkink et al., 2010). COSMIN is an international standard for scale development proposed by experts in epidemiology, psychology, clinical medicine, and statistics (Mokkink et al., 2016).
COSMIN captures scale properties in terms of validity, reliability, responsiveness, and interpretability. Therefore, this scale was developed in accordance with COSMIN.
From this construct, the study created a temporary questionnaire and verified its content validity (Nagai et al., 2020). Finally, the study verified the questionnaire’s reliability and validity using the item response theory (IRT) recommended by COSMIN.
Method
Ethics statement
This study was designed in accordance with the contents of the Declaration of Helsinki. Further, the research was conducted with the approval of the Research Ethics Committee of Heisei College of Health Sciences Review Board. In this study, along with the survey form, we enclosed a letter explaining the purpose and method and asking for informed consent. All participation was voluntary, and participants had the right to leave the study at any time without providing a reason. We regarded the return of the survey form as consent for participation. The survey form was returned anonymously in sealed submission envelopes.
Item Pool
To develop the OAQC item pool, an evaluation was performed based on the construct ‘occupation of nursing care engaged in by family caregivers’.
In order to develop such a scale, the first step is to examine the concept of composition. Although there are many evaluations of the burden of nursing care on family caregivers, no previous study has conceptualised the ‘occupation of nursing care engaged in by family caregivers’.
Therefore, the first author started by creating a concept of composition.
Unstructured interviews were conducted with 16 family caregivers who had provided at-home care for their family members for at least one month. Transcripts of the interviews were analysed using the Steps for Coding and Theorization (SCAT) method. Steps for Coding and Theorization is a method of analysis that segments word-based data, such as interview records, and devises and appends codes following the four steps described.
This analytical method describes the storyline and theory by drawing out its constitutive concepts. This method is also useful for analysing qualitative data from relatively small samples, such as a single case or a case-free description on a questionnaire (Otani, 2007). As a result, to form the constructs, 102 content codes were identified and categorized into the following three major categories: feelings of family caregivers, caregiving life, and caregiving and environment (Nagai et al., 2020). Based on the generated concepts, we created a draft scale item.
The scale comprised 64 items. Subsequently, the Delphi method was applied to verify the scale’s content validity. The Delphi method is a method in which experts judge a problem by its text. Experts are asked a number of questions individually and summarize their views until some agreement is reached. However, since the Delphi method does not have any guidelines and is performed in a variety of ways, this study was conducted by adopting Zamanzadeh's method, which clearly shows the procedures of the Delphi method (Zamanzadeh, 2015).
In this study, we selected experts who had all three of the following requirements: (1) experience in community health care, (2) a master's degree or higher in health and welfare, and (3) experience in scale development or qualitative research. The study was conducted with the help of eight selected experts who were asked to score each item on a three-point scale of ‘not necessary’, ‘useful but not essential’, and ‘not essential’. The content validity ratio varies from 1 to -1. A higher score indicates a higher level of agreement among the experts members about the need for that item.
The content validity ratio was also calculated to verify the content validity of the scale. The formula of content validity ratio is CVR = (Ne–N/2)/(N/2), in which Ne is the number of experts indicating ‘essential’ and N is the total number of experts. All items were repeated until a CVR of 75% or more was achieved. Finally, 41 items were confirmed to appropriately represent the domain. In this study, this scale was used for field tests.
Participants
Family caregivers who had been caring for a person in need of care at home for more than one month participated in this study. Family caregivers with significantly impaired cognitive function using medical or welfare services were removed from the sample. The recruiting method was as follows.
Requests to research cooperation facilities
We randomly selected hospitals providing care services in the Chubu region. The hospitals that agreed to the request for participation in this study were designated as research cooperation facilities.
Selection of research participants
We requested the research cooperation facilities to distribute our questionnaire among the family caregivers of all users of the outpatient service establishments (day care service, day service, and rehabilitation) affiliated with each facility. The questionnaire was distributed in an envelope, along with a set of other documents, kept in the contact book file used by the facility’s office. Family caregivers returned the completed questionnaires by post. Further, the aforementioned set of documents included a research cooperation request document, basic information (to collect age, gender, years of care, and level of care required), the OAQC, and a reply envelope.
Descriptive statistics
We summarised the types of participants, including gender, age, years of caregiving, and the type of illness of those requiring care.
Using the collected data, the average and standard deviation (SD), ceiling effects (CE), and floor effects (FE) were calculated for each questionnaire item. Items outside the required range (1–7) were deleted. HAD Ver. 16.0 (Shimizu, 2016) was used for statistical analysis.
Item analysis
The items’ validity were examined using exploratory categorical factor analysis. Accordingly, the polyserial correlation coefficient (PCC) estimates the relationship between the total score of the complete scale and each item. Further, the correlation coefficient was set to 0.4 or more, although 0.2 is often used as the reference value (Murakami, 2006). In the scale used by the current study, 0.4 was set as the standard to ensure that the number of items was practical.
Evaluation of construct validity
The OAQC factor structure was determined using exploratory factor analysis (EFA) and the Maximum Likelihood Estimation method of Mplus Ver. 8.4 (Muthén & Muthén, 2012). The items that did not load on a factor (factor loading < 0.4) were deleted from the scale; subsequently, analysis was on the reduced item set. Further, the percentage of variance among the items accounted for by a factor was estimated using eigenvalues.
We used three indexes to assess model data fit. The first index was the root mean square error of approximation (RMSEA) (MacCallum et al., 1996), whose critical values from 0.08 to 0.10 imply a mediocre fit and values below 0.08 indicate a good fit. Finally, the second and third indexes were the comparative fit index (CFI) and Tucker–Lewis index (TLI), both with critical values above 0.95 (Kline, 2011).
Evaluation of internal consistency reliability
To evaluate internal consistency, we evaluated the ω coefficient, and a value of 0.7 or more was used as the reference value (Okada, 2011).
Item response
The IRT was applied in the analysis using the maximum likelihood method provided by Exametrika (Bock & Aitkin, 1981; Kyougoku et al., 2015; Thomas et al., 2013). The IRT was applied to calculate the discrimination ability and difficulty. Moreover, the IRT estimated the OAQC test response function (TRF) and test information function (TIF). According to the IRT, an item’s performance was judged according to its discriminating ability and difficulty. Whereas the discriminating ability ranged from 0.2 to 2.0, the difficulty was within an absolute value of 4.0.
Results
Sample characteristics
In this study, 216 family caregivers, including 51 men, 159 women, and 6 individuals who did not specify their gender, with an average age of 65.6 ± 12.6 years, responded to the survey. The average length of nursing was 5.54 ± 4.94 years. A person suffering from a stroke was the most common illness among those requiring care; that was followed by old age weakness and dementia, which was present in 80% of the total number of respondents (Table 1).
Participant characteristics (n = 216).
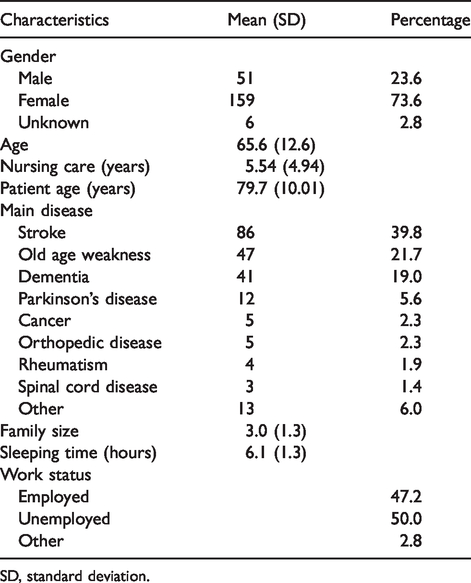
SD, standard deviation.
Item analysis
For five questionnaire items, the CE and FE were outside the specified range. Further, the PCC was less than 0.4 in 19 items. Twenty-four of the 41 items were deleted, and 17 items were retained (Table 2). The points that were subject to deletion are shaded.
Results of analysing the 41 items of OAQC.
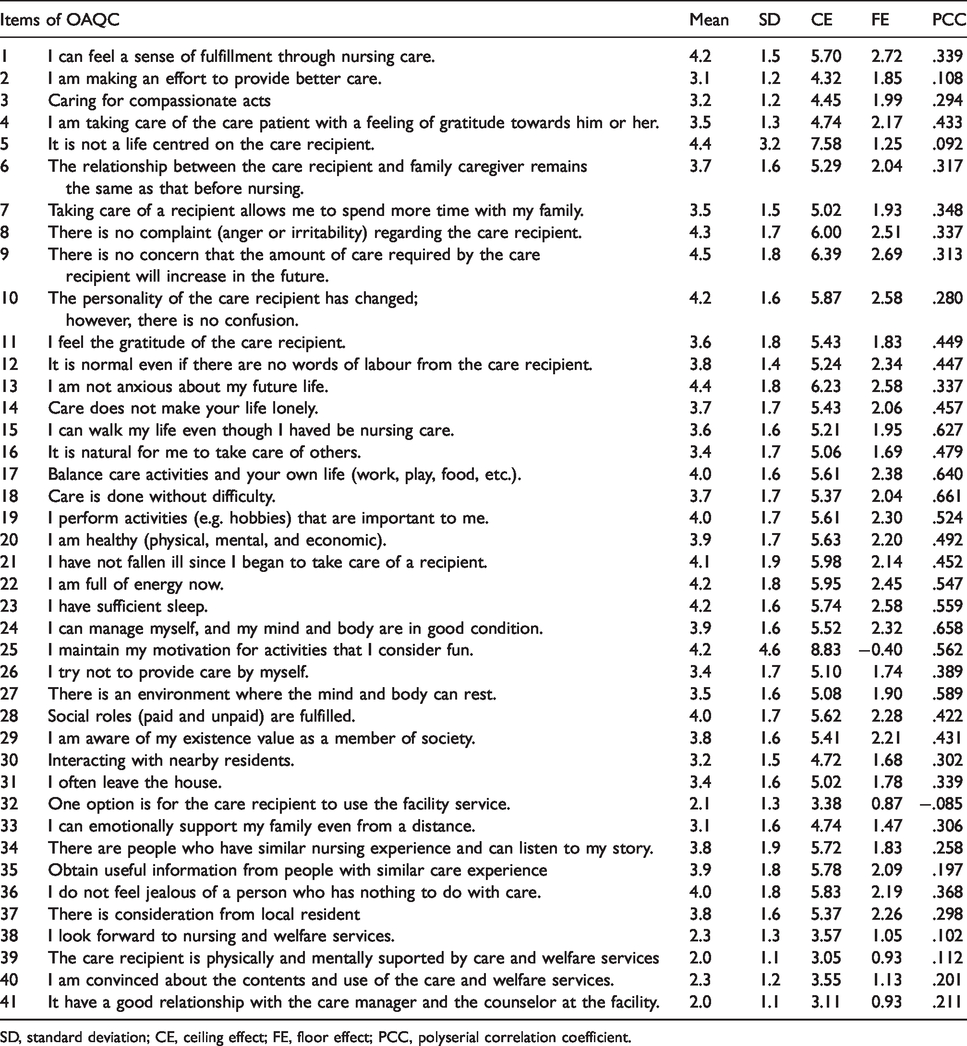
SD, standard deviation; CE, ceiling effect; FE, floor effect; PCC, polyserial correlation coefficient.
Construct validity
One item with a factor loading < 0.4 was deleted. Table 3 depicts the EFA results for 16 items. It is noted that five factors were generated from the EFA procedure: feeling for compassion (two items), balance of life (seven items), caring awareness (three items), my health (two items), and social existence value (two items).
Construct validity of OAQC.
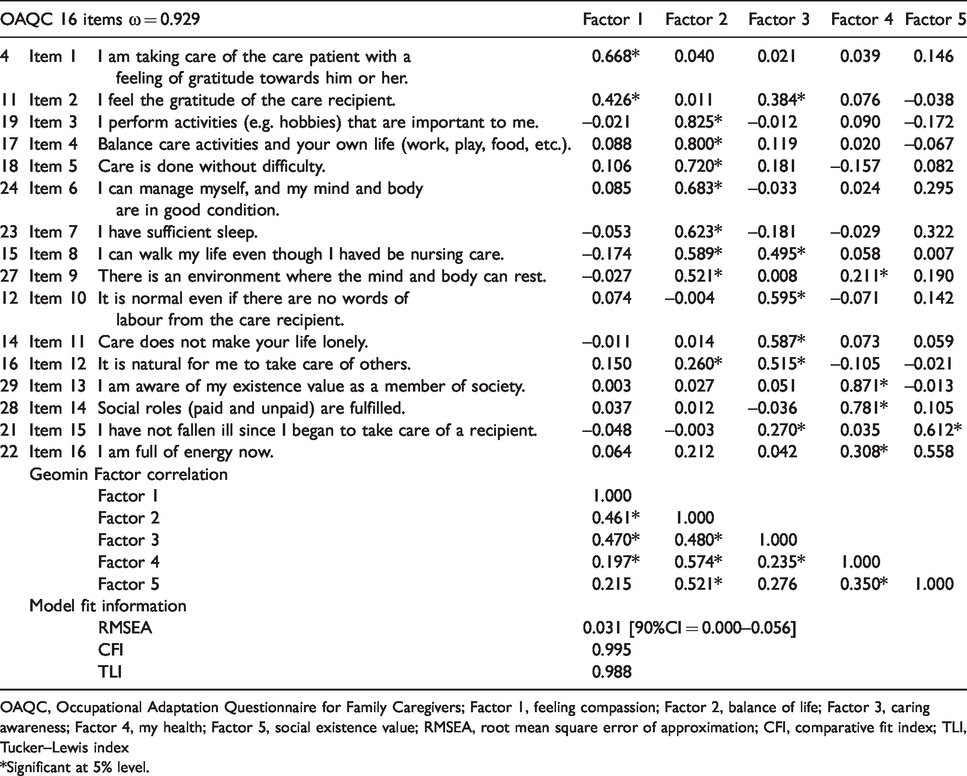
OAQC, Occupational Adaptation Questionnaire for Family Caregivers; Factor 1, feeling compassion; Factor 2, balance of life; Factor 3, caring awareness; Factor 4, my health; Factor 5, social existence value; RMSEA, root mean square error of approximation; CFI, comparative fit index; TLI, Tucker–Lewis index
*Significant at 5% level.
Three indexes were used to evaluate the scale's fit. The CFI was 0.995 and TLI 0.988, and all values exceeded the critical value of 0.95. Further, the RMSEA value was 0.031. Critical values with RMSEA < 0.08 indicate a good fit (Table 3). The data are shaded for each factor.
Internal consistency and reliability
The ω coefficient was 0.929, which confirmed the scale’s internal consistency and reliability (Table 3).
Item response
Table 4 depicts the results of item slope parameters (α) and item difficulty parameters (β). Overall, 16 items on the OAQC demonstrated satisfactory item response, with item slopes ranging from 1.049 to 1.696.
Item response of OAQC.
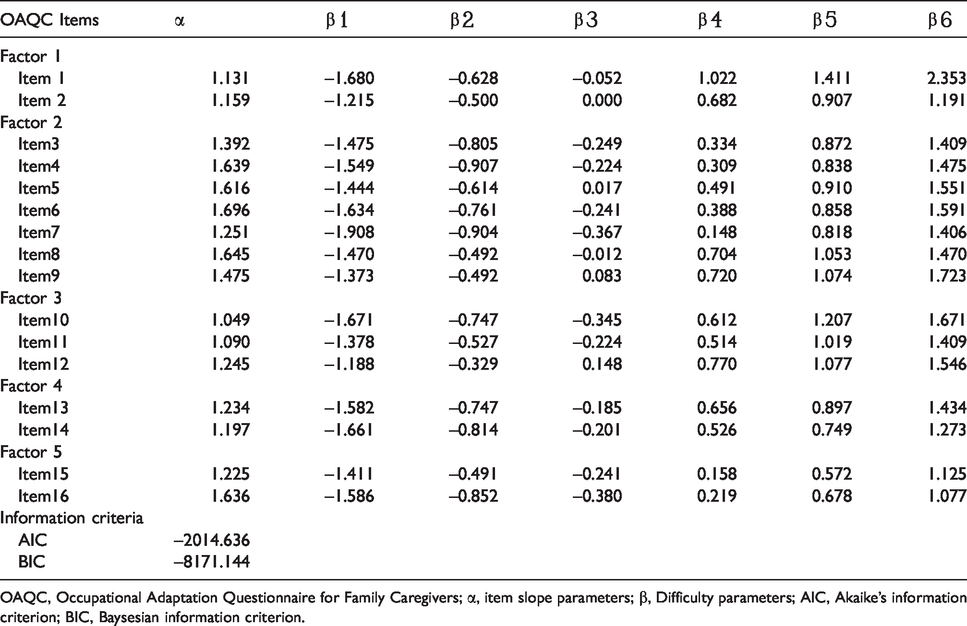
OAQC, Occupational Adaptation Questionnaire for Family Caregivers; α, item slope parameters; β, Difficulty parameters; AIC, Akaike's information criterion; BIC, Baysesian information criterion.
Further, Figures 1 and 2 present the OAQC’s TRF and TIF measures.
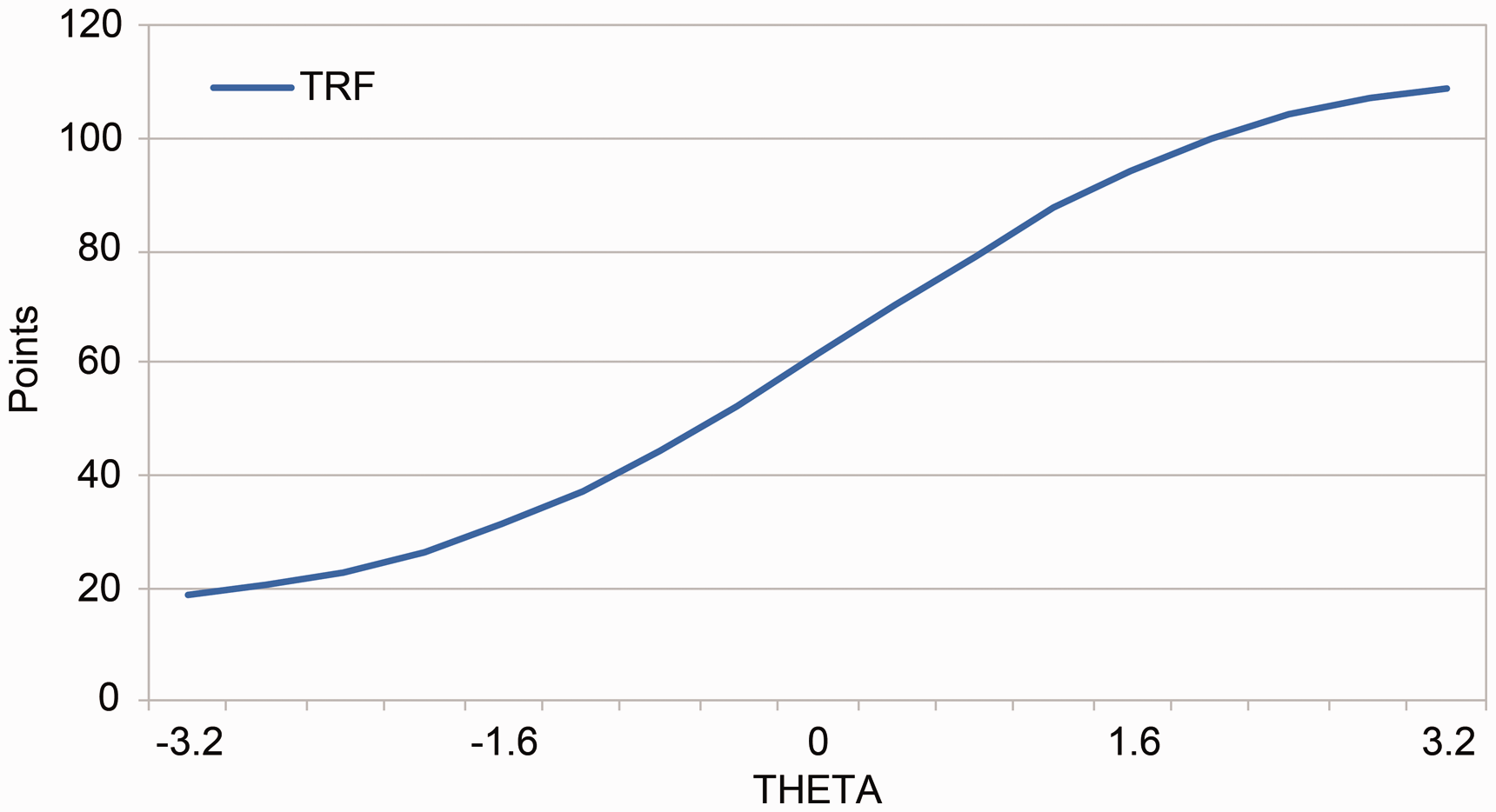
Test response function (TRF) of the Occupational Adaptation Questionnaire for Family Caregivers.
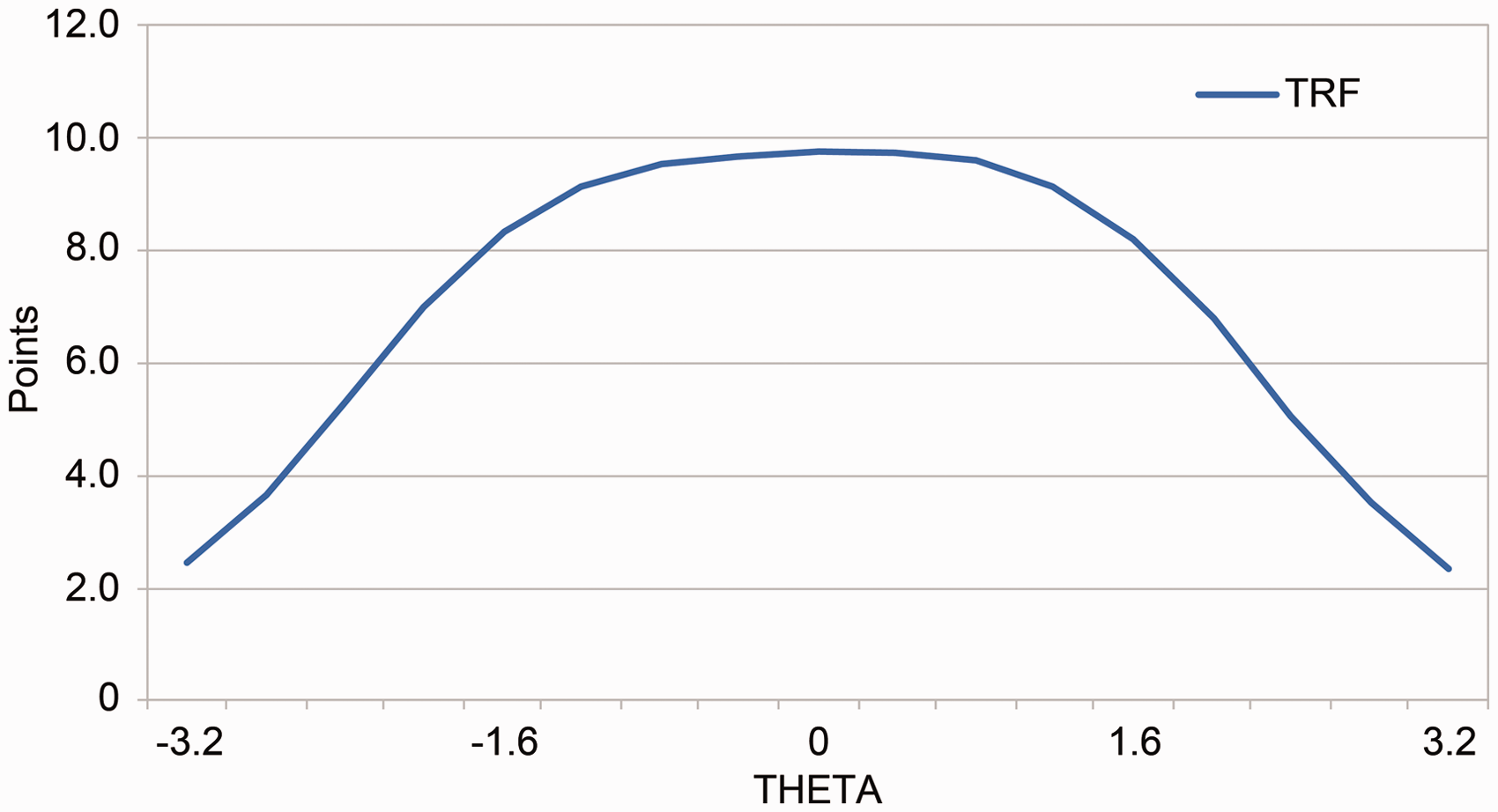
Variation in the test information function (TIF).
Overall, the OAQC measured an approximately equally wide range of occupational adaptation values with high precision.
Discussion
This study is novel in its development of a tool to assess the occupational adaptation of family caregivers from the professional perspective of occupational therapy. The scale has been found to be reliable and valid and can be used in clinical practice.
Psychometric properties of the OAQC
Following OAQC development, the questionnaire was evaluated from the professional viewpoint of OTs to provide caregiver support. Overall, the questionnaire’s reliability and validity were satisfactory. Several results provide evidence for the effectiveness and reliability of the OAQC (Tables 2 to 4). Further, construct validity, which was assessed using EFA, was acceptable for 16 items with 5 factors (Table 3). Regarding model fit information, RMSEA and CFI/TLI showed very good values. In this manner, we proved that it is compatible with the data provided by family caregivers. In addition, the value of the ω coefficient proved the questionnaire’s internal consistency, and the OAQC was recognized as having high reliability.
The items’ characteristics were clarified using the IRT. The OAQC score had high item slope parameters, 1.049–1.696. Moreover, difficulty parameter scores varied widely, from −1.908 to 2.353. These data strongly supported good item response of item slope parameters and difficulty parameters (Table 4). Hence, we estimated that the questionnaire can be used to measure caregivers’ occupational adaptation appropriately.
Practical implications of the study
Caregivers require help to ensure that their life is not dominated by caregiving. It is a comprehensive view of the life of one person, rather than merely the medical aspects of caring for the recipients who require care. It is very important to support caregivers from the viewpoint of occupational adaptation, as well. The OAQC plays a significant role in supporting caregivers’ occupational adaptation. Support must be provided to caregivers to overcome the problems identified by the OAQC. Aneshensel Pearlin et al. (1995) clarified the importance of nursing at one’s own pace through the use of social services. Based on these points, it would be preferable to provide total support for the health of family caregivers. To better understand the situation, we used the OAQC to extract the problems of family caregivers. This assists the occupational therapist with specific support. When such support is possible, we will be closer to a society where people who need care and their family caregivers can live at home in good health for a long time.
Limitations of the study
This study has some limitations. First, we did not examine the questionnaire’s retest reliability or criterion validity. Further, the study did not set any cut-off values for the OAQC. Hence, further research focusing on these limitations must be conducted in the future.
Conclusions
The OAQC is useful to evaluate the occupational adaptation of family caregivers. The study ensured construct validity and internal consistency, and item responses revealed satisfactory adaptation.
Footnotes
Ethics statement
The research was conducted with the approval of the Heisei Medical College Ethics Review Board (approval number H30-12).
Acknowledgments
The authors thank all family caregivers for cooperating with the questionnaire in this study. We also thank the hospitals and facilities that provided the subjects.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.