
Abstract
Objective/background
The rapidly increasing incidence of patients with dementia in Japan is creating an urgent demand for evidence-based occupational therapy (EBOT), which has been reported to improve clinical efficacy. This study aimed to examine the current practice of EBOT for patients with dementia in Japan and clarify factors influencing its application.
Methods
We conducted an anonymous, self-administered questionnaire survey by mail. The participants were 432 occupational therapists treating patients with dementia at 432 designated medical institutions nationwide. Descriptive statistics were calculated, and multiple regression analysis was performed to clarify the factors influencing the present application of EBOT.
Results
The response rate was 31.3%. Among the participants, 46.3% responded ‘somewhat frequently’ or more (5, 6, and 7 on a 7-grade scale) to a question on the frequency of practice of EBOT. Using multiple regression analysis with the stepwise method, we selected the model with the highest degree of fit. This model extracted three factors, namely, ability to understand scientific papers, sufficiency of means of getting information, and availability of advice, which had standardized partial regression coefficients (β) of 0.419, 0.214, and 0.158, respectively.
Conclusions
The three factors extracted using the multiple regression analysis indicate that in order to encourage EBOT for patients with dementia, occupational therapists need to acquire reading comprehension skills, so that they can assess the quality of scientific papers. Furthermore, it is important to create environments where they have access to publications and can discuss research with superiors and colleagues.
Introduction
In 2012, approximately 4.62 million people in Japan had dementia, and this figure is projected to increase approximately 1.5-fold to around 7 million by 2025 (Ninomiya, 2015). Therefore, in 2015, the Japanese Ministry of Health, Labour and Welfare and other related government agencies formulated a comprehensive strategy for promoting policies on dementia—the new orange plan. The objective of this plan is to ‘realize a society that respects the desires of people with dementia and allows them to continue to live in the communities they are accustomed to as long as possible’ (Ministry of Health, Labour and Welfare, 2015, p. 1). The plan has seven pillars, which include research on dementia prevention, treatment, and rehabilitation, as well as dissemination of the results (Ministry of Health, Labour and Welfare, 2015).
Recently, evidence-based practice (EBP) has been required of many medical professionals, including occupational therapists, to increase their clinical benefits (Thomas et al., 2017). Bennett and Bennett (2000, p.172) defined evidence-based occupational therapy (EBOT) as ‘a process that synthesizes clinical expertise, with the best evidence available from systematic research, and the values and preferences of patients. EBOT is becoming an integrated guiding framework for the practice of occupational therapy (Law et al., 2004; Law & Baum, 1998). As with EBP, EBOT consists of the following five steps (Buchanan et al., 2015; Sackett, 1997): (1) Convert information needs into answerable questions, (2) Find the best evidence to answer the question, (3) Critically appraise the evidence, (4) Apply the evidence in practice, and (5) Evaluate practice. For occupational therapists, practicing EBOT is essential for improving the clinical efficacy (Salls et al., 2009), and is becoming even more important with the anticipated rapid increase in dementia populations (Canevelli et al., 2016; Illiffe, 2015; Torke, 2014). Under these circumstances, the Japanese Association of Occupational Therapists (JAOT) recently published the ‘Japanese guidelines for occupational therapy: dementia’ (Takehara, 2018). Despite the existence of such guidelines, it is unclear the extent to which EBOT is actually being practiced in clinical settings for patients with dementia. Research on the factors affecting EBOT practice for patients with dementia has been conducted (Van’t Leven et al., 2012). However, the study did not examine how these factors relate to the practice of EBOT.
To promote EBOT for patients with dementia, the current situation of EBOT practice and the factors affecting its application need to be investigated. Therefore, the present study aimed to examine the current practice of EBOT for patients with dementia in Japan and to investigate the factors affecting its present application. Therefore, we conducted a survey among occupational therapists treating patients with dementia using anonymous self-administered questionnaires, posted by mail. Understanding these factors will make it possible to propose policies that will help promote EBOT, which in turn would enable the more effective delivery of occupational therapy services for patients with dementia.
Methods
We conducted a survey using an anonymous self-administered questionnaire posted by mail. To obtain a large sample of therapists with relatively high involvement in the care of patients with dementia, we recruited occupational therapists working for institutions designated as dementia care centres. When the survey was conducted in October 2018, 432 institutions were designated as dementia care centres nationwide. We contacted 432 participants, with one occupational therapist from each institution. The heads of the occupational therapy departments at each institution were asked to select the occupational therapist who would be the participant. The inclusion criteria were being a full-time occupational therapist currently treating patients with dementia and being within the following specified age ranges: 21 to 30 years, 31 to 40 years, and 41 years and older. When creating the allotments, we referred to the nationwide age composition of occupational therapists from the 2015 occupational therapy white paper (JAOT, 2017) and assigned 181 participants to the age group 21–30 years (42%), 169 participants to the age group 31–40 years (39%), and 82 participants to the age group 41 years and over (19%). We explained to the department heads that if there was no one available in the relevant age group, there was no need to respond; however, the director of the occupational therapy department could respond if he/she met the selection criteria. The survey questionnaires were collected from October 30 to November 29, 2018.
The questionnaire used in this study consisted of five question items: (1) basic attributes, (2) programmes with practical experience (binary choice method), (3) frequency of practice of each EBOT step (five grades), (4) frequency of practice of regular EBOT (seven grades), and (5) factors affecting the frequency of EBOT practice (five grades). In addition, before the question item (3) (frequency of practice in each EBOT step), we provided detailed definitions of EBOT and its five steps. These explanations were intended to give participants a thorough understanding of each EBOT step, so that the assessments could be objective. If the question item (3) could be objectively assessed, this would help ensure objectivity for the question item (4).
Basic attributes
The participants were asked about seven attributes: gender, age, years of clinical experience as an occupational therapist, qualifications related to dementia support apart from the occupational therapist qualification, academic degree, number of conferences and other such meetings attended in the last year (conferences attended), and type of dementia care centre designated (centre type).
Programmes with practical experience
This item was created by referring to the Japanese guidelines for occupational therapy: dementia (Takehara, 2018). These guidelines include recommendation content and grades for each clinical question, along with levels of evidence for occupational therapy interventions. Removing duplicate treatment techniques and integrating together multiple approaches left 20 programmes. The participants answered ‘yes’ or ‘no’ as to whether they had practiced a programme in the past year, regardless of the time spent or number of times practiced. The 20 programmes were: reminiscence therapy, leisure activities, music, recreation, cognitive stimulation therapy, cognitive rehabilitation, errorless learning, aerobic exercise, Snoezelen, environmental design changes, gardening, drawing/painting, urinary approaches, sleep approaches, Montessori-based activities, olfactory and other sensory stimuli, physical function training involving multiple tasks, family caregiver approaches, programmes embedding the elements of model of human occupation explicitly, and brain activation rehabilitation. Simple explanations and examples of each programme were also given to unify the understanding of the participants.
Frequency of practice of each EBOT step
This item was created by referencing reports that describe EBOT (Bennett & Bennett, 2000; Johnson, 2008; Rappolt, 2003). There were five questions, one for each of the five EBOT steps. For each EBOT step, the participants were asked how frequently they practiced it in the past year based on a 5-grade scale from 1 indicating Never; 2, Rarely; 3, Sometimes; 4, Often; and 5 indicating Very Often.
Frequency of practice of regular EBOT
To confirm the frequency of practice of regular EBOT, a question was asked to create a representative value of how frequently the participants practiced all the steps in their regular work. The question asked was, ‘Based on a comprehensive assessment of your answers to question item (3) on the frequency of practice in each EBOT step, how often did you practice EBOT in your regular work in the past year’? The responses were given on a 7-grade scale from 1 indicating Never; 2, Very Infrequently; 3, Infrequently; 4, Sometimes; 5, Somewhat Frequently; 6, Frequently; and 7 Very Frequently.
Factors affecting the frequency of EBOT practice
These items were selected based on a study by Dysart and Tomlin (2002) that investigated factors affecting EBOT practice in the United States and a systematic review of barriers to evidence-based medicine by Sadeghi-Bazargani et al. (2014). We selected 11 questions that asked about the ability to understand scientific papers, experience learning about EBOT, sufficiency of scientific papers, sufficiency of means of obtaining information, financial burden of participating in conferences, availability of supplies, ease of making changes or introducing things, availability of advice, busyness of work, busyness of private life, and willingness to practice EBOT. Participants were asked to rate each of these 11 questions on a 5-grade scale from 1 indicating Strongly Disagree; 2, Disagree; 3, Undecided; 4, Agree; and 5 indicating Strongly Agree.
After creating the questionnaire, as a preliminary survey, we asked four occupational therapists working at medical institutions that were not dementia care centres, but who treated patients with dementia, to respond to the questionnaire and provide advice on the clarity, suitability, and validity of the questions. The questionnaire was revised based on this advice to create the final version.
The occupational therapy department heads and participants at the participating institutions received a full explanation of the study in writing and were told that returning the questionnaire would be taken as consent to participate in the study. The Ethics Committee of the Faculty of Health Sciences at Hokkaido University approved the study protocol (Approval number 18–56).
Statistical analysis
First, descriptive statistics were calculated for all data. Next, to investigate the factors affecting the present application of EBOT for patients with dementia, multiple regression analysis was performed with the question item (4) as the dependent variable and the question item (5) (factors affecting the frequency of EBOT practice) as the independent variable. A stepwise method and the Akaike’s Information Criterion (AIC) were adopted to extract optimal models. In addition, Spearman’s rank correlation coefficients were calculated between the question item (4) and various other questions (e.g., age, clinical experience, number of qualifications, conferences attended, number of programmes experienced) and the question item (2) (programmes with practical experience). Further, although the programmes experienced in question item (2) included those with a low recommended grade (C2: no scientific basis to recommend performing it), they were included in the analysis, even though the evidence level was low because EBOT was defined as the best evidence from research, programmes that have been shown to be effective in intervention studies. In addition, we examined how responses to the question item (4) varied based on differences in the participant's gender, academic degree, and centre type. As the question item (4) did not show a normal distribution, the Mann–Whitney U test was used to compare genders. The Kruskal–Wallis test was used for academic degree and centre type. All statistical analyses were performed using SPSS Statistics 22.0 (IBM SPSS Inc., Chicago, IL, USA), and the significance level was set at p = 0.05.
Results
In total, 135 occupational therapists responded to the survey, yielding a response rate of 31.3%. None of the questionnaires that were received had the names or affiliations of the occupational therapists written on them. As ‘financial burden of participating in conferences’, ‘busyness at work’, and ‘busyness in private life’ in question item (5) were reverse-scored items, the responses to these items were reversed before performing the analysis.
The participants’ basic attributes are shown in Table 1. Table 2 shows the percentage of participants who answered ‘yes’ to the programmes in question item (2). Table 3 shows the total for the responses to the question items (3) and (4). Responses of ‘somewhat frequently’ or higher (5, 6, and 7) to the question item (4) were used to represent the frequency of practice of regular EBOT, with 46.3% of responses falling in this range. Table 4 shows the total responses to question item (5).
Basic respondent characteristics (n = 135).
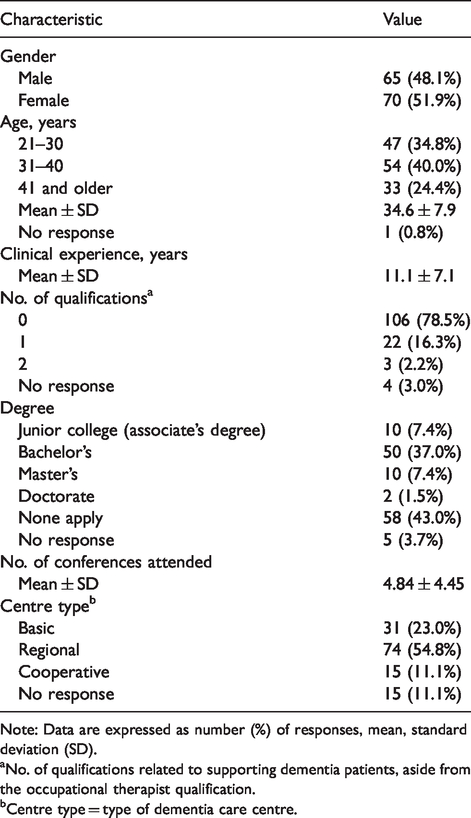
Note: Data are expressed as number (%) of responses, mean, standard deviation (SD).
aNo. of qualifications related to supporting dementia patients, aside from the occupational therapist qualification.
bCentre type = type of dementia care centre.
Proportions with practical experience with each programme (n = 135).
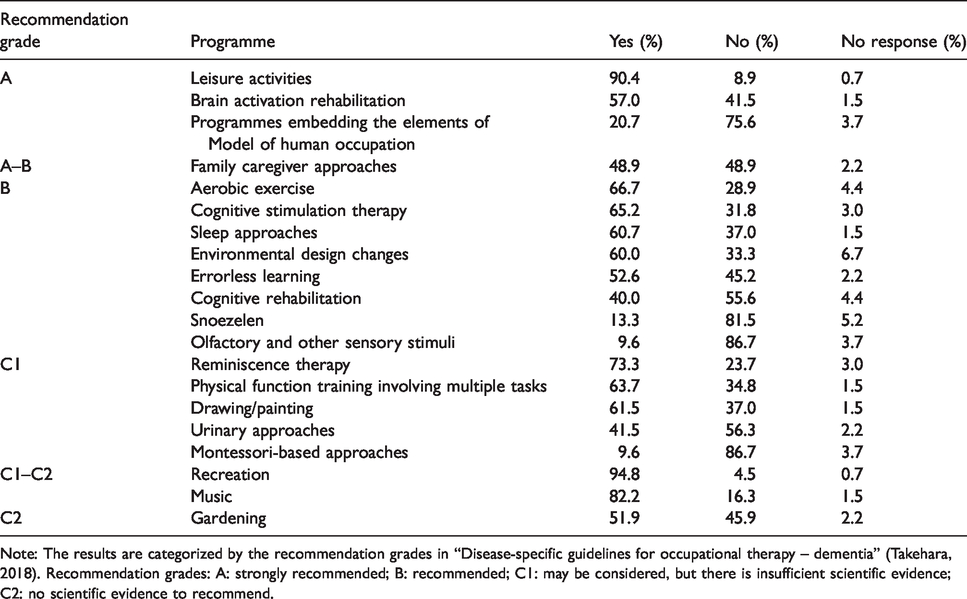
Note: The results are categorized by the recommendation grades in “Disease-specific guidelines for occupational therapy – dementia” (Takehara, 2018). Recommendation grades: A: strongly recommended; B: recommended; C1: may be considered, but there is insufficient scientific evidence; C2: no scientific evidence to recommend.
Frequency of practice of each EBOT step and of regular EBOT (n = 135).
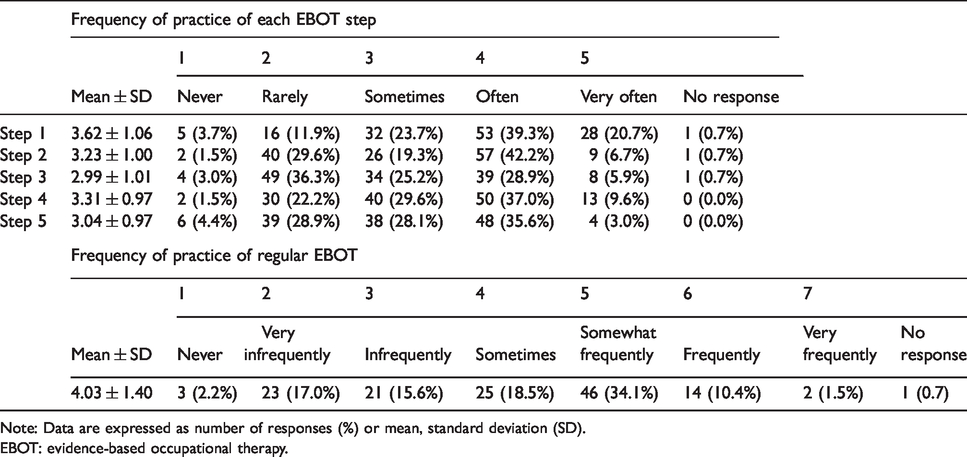
Note: Data are expressed as number of responses (%) or mean, standard deviation (SD).
EBOT: evidence-based occupational therapy.
The factors affecting the frequency of EBOT practice (n = 135).
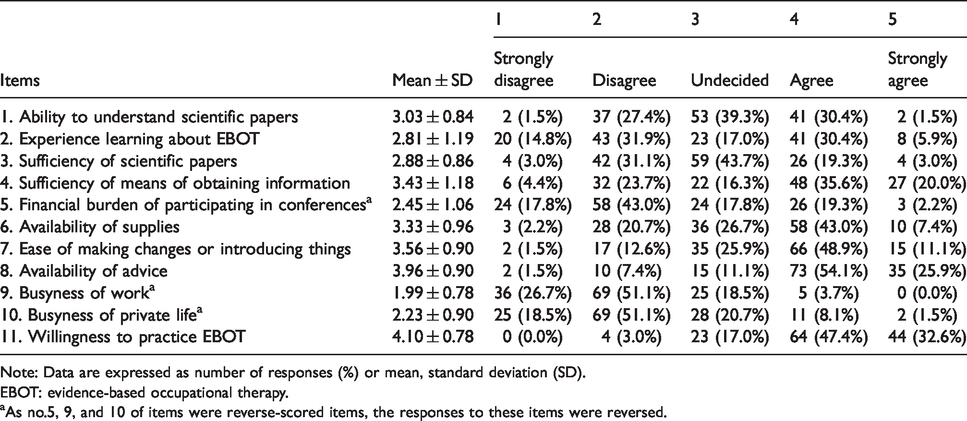
Note: Data are expressed as number of responses (%) or mean, standard deviation (SD).
EBOT: evidence-based occupational therapy.
aAs no.5, 9, and 10 of items were reverse-scored items, the responses to these items were reversed.
Table 5 shows the results of multiple regression analysis for the factors affecting the practice of EBOT for patients with dementia. Three models were extracted using the stepwise method. We compared AIC for the three models and adopted the model with the lowest AIC. This model extracted three factors: ability to understand scientific papers, sufficiency of means of obtaining information, and availability of advice. The standardised partial regression coefficient (β) was 0.419 for the ability to understand scientific papers, 0.214 for sufficiency of means of obtaining information, and 0.158 for the availability of advice. In this model, the collinearity statistic variance inflation factor was around 1.1, and there were no independent variables with multicollinearity. As a residual analysis, we calculated the Durbin–Watson ratio (1.893), which confirmed there was no autocorrelation in the error term. Further, the Shapiro–Wilk test showed that the standardised residual was normal.
Factors affecting the present application of EBOT for patients with dementia (n = 134).
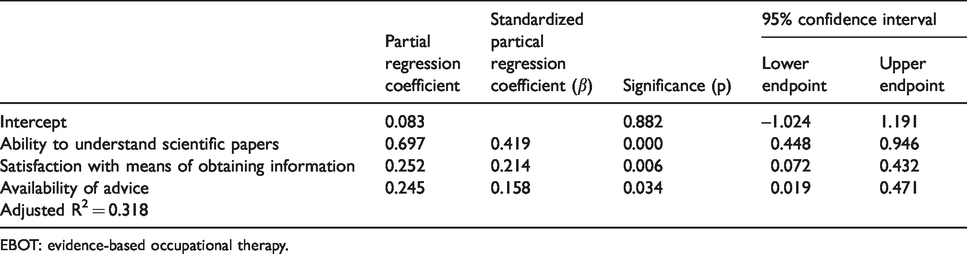
EBOT: evidence-based occupational therapy.
Examining Spearman’s rank correlation coefficients between the question item (4) and other questions showed a weak positive correlation with the number of programmes experienced in question item (2) (r = 0.366, p < 0.01) (Table 6).
Correlations between frequency of practice of regular EBOT and other questions.
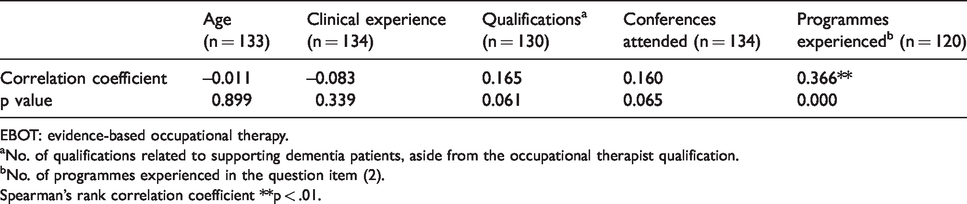
EBOT: evidence-based occupational therapy.
aNo. of qualifications related to supporting dementia patients, aside from the occupational therapist qualification.
bNo. of programmes experienced in the question item (2).
Spearman's rank correlation coefficient **p < .01.
There were no significant differences in gender (p = 0.262) and the results of the question item (4) (p > 0.05). Similarly, there were no significant differences observed between the results of the question item (4), academic degree, or centre type (p = 0.706, p = 0.422, and p > 0.05, respectively).
Discussion
This study aimed to examine the current practice of EBOT for patients with dementia in Japan and to investigate the factors affecting the present application of EBOT. Multiple regression analysis was conducted to investigate the latter's purpose. The model extracted three factors with β values, meaning these three factors positively affected the results of the question item (4) (frequency of practice of regular EBOT), with higher β values representing greater impacts. However, the β values and contribution ratios (R2) of these three factors are not sufficiently high, indicating that they have limited impact. Further, the existence of other factors that were not detected in the present study cannot be ruled out.
The item ‘ability to understand scientific papers’ was intended to determine whether the participants considered themselves capable of fully understanding the contents of scientific articles. Masuda et al. (2018) reported that among occupational therapists working in convalescent rehabilitation wards, self-efficacy about EBP was the most important factor associated with EBP. This factor included a sub-item with reading systematic reviews, or meta-analysis, and understanding the best scientific evidence. This study’s results were consistent with those of Masuda et al. (2018), which, despite being from different fields, indicated that the ability to understand scientific papers is important to the practice of EBOT. In addition, Döpp et al. (2012) reported that the biggest barrier to EBP among Dutch occupational therapists was the ability to assess the quality of evidence, that is, the ability to examine an article critically. Bennett et al. (2003) reported that 61.9% of Australian occupational therapists said they had little or no confidence in assessing the validity of research. In addition, a survey by Bennett et al. (2003) on barriers to practicing EBP found that 54.7% of the participants said they lacked the skills to find the best research evidence, and 45.4% said they lacked the skills to understand research. In the present study, ‘ability to understand scientific papers’ was the factor with the largest impact, and the step that was practiced most infrequently in question item (3) was ‘critical examination of the available information’. This suggests that among occupational therapists who care for patients with dementia in Japan, a lack of reading skills for evaluating the quality of scientific papers is a barrier to EBOT practice. In Japan, there are many occupational therapists who obtain information from both Japanese and English articles. Therefore, the question on ‘ability to understand scientific papers’ was not limited by the language of the published papers.
The item ‘sufficiency of means of obtaining information’ was intended to determine whether the participants were in environments where they had easy access to electronic databases and publications. The item ‘availability of advice’ was intended to determine whether they could get advice from people such as colleagues, non-work acquaintances, and former teachers. Lower-order items to these factors include the availability of the internet, electronic databases, and other facilities, and the presence of superiors and colleagues who can be asked about EBP. These lower-order items, along with ‘sufficiency of means of obtaining information’ ‘availability of advice’, and ‘ability to understand scientific papers’, which were extracted by the multiple regression analysis, are consistent with the results of Masuda et al. (2018), Döpp et al. (2012), and Bennett et al. (2003). Bennett et al. (2003) found that 49.7% of participants were aware that not having access to research literature was a barrier to EBP. In addition, Masuda et al. (2018) cited a work environment that supports EBP as a factor affecting the practice of EBP by occupational therapists working in convalescent rehabilitation wards. In Japan, it is common for occupational therapists to participate in gatherings, such as journal clubs, for self-improvement. However, in general, it seems that the purpose is not to examine the methodology and the results of scientific papers closely. Although national qualifications for occupational therapists do not require renewal, JAOT has made available two qualifications (Authorized or Specialized Occupational Therapists) as additional qualifications to the national qualifications. To acquire and renew these qualifications, knowledge of and the ability to conduct research are required (JAOT, 2020a). As of 2020, occupational therapists who have acquired the additional qualifications are only approximately 0.01% and 0.001% of all occupational therapists in Japan, respectively (JAOT, 2020b). To improve ‘ability to understand scientific papers’, it is important not only to promote classes on research at universities but also to enrich programmes related to EBOT by JAOT.
In the present study, the participants’ age, years of clinical experience, number of qualifications, and number of conferences attended did not correlate with the question item (4) ‘frequency of practice of regular EBOT’. Further, there were no significant differences in practice frequency based on gender, academic degree, or centre type. This suggests that these factors do not affect the practice of EBOT. In a review of the literature on EBOT, Thomas and Law (2013) stated that a graduate education was associated with increased use of research and greater confidence toward EBP skills. However, the present study’s results did not show a correlation between academic degree and the frequency of EBOT practice. In the present study, only 9% of participants had a master’s or doctoral degree, which may indicate that postgraduate education is not widespread enough to show statistical differences due to academic degree. Meanwhile, a weak but significantly positive correlation was observed between the question item (4) and the number of programmes experienced in question item (2). This suggests that more frequent EBOT practice leads to experience with more types of evidence-backed treatment programmes. While this is only a correlation, it is difficult to consider the causal relationship going in the other direction. Therefore, we believe that frequent EBOT practice promotes treatment programmes backed by evidence.
Our study had several limitations. The low response rate may be a source of nonresponse bias, and the presence of selection bias in the participants chosen by the occupational therapy department directors may have affected the results. In addition, there are also many occupational therapists who treat patients with dementia at medical institutions that are not designated as dementia care centres. Therefore, the participants might not adequately reflect the occupational therapist population. However, because patients with dementia in Japan visit various medical institutions, we had no better way of selecting the institutions. Furthermore, because a questionnaire was used, there is a possibility that the participants’ subjectivity affected the results. We attempted to increase survey objectivity as much as possible by adding explanations to clarify the criteria and by having the participants assess the frequency of practicing all EBOT steps, e.g. the frequency of practice of regular EBOT, only after responding to questions about individual steps. Other limitations included inadequate number of occupational therapists reviewed the preliminary questionnaire. Furthermore, neither information about their years of experience with dementia, dementia-specific training attended by the occupational therapists, nor the clinical models used in their settings was obtained.
Conclusion
The three factors extracted in this study, namely ability to understand scientific papers, sufficiency of means of obtaining information, and availability of advice, indicate that to promote EBOT practice for patients with dementia, it is important for occupational therapists to improve their reading comprehension skills so they can evaluate the quality of articles, and to create environments where they have access to publications and where they can easily discuss research with superiors and colleagues.
Meanwhile, the frequency of EBOT practice did not correlate with gender, age, clinical experience, number of qualifications, academic degree, conferences attended, or centre type. This indicates that enhancing the three extracted factors is important to promote EBOT for patients with dementia.
Footnotes
Acknowledgements
We would like to thank Ms. Misato Sasaki, Ms. Sara Kuriki, and Ms. Miki Kobayashi for helping in the preliminary survey. We also thank all the occupational therapists working at the designated dementia care centres nationwide who cooperated with the study. We would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.